Embed Size (px)
Citation preview
BREAST CANCERBREAST CANCER
March. 22. 2015March. 22. 2015
Breast Carcinoma Statistics• One in eight women will get
breast cancer,
• one third of women with breast cancer will die of the disease.
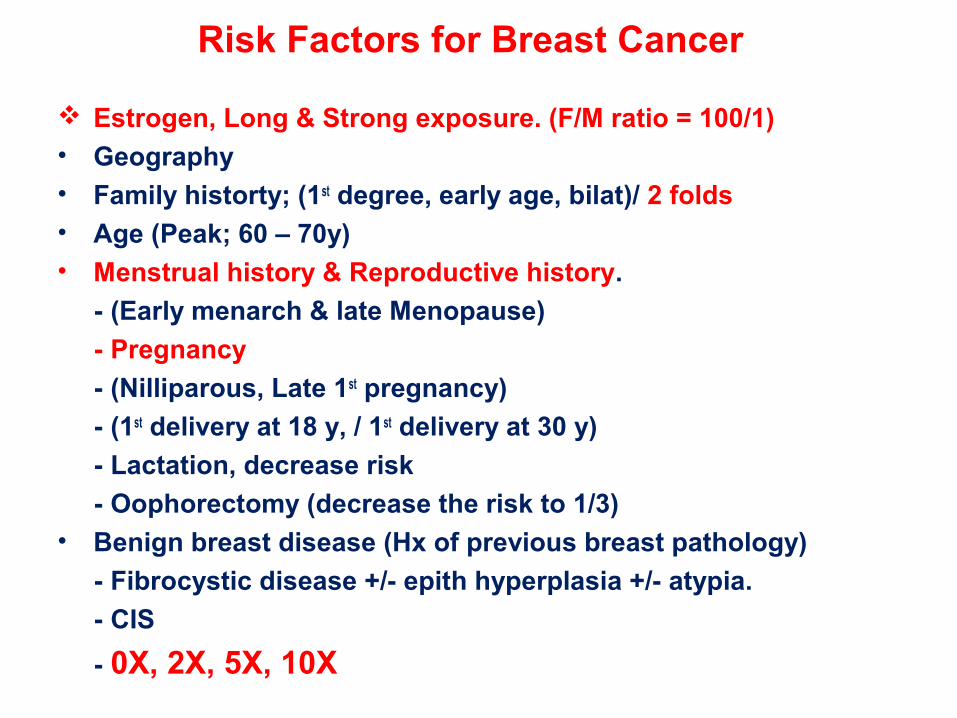
Risk Factors for Breast Cancer
Estrogen, Long & Strong exposure. (F/M ratio = 100/1)• Geography• Family historty; (1st degree, early age, bilat)/ 2 folds • Age (Peak; 60 – 70y)• Menstrual history & Reproductive history.
- (Early menarch & late Menopause)
- Pregnancy
- (Nilliparous, Late 1st pregnancy)
- (1st delivery at 18 y, / 1st delivery at 30 y)
- Lactation, decrease risk
- Oophorectomy (decrease the risk to 1/3) • Benign breast disease (Hx of previous breast pathology)
- Fibrocystic disease +/- epith hyperplasia +/- atypia.
- CIS
- 0X, 2X, 5X, 10X
Risk Factors for Breast Cancer
• Estrogen (exogenous), increase risk to 2.5 folds In 2002 Estrogen declared as carcinogen by National
Toxicology Program.• Oral contraceptive• Radiation Exposure • Carcinoma of the contralateral breast or endometrium • Obesity• High fat diet• Alcohol• Smoking• Environmental Toxins• Breast augmentation. • ABORTIONS?
Causes of Breast Cancer
• Genetic
• Environmental
• Hormonal
Breast Cancer Pathology
Ductal Ca. (85 – 93%)Lobular Ca. (7 – 15%)
In Situ Carcinomas (CIS) (15 )
Invasive Carcinomas (85%)
Special Subtypes (> 5%)
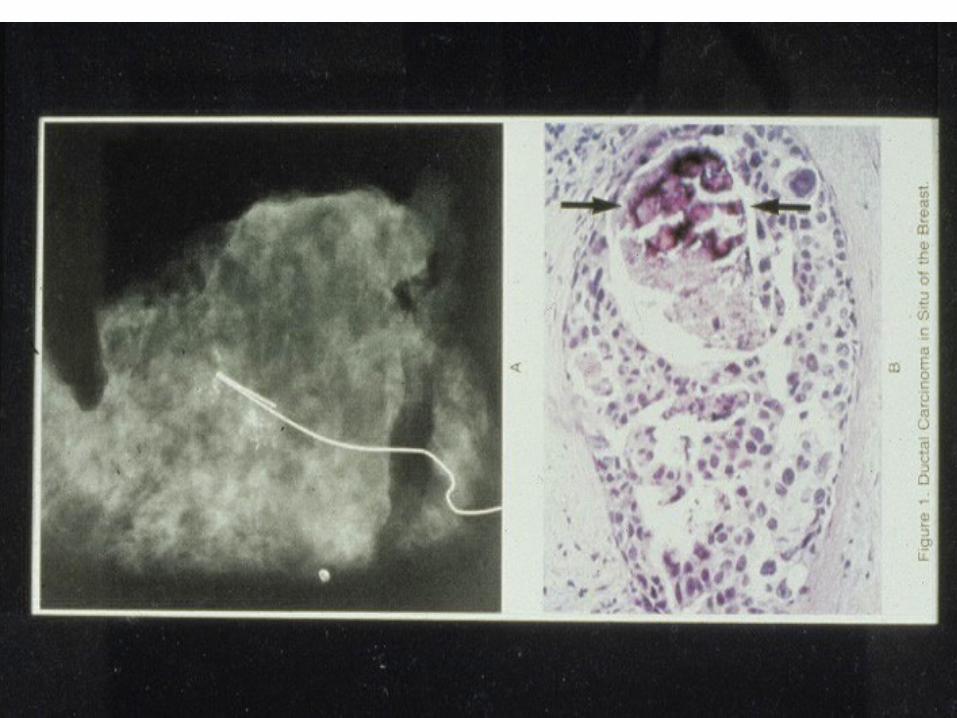
Ductal Carcinoma in Situ
• Clinical:– DCIS usually does not present as a palpable
mass, if it does it is usually high grade and a large lesion
• Mammogram:– The most common method of detection is by
identifying calcifications
• MRI
• FNA
• Biopsy
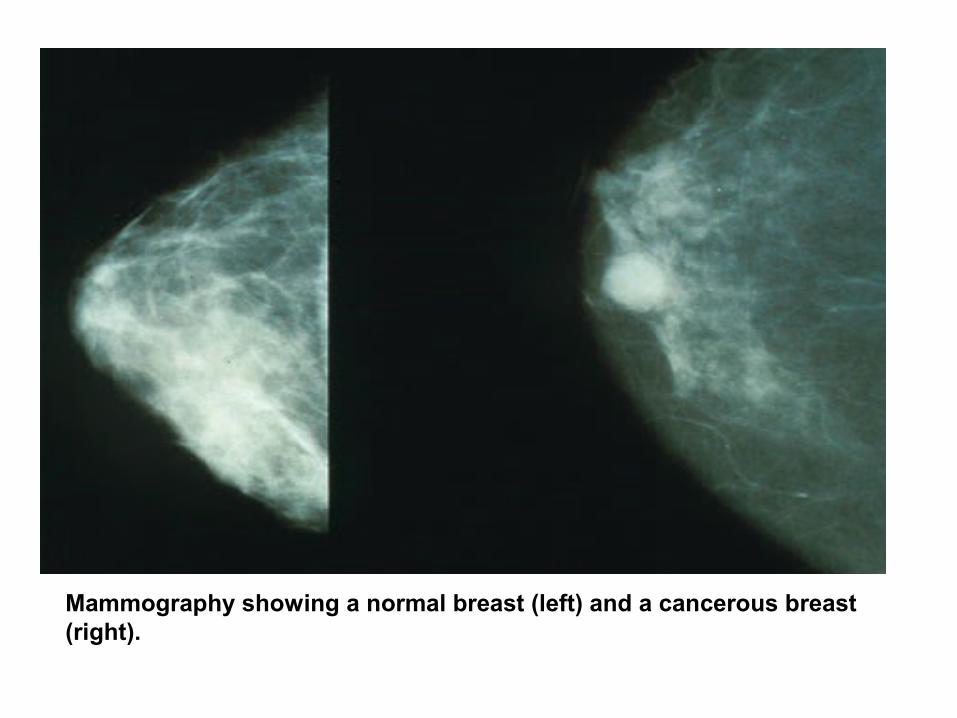
Mammography showing a normal breast (left) and a cancerous breast (right).
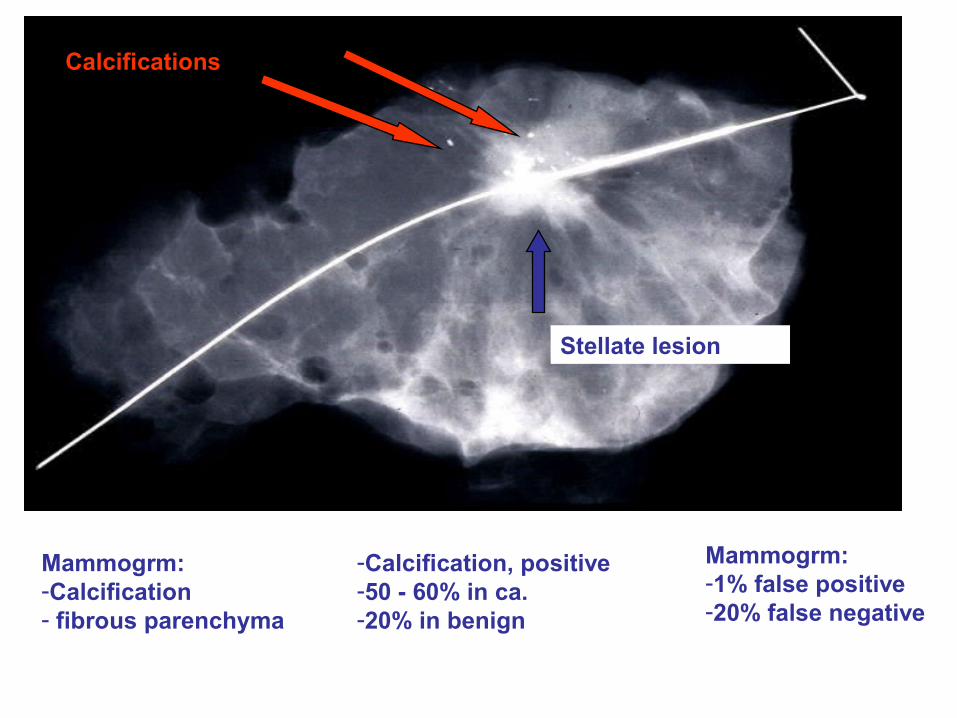
Stellate lesion
Calcifications
Mammogrm:-Calcification- fibrous parenchyma
Mammogrm:-1% false positive-20% false negative
-Calcification, positive -50 - 60% in ca.-20% in benign
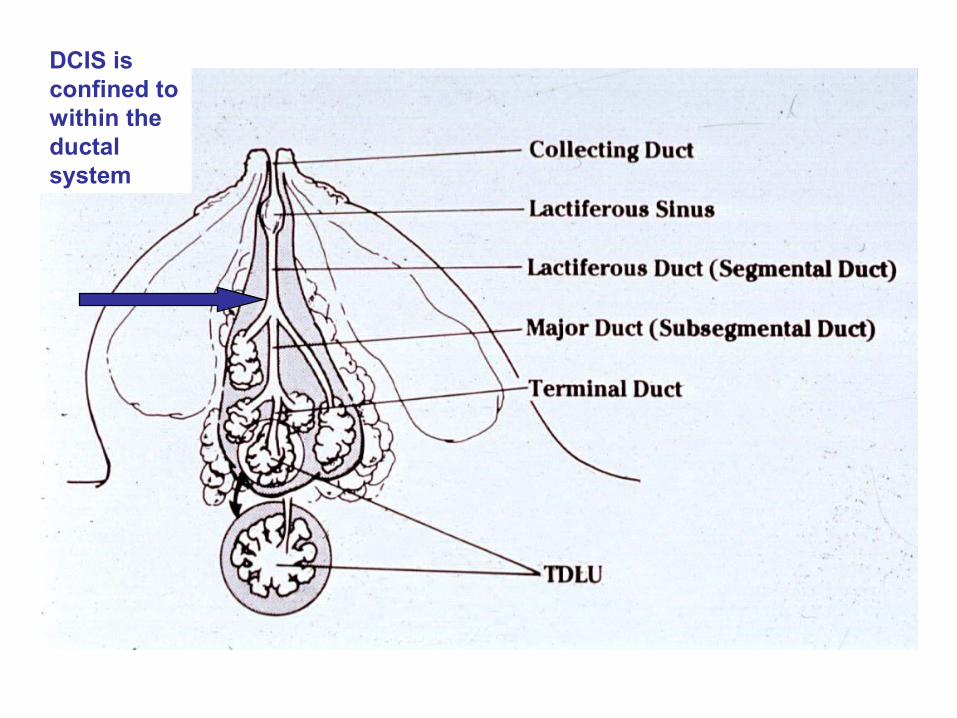
DCIS is confined to within the ductal system
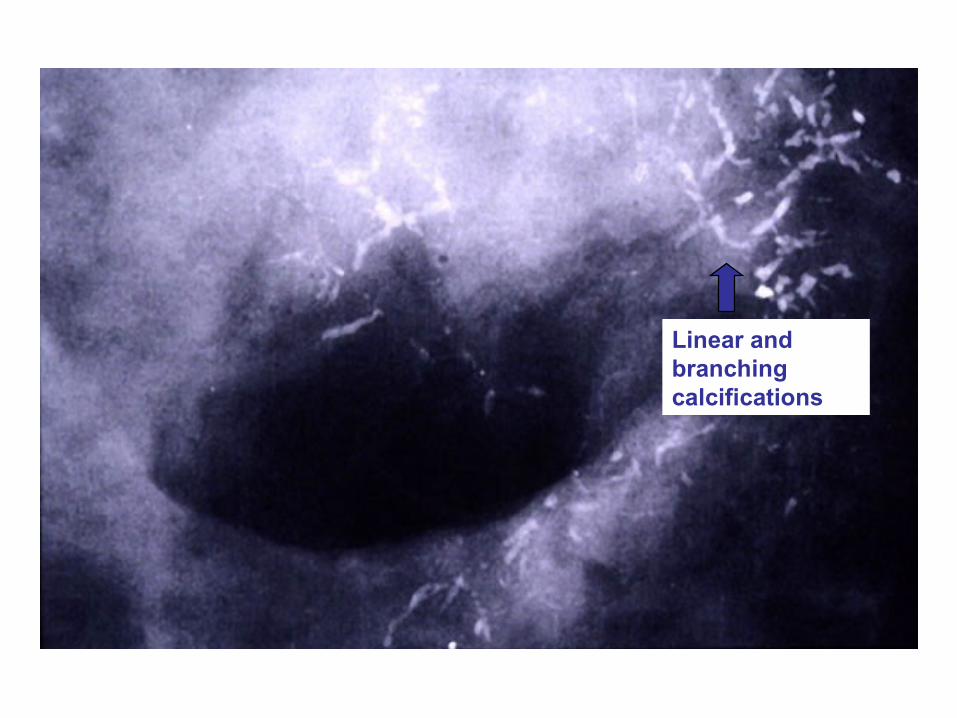
Linear and branching calcifications
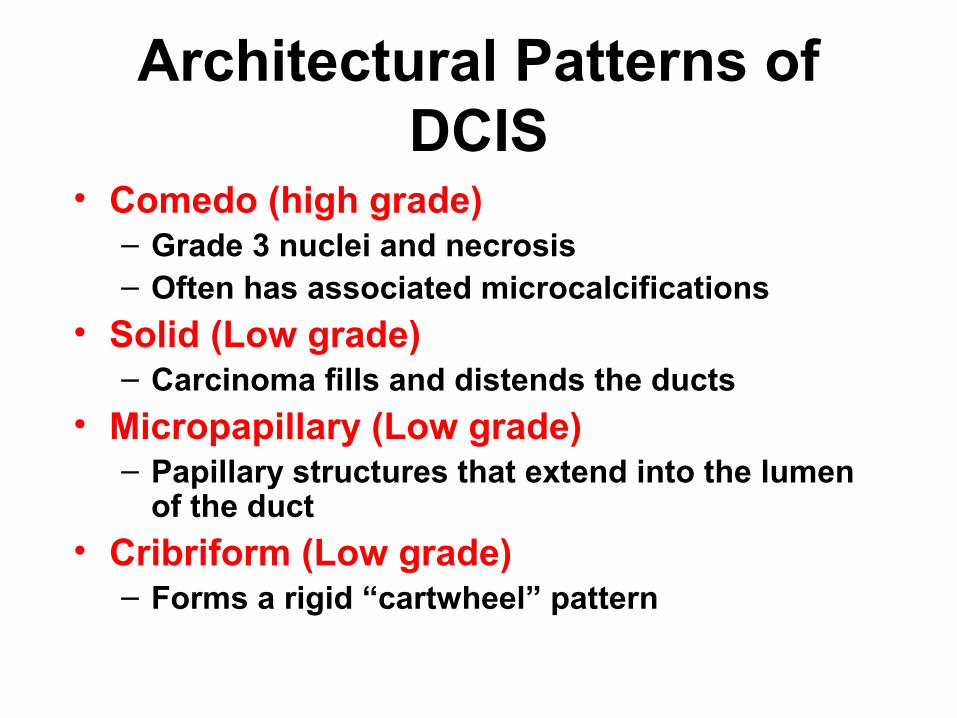
Architectural Patterns of DCIS
• Comedo (high grade)– Grade 3 nuclei and necrosis– Often has associated microcalcifications
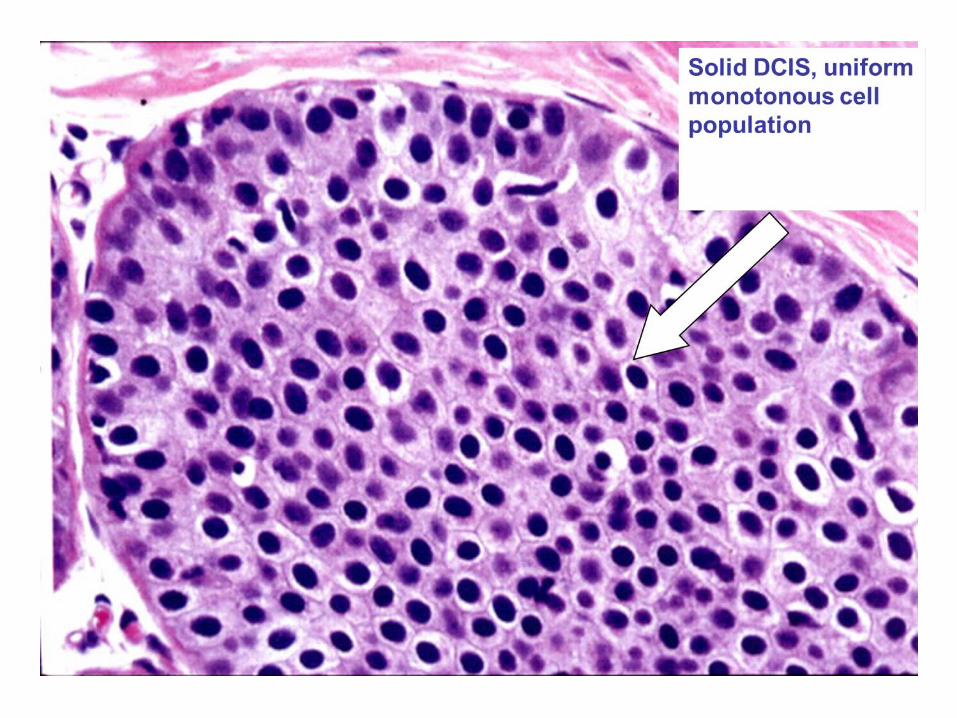
• Solid (Low grade)– Carcinoma fills and distends the ducts
• Micropapillary (Low grade)– Papillary structures that extend into the lumen
of the duct
• Cribriform (Low grade)– Forms a rigid “cartwheel” pattern
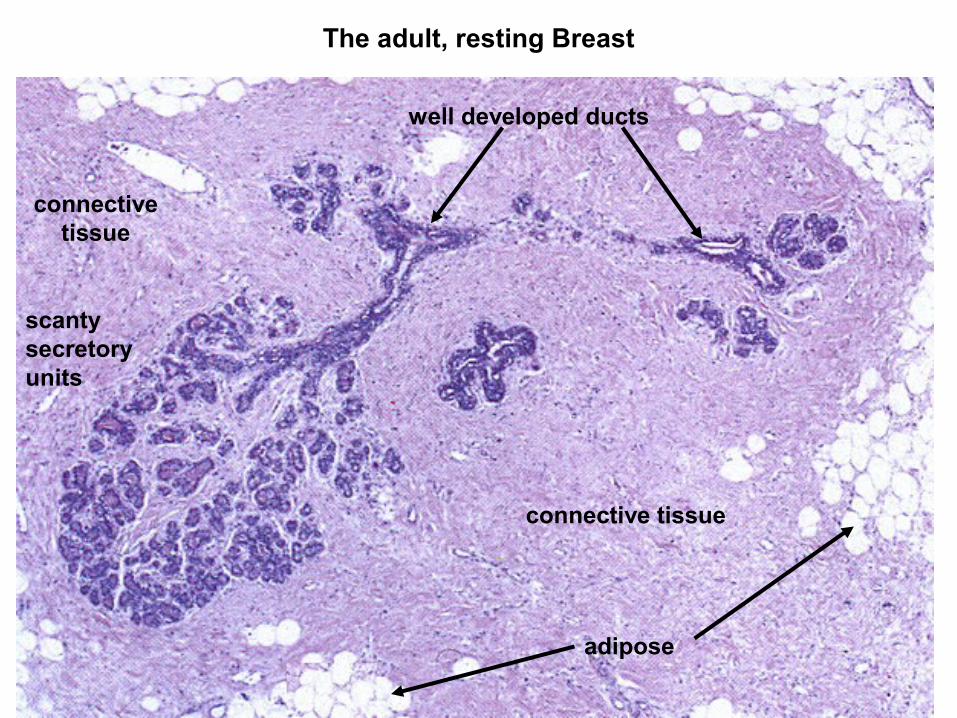
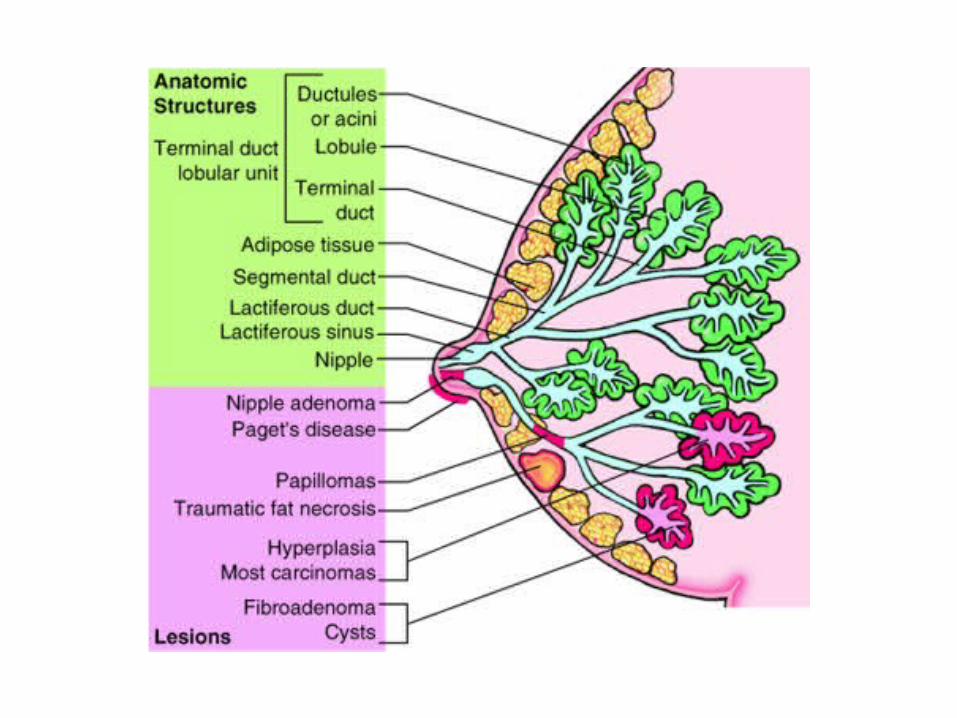
The adult, resting Breast
connective tissue
adipose
well developed ducts
connective tissue
scanty secretory units
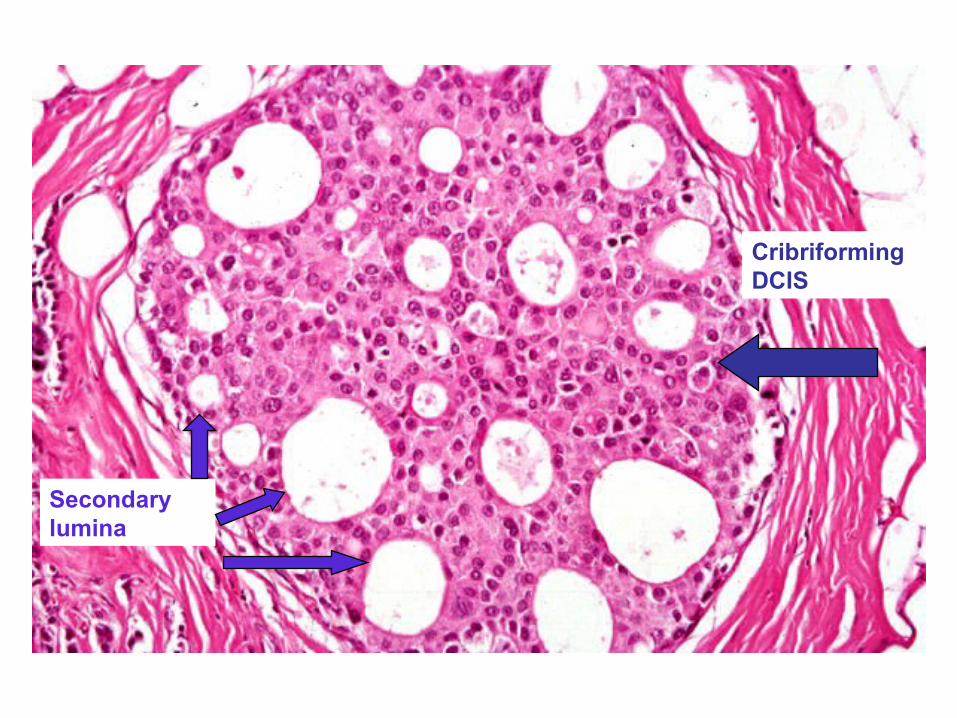
Cribriforming DCIS
Secondary lumina
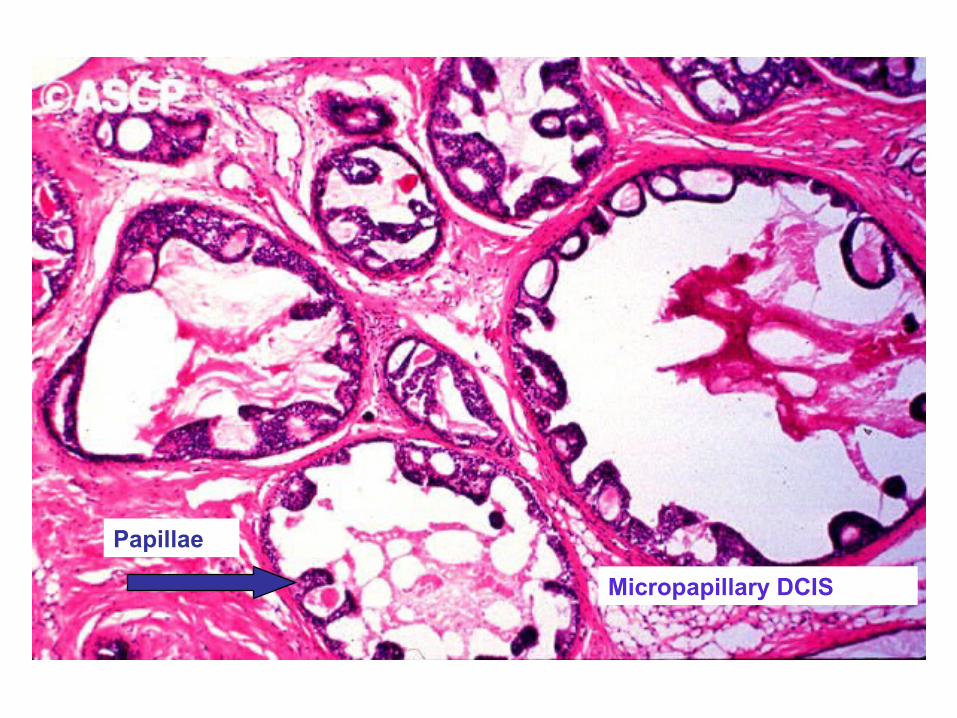
Micropapillary DCIS
Papillae
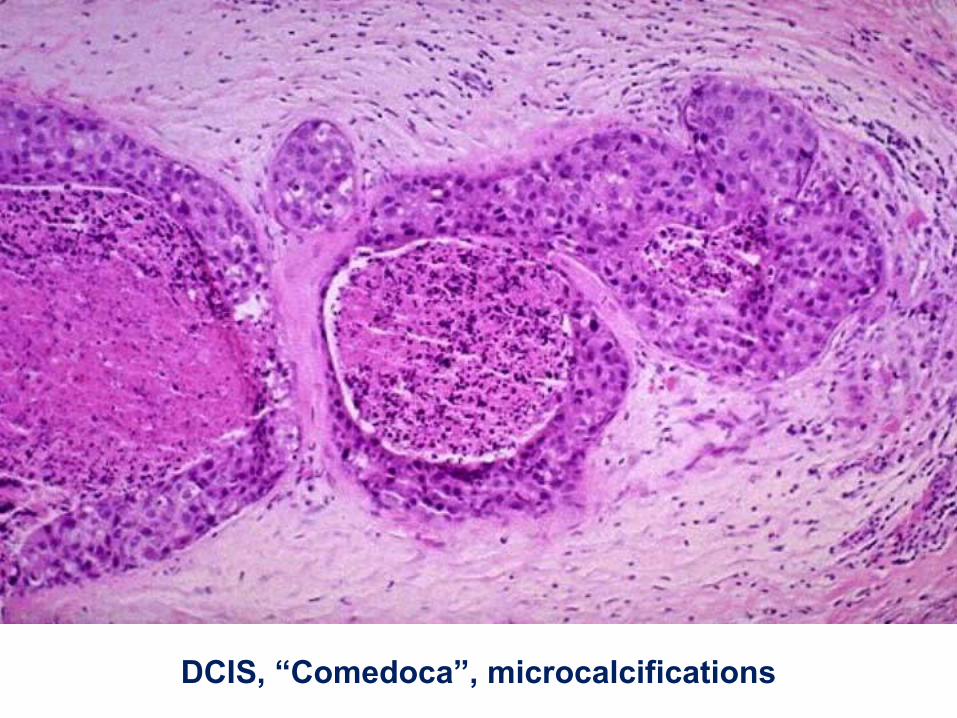
DCIS, “Comedoca”, microcalcifications
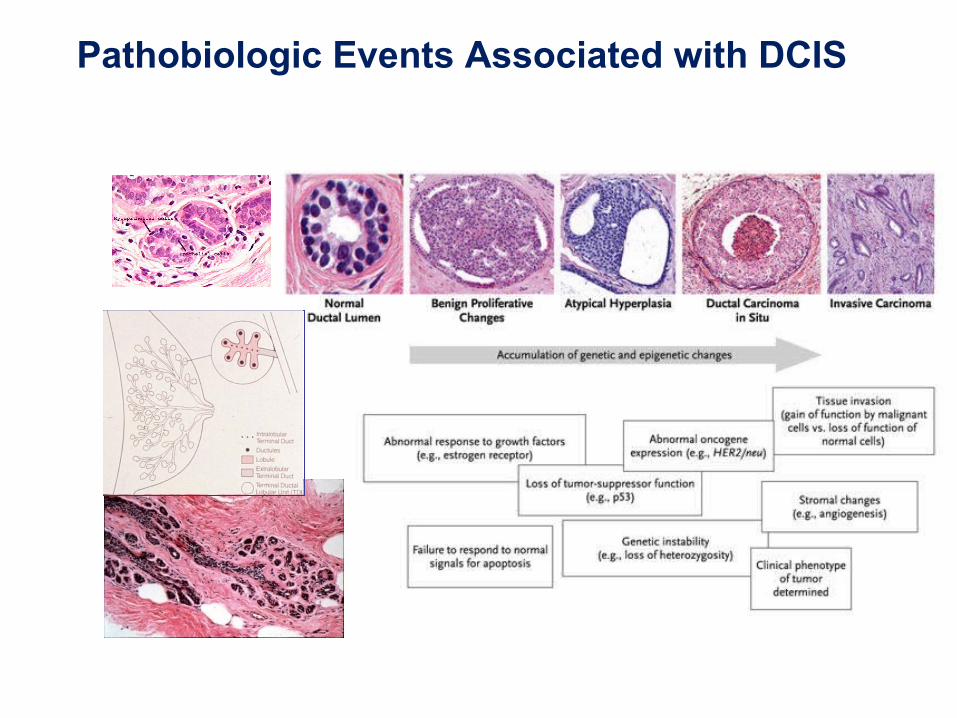
Pathobiologic Events Associated with DCIS
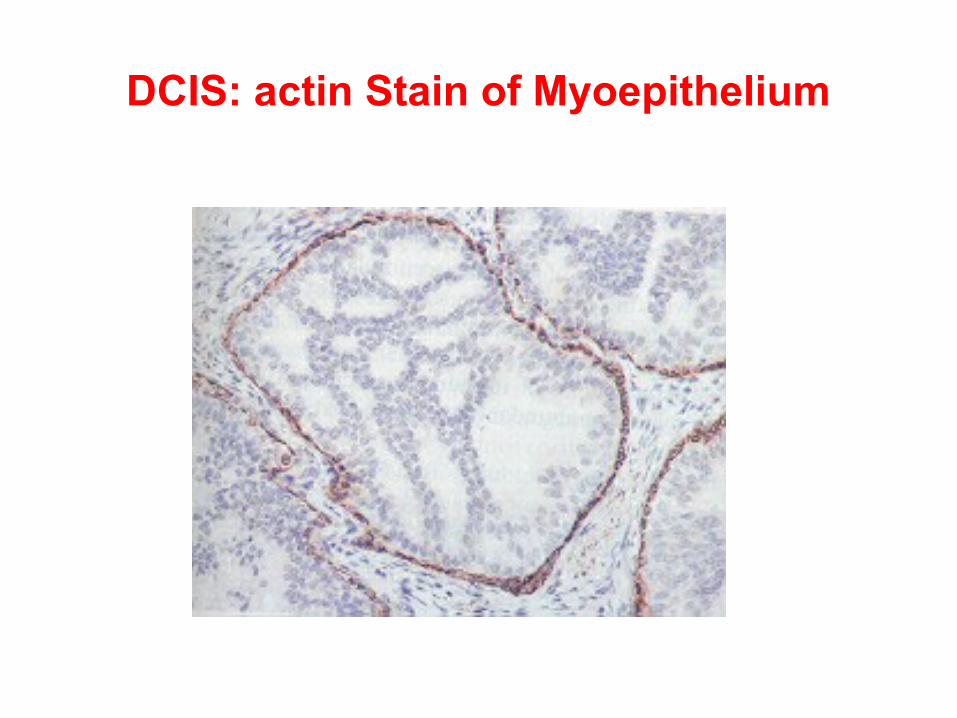
DCIS: actin Stain of Myoepithelium
Natural History
• 5 Year survival = 100% < 50 or > 50 year• If untreated ;
– 28% developed invasive cancer– 10 fold increase in RR to controls
Axillary lymph nodes
• Axillary LN involvement is <1%• Axillary LN dissection is not recommended• Sentinel lymph node biopsy?
– Not recommended.– Consider: extensive high grade DCIS or
palpable mass (increased chance of invasive disease being found)
• Mammography is the standard for detection of DCIS.
• MRI could help especially in high-grade DCIS
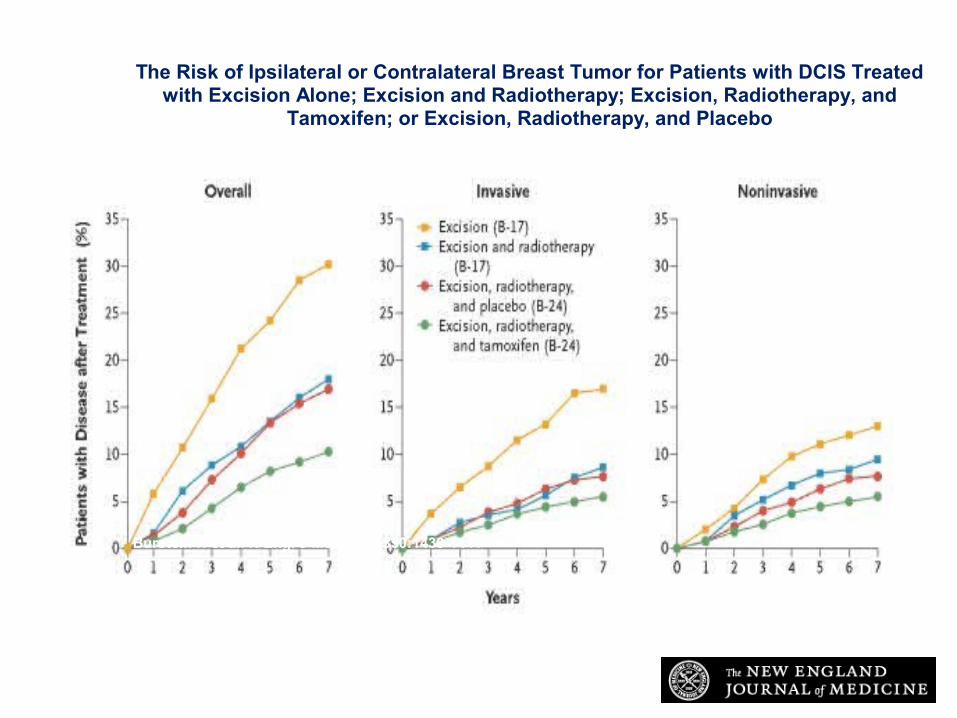
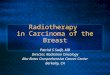
Burstein H et al. N Engl J Med 2004;350:1430-1441
The Risk of Ipsilateral or Contralateral Breast Tumor for Patients with DCIS Treated with Excision Alone; Excision and Radiotherapy; Excision, Radiotherapy, and
Tamoxifen; or Excision, Radiotherapy, and Placebo
Lobular Carcinoma in Situ (LCIS)
• Multicentric , Bilateral• Proliferation of neoplastic population of
cells within the TDLU • may extend into adjacent ducts.
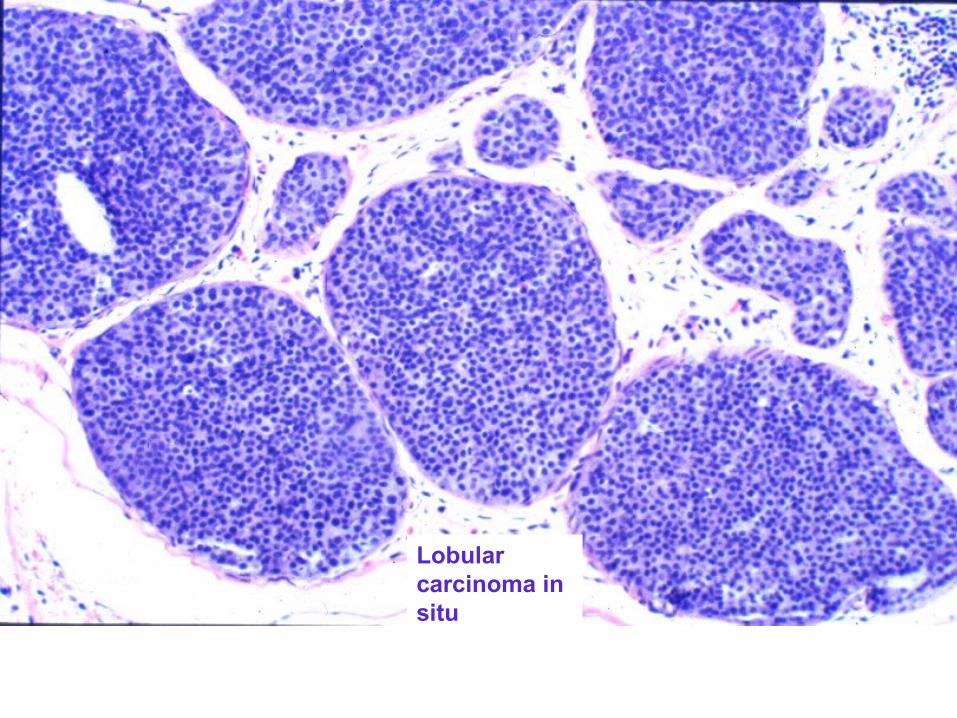
Lobular carcinoma in situ
Invasive (Infiltrating) Breast Carcinoma
Main histological types;• Invasive ductal ca.(85%)• Invasive lobular ca. (7 – 15%)
• Medullary ca. (2%)
• Mucoid ca. (2%)• Tubular ca. (2%)
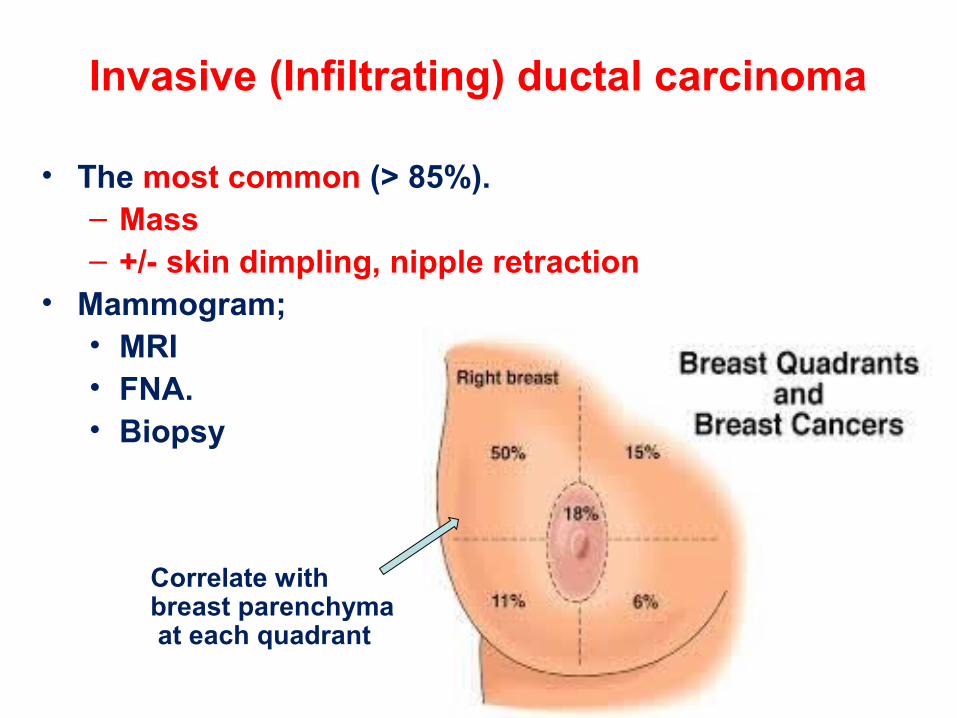
Invasive (Infiltrating) ductal carcinoma
• The most common (> 85%).– Mass– +/- skin dimpling, nipple retraction
• Mammogram; • MRI • FNA.• Biopsy
Correlate with breast parenchyma at each quadrant
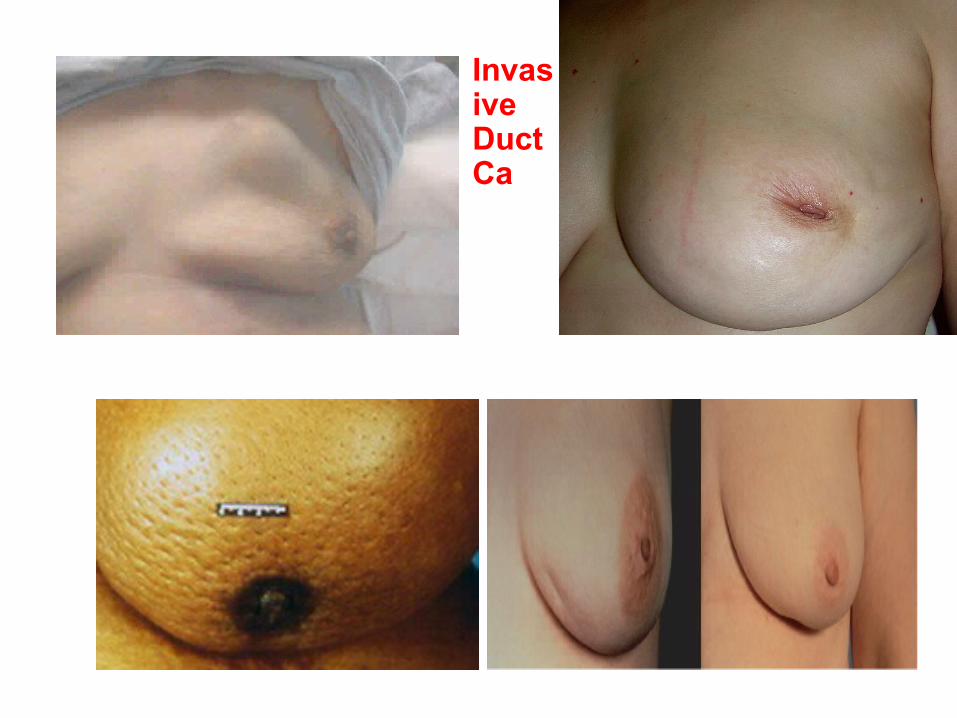
Invasive Duct Ca

Stellate lesion
Calcifications
Mammogrm:-Calcification- fibrous parenchyma
Mammogrm:-1% false positive-20% false negative
-Calcification, positive -50 - 60% in ca.-20% in benign
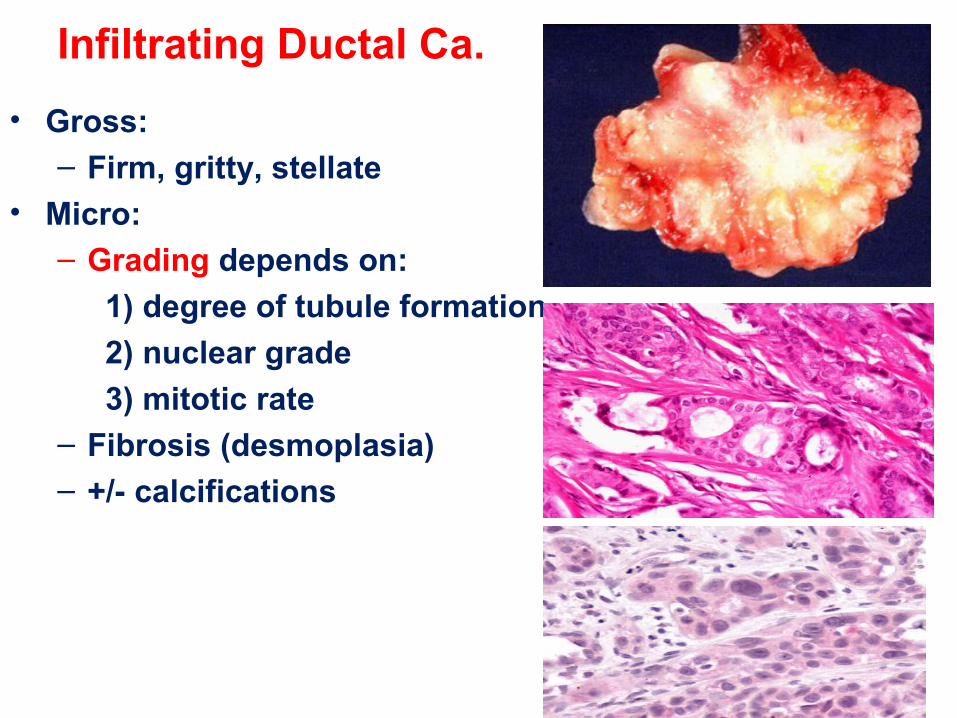
Infiltrating Ductal Ca.
• Gross:– Firm, gritty, stellate
• Micro:– Grading depends on:
1) degree of tubule formation
2) nuclear grade
3) mitotic rate– Fibrosis (desmoplasia)– +/- calcifications
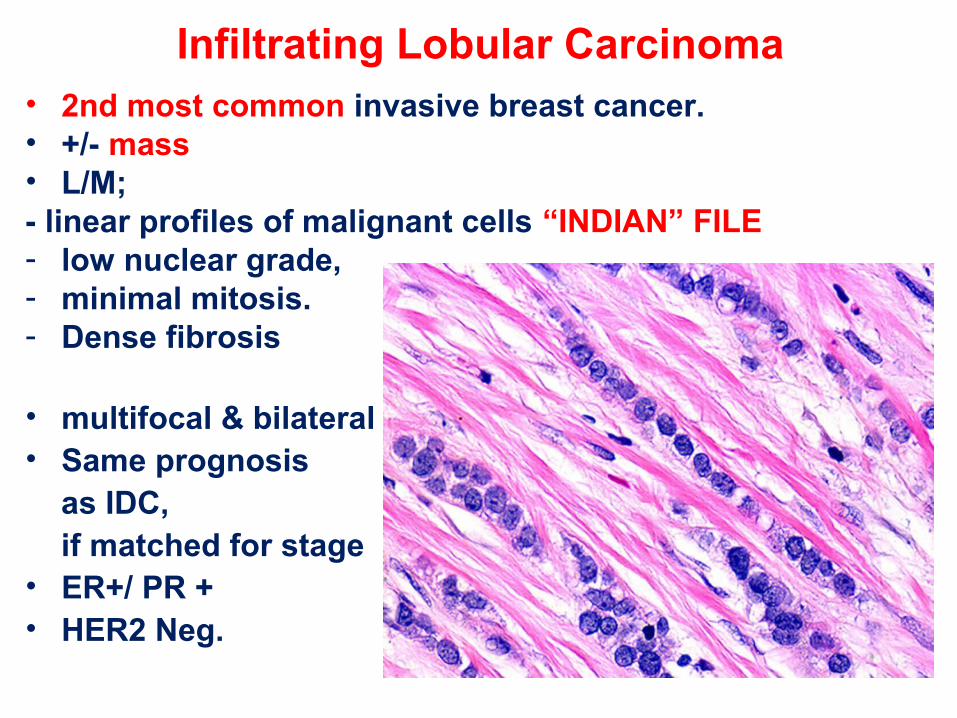
Infiltrating Lobular Carcinoma • 2nd most common invasive breast cancer.• +/- mass• L/M; - linear profiles of malignant cells “INDIAN” FILE- low nuclear grade, - minimal mitosis.- Dense fibrosis
• multifocal & bilateral• Same prognosis as IDC, if matched for stage• ER+/ PR +• HER2 Neg.
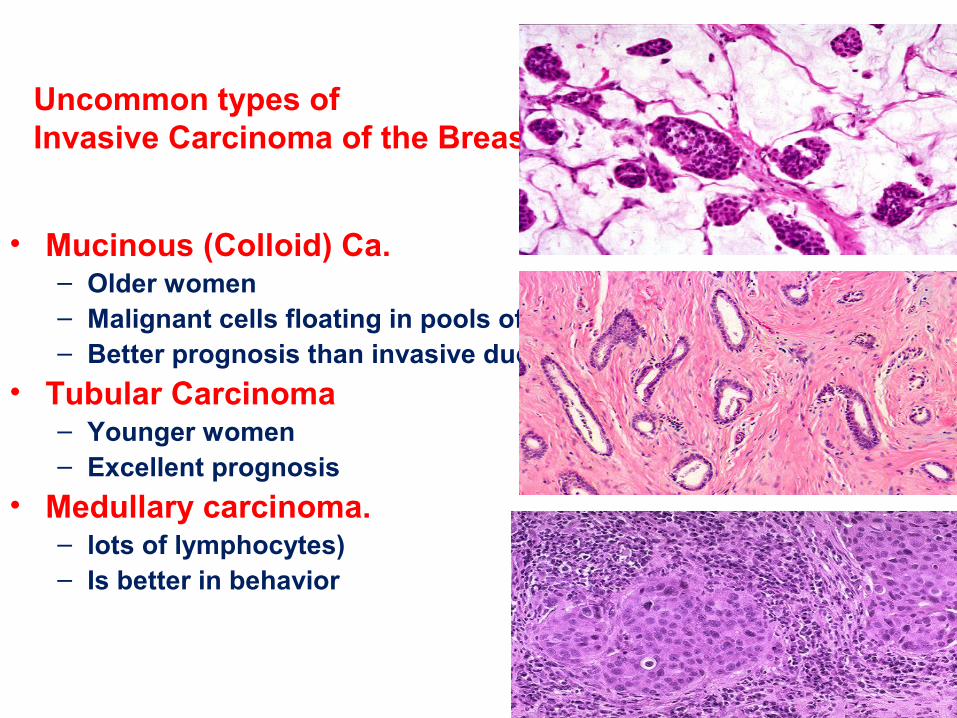
Uncommon types of Invasive Carcinoma of the Breast
• Mucinous (Colloid) Ca.– Older women– Malignant cells floating in pools of mucin– Better prognosis than invasive ductal or lobular
• Tubular Carcinoma– Younger women– Excellent prognosis
• Medullary carcinoma.– lots of lymphocytes) – Is better in behavior
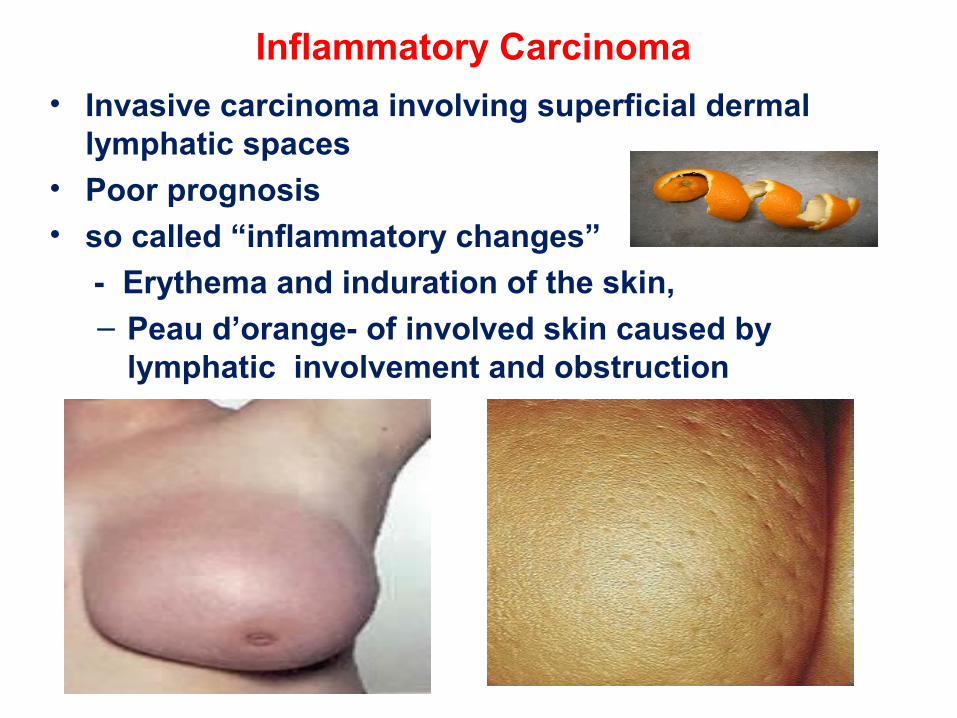
Inflammatory Carcinoma
• Invasive carcinoma involving superficial dermal lymphatic spaces
• Poor prognosis• so called “inflammatory changes”
- Erythema and induration of the skin,
– Peau d’orange- of involved skin caused by lymphatic involvement and obstruction
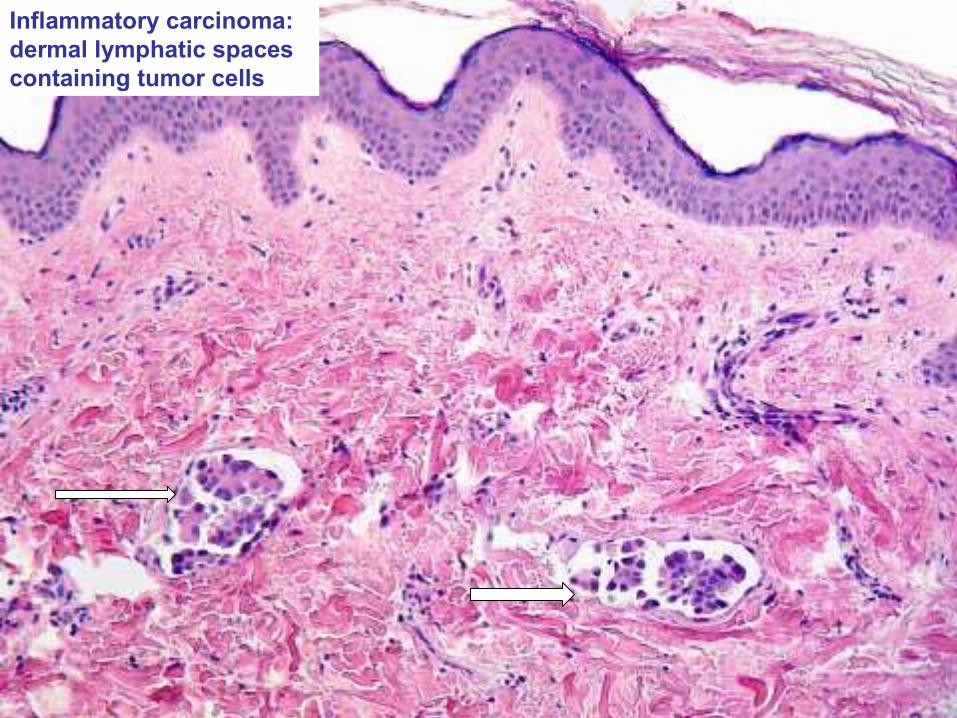
Inflammatory carcinoma: dermal lymphatic spaces containing tumor cells
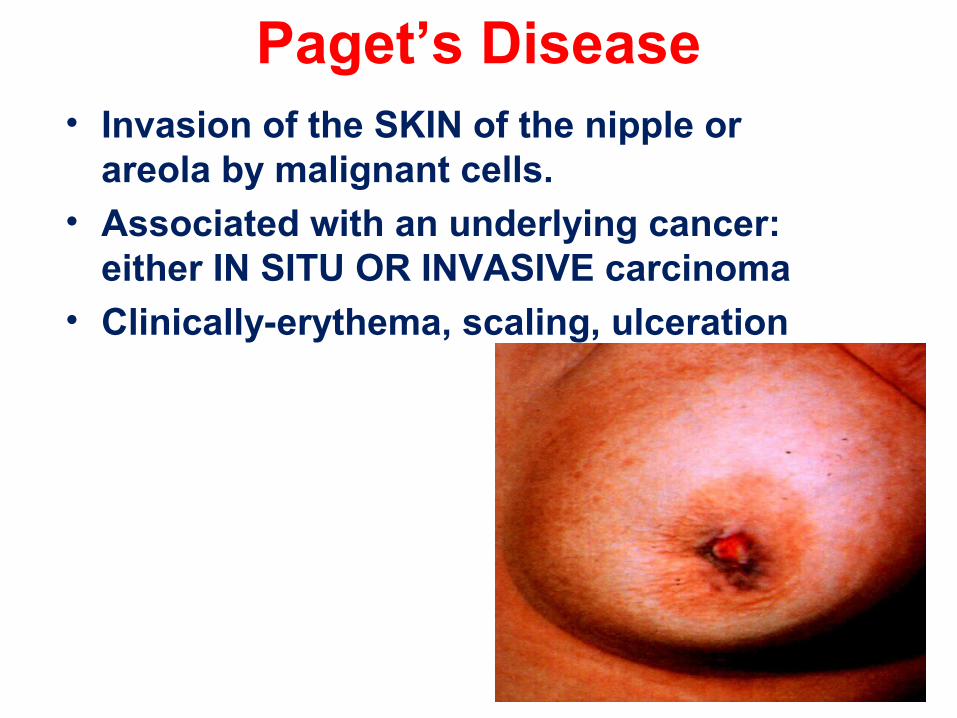
Paget’s Disease• Invasion of the SKIN of the nipple or
areola by malignant cells.• Associated with an underlying cancer:
either IN SITU OR INVASIVE carcinoma• Clinically-erythema, scaling, ulceration
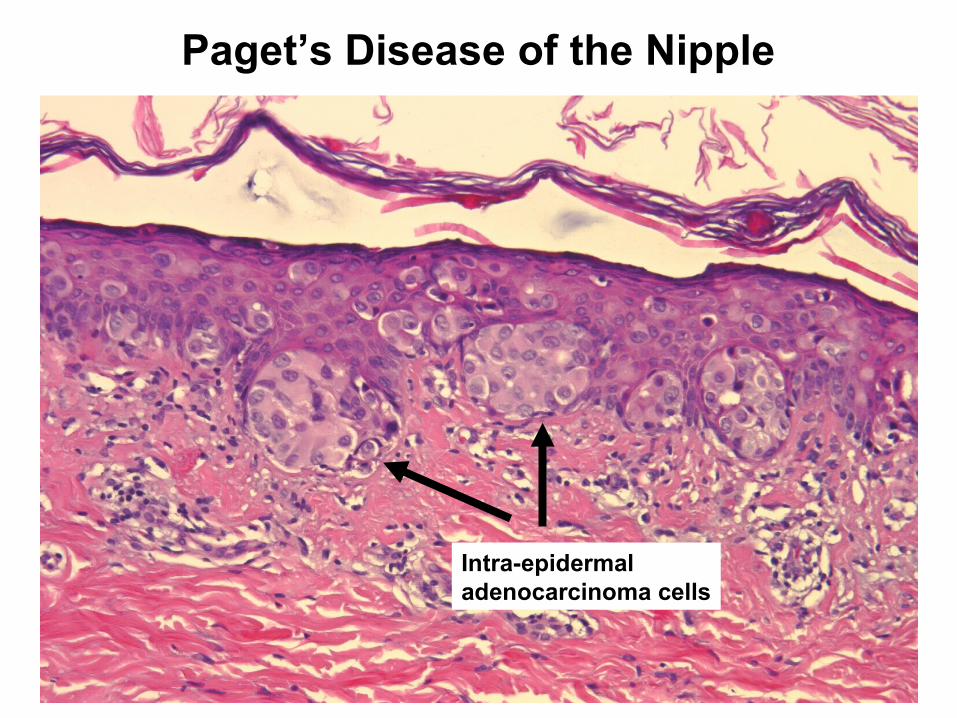
Paget’s Disease of the Nipple
Intra-epidermal adenocarcinoma cells
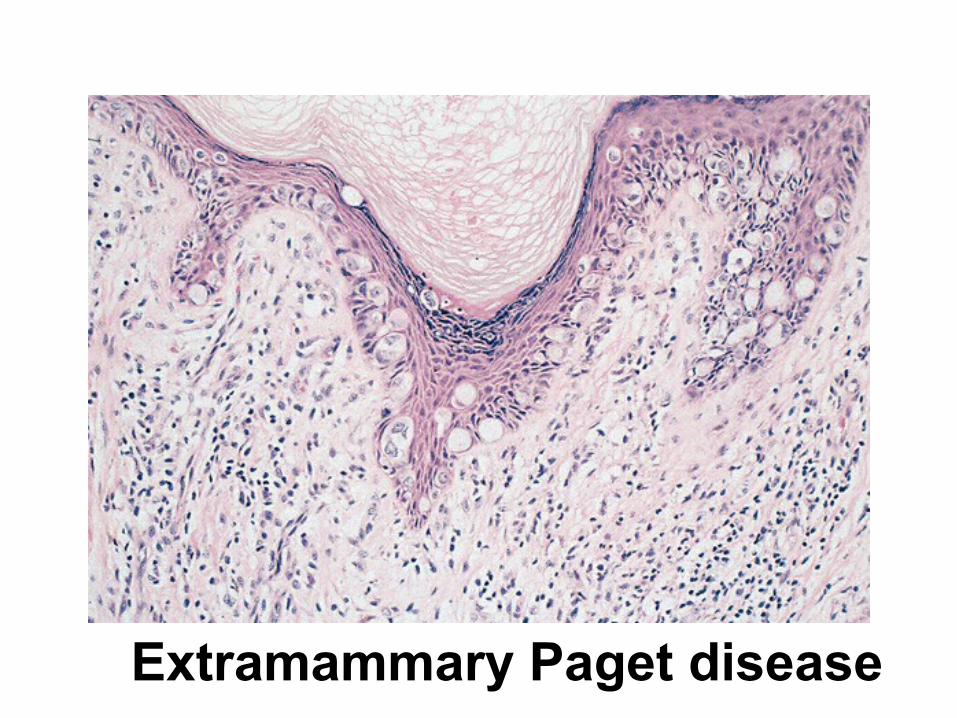
Extramammary Paget disease
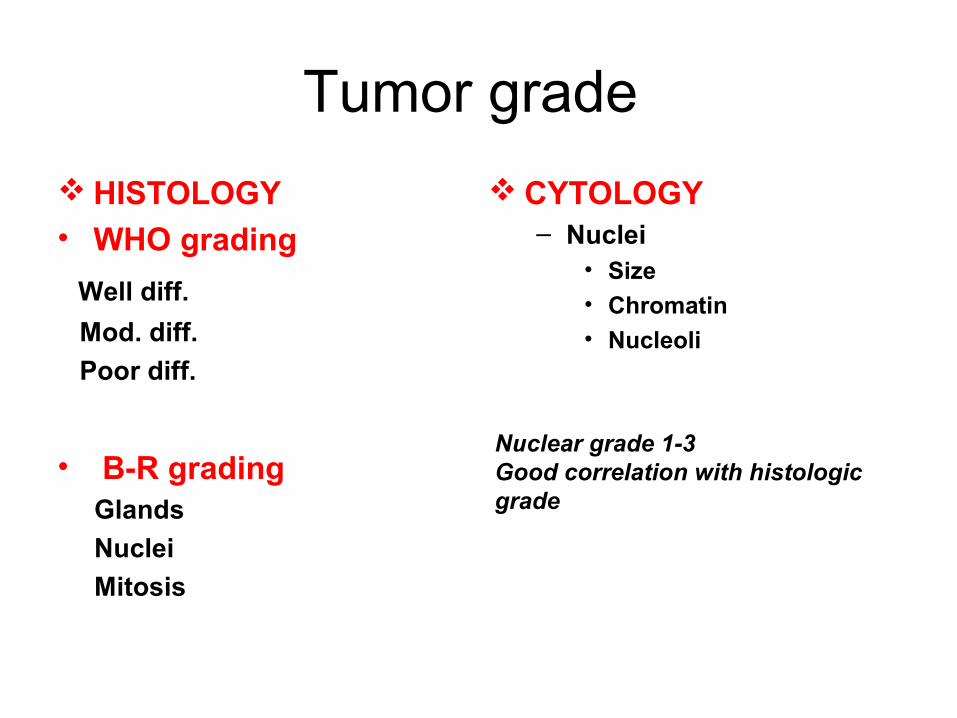
Tumor grade
HISTOLOGY • WHO grading
Well diff.
Mod. diff.
Poor diff.
• B-R grading Glands
Nuclei
Mitosis
CYTOLOGY– Nuclei
• Size
• Chromatin• Nucleoli
Nuclear grade 1-3Good correlation with histologic grade
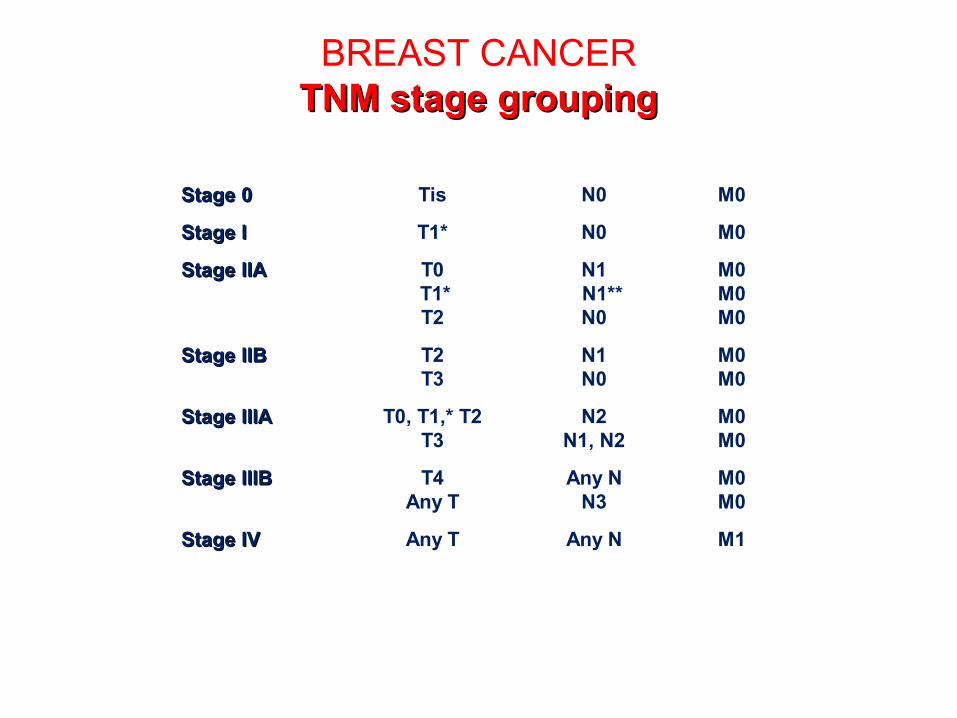
BREAST CANCERTNM stage groupingTNM stage grouping
Stage 0Stage 0 Tis N0 M0
Stage IStage I T1* N0 M0
Stage IIAStage IIA T0 N1 M0 T1* N1** M0T2 N0 M0
Stage IIBStage IIB T2 N1 M0T3 N0 M0
Stage IIIAStage IIIA T0, T1,* T2 N2 M0T3 N1, N2 M0
Stage IIIBStage IIIB T4 Any N M0Any T N3 M0
Stage IVStage IV Any T Any N M1
* Note: T1 includes T1 mic.** Note: The prognosis of patients with N1a is similar to that of patients with pN0.
AJCC® Cancer Staging Manual, 5th edition (1997) published by Lippincott-Raven Publishers,
Philadelphia, Pennsylvania.
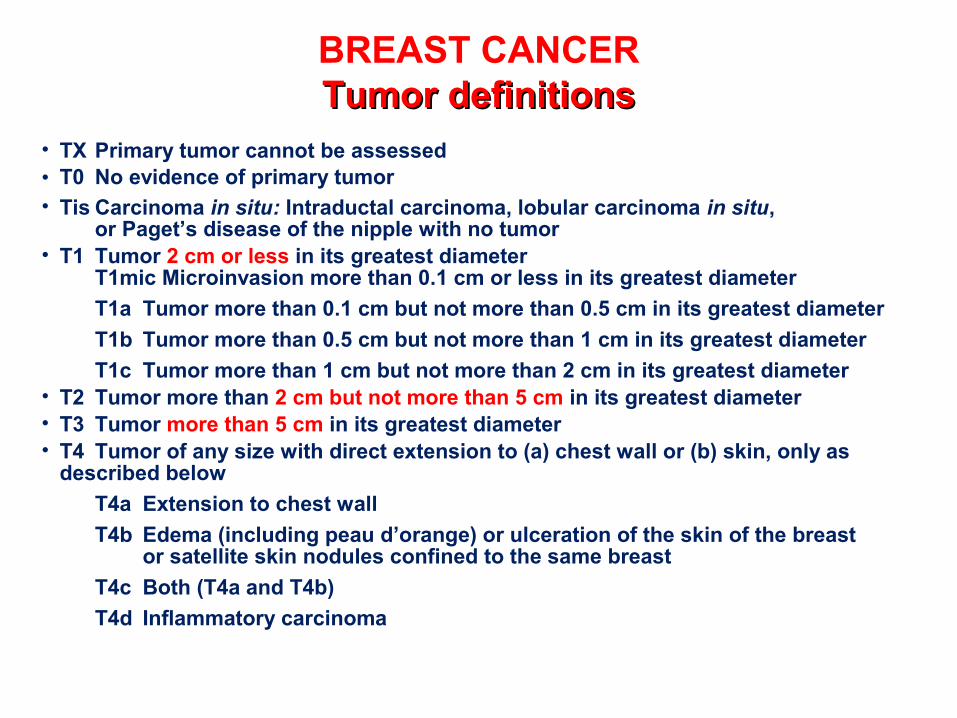
BREAST CANCERTumor definitionsTumor definitions
• TX Primary tumor cannot be assessed• T0 No evidence of primary tumor• Tis Carcinoma in situ: Intraductal carcinoma, lobular carcinoma in situ,
or Paget’s disease of the nipple with no tumor• T1 Tumor 2 cm or less in its greatest diameter
T1mic Microinvasion more than 0.1 cm or less in its greatest diameter
T1a Tumor more than 0.1 cm but not more than 0.5 cm in its greatest diameter
T1b Tumor more than 0.5 cm but not more than 1 cm in its greatest diameter
T1c Tumor more than 1 cm but not more than 2 cm in its greatest diameter• T2 Tumor more than 2 cm but not more than 5 cm in its greatest diameter• T3 Tumor more than 5 cm in its greatest diameter• T4 Tumor of any size with direct extension to (a) chest wall or (b) skin, only as
described below
T4a Extension to chest wall
T4b Edema (including peau d’orange) or ulceration of the skin of the breast or satellite skin nodules confined to the same breast
T4c Both (T4a and T4b)
T4d Inflammatory carcinomaAJCC® Cancer Staging Manual, 5th edition (1997)
published by Lippincott-Raven Publishers, Philadelphia, Pennsylvania.
BREAST CANCER
Commonly assessed prognostic Commonly assessed prognostic factorsfactors
Slamon DJ. Chemotherapy Foundation. 1999;46.Winer E, et al. Cancer: Principles & Practice of Oncology. 6th ed.
2001;1651-1717.
Nuclear grade
Estrogen/progesteronereceptors
HER2/neu overexpression
Number of positive axillary nodes
Tumor size
Lymphatic and vascular invasion
Histologic tumor type
Histologic grade
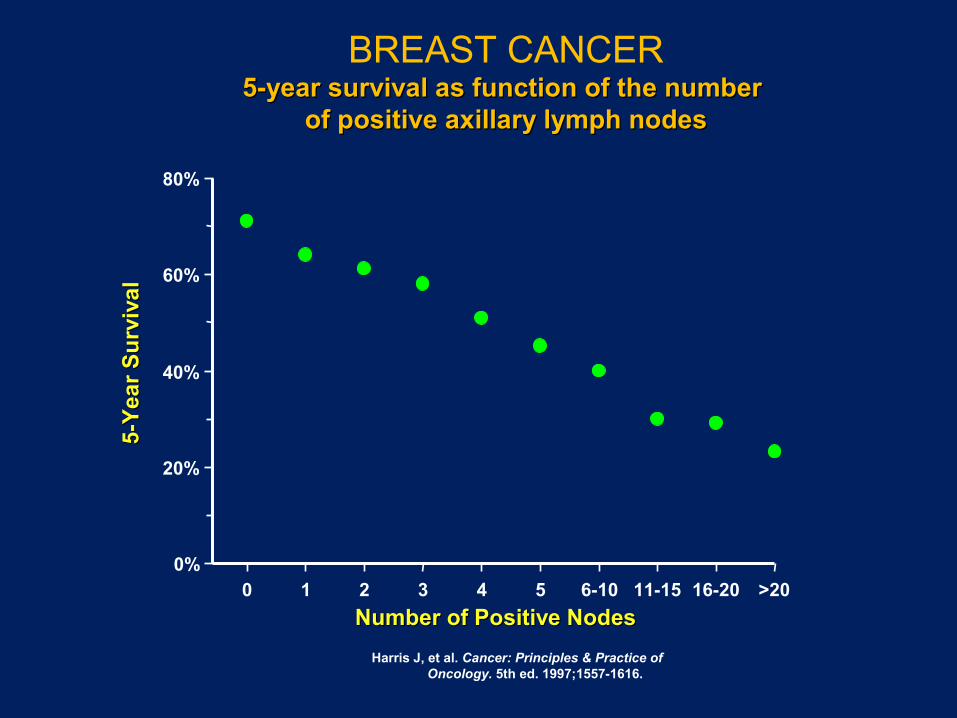
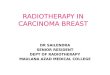
BREAST CANCER5-year survival as function of the number 5-year survival as function of the number
of positive axillary lymph nodesof positive axillary lymph nodes
0%
20%
40%
60%
80%
5-Y
ear
Su
rviv
al
5-Y
ear
Su
rviv
al
0 1 2 3 4 5 6-10 11-15 16-20 >20
Number of Positive NodesNumber of Positive Nodes
Harris J, et al. Cancer: Principles & Practice of Oncology. 5th ed. 1997;1557-1616.
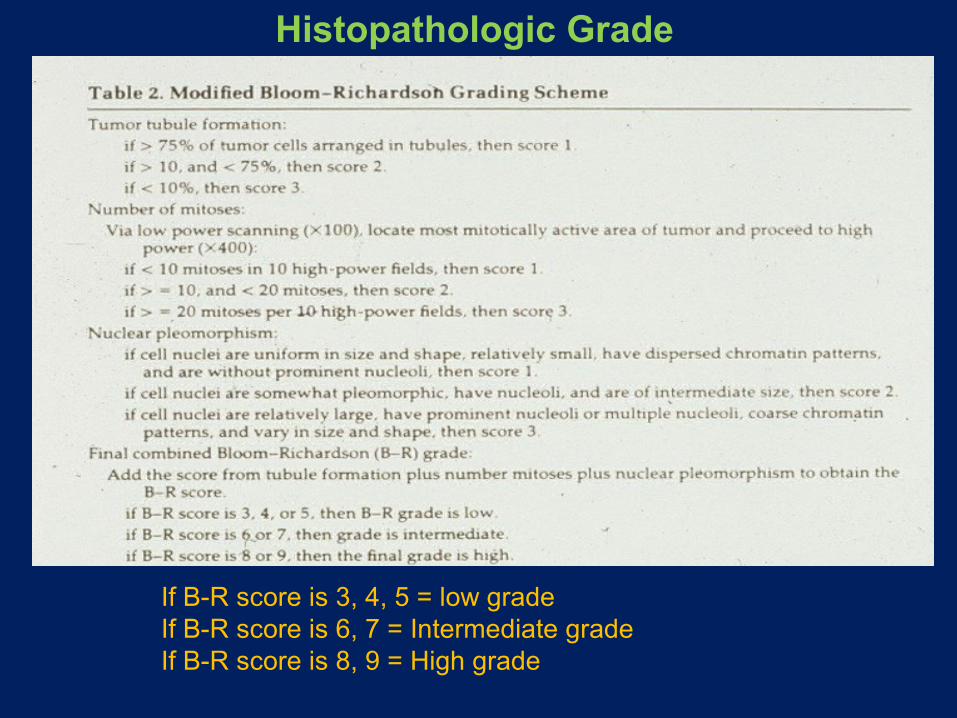
Histopathologic Grade
If B-R score is 3, 4, 5 = low gradeIf B-R score is 6, 7 = Intermediate gradeIf B-R score is 8, 9 = High grade
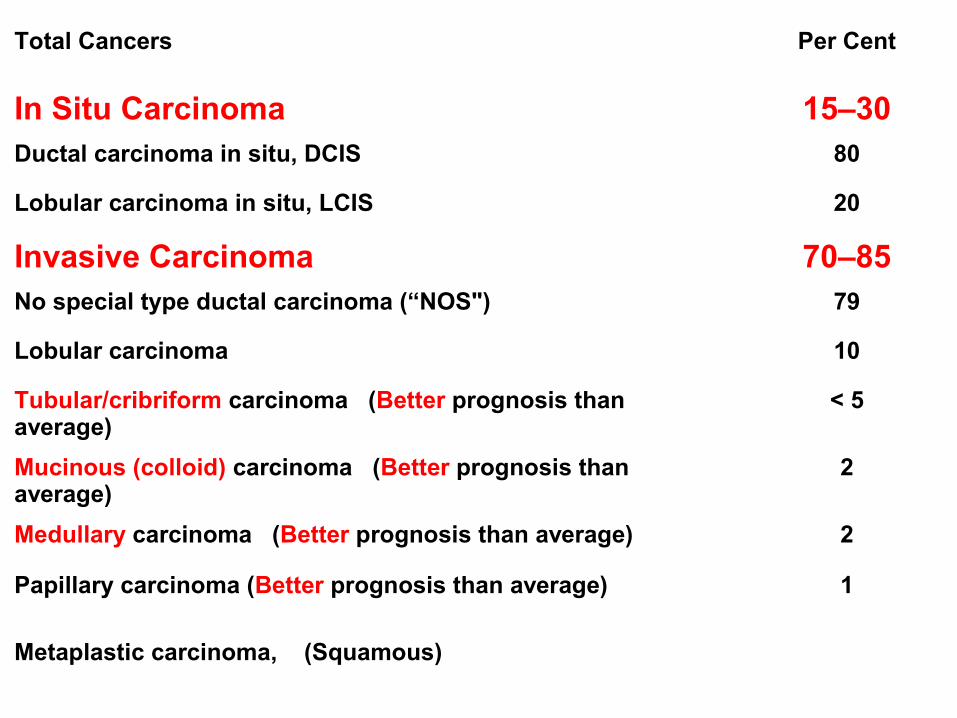
Total Cancers Per Cent
In Situ Carcinoma 15–30Ductal carcinoma in situ, DCIS 80
Lobular carcinoma in situ, LCIS 20
Invasive Carcinoma 70–85No special type ductal carcinoma (“NOS") 79
Lobular carcinoma 10
Tubular/cribriform carcinoma (Better prognosis than average)
< 5
Mucinous (colloid) carcinoma (Better prognosis than average)
2
Medullary carcinoma (Better prognosis than average) 2
Papillary carcinoma (Better prognosis than average) 1
Metaplastic carcinoma, (Squamous)
The “Triple Test”: (Screening)– Clinical picture– Mammographic findings– Cytologic findings
Biopsy. (diagnosis)
MALE BREAST
• GYNECOMASTIA (related to hyperestrogenism)
• CARCINOMA (1% of ♀ )

Gynecomastia
• Reversible enlargement of the male breast• Unilateral or bilateral subareolar mass +/-pain• Ductal and stromal proliferation• Etiology- Systemic disease-hyperthyroidism,
cirrhosis, chronic renal failure– Drugs-cimetidine, digitalis, tricyclic
antidepressants, marijuana– Neoplasms-pulmonary, testicular germ cell tumors– Hypogonadism: testicular atrophy, exogenous
estrogen, Klinefelter’s syndrome


GYNECOMASTIA (NO lobules)
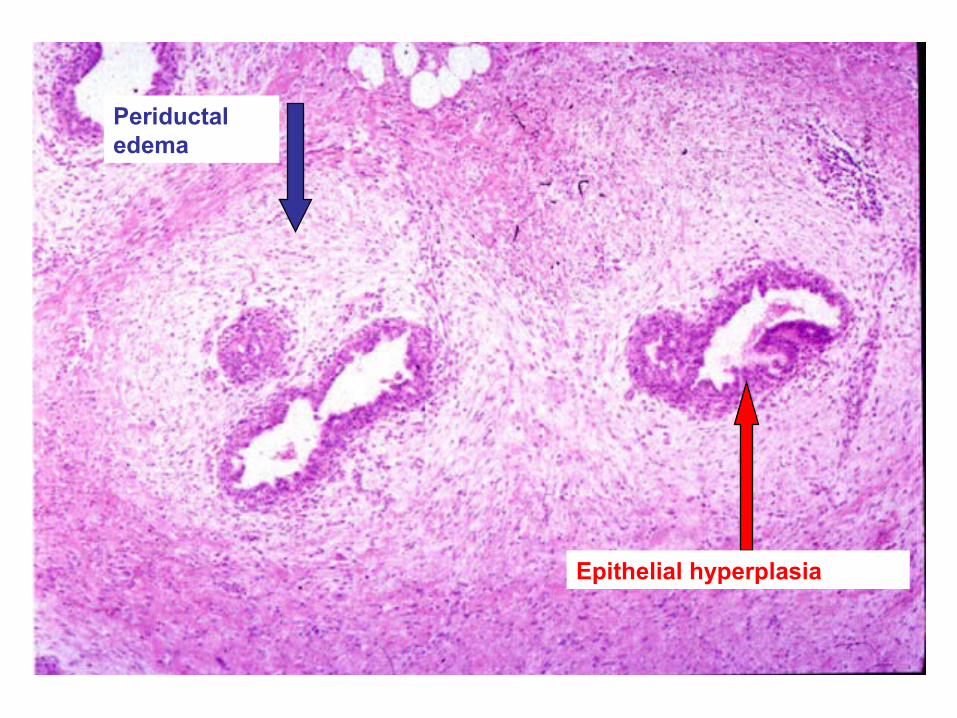
Periductal edema
Epithelial hyperplasia
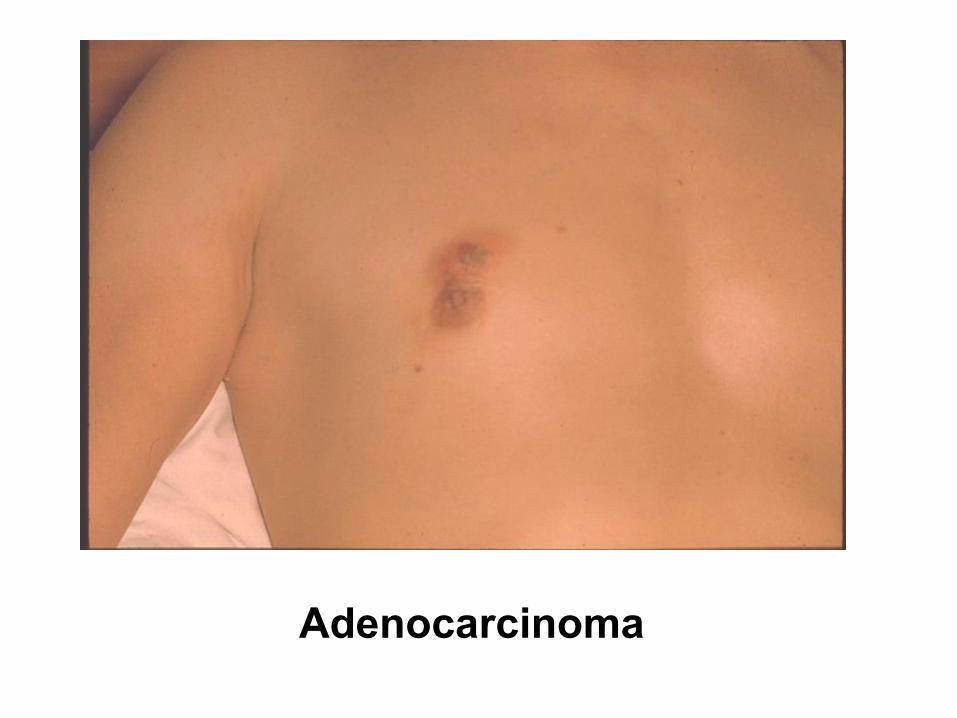
Adenocarcinoma
Carcinoma of the Male Breast
• < 1% of breast cancer• Very rare occurrence; F/M = 100:1• Infiltrating ductal carcinoma.• Tends to present at a more advanced stage
– Less fat and breast tissue, therefore involvement of chest wall occurs earlier
• Similar prognosis when matched, stage for stage, with female breast cancer
• Associated with inherited BRCA2 mutation
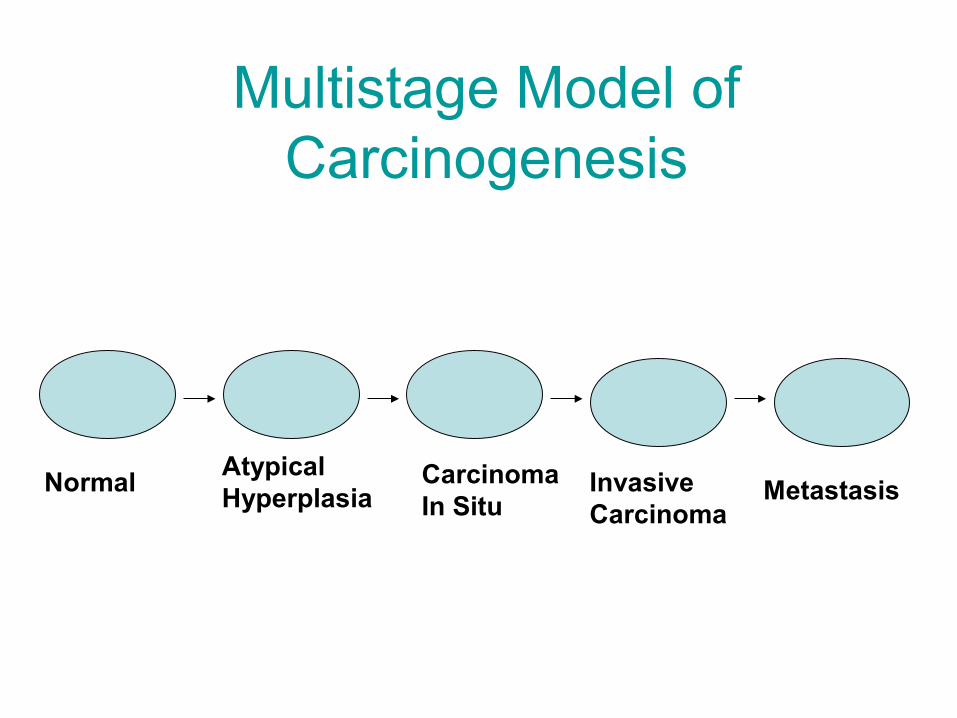
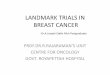
Multistage Model of Carcinogenesis
NormalAtypicalHyperplasia
Carcinoma In Situ
Invasive Carcinoma
Metastasis
QUIZ
1. List the benign breast diseases that increase a
patient’s risk of developing breast cancer and
classify these conditions by the degree of risk.