Embed Size (px)
Citation preview
CROSS FIRE UNA FILA VS DOBLE FILA
TRATAMIENTO ATROSCOPICO
SERGIO REA
UNIVERSIDAD CENTRAL DEL ECUADOR
POSTGRADO ORTOPEDIA Y TRAUMATOLOGIA
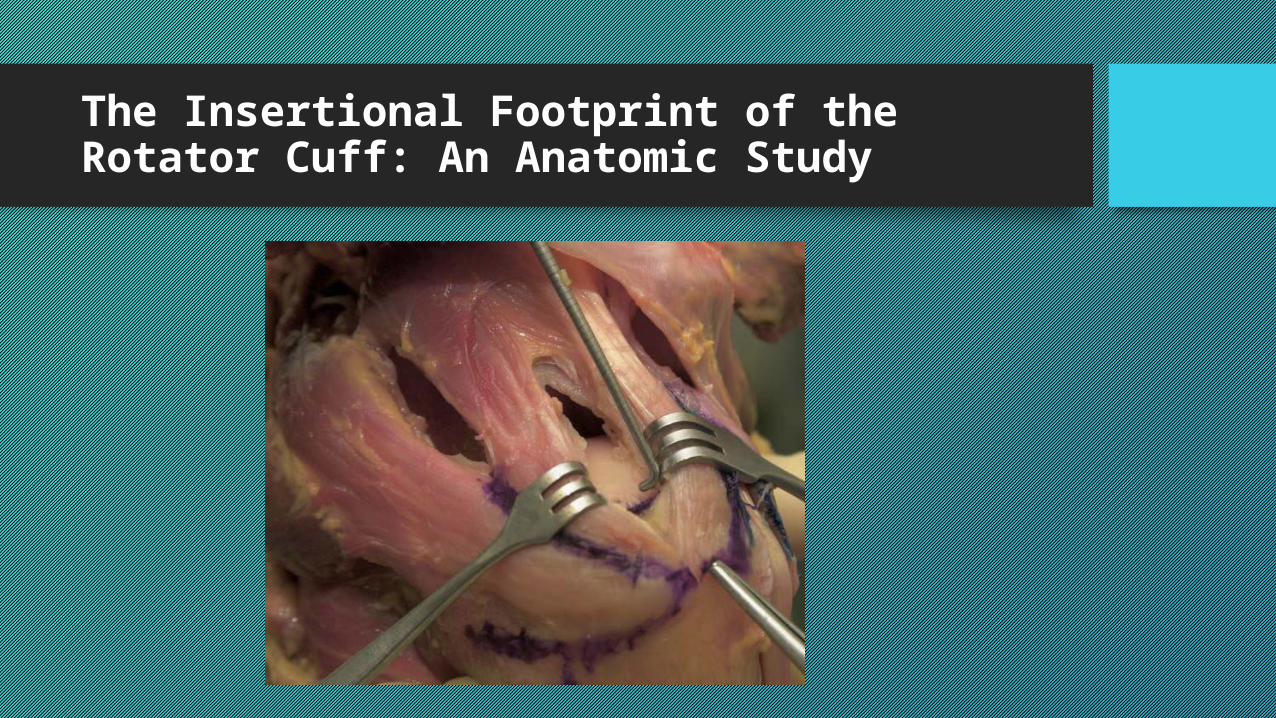
The Insertional Footprint of the Rotator Cuff: An Anatomic Study Alan S. Curtis, M.D., Kelton M. Burbank, M.D., John
J. Tierney, D.O., Arnold D. Scheller, M.D., and Andrew R. Curran, D.O.Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 22, No 6 (June), 2006
• El propósito de este estudio fue definir toda la huella.
• 36 Hombros de cadáveres, la edad y el sexo del especímenes eran desconocido
• Anatomía macroscópica y microscópica
• Identificaron las inserciones, longitud y anchura medida.
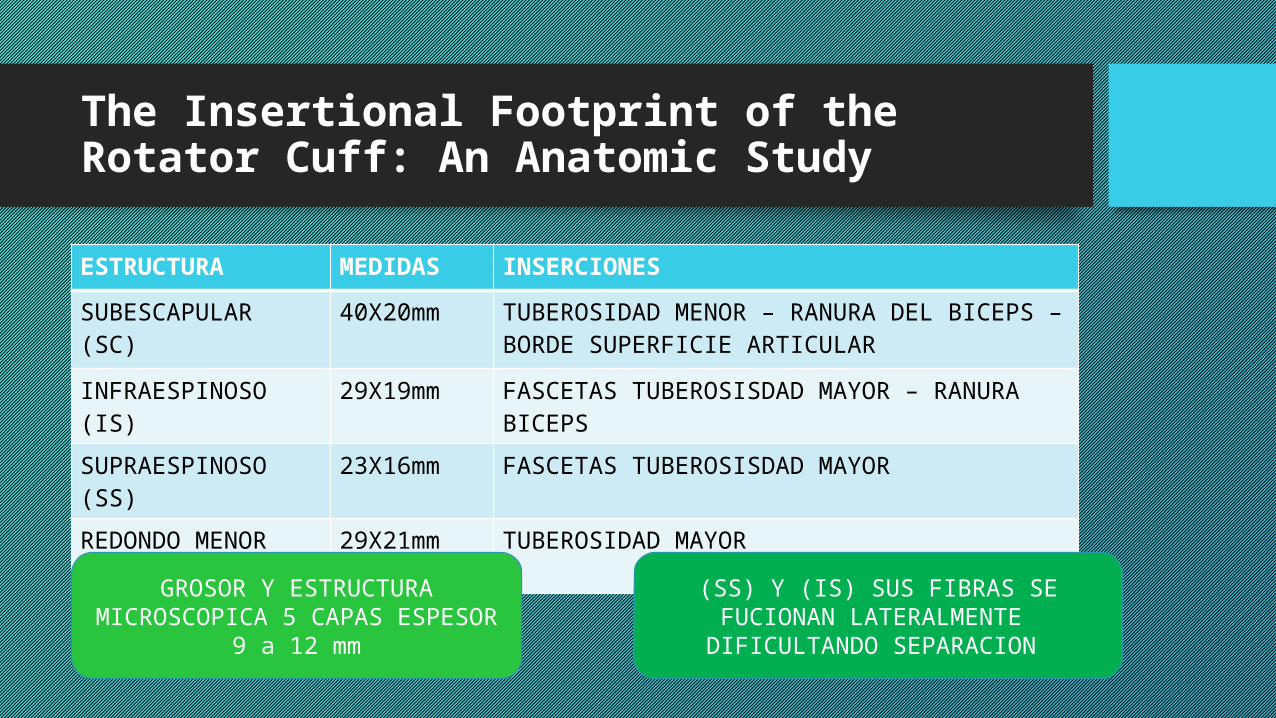
The Insertional Footprint of the Rotator Cuff: An Anatomic Study
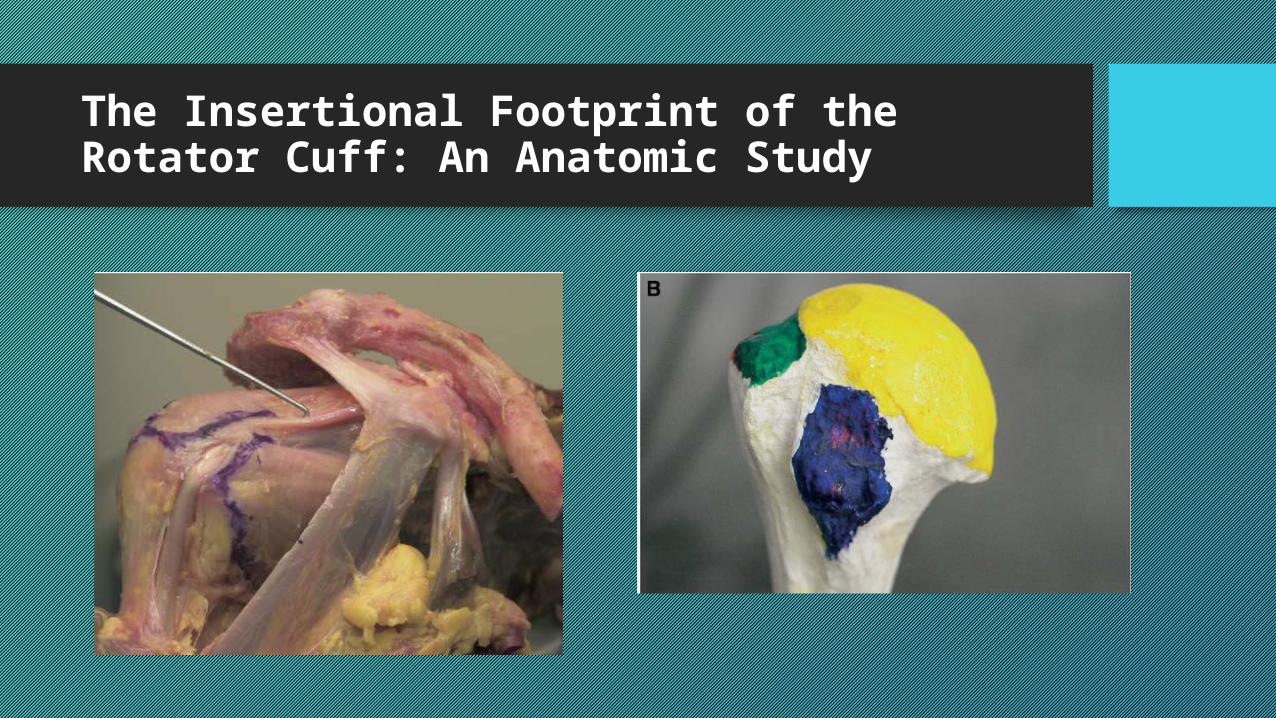
ESTRUCTURA MEDIDAS INSERCIONES
SUBESCAPULAR (SC)
40X20mm TUBEROSIDAD MENOR – RANURA DEL BICEPS – BORDE SUPERFICIE ARTICULAR
INFRAESPINOSO (IS) 29X19mm FASCETAS TUBEROSISDAD MAYOR – RANURA BICEPS
SUPRAESPINOSO (SS)
23X16mm FASCETAS TUBEROSISDAD MAYOR
REDONDO MENOR (TM)
29X21mm TUBEROSIDAD MAYOR
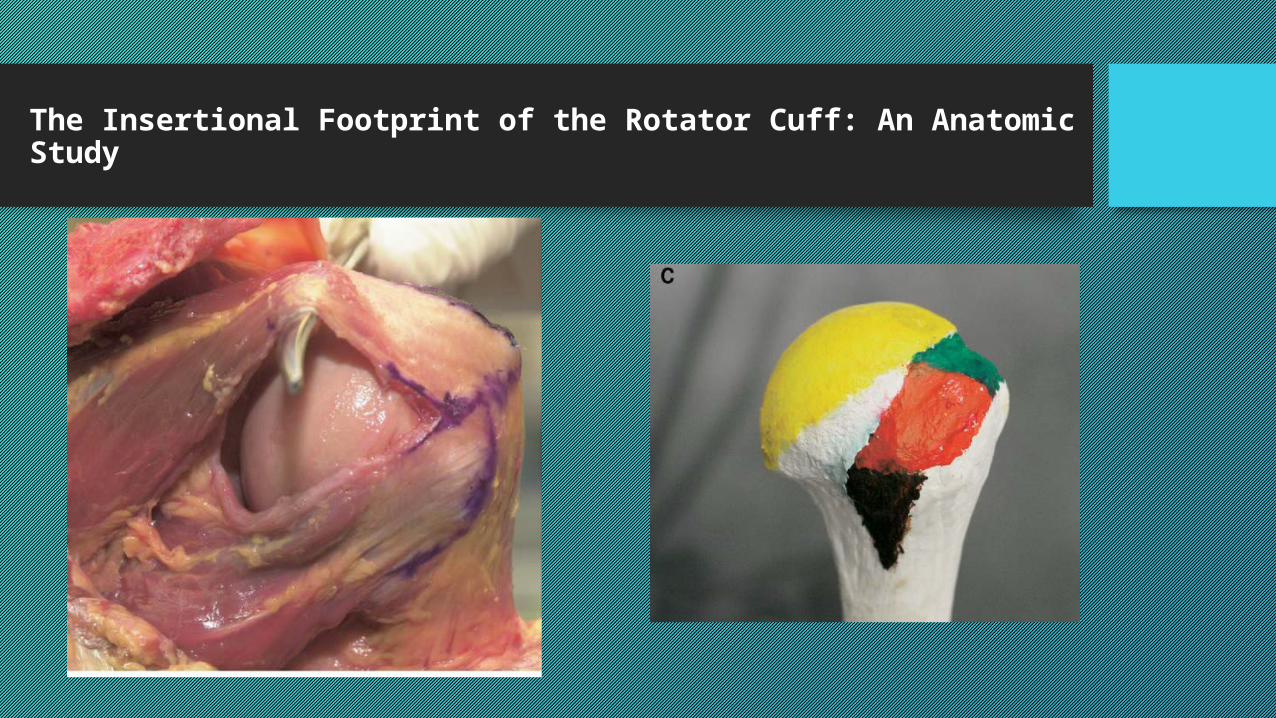
GROSOR Y ESTRUCTURA MICROSCOPICA 5 CAPAS ESPESOR
9 a 12 mm
(SS) Y (IS) SUS FIBRAS SE FUCIONAN LATERALMENTE DIFICULTANDO
SEPARACION
The Insertional Footprint of the Rotator Cuff: An Anatomic Study
The Insertional Footprint of the Rotator Cuff: An Anatomic Study
The Insertional Footprint of the Rotator Cuff: An Anatomic Study
The Insertional Footprint of the Rotator Cuff: An Anatomic Study
The Insertional Footprint of the Rotator Cuff: An Anatomic Study
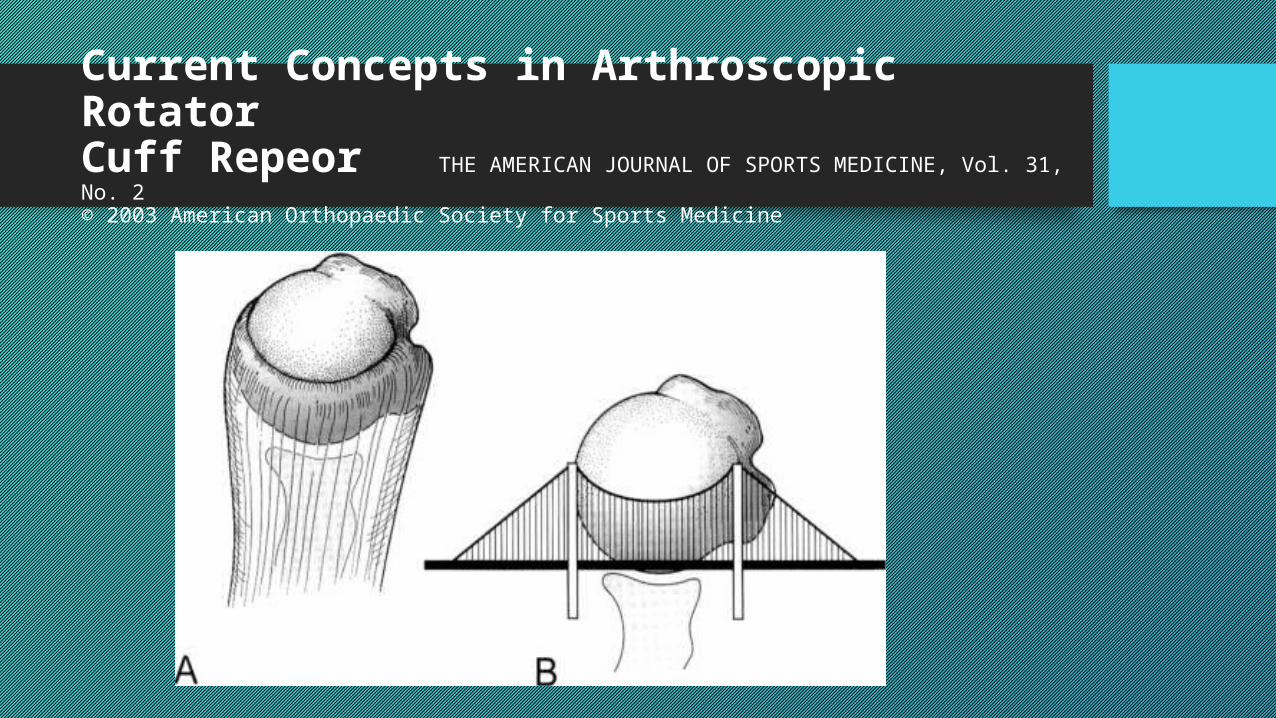
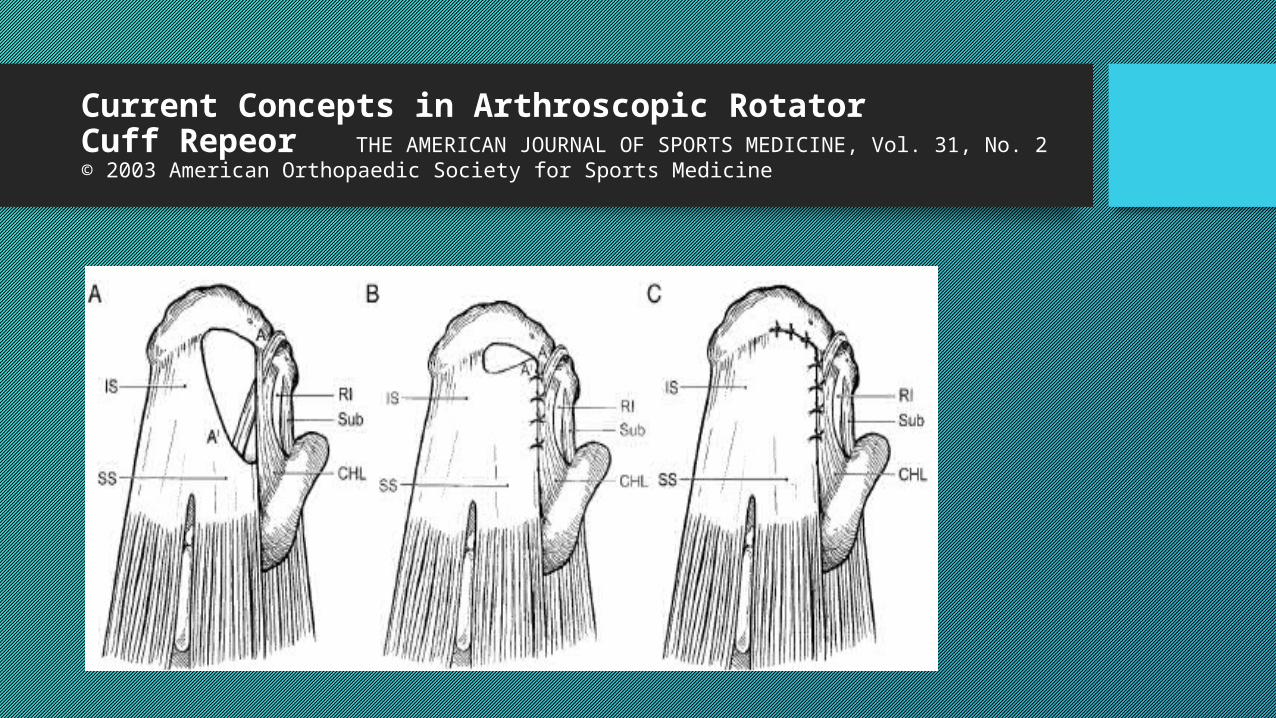
Current Concepts in Arthroscopic RotatorCuff Repeor THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 31, No. 2© 2003 American Orthopaedic Society for Sports Medicine
Current Concepts in Arthroscopic RotatorCuff Repeor THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 31, No. 2© 2003 American Orthopaedic Society for Sports Medicine
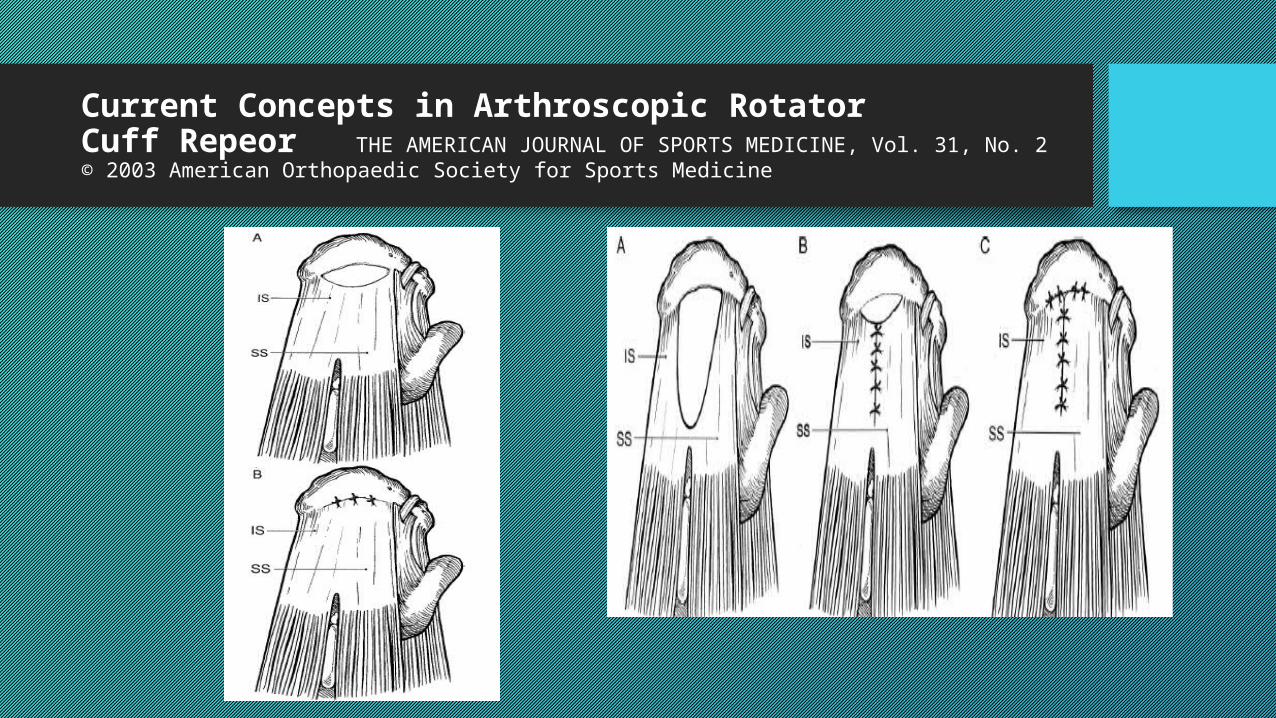
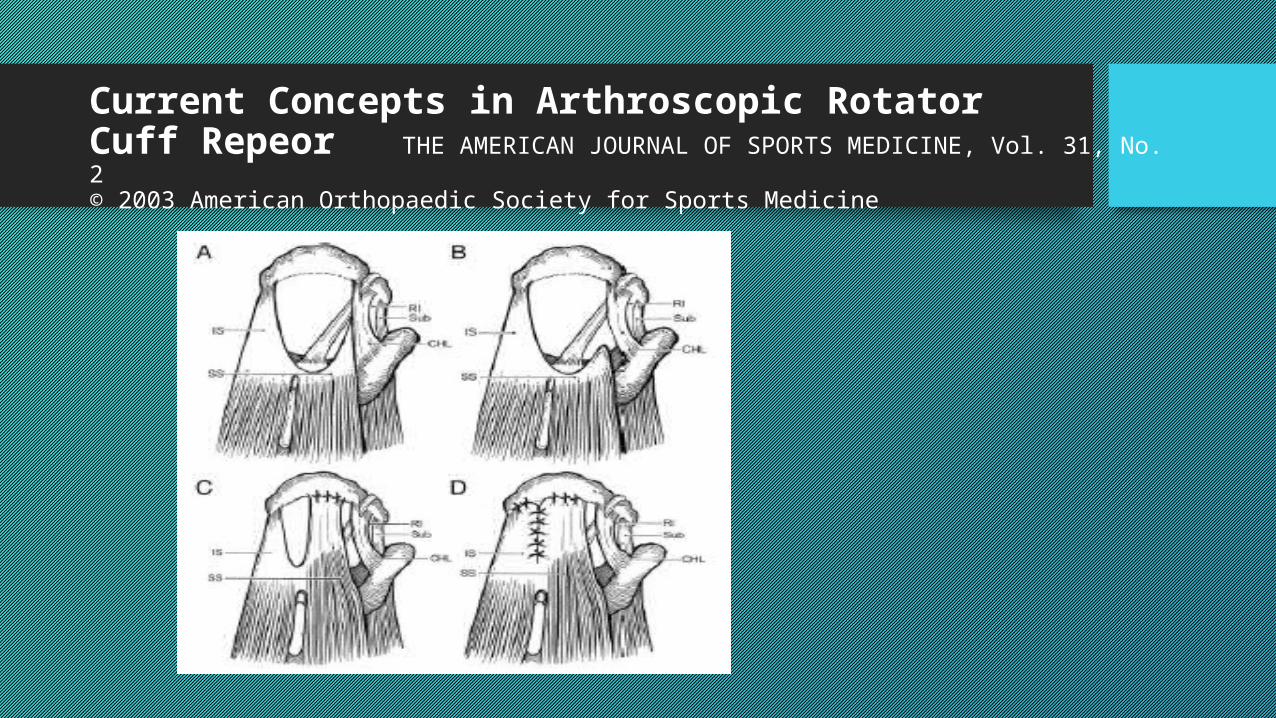
Estas cuatro categorías son: 1) Medialuna2) Forma de U3) Forma de L4) Las lesiones masivas
Current Concepts in Arthroscopic RotatorCuff Repeor THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 31, No. 2© 2003 American Orthopaedic Society for Sports Medicine
Current Concepts in Arthroscopic RotatorCuff Repeor THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 31, No. 2© 2003 American Orthopaedic Society for Sports Medicine
Current Concepts in Arthroscopic RotatorCuff Repeor THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 31, No. 2© 2003 American Orthopaedic Society for Sports Medicine
Current Concepts in Arthroscopic RotatorCuff Repeor THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 31, No. 2© 2003 American Orthopaedic Society for Sports Medicine
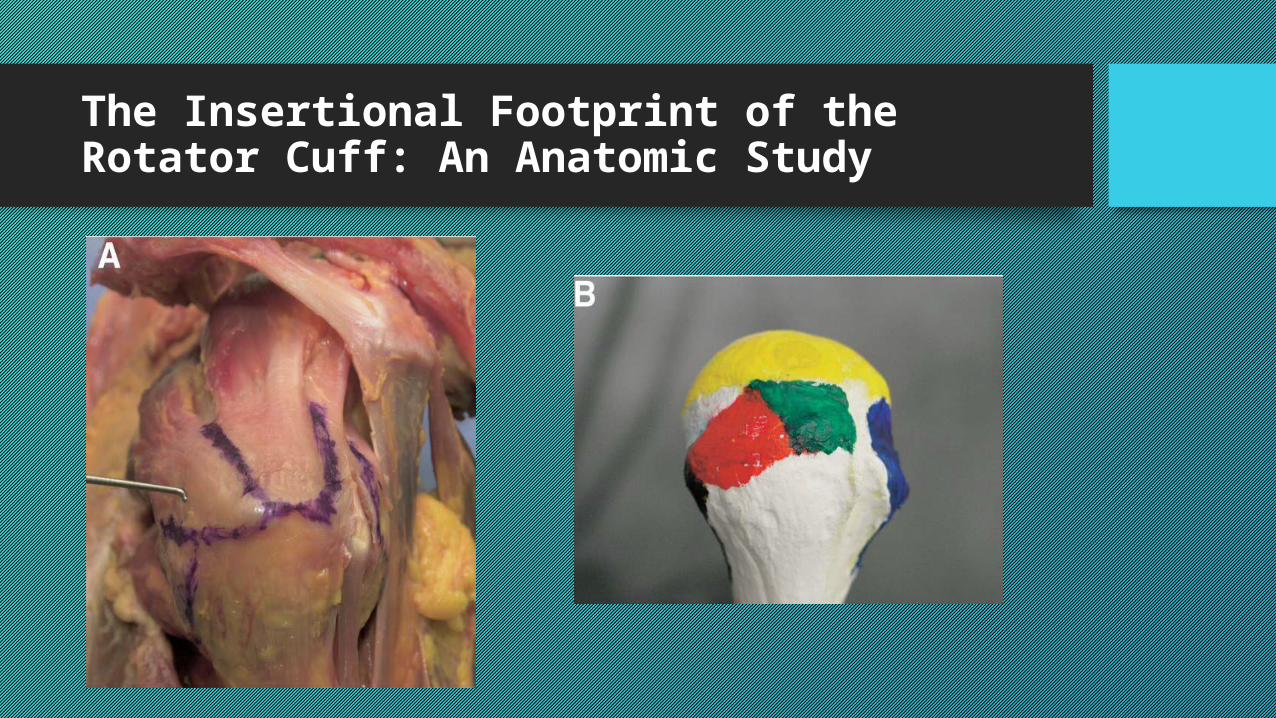
The Insertional Footprint of the Rotator Cuff: An Anatomic Study
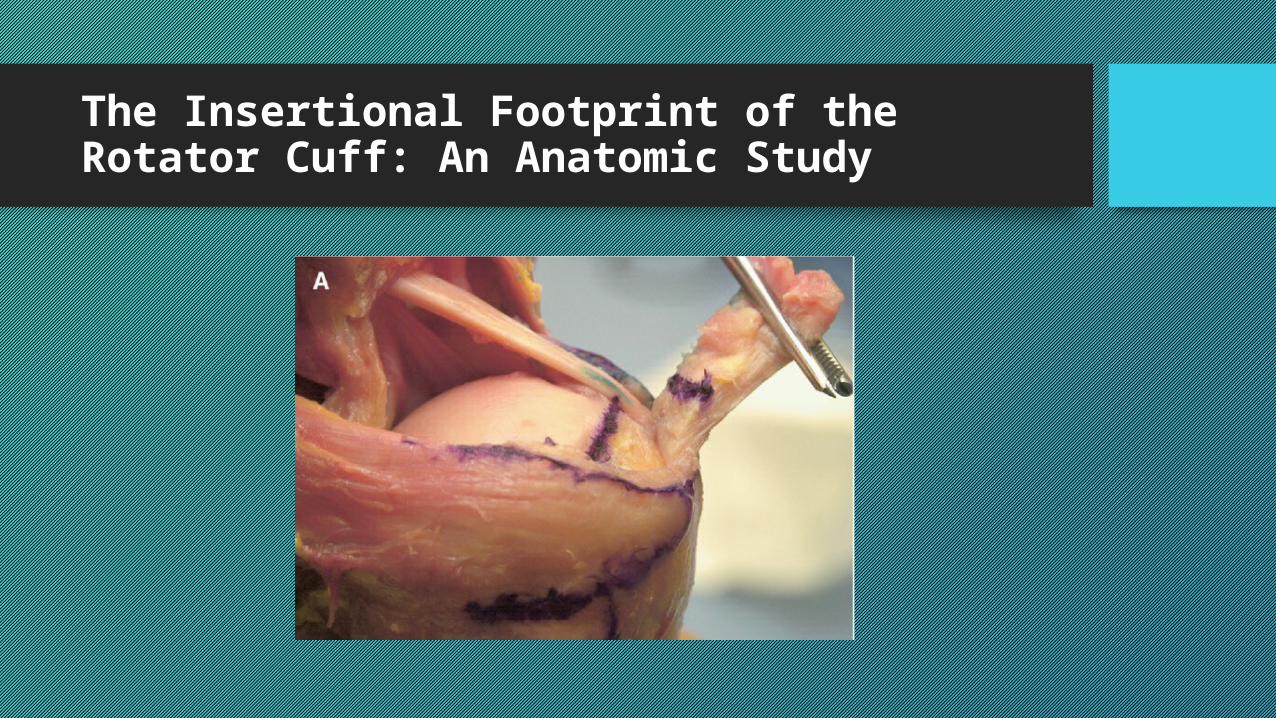
• Inserción propia y única
• Ranura bíceps, la superficie articular, y el área desnuda.
•Huella
The Insertional Footprint of the Rotator Cuff: An Anatomic Study
Teniendo en cuenta la anatomía de inserción normal, una reparación ideal debe volver a crear una amplia zona de contacto hueso-tendón, que debería mejorar la curación y
teóricamente disipar fuerzas sobre un área mayor. Este es el concepto que ha
popularizado recientemente la técnica de reparación "doble fila".
Meta-analysis
Arthroscopic Single-Row Versus Double-Row Rotator Cuff Repair: A Meta-analysis of the Randomized Clinical TrialsShahin Sheibani-Rad, M.D., M. Russell Giveans, Ph.D., Steven Paul Arnoczky, D.V.M., and Asheesh Bedi, M.D.
Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 29, No 2 (February), 2013
Arthroscopic Single-Row Versus Double-Row Rotator Cuff Repair: A Meta-analysis of the Randomized Clinical Trials
El propósito de este meta-análisis fue evaluar críticamente si existen diferencias en los resultados clínicos entre una sola fila y de doble hilera de reparación del manguito de los rotadores en estudios prospectivos aleatorizados Nivel I.
Arthroscopic Single-Row Versus Double-Row Rotator Cuff Repair: A Meta-analysis of the Randomized Clinical Trials
Nivel I ensayos aleatorios prospectivos
de artroscopia
FILA I VS FILA II
12 MESES DE SEGUIMIENTO
BUSQUEDA ENERO 1991 A 2012
4487 ESTUDIOS4358 EXCLUIDOS183 REVISADOS
5 INCLUIDOS
Arthroscopic Single-Row Versus Double-Row Rotator Cuff Repair: A Meta-analysis of the Randomized Clinical Trials
edad media fue de 59,6 años (rango, de 38 a 82
años)
tiempo medio de seguimiento fue de 21,2 meses (rango,
12-44 meses).
indicación para la cirugía fue un fracaso del tratamiento conservador para
3 a 4 meses en pacientes con un desgarro crónico y más reparación inmediata para los pacientes con un desgarro
agudo
Arthroscopic Single-Row Versus Double-Row Rotator Cuff Repair: A Meta-analysis of the Randomized Clinical Trials
FILA SIMPLE 46 - 67%
FILA DOBLE 100%
Arthroscopic Single-Row Versus Double-Row Rotator Cuff Repair: A Meta-analysis of the Randomized Clinical Trials
Meier y Meier han demostrado que la doble hilera técnica de reparación reduce interfase hueso-tendón de movimiento a través de su disposición de puntos de fijación, así como proporcionando la restauración anatómica del supraespinoso inserción del tendón.
Debido a que la técnica de reparación de doble hilera tiene más puntos de fijación a la tuberosidad, que proporciona una mayor área de superficie de contacto huella, lo que lleva a una inserción más grande y una mejor curación.
Arthroscopic Single-Row Versus Double-Row Rotator Cuff Repair: A Meta-analysis of the Randomized Clinical Trials
Las desventajas de la doble hilera técnica de anclaje de sutura son un aumento del tiempo quirúrgico, aumento de los costos, el flujo sanguíneo disminuido, y el aumento dificultad técnica.
CONSENSOArthroscopic Single-Row Versus Double-Row Rotator Cuff Repair: A Meta-analysis of the Randomized Clinical Trials
88 PACIENTES 2002 a 2004 43 sola fila
42 doble fila
78 hombres 54%36 mujeres 46%Edad media 56
años
ASES CONSTANT PRE –
POST QX25 MESES
UNA FILA PEQUEÑAS Y
MEDIANAS LESIONES
DOBLE FILA GRANDFES LESIONES
UNA FILA VS DOBLE FILA
CLINICAMENTE
Curten Concepts
Management of Disorders of the Rotator Cuff: Proceedings of the ISAKOS Upper Extremity Committee Consensus MeetingGuillermo Arce, M.D., Klaus Bak, M.D., Gregory Bain, M.D., Emilio Calvo, M.D.,Benno Ejnisman, M.D., Giovanni Di Giacomo, M.D., Vicente Gutierrez, M.D.,Dan Guttmann, M.D., Eiji Itoi, M.D., W. Ben Kibler, M.D., Tom Ludvigsen, M.D.,Augustus Mazzocca, M.D., Alberto de Castro Pochini, M.D., Felix Savoie III, M.D.,Hiroyuki Sugaya, M.D., John Uribe, M.D., Francisco Vergara, M.D., Jaap Willems, M.D.,Yon Sik Yoo, M.D., John W. McNeil II, B.A., and Matthew T. Provencher, M.D.
Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 29, No 11 (November), 2013
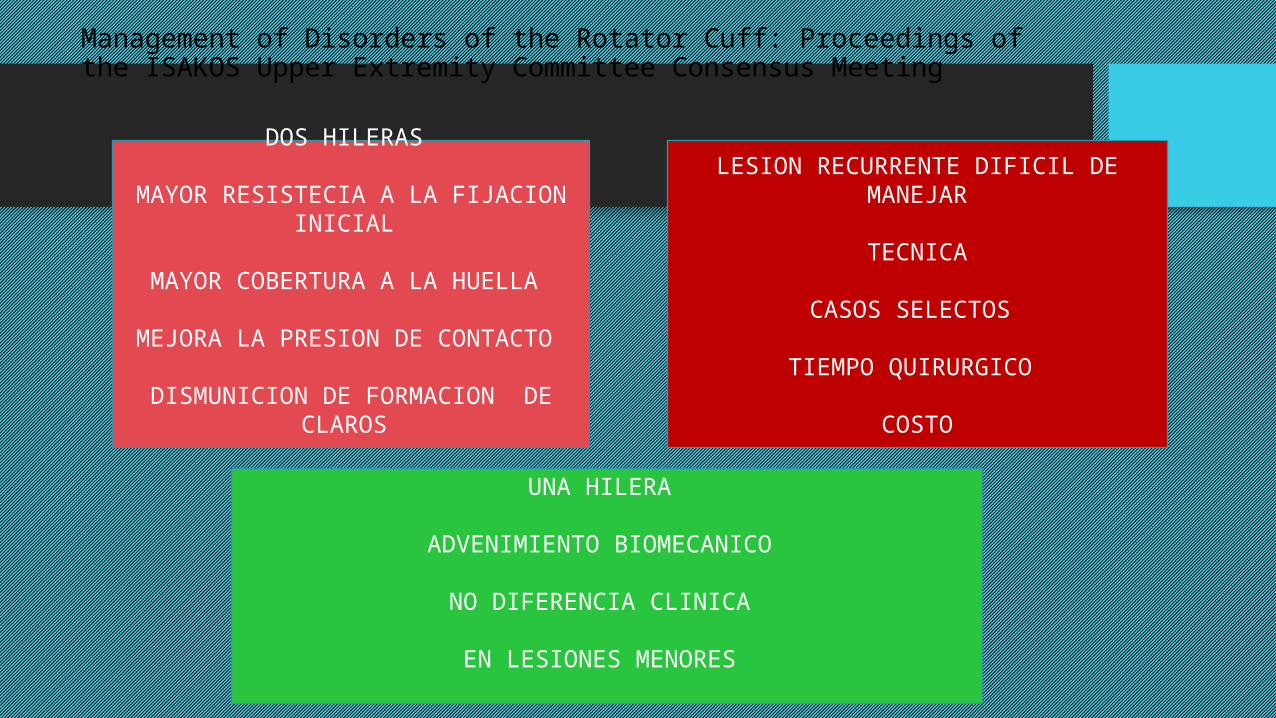
Management of Disorders of the Rotator Cuff: Proceedings of the ISAKOS Upper Extremity Committee Consensus Meeting
DOS HILERAS
MAYOR RESISTECIA A LA FIJACION INICIAL
MAYOR COBERTURA A LA HUELLA
MEJORA LA PRESION DE CONTACTO
DISMUNICION DE FORMACION DE CLAROS
UNA HILERA
ADVENIMIENTO BIOMECANICO
NO DIFERENCIA CLINICA
EN LESIONES MENORES
LESION RECURRENTE DIFICIL DE MANEJAR
TECNICA
CASOS SELECTOS
TIEMPO QUIRURGICO
COSTO





























