Embed Size (px)
Citation preview
Rachael Lang1006190l
Signalment: 8 week old, male entire, Italian Greyhound purchased 2 weeks ago
History: Vomited twice and diarrhoea twice throughout day. Quieter in demeanour, inappetent and not drinking.
Clinical exam: HR 180, pale mm, pulses narrow, RR 36, T 38.1, no skin tent, quiet mentation.
Diagnostics: PCV/TS: 35/50 Blood gas and electrolytes: WNL Haematology: degenerate left shift with a monocytosis Faecal smear: mixed bacterial population and occasional WBC
(normal) Parvo Antigen test: negative Fast scan: no free fluid or distended small intestine loops Faecal sample for c&s not sent off as resolved
Differentials: Dietary indiscretion, parvo virus, bacterial enteritis, foreign body ingestion, parasites
Treatment: Admit for IVFT Hartmanns 10ml/kg bolus then 40ml/hr Buprenorphine 0.01mg/kg q 8 Metronidazole 10mg/kg IV q12 then oral tablets for 5 days Protexin Probiotic
Outcome: Following day he was stable and eating chicken without any
vomiting or diarrhoea. No abnormalities found on clinical exam.
Discharged with a 5 day course of oral metronidazole and protexin probiotic.
Informed to come back if any further gastrointestinal signs occurred
Signalment: 9 month old female entire Kelpie cross Reason for presentation: Hit by car going at 40-
50km/he about 1.5 hrs ago. Clinical exam: Very dull mentation, HR 140, white
mucous membranes, CRT 3s, pulses short and shallow, painful on gentle abdominal palpation, T:38.1
Stabilisation: Free flow oxygen by mask IVFT: Hartmanns 800ml/hr bolus for fifteen minutes then
reassessed and decreased to 200ml/hr Pain relief: Methadone 0.01mg/kg (twice) Abdominal wrap to reduce venous bleeding
Diagnostics: Fast scan:
Abdomen: Large volume of free fluid around bladder (ddx: uroabdomen vs haemoabdomen).
Splenic mass on repeat fast scan. Thorax: no FF
Abdominocentesis: Frank blood in abdomen; PCV/TP of fluid: 51/46
BP: systolic 120 SpO2: 91% Urine: grossly normal ECG: right bundle block, intermittent VPC’s and transient runs of
V-tach Bloods:
PCT/TP: 41/46 (decreased after fluid therapy to 21/29 Blood Gas and lytes: metabolic acidosis (SBEc:-6
) with no respiratory compensation. Lactate high due to hypoperfusioninjury. Glucose high due to stress
Treatment: Packed red cells transfusion (after cross matching) as Olive’s PCV/TP
dropped to 21/29 and she became tachycardic. Post transfusion her mucous membranes became more pale pink than white, her HR dropped to 120 and her pulses were much better
IVFT which was tapered based on her clinical signs down eventually to maintenance 2 days after presentation
Pain relief: 2mg methadone was given for first two days. Tramadol was used instead of methadone after day 2 as she did not seem to painful
and responded well to the first trial of tramadol
Other medications: Maropitant as Olive was hypersalivating and seemed nauseous after methadone
Outcome:Olive went home on 50mg Tramadol TID after her PCV had increased and her clinical parameters returned to normal. The amount of free fluid in her abdomen decreased due to reabsorption.
Signalment: 4 year old MN outdoor DSH History: Owner saw cat in fight yesterday and today he
seems dull, lethargic, in-appetant and not himself. Clinical exam: HR 200, mm pink and moist, CRT 1s, pulses
normal, Temp: 39.6, R 20, normal auscultation, Abdopalpation normal, integument had several cat scratches and after searching a cat bite which was inflamed and painful was identified on the left hind leg, orthopaedic and neuroexams normal.
Diagnostics: Searched whole body for cat bites as history of being in fight. Shaved cat in area where sore and located bite
Treatment: Amoxycillin and clavulonic acid injection and 5 day course PO 0.06mg Buprenorphine subcut and 5 days sublingual
Buprenorphine
Signalment: 4 year old female entire Chow Chow History: Season started 4 weeks ago (usually lasts 2 weeks),
bleeding throughout but had decreased in past week till today when increased again. Drinking twice as much as normal. Reduced appetite for 2 weeks and today completely inappitant.Lost 4kg in weight in 2 weeks. Vomited twice last night. Ate bone two weeks ago and not been right since.
Diagnostics: Clinical exam: HR 160, Pulses tall and narrow, distended abdomen, Caudal
abdominal pain, very flat mentation, T 40.6, panting Abdominal Ultrasound – 2 large fluid filled uterine horns visible but no
flocculent material Abdominal rads to rule out FB refused by owner Full bloods: refused by owner (suspect neutrophilia or neutropaenia also
potentially azotaemia) PCV/TP 37/110 Glucose 3.3mmol/l (indicates likely septic) Lactate 2.2, Cl 127, SBE -11 (metabolic acidosis)
Rectal exam: tachy mucosa, normal faeces Vaginal exam: no free flowing discharge, smear of vaginal mucous showed
no WBCs
Ddx: Pyometra – closed or open but not currently discharging or foreign body
Stabilisation IVFT LRS Bolus of 60ml/kg/hr for 15 minutes
Treatment: Advised spaying but refused due to financial concerns so stabilised as much as possible. Plan to take to GP vets in morning. Advised against medical management as presented so sick. Warned of risks of deterioration, sepsis and uterine rupture. IV Ticarcillin 40mg/kg q 6 IV Buprenorphine 0.01mg/kg q 8 IVFT LRS post bolus of 5ml/kg/hr spiked with 2.5% glucose as
heart rate decreased to 130 but only lasted 20 minutes before coming back up
Outcome: Temp reduced overnight to 38.6, panting all night and taken to GP vets at 8am.
Signalment: 2 SBT, 10 yr and 13 yrs MN History: Owner found both dogs near chocolate bar (200g plain
milk chocolate – 40mg/kg if one dog ate it – toxic GI dose) which they had stolen. Didn’t know if both or which dog had eaten it. Both had no seizures, vomiting or diarrhoea. Healthy otherwise.
CS: Dog 1 HR 104, Dog 2 HR 132. Rest of clinical exam as WNL Dog 2 was checked for oesophageal pain on palpation due to FB
and none was noted and no S/C emphysema. Suggested should radiograph to check for gas leaving oesophagus if FB caused a perforation
Treatment: Induce emesis with ½ tablet conjunctival apomorphine
Dog 2: V++ straight away, no chocolate but plastic sharp FB produced! Dog 1: No V, gave another ¼ tablet, waited 10 minutes: no V so gave 0.13mg
IV apomorphine: V++ immediately with lots of choclate. Once stopped V gave Metocloprimide to prevent further emesis.
Signalment: 11 month old ME German Shepard Dog History: No GDV history, on treatment for ear and skin problems. Was
fed at 8am then taken for a two hour run with ball. When came back had a drink and then lay away himself which is not normal. After one hour was salivating and not himself – taken to his own vets.
GP: painful abdomen, rads showed very dilated GDV. Referred. Cex: T 38.5, HR 132, pulses short, R 20, mm pink and CRT <2, normal
abdominal palpation (suspect may have untwisted as so stable) Warned owners that if had been GDV since 10am (now 3pm) may be too
much necrosis of stomach wall or spleen and of post op ileus. Diagnostics:
Repeat rads –Right lateral abdominal radiograph shows pylorus remains displaced dorsally. Distension of stomach has much reduced however.
Blood gas and Lytes: metabolic acidosis. Lactate 2.3(would expect higher if dilation was big and causing hypoperfusion), Hypercalcaemia: ionised Ca: 1.42
BP and ecg: showed no abnormalities before, during or after surgery
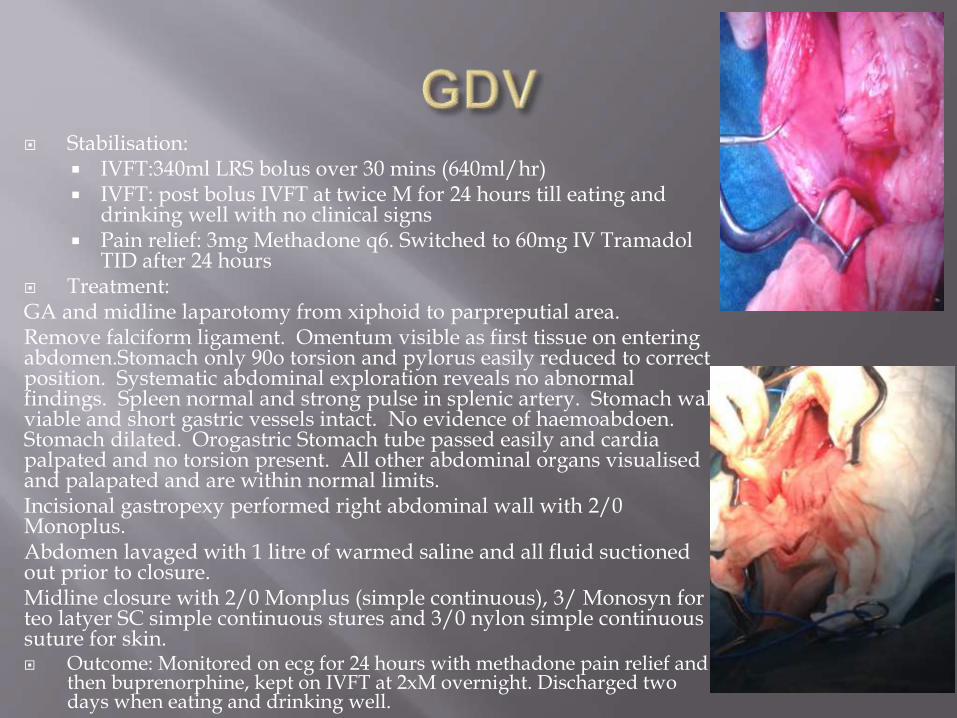
Stabilisation: IVFT:340ml LRS bolus over 30 mins (640ml/hr) IVFT: post bolus IVFT at twice M for 24 hours till eating and
drinking well with no clinical signs Pain relief: 3mg Methadone q6. Switched to 60mg IV Tramadol
TID after 24 hours Treatment:GA and midline laparotomy from xiphoid to parpreputial area.Remove falciform ligament. Omentum visible as first tissue on entering abdomen.Stomach only 90o torsion and pylorus easily reduced to correct position. Systematic abdominal exploration reveals no abnormal findings. Spleen normal and strong pulse in splenic artery. Stomach wall viable and short gastric vessels intact. No evidence of haemoabdoen. Stomach dilated. Orogastric Stomach tube passed easily and cardiapalpated and no torsion present. All other abdominal organs visualised and palapated and are within normal limits.Incisional gastropexy performed right abdominal wall with 2/0 Monoplus.Abdomen lavaged with 1 litre of warmed saline and all fluid suctioned out prior to closure.Midline closure with 2/0 Monplus (simple continuous), 3/ Monosyn for teo latyer SC simple continuous stures and 3/0 nylon simple continuous suture for skin. Outcome: Monitored on ecg for 24 hours with methadone pain relief and
then buprenorphine, kept on IVFT at 2xM overnight. Discharged two days when eating and drinking well.
Signalment: 13 year old FN spotted mist cat History: Diagnosed with Diabetes four months ago and been treated with 1IU of
Glargine BID until 2 weeks ago when increased to 4IU of Glargine BID as BG on dipsticks and curves have been consistently high. Owner reports been more lethargic recently. Owner returned home today and found cat curled up, unresponsive and to have urinated in bed so brought straight here. Most recent dipstick showed no glucouria
Cex: T 33.6, HR 220, R 12, mm pale pink, CRT 2S, pulses tall and narrow, minimally responsive, marked mydriasis, mucoid diarrhoea
Differentials: Diabetic remission or insulin overdose Diagnostics:
Glucometer BG 1.1mmol/l Electrolytes: glucose= 0.9mmol/l, sodium= 156 mmol/L, potassium= 3.4mmol/L, chloride 124
mmol/L
Stabilisation: IVC placed 0.5ml/kg IV 50%glucose given diluted in 10ml 0.9% Saline (responded very fast) Feed asap (ravenous) BG monitored every hour, dropped again 3 hours later to 2.6mmol/l so gave another 50% glucose
bolus IV (0.5ml/kg)
Outcome: Overnight if BG > 11 gave 1IU Glargine, if BG >15 gave 2IU Units Glargine, none if <11mmol/l Transferred to medicine and started on 2IU Glargine BID
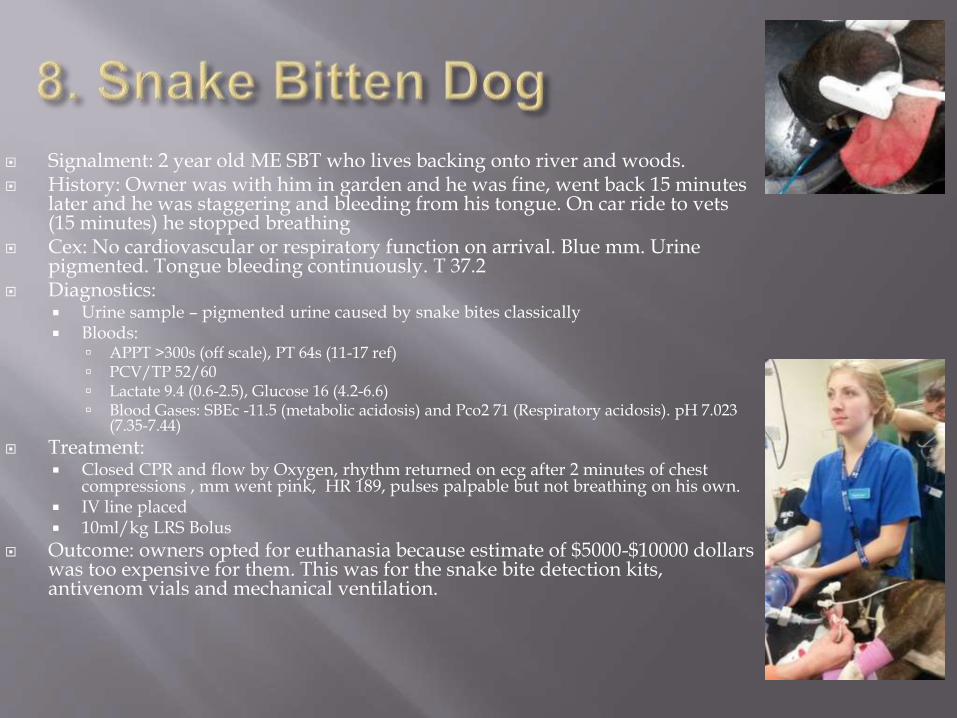
Signalment: 2 year old ME SBT who lives backing onto river and woods. History: Owner was with him in garden and he was fine, went back 15 minutes
later and he was staggering and bleeding from his tongue. On car ride to vets (15 minutes) he stopped breathing
Cex: No cardiovascular or respiratory function on arrival. Blue mm. Urine pigmented. Tongue bleeding continuously. T 37.2
Diagnostics: Urine sample – pigmented urine caused by snake bites classically Bloods:
APPT >300s (off scale), PT 64s (11-17 ref) PCV/TP 52/60 Lactate 9.4 (0.6-2.5), Glucose 16 (4.2-6.6) Blood Gases: SBEc -11.5 (metabolic acidosis) and Pco2 71 (Respiratory acidosis). pH 7.023
(7.35-7.44)
Treatment: Closed CPR and flow by Oxygen, rhythm returned on ecg after 2 minutes of chest
compressions , mm went pink, HR 189, pulses palpable but not breathing on his own. IV line placed 10ml/kg LRS Bolus
Outcome: owners opted for euthanasia because estimate of $5000-$10000 dollars was too expensive for them. This was for the snake bite detection kits, antivenom vials and mechanical ventilation.
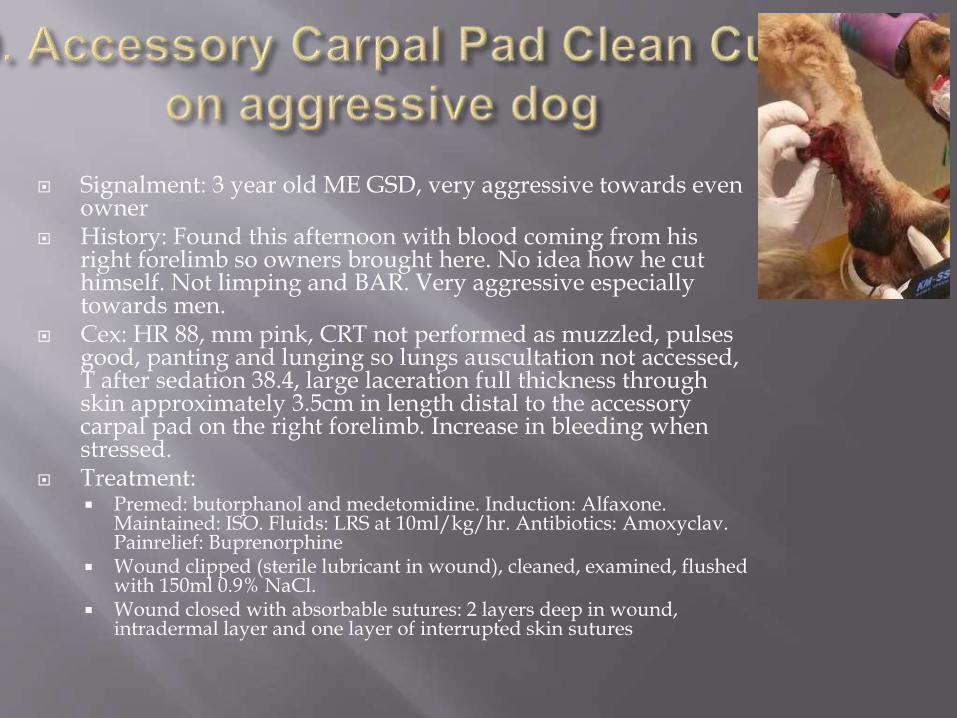
Signalment: 3 year old ME GSD, very aggressive towards even owner
History: Found this afternoon with blood coming from his right forelimb so owners brought here. No idea how he cut himself. Not limping and BAR. Very aggressive especially towards men.
Cex: HR 88, mm pink, CRT not performed as muzzled, pulses good, panting and lunging so lungs auscultation not accessed, T after sedation 38.4, large laceration full thickness through skin approximately 3.5cm in length distal to the accessory carpal pad on the right forelimb. Increase in bleeding when stressed.
Treatment: Premed: butorphanol and medetomidine. Induction: Alfaxone.
Maintained: ISO. Fluids: LRS at 10ml/kg/hr. Antibiotics: Amoxyclav. Painrelief: Buprenorphine
Wound clipped (sterile lubricant in wound), cleaned, examined, flushed with 150ml 0.9% NaCl.
Wound closed with absorbable sutures: 2 layers deep in wound, intradermal layer and one layer of interrupted skin sutures
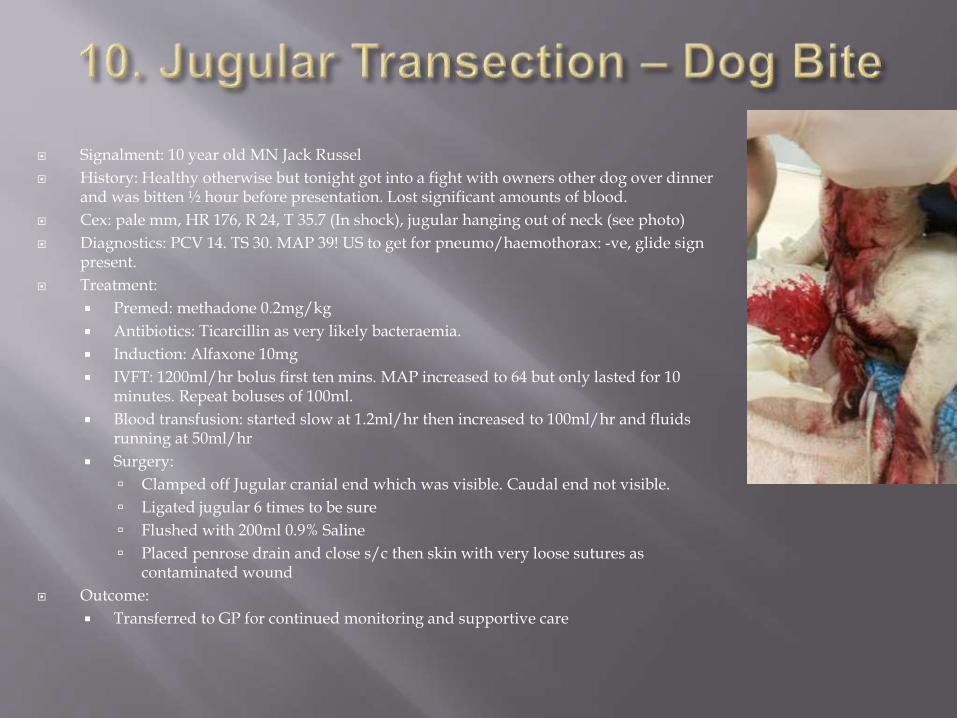
Signalment: 10 year old MN Jack Russel
History: Healthy otherwise but tonight got into a fight with owners other dog over dinner and was bitten ½ hour before presentation. Lost significant amounts of blood.
Cex: pale mm, HR 176, R 24, T 35.7 (In shock), jugular hanging out of neck (see photo)
Diagnostics: PCV 14. TS 30. MAP 39! US to get for pneumo/haemothorax: -ve, glide sign present.
Treatment:
Premed: methadone 0.2mg/kg
Antibiotics: Ticarcillin as very likely bacteraemia.
Induction: Alfaxone 10mg
IVFT: 1200ml/hr bolus first ten mins. MAP increased to 64 but only lasted for 10 minutes. Repeat boluses of 100ml.
Blood transfusion: started slow at 1.2ml/hr then increased to 100ml/hr and fluids running at 50ml/hr
Surgery:
Clamped off Jugular cranial end which was visible. Caudal end not visible.
Ligated jugular 6 times to be sure
Flushed with 200ml 0.9% Saline
Placed penrose drain and close s/c then skin with very loose sutures as contaminated wound
Outcome:
Transferred to GP for continued monitoring and supportive care
Signalment: 14 year old FN DSH History: owner returned from work to find her lying immobile with her pupils dilated.
She was bitten by a snake before and showed the same signs so owners brought her straight to the ECC.
Cex: collapsed, HR 204 - intermittent gallop sounds mm pink, CRT 1.5s, T36.9, R 32 -Paradoxical abdominal movement, non ambulatory tetraparesis, alert but LMN weakness causing minimal responsiveness, bilateral mydriasis, absent PLR.
Diagnostics: Urine: pigmented and on Snake detection kit strong positive (blue) for tiger envenomation Bloods:
PCV/TP 38/74 Blood gas & Lyes:
Treatment: Premed: chloramphenimine 2 vials of tiger/brown antivenom (diluted in 40ml 0.9% saline IV) Methadone 0.8mg IV q4hr Lacrilube eyes q2hr
Outcome: Treated in ICU for 4 days as developed colitis and did not eat for 4 days - had an O tube placed. Case still active when we left
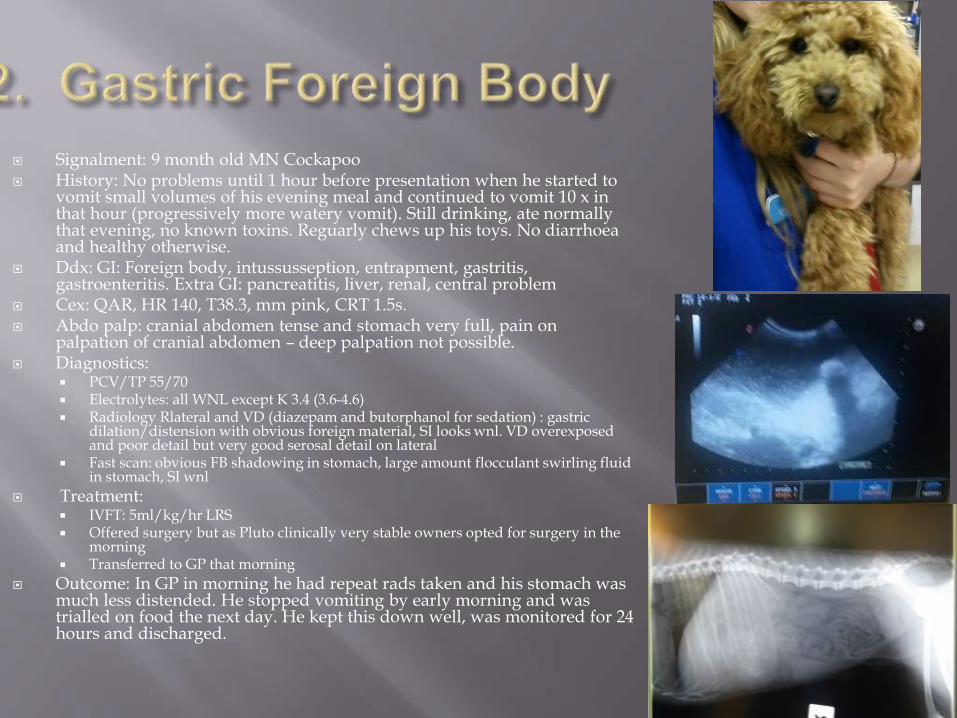
Signalment: 9 month old MN Cockapoo History: No problems until 1 hour before presentation when he started to
vomit small volumes of his evening meal and continued to vomit 10 x in that hour (progressively more watery vomit). Still drinking, ate normally that evening, no known toxins. Reguarly chews up his toys. No diarrhoea and healthy otherwise.
Ddx: GI: Foreign body, intussusseption, entrapment, gastritis, gastroenteritis. Extra GI: pancreatitis, liver, renal, central problem
Cex: QAR, HR 140, T38.3, mm pink, CRT 1.5s. Abdo palp: cranial abdomen tense and stomach very full, pain on
palpation of cranial abdomen – deep palpation not possible. Diagnostics:
PCV/TP 55/70 Electrolytes: all WNL except K 3.4 (3.6-4.6) Radiology Rlateral and VD (diazepam and butorphanol for sedation) : gastric
dilation/distension with obvious foreign material, SI looks wnl. VD overexposed and poor detail but very good serosal detail on lateral
Fast scan: obvious FB shadowing in stomach, large amount flocculant swirling fluid in stomach, SI wnl
Treatment: IVFT: 5ml/kg/hr LRS Offered surgery but as Pluto clinically very stable owners opted for surgery in the
morning Transferred to GP that morning
Outcome: In GP in morning he had repeat rads taken and his stomach was much less distended. He stopped vomiting by early morning and was trialled on food the next day. He kept this down well, was monitored for 24 hours and discharged.
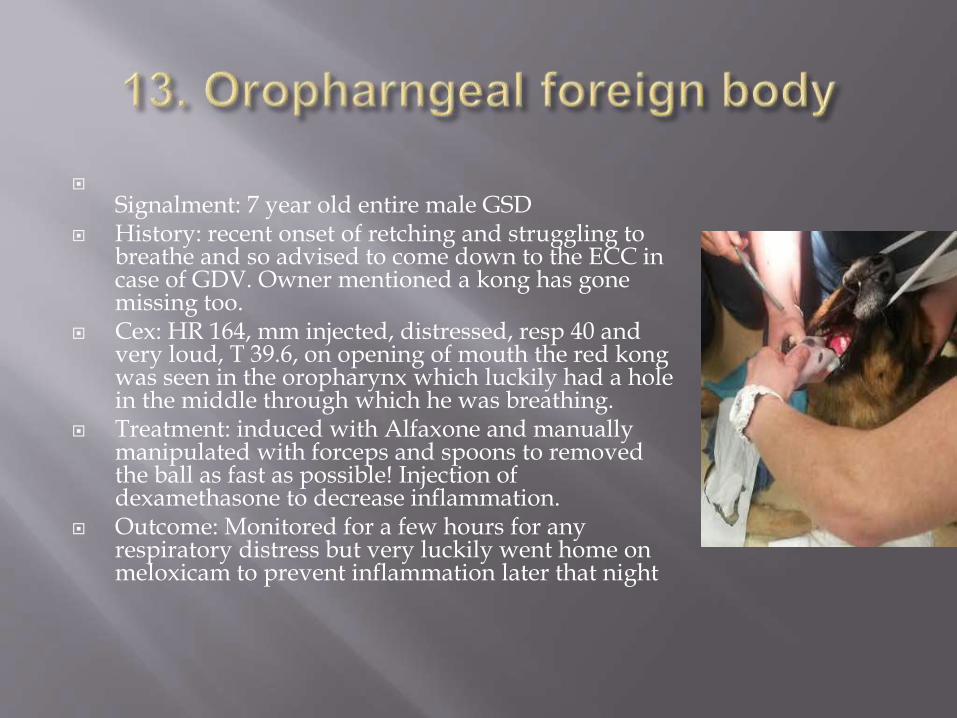
Signalment: 7 year old entire male GSD History: recent onset of retching and struggling to
breathe and so advised to come down to the ECC in case of GDV. Owner mentioned a kong has gone missing too.
Cex: HR 164, mm injected, distressed, resp 40 and very loud, T 39.6, on opening of mouth the red kongwas seen in the oropharynx which luckily had a hole in the middle through which he was breathing.
Treatment: induced with Alfaxone and manually manipulated with forceps and spoons to removed the ball as fast as possible! Injection of dexamethasone to decrease inflammation.
Outcome: Monitored for a few hours for any respiratory distress but very luckily went home on meloxicam to prevent inflammation later that night
Signalment: 7 year odl MN Cocker History: Travelled to NSW one month ago in a campervan which he now plays in in
the back garden. Owner noticed a tick on his Left eye last night and removed it asap. He did not show any signs of being ill until the owner returned from work the following afternoon and heard immediately that his bark had changed and he was weak in his hind limbs. He was coughing and out of breath when excited. His eye was also swollen where the tick was and dropping. She took him straight to the vets who referred him to ECC. Owner brought tick to ECC.
Cex: HR 140, Pink mm, CRT 1s, pulses normal, T 38.4, Resp: panting and coughing, choaking occasionally, left eye dropping and unable to blink.
Diagnostics: Examined tick and confirmed its middle legs were lighter than the caudal and
cranial legs and the legs were all cranial on the tick – Ixodes Holocyclus(Australian Paralysis tick)
BP: 181/133 Blood gas: all WNL, PCV/TP: 46/66 Full body clip and tick search – including orifices Ecg monitored constantly
Treatment : 1ml/kg tick antiserum given slowly over ½ hour by syringe driver. Full body tick bath with pyrethrin shampoo
Outcome: recovered well and went home the next day when breathing returned to normal
Signalment: 13 year old FE SBT History: in past 5 hours has ingested an unknown amount of Snail Bait. The owners
other dog also ingested snail bait and was at another vets having seizures. The ref vets had suggested to the owner to give soda crystals (1 or 2) to the owners dog to make it vomit but he had given two full handfuls. After the first handful the dog had vomited up a lot of metaldehyde and he gave another handful. This handful had not caused much vomiting so it was presumed there was around a handful of soda crystals still in the dogs stomach (given 1 hour ago).
Cex: Muscle trembling but T 38.7, HR 180, mm injected, CRT 1s, pulses short and narrow, panting. Able to stand but falling into sternal.
Diag: Fast Scan: no abdominal FF so hopeful soda crystals had not yet perforated the stomach. Bloods: PCV/TP 50/75, all electrolytes and blood gas WNL
Treatments: Induce emesis: Apomorphine IV and subcut – two doses given and no V+ produced Metoclopramide and Ondansatron to prevent emesis for induction (after 40 mins) Gastric Lavage: Induced with Alfaxone, maintained on iso. Produced small amount of blue-green
tinged liquid Enema x2: large amount of thick blue-green paste like material consistant with metaldehyde and
some blood flakes Giafen small amount given to stop muscles tremors Metronidazole to prevent GIT infection Plan to start charcoal in am
Signalment: 7 week old minlop, 0.78kg Hx: owner noticed today when he went to spray water over
the rabbits to cool them down that when all the rabbits scattered this one did not move. All of the rabbits are kept in a shaded aviary in the back garden, they were seperatedfrom their dam 4 days previous to presentation. They are fed pellets and hay but owner not sure how much this rabbit would have had as they are all together.
Cex: HR 280, T 38.9, R 176, CRT <1, mm pink, Pulses strong, GIT: no sounds heard on auscultation but faecal pellets palpable, head tilt and very floppy
Diagnostics: BG 9.1mmol/l Dx: Presumed floppy bunny syndrome Tx:
Subcut 40ml 0.9% NaCl Panacur: 20mg/kg Meloxicam: 5kg mark Critical care mix 5ml syringed every 2 hours Owners offered to bring rabbit in for hospital care but declined
Outcome: Owners returned 2 hours later with rabbit unable to get it to eat and PTS