Embed Size (px)
Citation preview

GENETICS OF PEDIATRIC ALL
Dr.Aakriti ManochaDr Ankita GroverDr. Prakriti Gupta
23-06-2015

Acute Lymphoblastic Leukaemia (ALL)
Most common childhood cancer◦ In India , Relative proportion varying between 25 & 40% ◦ 60 to 85% of all leukemias reported are acute lymphoblastic
leukemia (ALL)
Compared to developed world, the biology of ALL appears different in India,◦ Higher proportion of T-Cell ALL (20-50% as compared to 10-20% in the developed world)

PATHOGENESIS ALL is malignant clonal proliferation of lymphoid progenitor cells,
most commonly of B-cell lineage (B-ALL).
ALL encompasses ◦ Chromosomal rearrangements◦ Structural variations ◦ Sequence mutations
Distrub cell proliferation, lymphoid maturation, cell growth suppression

Genetic classification of ALL is paramount for risk stratification & in treatment evaluation.

Childhood ALL ◦ B-cell more common than T-cell lineage◦ Hyperdiploidy & chromosomal rearrangements (ETV6–RUNX1) are common.
Adolescents & adults with ALL◦ Inferior outcomes◦ Partly because of lower frequency of favorable genetic features e.g. ETV6–
RUNX1 & hyperdiploidy ◦ Higher frequency of BCR–ABL1





Genetic alterations in ALL
T -ALL
B -ALL
PAX5JAK2CRLF2IKZF1


B-ALL

Recurrent translocations

BCR-ABL1 (Philadelphia chromosome)
INCIDENCE : 3-5% of childhood B-ALL cases
C/F : ◦ Older age ◦ Higher leukocyte count◦ Frequent CNS involvement
PROGNOSIS : Poor
TKIs improved 3-year EFS in children & adolescents
Use of second generation TKI, dasatinib is under investigation

GENETICS : ◦ t(9;22)(q34;q11) translocation ‘Philadelphia chromosome’ (Ph + B-ALL)
◦ Fusion of 5’ sequence of breakpoint cluster region (BCR) on chromosome 22 to 3’ sequence of the ABL1 gene on chromosome 9
◦ Oncoprotein : Constitutively active non receptor tyrosine kinase
( responsible for leukemogenesis)

◦ BCR region contains two breakpoint areas : major BCR (M-bcr) : chronic myelogenous leukemia (CML) minor BCR (m-bcr) : pediatric B-ALL 190 kDa fusion protein
(p190)
IMPORATANCE : ABL1 tyrosine kinase inhibitors (TKIs) e.g. imatinib used in treatment Ph + B-ALL.

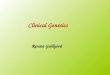
ETV6-RUNX1 (TEL-AML1)
INCIDENCE :◦ Most common chromosomal rearrangement in B- ALL◦ Occurs in 25% of children with B-ALL
Is not associated with any unique clinical features, morphologic or cytochemical features
PROGNOSIS : ◦ Confers an excellent prognosis

GENETICS :
Translocation between TEL (ETV6) gene on chromosome 12 with AML-1 gene on chromosome 21 { t(12;21)(p13;q22) }
◦ NORMAL HEMATOPOIESIS : ETV6 & RUNX1 transcription factors ETV-6 is a transcriptional repressor Co-repressors : mSin3A , N-CoR, HDACs
◦ In ALL : N – terminal of ETV-6 ( TEL - translocation – ETS- leukemia)
is fused to coding region of RUNX-1
◦ ETV6-RUNX1 fusion protein disrupts normal expression of RUNX1-regulated genes
Converts RUNX1 to a transcriptional repressor

FIFISH technique

MLL gene rearrangements INCIDENCE : 80% of Infant B-ALL 10% of Childhood B-ALL
CLINICAL FEATURES : ◦ Very high WBC counts >100 X 10^9◦ High frequency of CNS involvement
IMMUNOPHENOTYPE :◦ CD10 negative◦ CD19 positive◦ CD24 negative◦ CD15 positive

GENETICS : ◦ MLL (mixed-lineage-leukemia) gene rearrangements at 11q23
◦ MLL gene encodes for protein with histone methyl transferase activity
Essential for hematopoietic regulation of HOXA & MEIS1 gene
expression

◦ Most common gene rearrangements : t(4;11) (q21;q23) (AF4) {50% of MLL} t(9;11) (p22;q23) (AF9) t(11;19) (q23;p13.3) t(10;11) (p13-14;q14-21) (AF10)
PROGNOSIS : Adverse outcomes◦ EFS of approx 35% (Cellular drug resistance)

MULTISTEP PATHOGENESIS OF MLL-REARRANGED ALL• MLL translocations
induce self-renewal in hematopoietic progenitors (1st step in leukemogenesis.)
• Presence of FLT3 mutations in MLL-rearranged ALLs support activation of FLT3 or other kinases as cooperating events in this disease.
• Clinical trials designed to assess the efficacy of FLT3 inhibitors in MLL-rearranged ALL are being developed.

TCF3-PBX1 (E2A-PBX1) INCIDENCE : The translocation occurs in 6% of childhood B-ALL
(pre– B-ALL)
IMMUNOPHENOTYPE : ◦ Strong CD 9 expression◦ Limited CD34 expression
PROGNOSIS : Poor
Advances in treatment now has intermediate prognosis

GENETICS : t(1;19)(q23;p13) rearrangement
TCF3(E2A) on chromosome 19p fuses with PBX1 on chromosome 1q
TCF3-PBX1 (E2APBX1) fusion protein comprises transactivation domains of TCF3 & DNA binding domain of homeobox protein PBX1.
◦ Converts PBX1 into a transactivating factor
◦ Reduces expression of TCF3 encoded transcription factors E12 & E47, required for early lymphoid development .

t (17;19)(q22;p13.3) INCIDENCE : 1% of paediatric ALL
GENETICS : Fuses TCF3 to HLF ( hepatic leukemia factor) Homologous to TCF3-PBX1 fusion protein
C/F : ◦ Occurs in adolecents◦ Present with DIC & hypercalcemia
PROGNOSIS :◦ Poor

IGH@ translocations Rearrangements of the immunoglobulin heavy chain locus (IGH@) on
chromosome 14q32 INCIDENCE : <5% of cases
CLINICAL FFEATURES :◦ Frequent in adolescents
PROGNOSIS : Poor
GENETICS : ◦ Most common IGH@ partners : CRLF2 (cytokine receptor-like factor 2) at
Pseudo Autosomal Region 1 (PAR1) of Xp22.3/ Yp11.3
◦ Result : Over expression of CRLF2◦ Others
ID4 (inhibitor of DNA binding 4) at 6p22 members of CEBP (CCAAT/enhancer binding protein) family
Translocations between IGH@ & EPOR (erythropoietin receptor) at 19p13

t(5;14) (q31;q32) ; IL3-IGH CLINICAL FEATURES :
◦ Similar to ALL◦ Or asymptomatic eosinophilia ◦ Blasts may not even be present in PB to raise suspicion of
leukemia
MORPHOLOGY : Striking feature: Increase in circulating eosinophils
GENETICS : Functional rearrangement between IL3 gene on chromosome 5 & IGH@ on chromosome 14
RESULT : Constitutive over expression of IL3 gene

Intrachromosomal amplification of chromosome 21 (iAMP21)
Presence of three or more copies of the RUNX1 gene within a
morphologically abnormal chromosome 21.
INCIDENCE : 2% of older children with B-ALL
PROGNOSIS : Poorer outcomes : Standard therapy :◦ Increased risk for early & late relapse◦ Treatment of these patients as high-risk provides significant
improvement in outcome

GENETICS :
Amplified regions on chromosome 21 (5.1 Mb region ) containing RUNX1
Abnormalities associated :◦ P2RY8-CRLF2 fusion results in overexpression of CRLF2
◦ Gain of X chromosome
◦ Abnormalities affecting genes IKZF1 (Ikaros), CDKN2A, PAX5, ETV6 & RB1
◦ Constitutional Robertsonian translocation rob(15;21) have 2700-fold increased risk of developing B-ALL with iAMP21

High Hyperdiploidy 51–65 chromosomes : Most common
INCIDENCE: 25-30% of childhood B-ALL cases
GENETICS : Nonrandom gain of chromosomes, Includes + X, +4, +6, +10, +14, +17, +18, & +21PROGNOSIS : Good prognosis EFS rates of approx 80% Overall survival (OS) rates of 90%
Aneuploidy

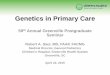
Evaluation of a 3 year-old boy with hyperdiploid B-ALL.
Hyperdiploid karyotype with extra copies of chromosomes X, 21, 9, 14.
12p deletion was observed in 89% of the nuclei examined
Suggestive of an underlying complex aneuploid (most likely hyperdiploid) karyotype.
FISH technique
Karyotyping
ALL

Hypodiploidy < 46 chromosomes
INCIDENCE : 5-8%
GENETICS : Current high risk COG protocol : Hypodiploidy < 44 chromosomes Hypodiploid B-ALL contain 45 chromosomes (MOSTLY)
High-hypodiploid 40–44 chromosomes Low hypodiploid 33–39 chromosomes Near haploid 24–29 chromosomes
PROGNOSIS : Hypodiploidy < 40 chromosomes confers poor prognosis

Ikaros Mutations (High-Risk B-Precursor ALL) Ikaros is DNA-binding transcription factor
◦ Required for development of all lymphoid lineages
IKZF1 deletions: 15% of childhood ALL cases
IKZF1 alterations : > 70% of BCR-ABL1 lymphoid leukemia
Ikaros deletions are strongly associated with: ◦ BCR–ABL-positive ALL◦ Acquired at transformation of CML to ALL (lymphoid blast crisis)

Ikaros deletions predict very high risk of treatment failure that appears to be independent of BCR–ABL
Patients with Ikaros -deleted, BCR–ABL negative ALL have similar poor prognosis as with BCR–ABL-positive ALL
Mutational activation of CRLF2-JAK2 signaling in Ikaros-deleted, BCR–ABL-negative ALL.
In view of clinical activity of imatinib in high-risk BCR–ABL ALL, there is a need for clinical trials of small molecule inhibitors of JAK-STAT signaling in this high-risk subtype of B-precursor ALL.

T-ALL

TAL1 (T-cell ALL 1/ Stem Cell leukemia)
INCIDENCE : 25% of T-ALL
GENETICS : t(1;14)
TAL1 and TAL2 are not expressed in the normal thymus but can be ectopically expressed in T-ALL
TAL1 (SCL, TCLS) maps on chromosome 1p32
Rearrangements of this locus are frequent in childhood T-ALL resulting in TAL1 activation either as a consequence of the t(1;14) (p32;q11)
More often due to a submicroscopic interstitial deletion generating the SIL-TAL1 fusion gene
Leukemogenic activity of TAL1 is not completely understood Aberrant TAL1 expression may contribute to leukemia by interfering with
differentiation and proliferation by inhibiting

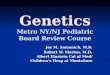
NOTCH SIGNAL
Fruit fly Drosophila with notched wing Resulted from partial loss of function of Drosophila Notch gene
FUNCTION: ◦ Regulates cell proliferation, differentiation, apoptosis & survival
Notch1 signaling is essential to induce T-cell lineage commitment from multipotent hematopoietic progenitor cells (HPCs)

Ligand-receptor interaction 2 successive proteolytic
cleavages of receptor:◦ First cleavage : Key
regulatory step in Notch activation
◦ Second cleavage : Mediated by the γ-secretase
Release the intracellular portion of the Notch receptor (ICN) from the plasma membrane
Translocates to nucleus Binds to DNA-binding
transcriptional factor CSL

LEVELS OF MODULATION OF NOTCH 1. Fringe proteins :
◦ Glycosyltransferases inhibit Notch signaling (interfere with Notch receptor-ligand)
◦ Fringe decreases T-cells & induces lymphoid progenitor to adopt B-cell fate in thymus
2. γ-secretase inhibitors (GSIs) :◦ Treatment of T-ALL cells with GSI results in cell cycle arrest
followed by apoptosis
3. MAMLs important for Notch-dependent CSL transcriptional activation

Early t-cell precursor ALL (ETP-ALL) Leukemic blasts exhibit expression of cytoplasmic CD3
no expression of CD1a & CD8
weak or absent expression of CD5 Aberrant expression of stem cell & myeloid markers
INCIDENCE: 10%-15% of childhood & adult ALL
PROGNOSIS : Poor treatment response induction failure poor event-free survival

NUP214-ABL1 IN T-CELL ALL
INCIDENCE: 6 % of childhood & adult T-cell ALL
GENETICS :
◦ Fusion of the genes NUP214 & ABL1 in the genomic region of chromosome 9q34
◦ Breakpoint of ABL1 is intron1 ( similar to PH+ CML & B-cell ALL)
◦ Breakpoint of NUP214 is variable
◦ Fusion protein : Constitutively active ABL1 tyrosine kinase activity
IMPORTANCE : Use of Imatinib or second generation tyrosine kinase in ABL1 + T– ALL

FLT3 IN MLL Rearranged ALL Receptor tyrosine kinase Highly expressed in early hematopoietic precursors
GENETICS: ◦ Activating mutations of FLT3◦ Constitutive receptor tyrosine kinase activity (even in the absence of ligand)
◦ Common in Myeloblasts in patients with AML Rare in adults with ALL◦ FLT3 in association with ALL : MLL gene rearrangements or
hyperdiploidy.
INCIDENCE : ◦ Activating mutations in 18% of infants with MLL-rearranged ALL◦ 21% to 24% of hyperdiploid ALL cases

INTERLEUKIN 7 receptor mutations in T-ALL
IL-7R alpha is required for normal T- cell development
INCIDENCE : 10% of T-ALL
GENETICS : ◦ Point mutations of IL-7R
◦ Induces ligand –dependent receptor dimerisation Activation of downstream oncogenic signal transduction
pathways e.g. JAK-STAT, PI3K-AKT.

TUMOR SUPPRESSOR GENES P-53 :
◦ Located on chromosome 17, band p13◦ Encodes a transcription factor involved in cell cycle & apoptosis
checkpoint regulator
Mutated or lost through chromosomal deletion
In 3 of 10 ALL cases who failed induction therapy or suffered early relapse show p-53 mutations
(p-53 inactivation is involved in disease progression)

p53:◦ Inactivated in :
B –ALL Burkitt lymphoma
◦ Mutated or deleted in: <3% pediatric B- precusor or T-cell ALL
◦ Associated with 25% of relapsed T-cell ALL : Role in resistant disease

Cyclin Dependant Kinase inhibitors ( CDK)
Tumor suppressors p15, p16, p18, p19 , p21, p27, p57 Inhibit CDK phosphorylation
Most common : Short arm of chromosome 9
9p21 deletions :◦ p16/ p14 : 20-30% B-All 70-80% of T ALL◦ p15 : 44% of primary B lineage

FBW7 in T-cell ALL
Targets transcriptionally active form of NOTCH, MYC & cyclin E Inactivated by : Deletion, mutation In 10% T- ALL cases
PAX-5 : Most common in B-ALL


These rearrangements are important initiating events in leukemogenesis
Widely used in diagnosis & risk stratification algorithms
However, are insufficient to fully explain leukemogenesis

To characterize genetic basis of leukemogenesis
To understand & predict treatment failure
To provide novel markers that may be integrated into diagnostic testing
Targeted with novel therapies
High resolution Genomic profiling

> 50 recurring deletions / amplifications have been identified
Lymphoid development PAX5, IZKF1, EBF1, LMO2
Cell-cycle regulation & tumor suppression◦ CDKN2A/CDKN2B, PTEN, RB1
Lymphoid signaling ◦ BTLA, CD200, TOX, glucocorticoid receptor NR3C1
Transcriptional regulation & coactivation◦ TBL1XR1, ETV6, ERG
Key role of Genes encoded proteins


Chromosomal rearrangements acquired early in leukemogenesis ◦ drive transcriptional & epigenetic dysregulation ◦ aberrant self-renewal
These lesions and/or secondary genetic alterations disrupt lymphoid development & result in an arrest in maturation.
Additional genetic alterations target multiple cellular pathways including cell-cycle regulation, tumor suppression, and chromatin
modification.
Result in the proliferation and establishment of the leukemic clone.
Diagnosis ALL samples are commonly clonally heterogeneous Genetic alterations in minor clones may confer resistance to therapy

CRLF2 rearrangements & JAK mutations in ALL
CRLF2 rearrangements : ◦ 7% of childhood ALL cases ◦ 50% of cases associated with Down syndrome (DS-ALL)
CRLF2 is◦ Rearranged (IGH@-CRLF2) or,◦ More commonly, by a focal deletion upstream of CRLF2 –
aberrant ◦ Overexpression of CRLF2 on the cell surface of leukemic
lymphoblasts

CRLF2 mutations / reaarangements are associated with :Mutations in JAK genes “JAK1 and JAK2”
Regardless of JAK mutation status, the leukemic cells harboring CRLF2 deregulation◦ Exhibit activation of JAK-STAT & PI3K/mTOR pathways◦ Sensitive to JAK and mTOR inhibitors in vitro and in vivo
An early-phase trial of JAK inhibitor ruxolitinib in relapsed & refractory childhood tumors (including cases with CRLF2
rearrangement and/or JAK mutations) has been initiated

BCR-ABL1–like ALL
Common in adolescent & young adult ALL
Lack chromosomal rearrangement but exhibit a gene expression profile highly similar to that of BCR-ABL1
Prognosis : poor
GEP- half cases harbor rearrangements of CRLF2 and JAK1/2 sequence mutations

Hypodiploidy Hypodiploidy with < 45 chromosomes is associated with very
high risk of treatment failure Genetic basis of which has been poorly understood
Sequencing showed that NH-ALL has a very high frequency of deletions & sequence mutations that activate Ras signaling
NH- and LH-ALL have a high frequency of inactivating alterations of the IKAROS genes IKZF2(HELIOS) and IKZF3 (AIOLOS) that are otherwise rare in ALL

GEP showed that NH- and LH-ALL are distinct diseases
Demonstration of Ras pathway activation by biochemical & phospho signaling analysis
Therapeutic targeting of this pathway Novel treatment outcome in this high-risk leukemia

CREBBP
Deletion / mutation of CREBBP ◦ encoding the transcriptional coactivators◦ acetyltransferase CREB binding protein (also known as
CBP)
Present in almost 20% of relapsed ALL cases
Enriched in relapsed hyperdiploid ALL, a subtype normally associated with favorable outcome

CREBBP mediates transcriptional response to glucocorticoid therapy
Mutations shown to disrupt normal transcriptional response to glucocorticoids.
Therefore,
◦ CREBBP mutations may represent an important mechanism underlying treatment failure in ALL
◦ May be targeted with agents that modulate level of histone acetylation in leukemic cells
(such as Histone deacetylase inhibitors)

ETP-ALL
ETP-ALL associated ◦ with poor treatment response◦ induction failure◦ poor event-free survival
10%-15% of childhood and adult ALL

Examined frequency of novel & recurring genetic alterations in an additional 54 ETP- and 42 non–ETP-ALL patients
Genes of 3 pathways are commonly mutated in ETP-ALL:
These pathways—◦ Hematopoietic development◦ Signaling ◦ Epigenetic regulation
Also frequently mutated in AML.
Transcriptional profile of ETP-ALL is highly similar to that of normal hematopoietic stem cells, and that of high risk AML but not normal human ETP

Findings suggest that non-ALL regimens whether myeloid directed, targeted, or epigenetic therapies,
should be pursued in this disease.

RECENTLY IDENTIFIED MUTATIONS

THANKYOU