Embed Size (px)
Citation preview

Chapter 7: Acute Respiratory Distress
SyndromeJames D. Fortenberry, MD, FCCM, FAAP
Medical Director, Critical Care Medicine and Pediatric/Adult ECMO
Children’s Healthcare of Atlanta at Egleston

ARDS: What Is It?
Term first introduced in 1967Acute respiratory failure with non-cardiogenic
pulmonary edema, capillary leak after diverse insultAdult RDS defined to differentiate from neonatal
surfactant deficiencyProblems with definition troubled literatureMurray score 1988: CXR, PEEP, Hypoxemia,
ComplianceSynonyms
Shock lung Da Nang Lung Traumatic wet lung
New and Improved
Adult Respiratory Distress Syndrome
Acute Respiratory Distress Syndrome

ARDS: New Definition
Criteria Acute onset Bilateral CXR infiltrates PA pressure < 18 mm Hg Classification
Acute lung injury - PaO2 : F1O2 < 300Acute respiratory distress syndrome - PaO2 : F1O2 < 200
- 1994 American - European Consensus Conference
ARDS - Epidemiology
New criteria allow better estimate of incidence
• 1994 criteria in Sweden: ALI 17.9/100,000; 13.5/100,000 ARDS
• US: may be closer to 75/1000,000• Prospective data pending• Incidence in children appears similar• 5-9% of PICU admissions

Clinical Disorders Associated with ARDS
Direct Lung Injury Indirect Lung Injury
Common causes Common CausesPneumonia SepsisAspiration of gastriccontents
Severe trauma with shock ,multiple transfusions
Less common causes Less common causesPulmonary contusion Cardiopulmonary bypassFat emboli Drug overdoseNear-Drowning Acute pancreatitisInhalational injury Transfusions of blood productsReperfusion pulmonaryedema

The Problem: Lung Injury
Etiology In Children
Other 4%
Hemorrhage 5%
Trauma 5%
Non-infectious Pneumonia 14%
Cardiac Arrest 12%
Septic Syndrome 32%
Infectious Pneumonia 28%
Davis et al., J Peds 1993;123:35

ARDS - Pathogenesis
Instigation• Endothelial injury: increased permeability of alveolar - capillary barrier
• Epithelial injury : alveolar flood, loss of surfactant, barrier vs. infection
• Pro-inflammatory mechanisms

ARDS Pathogenesis: Resolution Phase
Equally important• Alveolar edema - resolved by active sodium transport
• Alveolar type II cells - re-epithelialize
• Neutrophil clearance needed


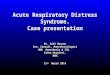
ARDS - Pathophysiology
• Capillary leak:non-cardiogenic pulmonary edema
• Inflammatory mediators• Diminished surfactant activity and airway
collapse• Reduced lung volumes• Heterogeneous• “Baby Lungs”• Altered pulmonary hemodynamics

ARDS:CT Scan View

ARDS - Pathophysiology: Diminished Surfactant Activity
• Surfactant production and composition altered in ARDS: low lecithin-sphingomyelin ratio
• Components of edema fluid may inactivate surfactant

ARDS - Pathophysiology: Diminished Surfactant Activity
• Surfactant product of Type II pneumocytes• Importance of surfactant:
P = 2T/r (Laplace equation; P: trans-pulmonary pressure, T: surface tension, r: radius)
• Surfactant proportions surface tension to surface area: thus



ARDS - Pathophysiology: Lung Volumes• Reduced lung volumes, primarily reduced FRC• FRC = ? Nl = • Low FRC-large intrapulmonary shunt, hypoxemia• Implies
lower compliance = flatter PV curve marked hysteresis PV curve concave above FRC and inflection point
at volume > FRC closing volume in range of tidal volume resistance increased primarily due to mechanical
unevenness (vs. airway R): high flow rates helpful




ARDS - Pathophysiology: Lung Volumes
• FRC = Volume of gas in lungs at end of normal tidal expiration; outward recoil of chest wall = inward recoil of lungs
• Normal FRC = • FRC decreased by 20-40% in ARDS• FRC decreased by 20-30% when supine:
elevate head!

ARDS - Pathophysiology: Mediators
• Massive literature• Mediators involved but extent of
cause/effect unknown• Cellular:
neutrophils-causative: depletion in models can obliterate lesion; ARDS can occur in neutropenic patient; direct endothelial injury, release radicals, proteolytic enzymes
macrophages-release cytokines
ARDS - Pathophysiology: Mediators
• Humoral: Complement Cytokines: TNF, IL-1 PAF, PGs, leukotrienes NO Coagulant pathways

ARDS - Pathophysiology:Pulmonary Edema
• Non-cardiogenic pulmonary edema-Starling formula
• What changes in ARDS? Q = K(Pc - Pis) - σ (Π pl - Π is)
Q = K = Pc = ; Pis = σ = Πpl = ; Π is =


Phases of ARDS
• Acute - exudative, inflammatory: capillary congestion, neutrophil aggregation, capillary endothelial swelling, epithelial injury; hyaline membranes by 72 hours
(0 - 3 days)• Sub-acute - proliferative: proliferation of type II
pneumocytes (abnormal lamellar bodies with decreased surfactant), fibroblasts-intra-alveolar, widening of septae
(4 - 10 days)• Chronic - fibrosing alveolitis: remodeling by
collagenous tissue, arterial thickening, obliteration of pre-capillary vessels; cystic lesions
( > 10 days)


ARDS - Outcomes
• Most studies - mortality 40% to 60%; similar for children/adults
• Death is usually due to sepsis/MODS rather than primary respiratory
• Mortality may be decreasing53/68 % 39/36 %

ARDS - Principles of Therapy
• Provide adequate gas exchange
• Avoid secondary injury

Therapies for ARDS
Innovations:NOPLVProningSurfactantAnti-Inflammatory
Mechanical Ventilation Gentle ventilation:
Permissive hypercapniaLow tidal volumeOpen-lungHFOV
ECMOIVOXIV gas exchange
AVCO2R
Total Implantable Artificial Lung
ARDS
Extrapulmonary Gas Exchange
The Dangers of Overdistention
• Repetitive shear stress• Injury to normal alveoli• inflammatory response• air trapping• Phasic volume swings: volume trauma

• compliance
• intrapulmonary shunt
• FiO2
• WOB
• inflammatory response
The Dangers of Atelectasis

0
10
20
13 33 38
Airway Pressure (cmH20)
Lun
g V
olum
e (m
l/kg)
AtelectasisAtelectasis
““Sweet Spot”Sweet Spot”
OverdistentionOverdistention
Lung Injury Zones
ARDS: George H. W. Bush Therapy
“Kinder, gentler” forms of ventilation:
•Low tidal volumes (6-8 vs.10-15 cc/kg)
•“Open lung”: Higher PEEP, lower PIP
•Permissive hypercapnia: tolerate higher pCO2


Lower Tidal Volumes for ARDS
• Multi-center trial, 861 adult ARDS• Randomized:
Tidal volume 12 cc/kgPlateau pressure < 50 cm H2O
vsTidal volume 6 cc/kgPlateau pressure < 30 cm H2O
ARDS Network,NEJM, 342: 2000

Lower Tidal Volumes for ARDS
0
5
10
15
20
25
30
35
40
Percent
Death
Ven
t freed
ays
Traditional Lower
*
*
* p < .001
ARDS Network,NEJM, 342: 2000
22% decrease

Is turning the ARDS patient “prone” to be
helpful?
Prone Positioning in ARDS
• Theory: let gravity improve matching perfusion to better ventilated areas
• Improvement immediate• Uncertain effect on outcome


Prone Positioning in Adult ARDS
• Randomized trial• Standard therapy vs. standard + prone positioning
• Improved oxygenation• No difference in mortality, time on ventilator, complications
Gattinoni et al., NEJM, 2001
Prone Positioning in Pediatric ARDS:Longer May Be Better
• Compared 6-10 hrs PP vs. 18-24 hrs PP
• Overall ARDS survival 79% in 40 pts.Relvas et al., Chest 2003

Brief vs. Prolonged Prone Positioning in Children
0
5
10
15
20
25
Pre-PP Brief PP Prolonged PP
Oxy
gena
tion
In
dex
(OI)
- Relvas et al., Chest 2003
*
***

High Frequency High Frequency Oscillation:Oscillation:A Whole Lotta A Whole Lotta Shakin’ Goin’ OnShakin’ Goin’ On

- Reese Clark- Reese Clark
It’s not absolute pressure, but volume or pressure
swings that promote lung injury or atelectasis.

• Rapid rate• Low tidal volume
• Maintain open lung• Minimal volume swings
High Frequency Ventilation

High Frequency Oscillatory Ventilation


HFOV is the easiest way to find the ventilation
“sweet spot”

HFOV: Benefits Vs. Conventional Ventilation

HFOV vs. CMV in Pediatric Respiratory Failure: Results
• Greater survival without severe lung disease
• Greater crossover to HFOV and improvement
• Failure to respond to HFOV strong predictor of death
Arnold et al, CCM, 1994

0
20
40
HFOV CV CV toHFOV
HFOV toCV
Surv
ival w
ith C
LD%
- - Arnold et al, Arnold et al, CCMCCM, 1994, 1994
**
HFOV vs. CMV in Pediatric Respiratory Failure
HFOV
• Reduces need for ECMO, chronic lung disease in neonates
• Improves survival without CLD in pediatric ARDS
HFOV: Outcomes of Randomized Controlled Trials


Pediatric ECMO
• Potential candidates• Neonate - 18 years• Reversible disease process• Severe respiratory/cardiac failure• < 10 days mechanical ventilation• Acute, life-threatening deterioration

Impact of ECMO on Survival in Pediatric Respiratory Failure
• Retrospective, multi-center cohort analysis• 331 patients, 32 hospitals• Use of ECMO associated with survival (p < .
001)• 53 diagnosis and risk-matched pairs:
ECMO decreased mortality (26% vs 47%, p < .01)
-Green et al, CCM, 24:1996

Impact of ECMO on Survival inPediatric Respiratory Failure
0
10
20
30
40
50
60
70
80
90
Mortality %
< 25% 25 - 50%
50 -75%
> 75%
ECMO
Non-ECMO
*
p < .05 - Green et al., CCM, 1996

Pediatric Respiratory ECMO - Children’s Healthcare of Atlanta
Diagnosis Number Survival % ELSO Survival%
ARDS/ARF 38 71 51
BacterialPneumonia
9 85 79
ViralPneumonia
24 86 53
Trauma 5 80 63
Burns 4 75 52
TOTAL 86 79% 62%

Other Cost Intensive Therapies
Therapy Cost/Patient
Pediatric ECLS $ 232, 941
Pediatric Liver Transplant $ 206, 375
Pediatric Heart Transplant $ 126,695
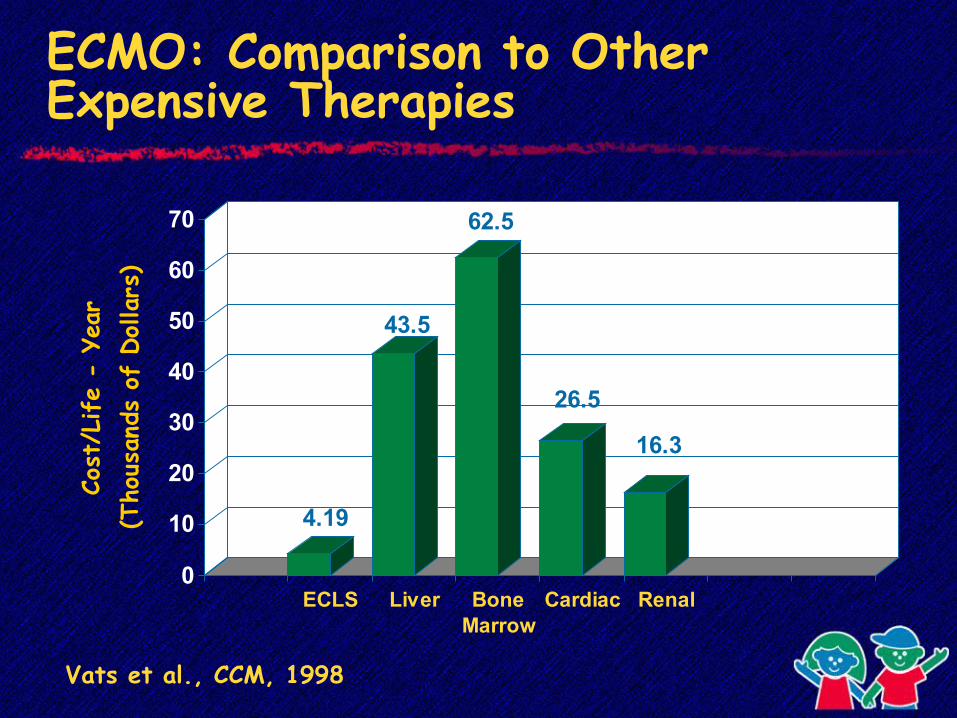
ECMO: Comparison to Other Expensive Therapies
4.19
43.5
62.5
26.5
16.3
0
10
20
30
40
50
60
70
Cost
/Life
- Ye
ar
(Tho
usan
ds o
f Dollars
)
ECLS Liver BoneMarrow
Cardiac Renal
Vats et al., CCM, 1998

If you think about ECMO, it is worth a call to consider
ECMO

Surfactant in ARDS
• ARDS: surfactant deficiency surfactant present is dysfunctional
• Surfactant replacement improves physiologic function

Calf’s Lung Surfactant Extract in Acute Pediatric Respiratory Failure
• Multi-center trial-uncontrolled, observational
• Calf lung surfactant (Infasurf) – intra-tracheal
• Immediate improvement and weaning in 24/29 children with ARDS
• 14% mortality-Willson et al,CCM, 24:1996

Surfactant in Pediatric ARDS
• Current randomized multi-center trial
• Placebo vs calf lung surfactant (Infasurf)
• Children’s at Egleston is a participating center-study closed, await results

Steroids in ARDS
• Theoretical anti-inflammatory, anti-fibrotic benefit
• Previous studies with acute use (1st 5 days)
No benefitIncreased 2° infection
Effects of Prolonged Steroids in Unresolving ARDS
• Randomized, double-blind, placebo-controlled trial
• Adult ARDS ventilated for > 7 days without improvement
• Randomized: Placebo Methylprednisolone 2 mg/kg/day x 4 days, tapered over 1 month
Meduri et al, JAMA 280:159, 1998
Steroids in Unresolving ARDS
• By day 10, steroids improved: PaO2/FiO2 ratios Lung injury/MOD scores Static lung compliance
• 24 patients enrolled; study stopped due to survival difference
Meduri et al, JAMA, 1998
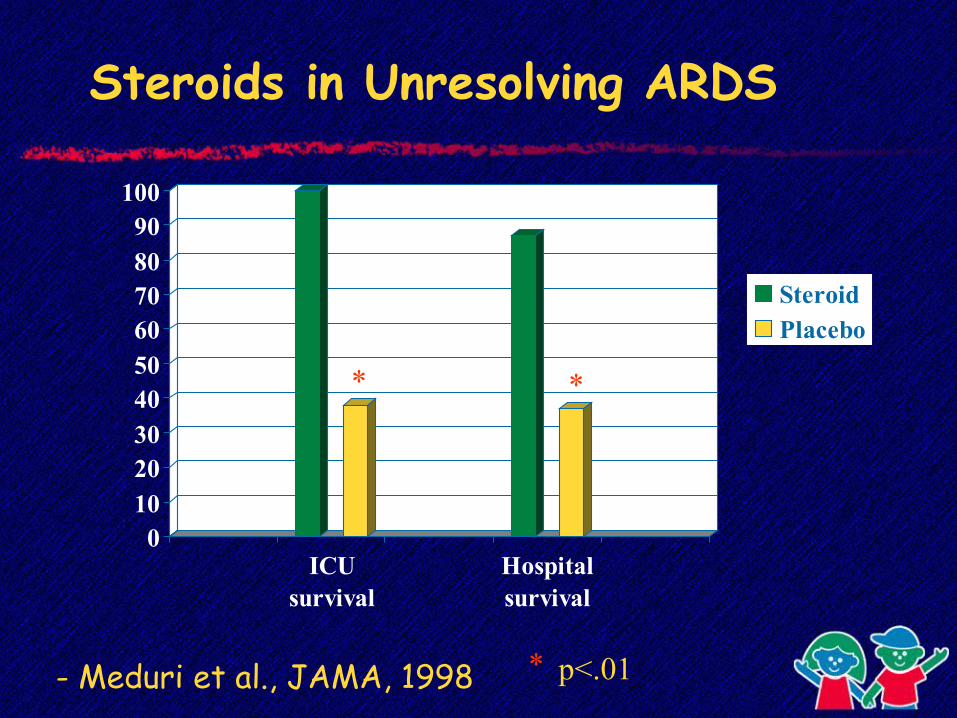
Steroids in Unresolving ARDS
0102030405060708090
100
ICUsurvival
Hospitalsurvival
Steroid Placebo
* *
p<.01*- Meduri et al., JAMA, 1998
Inhaled Nitric Oxide in Respiratory Failure
Neonates Beneficial in term neonates with PPHN Decreased need for ECMO
Adults/Pediatrics Benefits - lowers PA pressures, improves gas exchange
Randomized trials: No difference in mortality or days of ventilation

ECMO and NO in Neonates
• ECMO improves survival in neonates with PPHN (UK study)
• NO decreases need for ECMO in neonates with PPHN: 64% vs 38% (Clark et al, NEJM, 2000)

Effects of Inhaled Nitric Oxide In Children with AHRF
• Randomized, controlled, blinded multi-center trial
• 108 children with OI > 15• Randomized: Inhaled NO 10 ppm vs. mechanical ventilation alone
Dobyns, Cornfield, Anas, Fortenberry et al., J. Peds, 1999

Inhaled NO and HFOV In Pediatric ARDS
5853
58
71
0
10
20
30
40
50
60
70
80
Surv
ival %
CMV
CMV + NO
HFOV
HFOV + NO Dobyns et al., Dobyns et al.,
J PedsJ Peds, 2000, 2000
*

Partial Liquid Ventilation

Partial Liquid Ventilation
Mechanisms of action oxygen reservoir recruitment of lung volume alveolar lavage redistribution of blood flow anti-inflammatory

Liquid Ventilation
Pediatric trials started in 1996 Partial: FRC (15 - 20 cc/kg)
Study halted 1999 due to lack of benefit
Adult study (2001): no effect on outcome
ARDS- “Mechanical” TherapiesProne positioning - Unproven outcome
benefitLow tidal volumes - Outcome benefit in
large studyOpen-lung strategy - Outcome benefit in
small studyHFOV -Outcome benefit in
small studyECMO - Proven in neonates
unproven in children

Pharmacologic Approaches to ARDS: Randomized Trials
Glucocorticoids - acute - no benefit - fibrosing alveolitis - lowered mortality,
small studySurfactant - possible benefit in
childrenInhaled NO - no benefitPartial liquid ventilation - no benefit

“…We must discard the old approach and continue to search for ways to improve mechanical ventilation. In the meantime, there is no substitute for the clinician standing by the ventilator…”
- Martin J. Tobin, MD