Embed Size (px)
Citation preview
OSAHS IN ELDERLY PATIENTS WITH INSOMNIAPilot studyCéline DegrandeJustine DegrandeJustine MestdaghAstrid VerschaeveSupervisor Prof. Dr. Degryse
2
Table of contents
Goal of the pilot study Background Methods Results Discussion Conclusion

3
Goal of the Pilot Study
• Prevalence of OSAHS in elderly patients with insomnia
• Validity and practical feasibility of questionnaires
4
A little quiz…
• How often do you think older patients complain of sleep disturbances such as insomnia?o 25%o 50%o 75%o 90%o I don’t know

5
Background: Insomnia• Dissatisfaction with either duration or quality
of sleep.
• 3 fundamental criteria• recurrent• despite adequate opportunities for sleep.• impairment of daytime functioning.
• Most common comorbidities:• psychiatric illness • sleep disordered breathing: OSAHS
• Associated with older age – underdiagnosis:• ‘Ageism’• mental illnesses – cognitive disorders• threshold consulting GP• burden of PSG

6
Background: OSAHS• Prevalence:
o 30-60 years:• ♂: 4%• ♀: 2%
o ↑ prevalence with age: • ♂: 28-62% • ♀: 19,5-60%
• Symptoms:o excessive daytime sleepinesso snoring
• Risk factors: o obesity, male gender, ageing, familial
history, sedating medication,…
• Comorbidities: o cardiovascular o metabolic o neurobehavioral
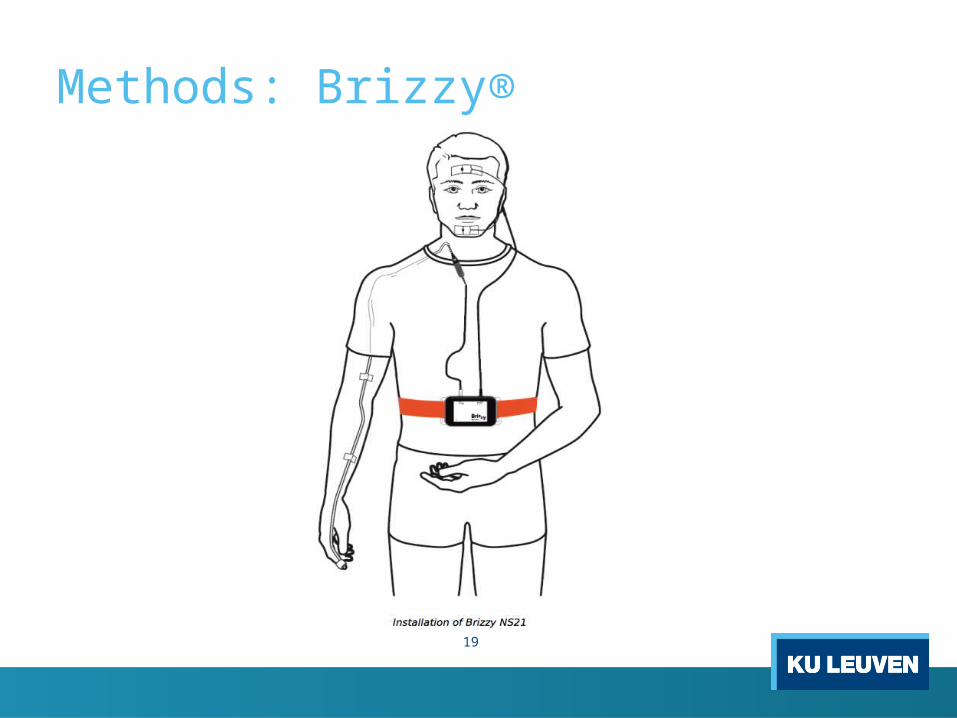
• Diagnosis:o PSG vs portable device (Brizzy®)
7
Background: Questionnaires
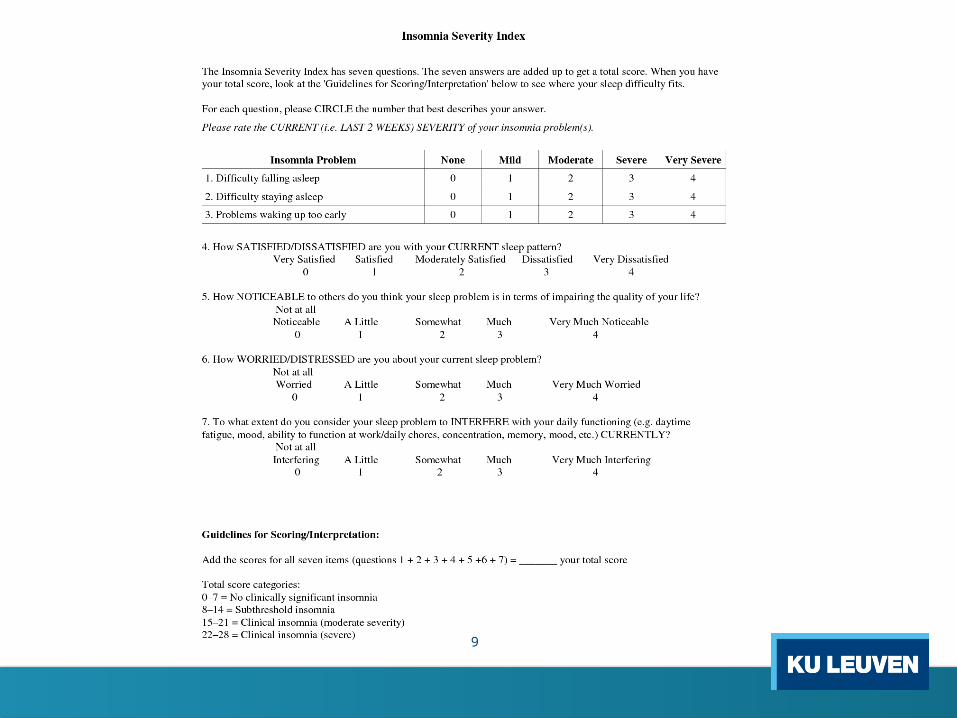
• Insomnia:o ISI
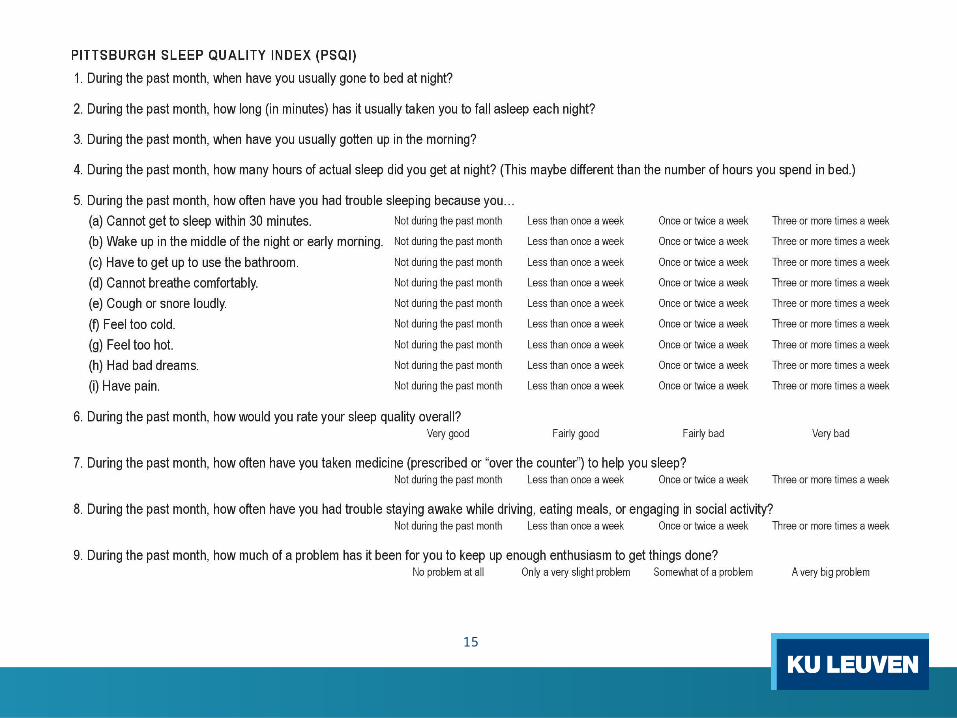
• Sleep quality: o PSQIo ESS
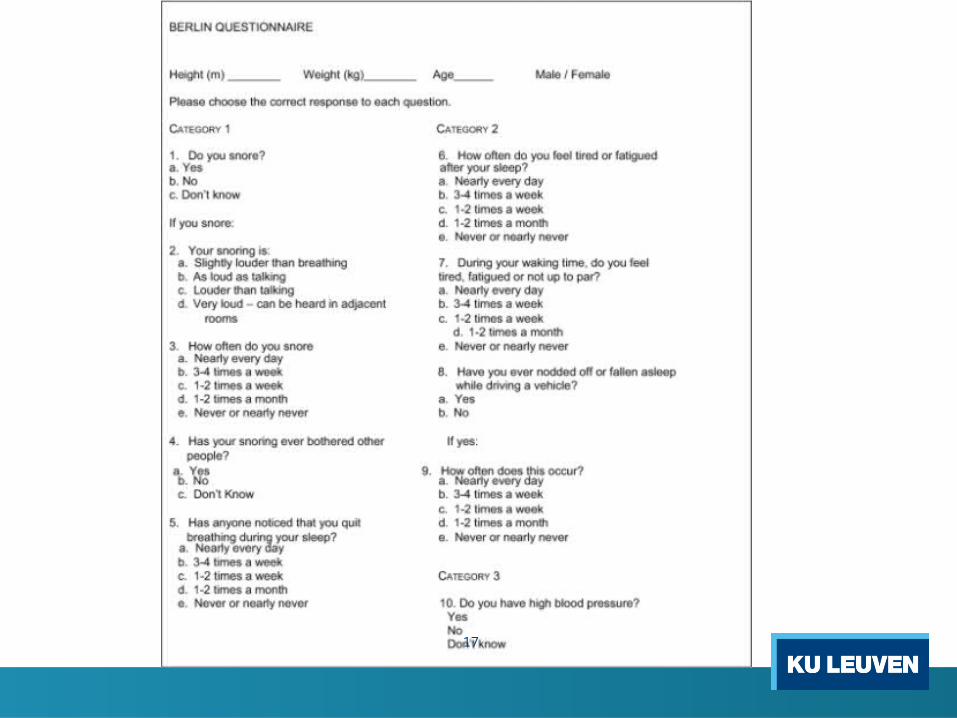
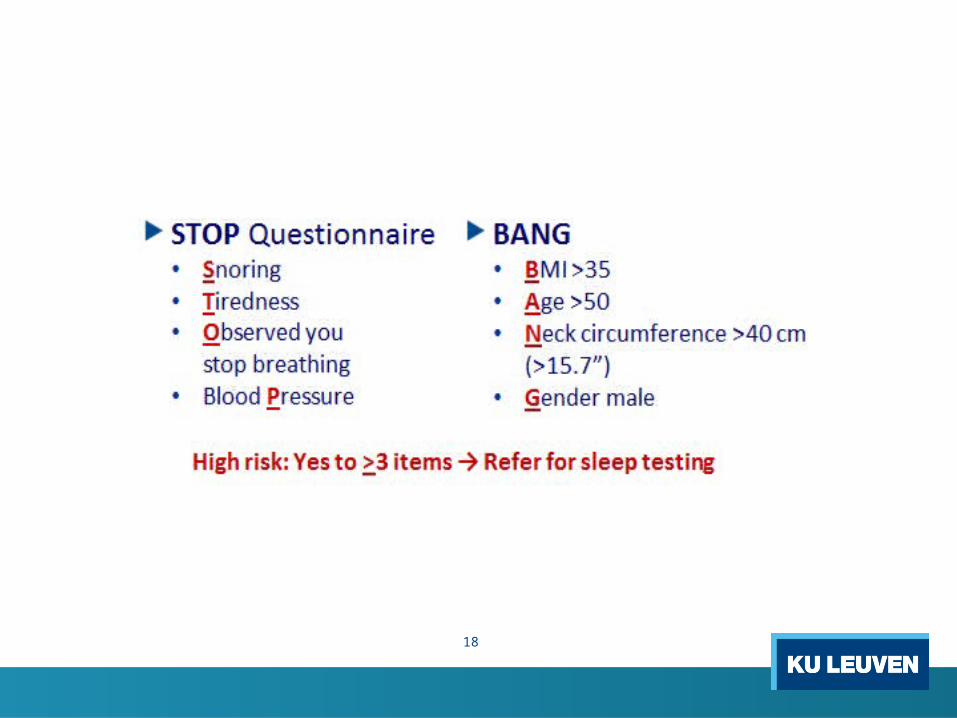
• OSAHS:o BQo STOP-BANG
• Snoring, Tired, Observed, blood Pressure, BMI, Age, Neck circumference, Gender

8
Methods
9
10
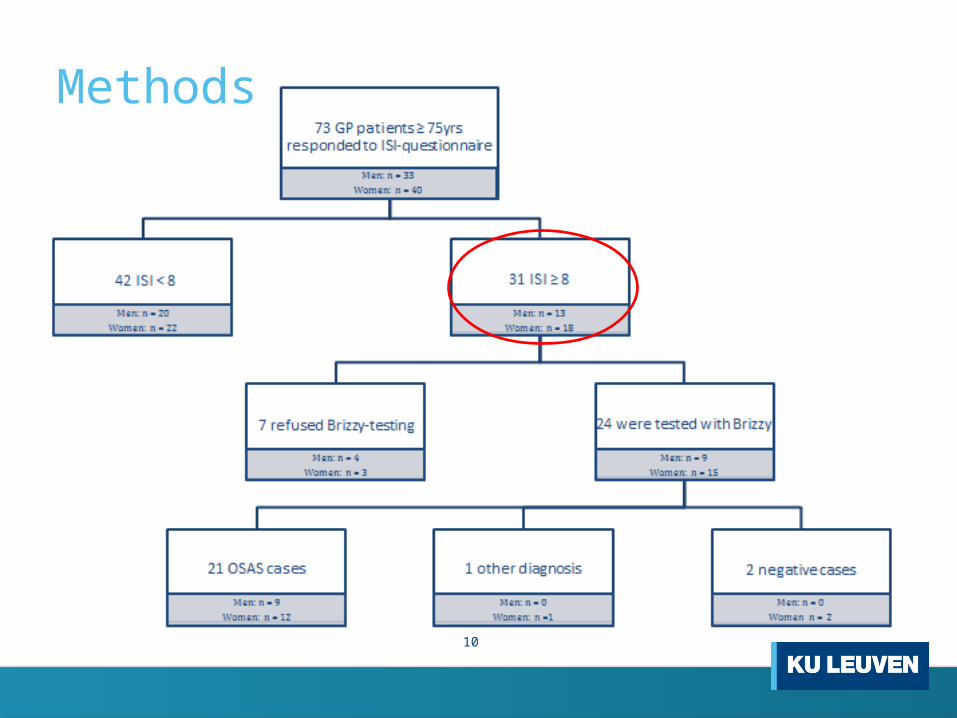
Methods

11
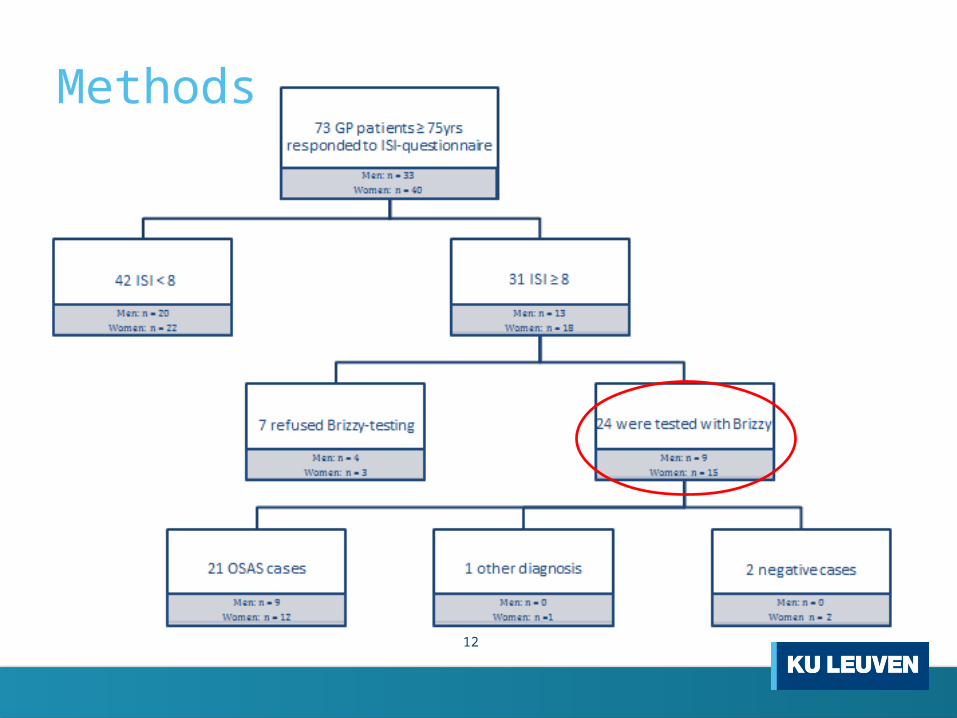
Methods
• Exclusion criteriao terminal patients (life expectancy < 3 months)o diagnosis of dementia (MMSE < 24) o acute precipitating factor for insomnia (physical or
psychological) o Already diagnosed with OSAHS by PSG
• Patients already taking sleep medication NOT excluded!
12
Methods

13
Methods
• Home visito Anamnesis
• History patient• CV RF (smoking, alcohol, familial history,
hypertension, hypercholesterolemia)• Medication use
o Clinical examination• Height, weight, neck circumference,
abdominal circumference, blood pressure,
heart rhythm

14
Methods
• Home visito Questionnaires
• PSQI• ESS• Berlin questionnaire• STOP-BANG
15

16
17
18
19
Methods: Brizzy®

20
Methods: JAWAC
21
Results
• Brizzy® report
• Patient characteristics
• Brizzy® analyses
• Questionnaires

22
Brizzy® report
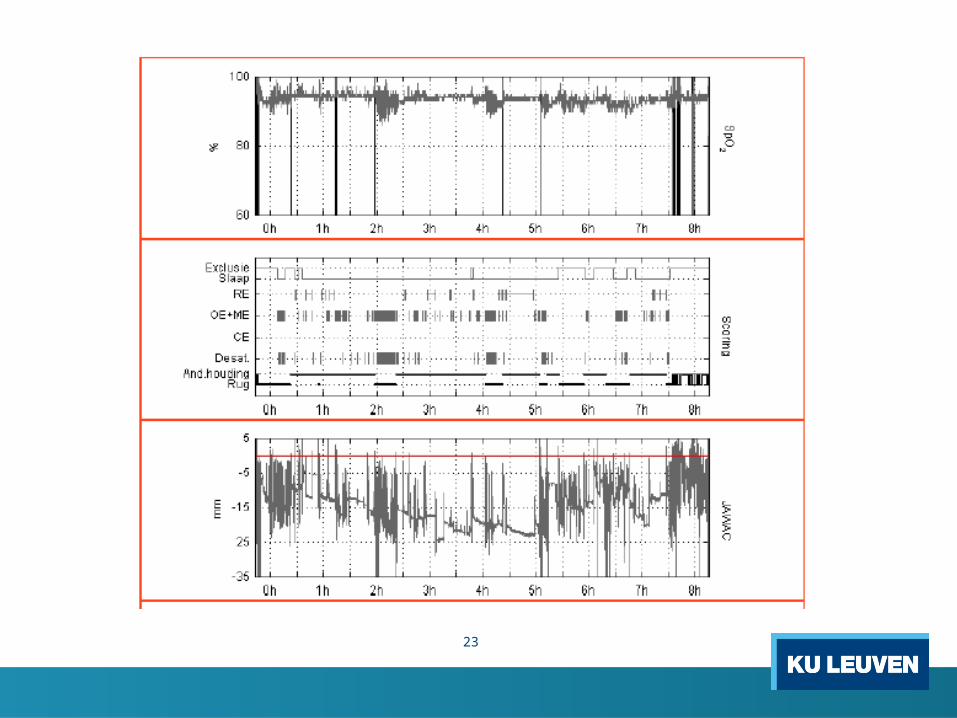
23
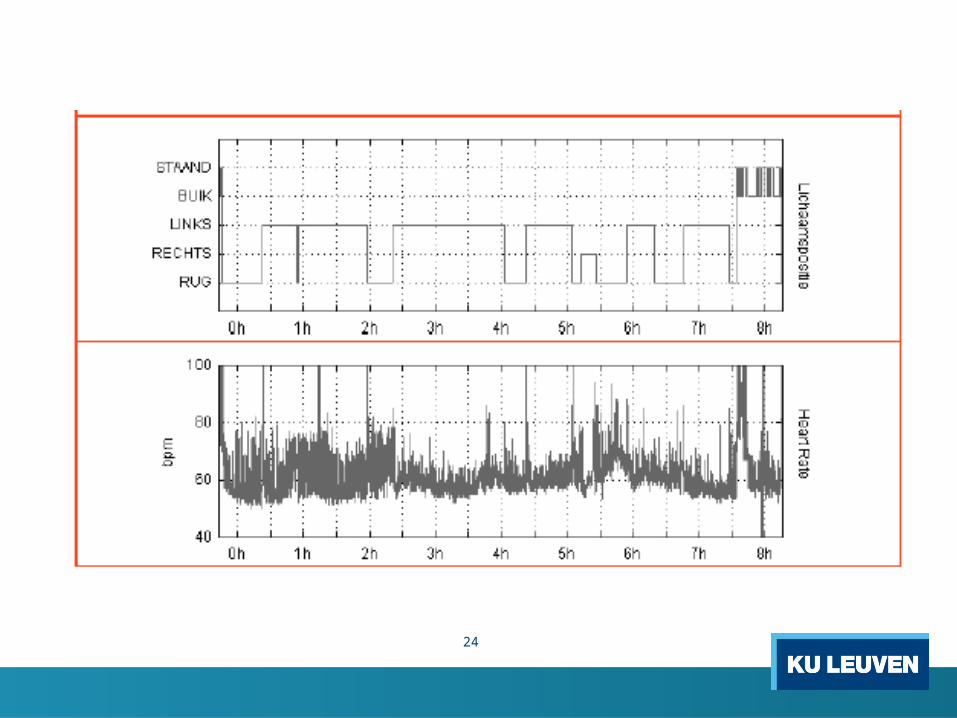
24
25
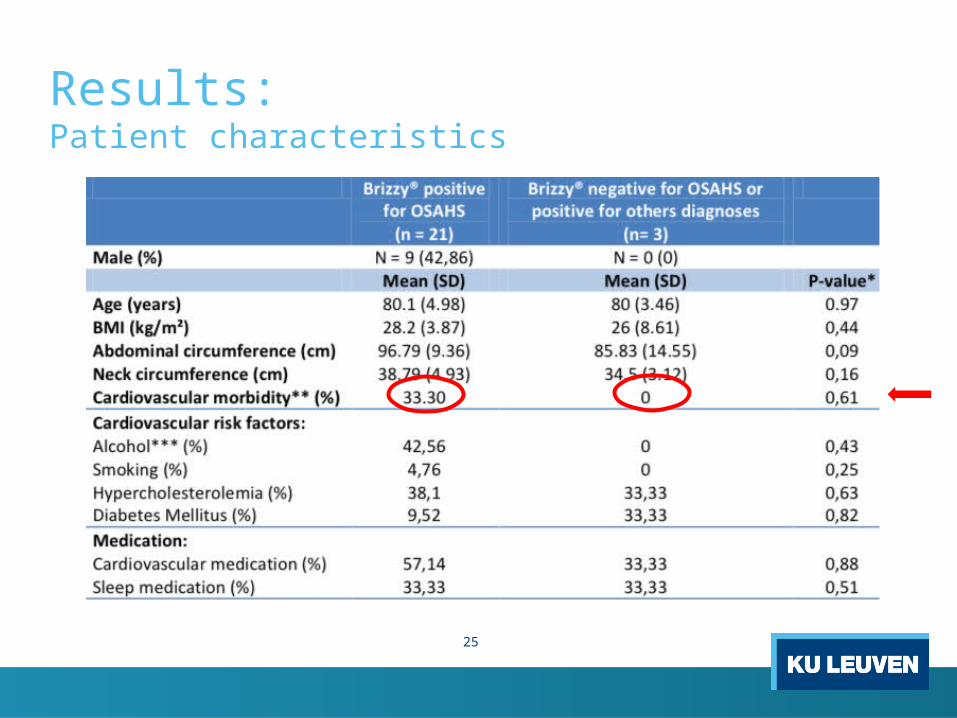
Results: Patient characteristics
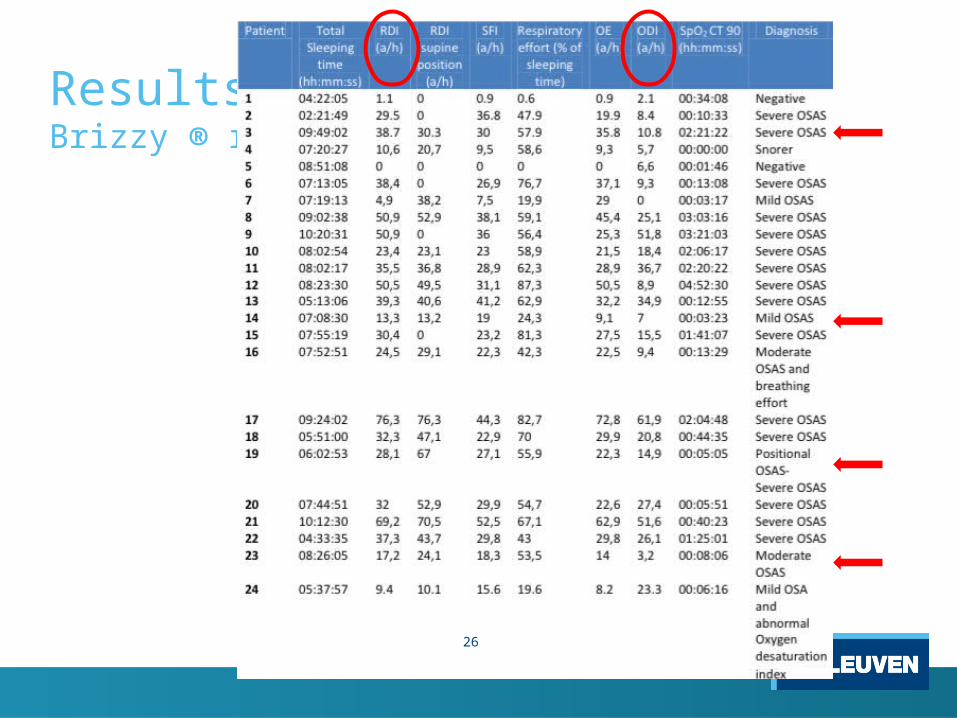
26
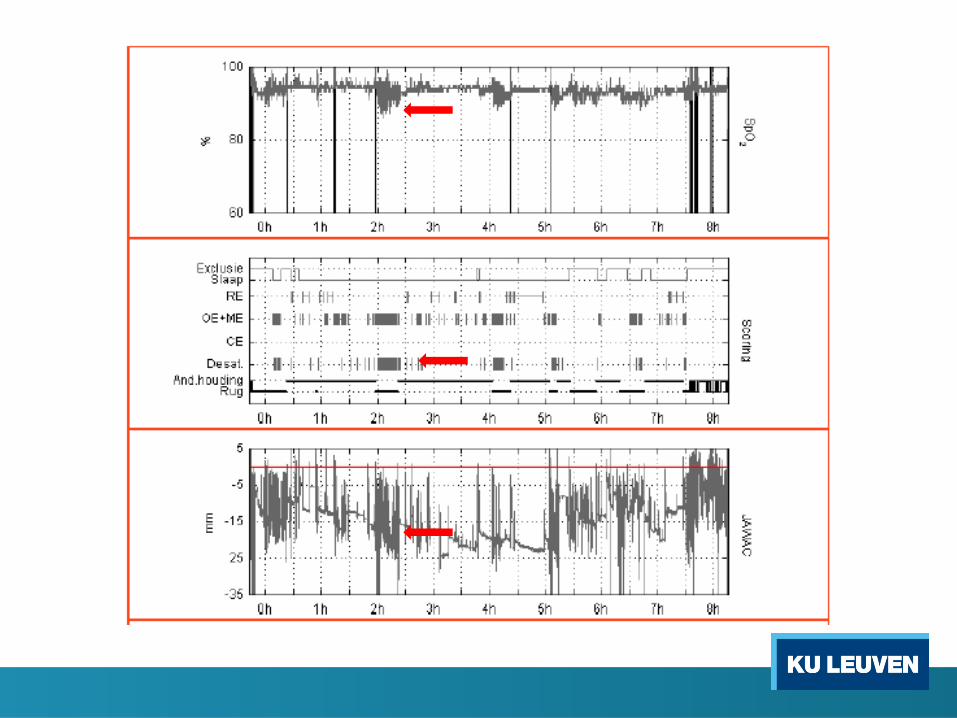
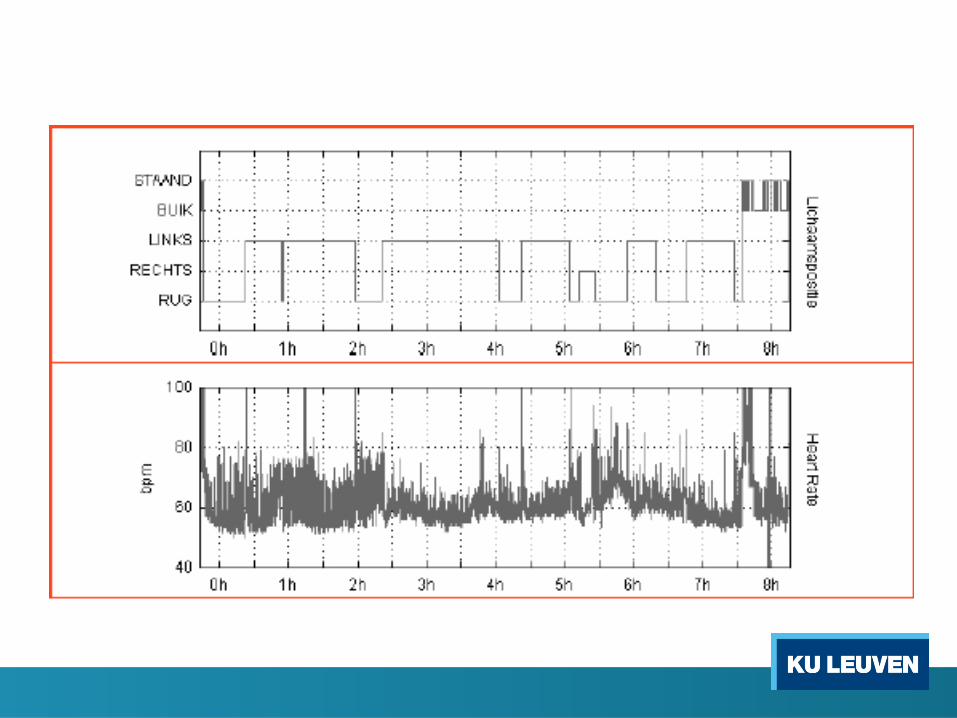
Results:Brizzy ® reports
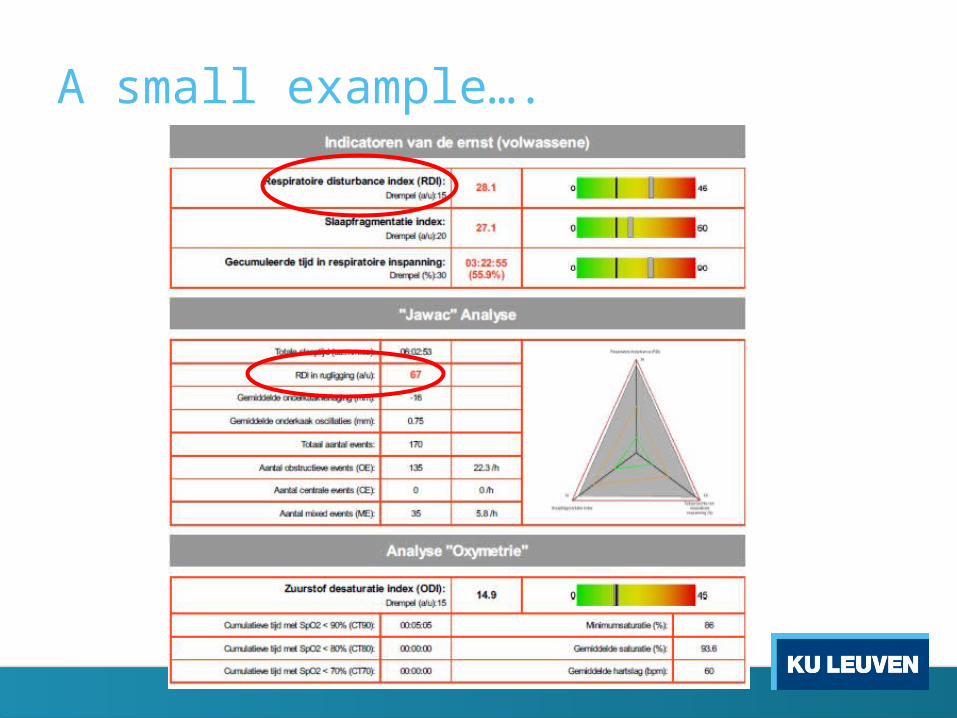
A small example….
30
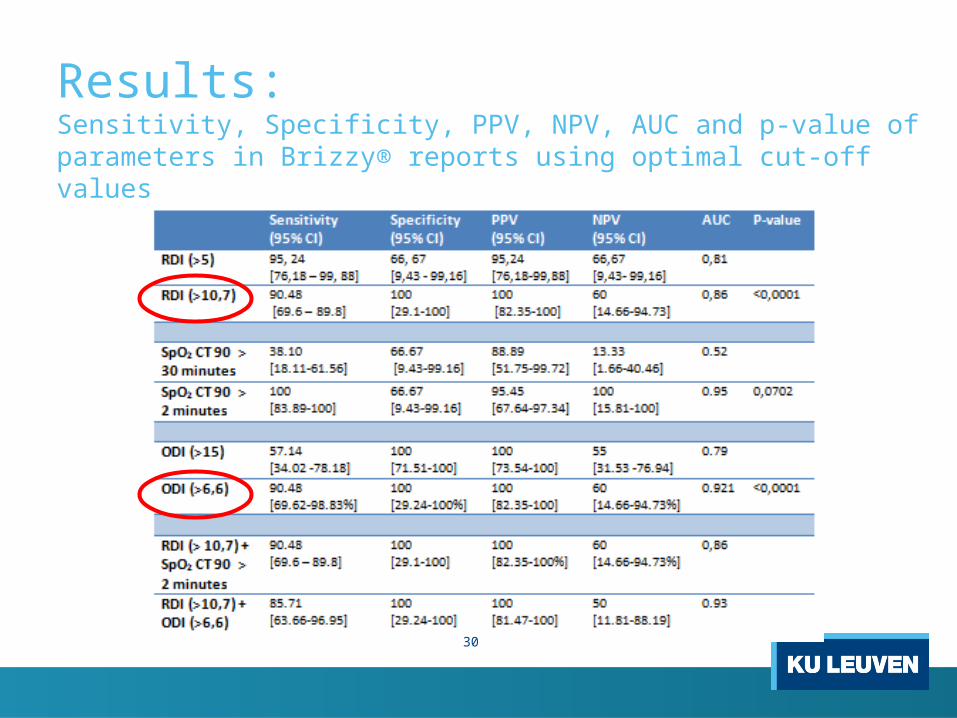
Results:Sensitivity, Specificity, PPV, NPV, AUC and p-value of parameters in Brizzy® reports using optimal cut-off values
31
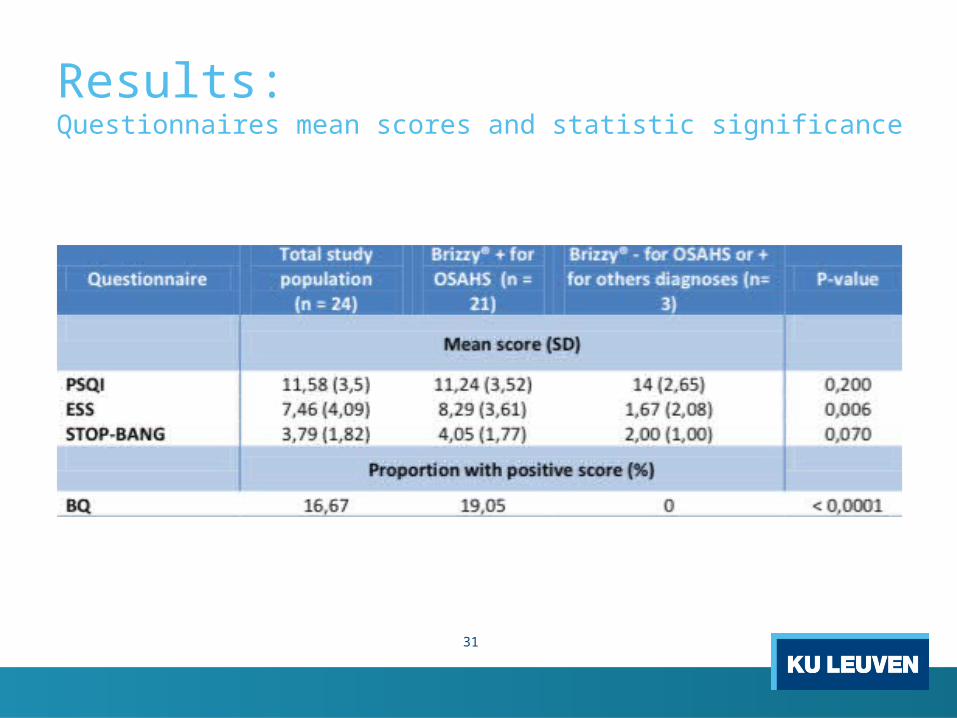
Results:Questionnaires mean scores and statistic significance

32
Results:Questionnaires sensitivity, specificity, PPV and NPV using normal cut-off values
33
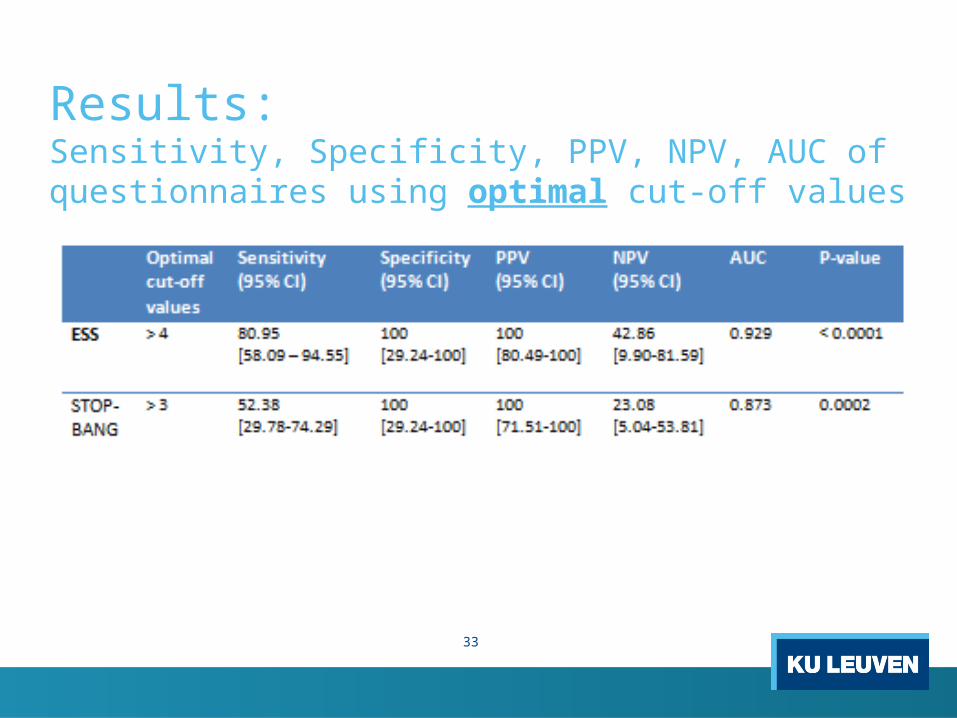
Results:Sensitivity, Specificity, PPV, NPV, AUC of questionnaires using optimal cut-off values

34
Discussion
• Strenghts o Uniformo First step in an unexplored domain
• Limitations o Sample sizeo Brizzy as golden standard o Interobserver variability

35
Discussion
• Underdiagnosis
• Case-finding protocol and ISI as screening tool highly suitable
• Patient characteristics
• RDI – ODI – CT SpO2 < 90%
• Brizzy as a valid ambulant alternative
• ESS – BQ valid questionnaires with optimal cut-off
Conclusion
• OSAHS: severe underdiagnosis • Brizzy as a practical and feasible alternative • Questionnaires in screening
36

37
THANKS FOR YOUR ATTENTION

38
Any questions?