Embed Size (px)
Citation preview
Endovenous Ablation: New MethodsWhere Do We Go From Here?
Steve Elias MD FACS
Director, Vascular Surgery Vein Programs
Columbia University, NY, USA
vein disease is an incurable disease
Vein disease is an incurable disease
New Technologies: Two Categories
• TT (Thermal, Tumescent)
• NTNT (Non Thermal, Non Tumescent)
Thermal Tumescent: TT
• Laser – HSLW, WSLW, radial/jacketed
• Radiofrequency – Closurefast, RFITT
• Steam – SVS, Veneti

Non Thermal, Non Tumescent: NTNT
• Mechanochemical – ClariVein
• Cyanoacrylate glue – Sapheon
• Polidocanol Endovenous Microfoam – BTG
• V Block – VVT Medical
CAG: NTNT
Pollak JS, JVIR, 2001
Permitted for use in endovascular procedures in Europe for several decades
FDA approved in U.S. 2000 Trufill CA (Cordis, Miami, FL) clearance for treatment of cerebral AVMs
CAG: NTNT
Pollak JS, JVIR, 2001Levrier O, J Neuroradiol
2003
Anionic substances such as plasma or blood polymerization of the adhesive upon contact, leading to occlusion
When introduced within a vessel triggers an acute inflammatory reaction in the wall and surrounding tissues
The resultant polymerization damages the vascular intima and induces immunological responses
CAG
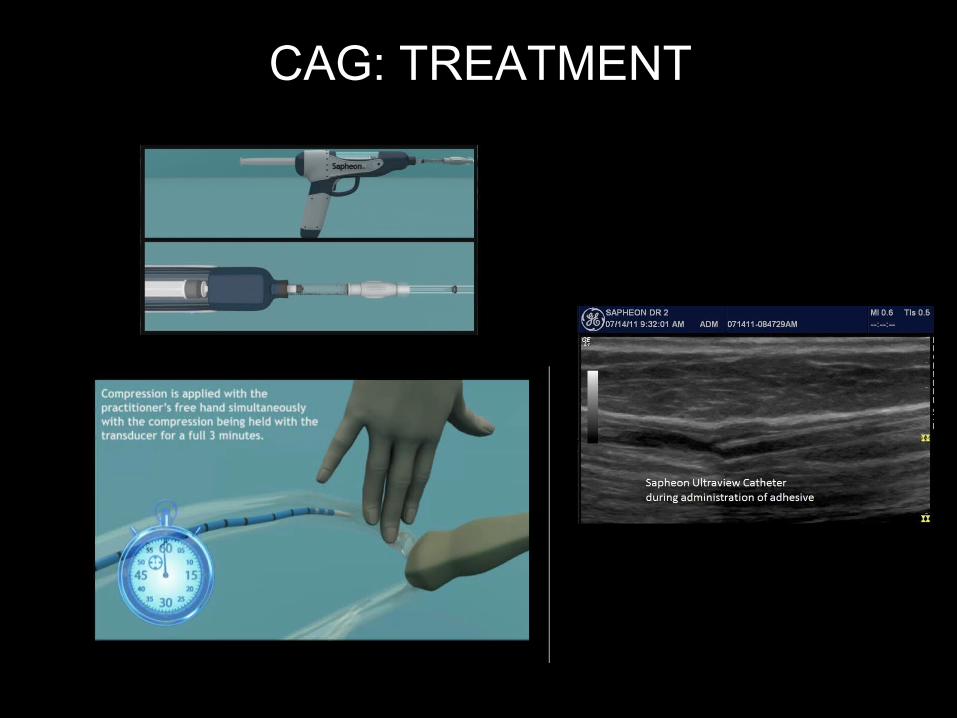
CAG: TREATMENT
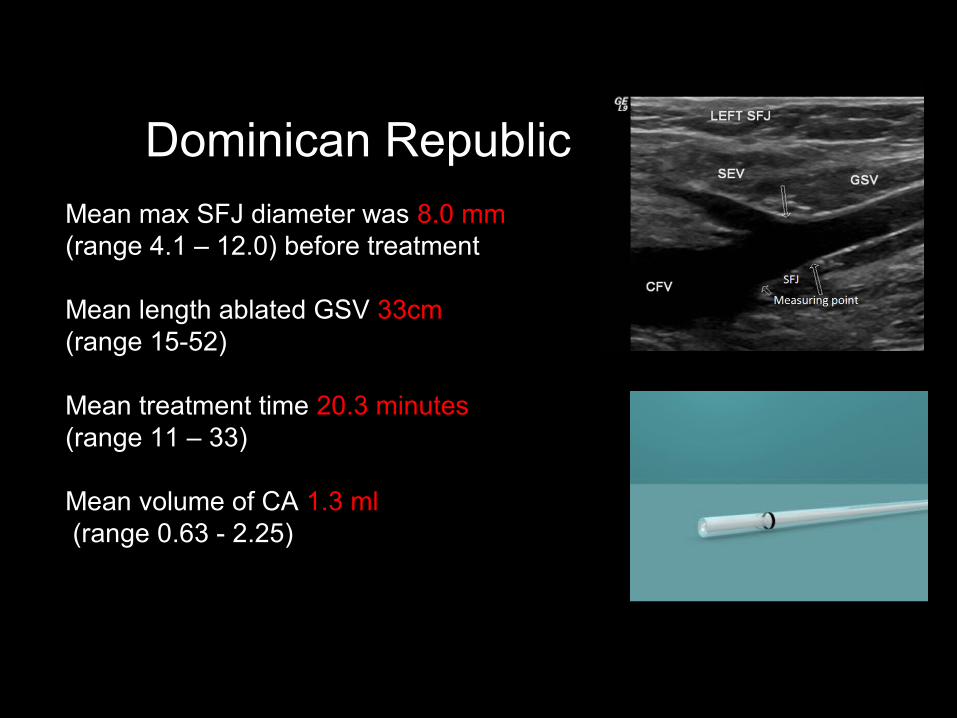
Mean max SFJ diameter was 8.0 mm (range 4.1 – 12.0) before treatment
Mean length ablated GSV 33cm (range 15-52)
Mean treatment time 20.3 minutes (range 11 – 33) Mean volume of CA 1.3 ml (range 0.63 - 2.25)
CAG Dominican Republic
Almeida JI, AVF 2012
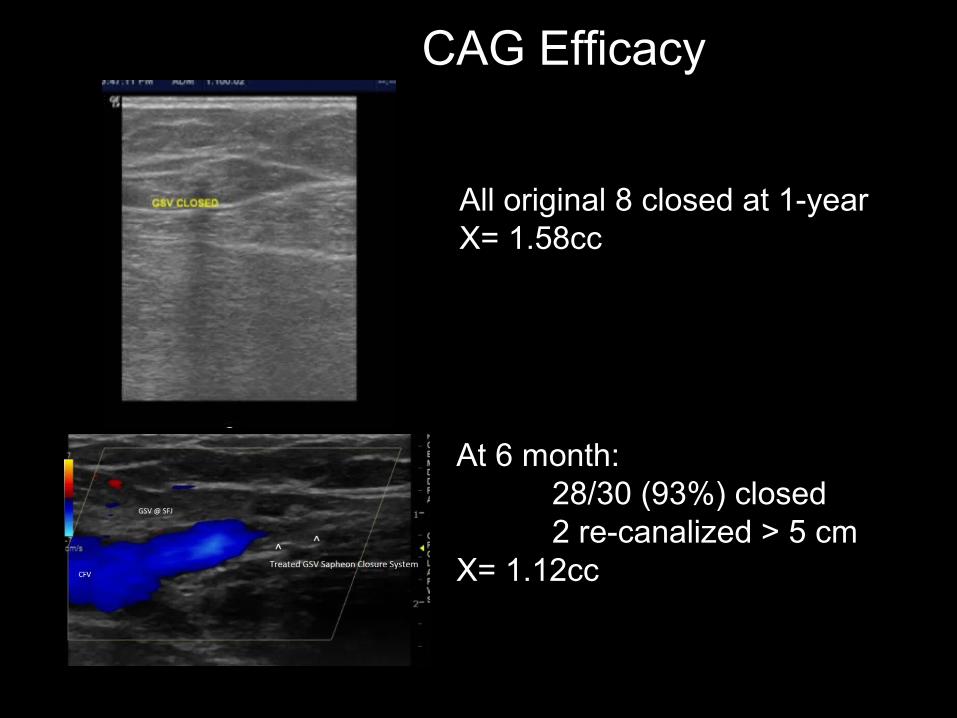
DR 30At 6 month:
28/30 (93%) closed 2 re-canalized > 5 cm
X= 1.12cc
DR 8All original 8 closed at 1-yearX= 1.58cc
CAG Efficacy
Almeida JI, AVF 2012
CAG: Recent Results
• 38 pts.• No compression/No tumescence• 1° Endpoint – safety/efficacy • 2° Endpoint – adverse events/VCSS change
Almeida JI, Javier JJ, Mackay E et al. First human use of cyanoacrylate adhesive for treatment of saphenous veinincompetence. J Vasc Surg:Venous and Lym Dis 2013;1:174-80.
Results
• 1 year – 92% occlusion
• Volume – 1.3 ml.
• Phlebitis – 15%
• Thrombus extension – 21% (self limited) (5 cm back now)
• VCSS – 6.1 to 1.5
Most Recent Results: European Multicenter Study
• 70 GSV – No tumescence – No compression
• 7 Centers
• 94% occlusion at 6 months
• VCSS – 4.3 to 1.3
Proebstle T et al. One year follow up of the European Multicenter Study oncyanoacrylate embolization of incompetent great saphenous veins. UIP 2013.
• Pharmaceutical-grade microfoam has been under development in Europe and the US for >12 years.
• Microfoam and the deliberate injection of gas into the venous circulation has presented unique challenges in demonstrating fundamental safety.
• A proprietary company has provided the experimental and trial data to answer important questions in relation to their specific microfoam O2, CO2, and trace N2
PEM: NTNT
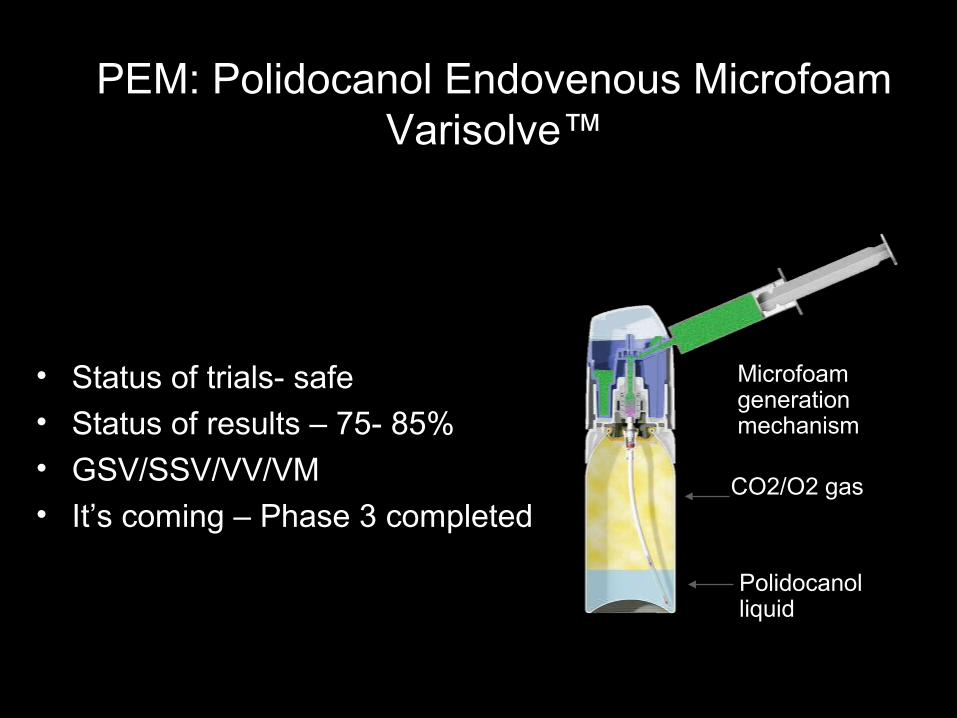
PEM: Polidocanol Endovenous MicrofoamVarisolve™
• Status of trials- safe• Status of results – 75- 85%
• GSV/SSV/VV/VM
• It’s coming – Phase 3 completed
Polidocanol liquid
CO2/O2 gas
Microfoam generation mechanism
PEM: Phase 3 Clinical TrialVANISH II
• 235 pts. – PLD .125%, .5%, 1% (176 pts.) – Placebo (59 pts.)
• PLD – 85% occlusion SFJ or GSV at 1 year
• Placebo – 20%
• Primary endpoint – pt. reported outcomes (VV SymQ) FDA approved QoL measure
Primary Endpoint: VV SymQ Patient reported outcome for symptoms
Secondary Endpoints: PA-V3 Patient reported assessment of varicose vein appearance
IPR-V3 Independent physician photographic assessment of appearance (Both endpoints are new and have been developed to most recent FDA standards and outcome tested for clinically meaningfulness.)
Tertiary endpoint : Duplex closure (regarded as a surrogate endpoint )
• Vanish 1 9.23 -5.44 (SE 0.29) 59% ↓p<0.0001
• Vanish 2 8.67 -5.53 (SE 0.33) 64% ↓p<0.0001
VV Sym Q: Symptoms
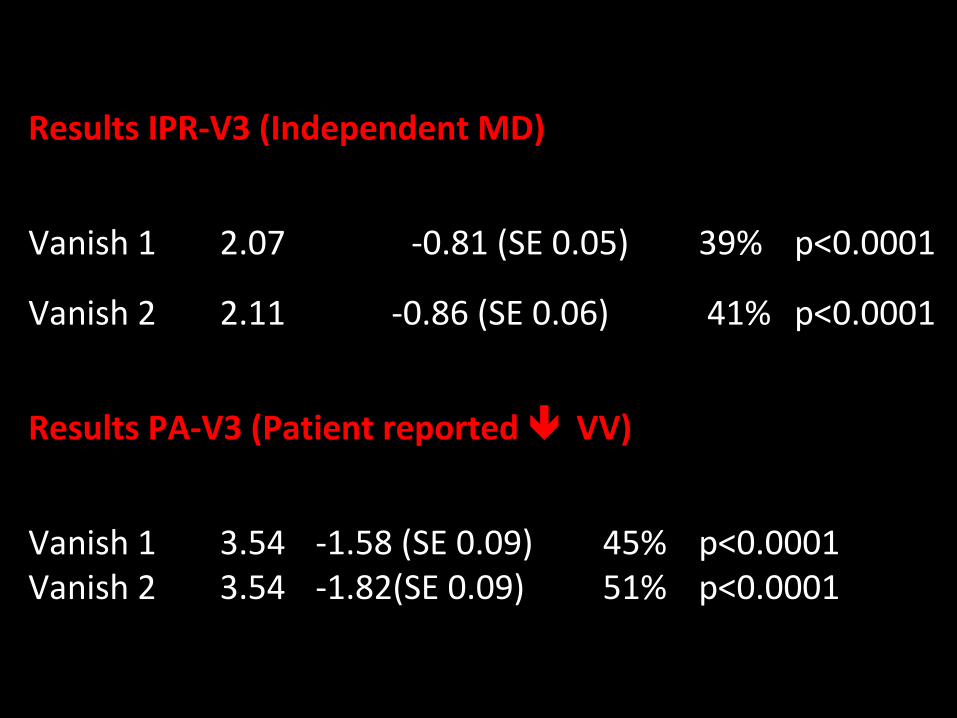
Results IPR-V3 (Independent MD)
Vanish 1 2.07 -0.81 (SE 0.05) 39% p<0.0001
Vanish 2 2.11 -0.86 (SE 0.06) 41% p<0.0001
Results PA-V3 (Patient reported VV)
Vanish 1 3.54 -1.58 (SE 0.09) 45% p<0.0001Vanish 2 3.54 -1.82(SE 0.09) 51% p<0.0001
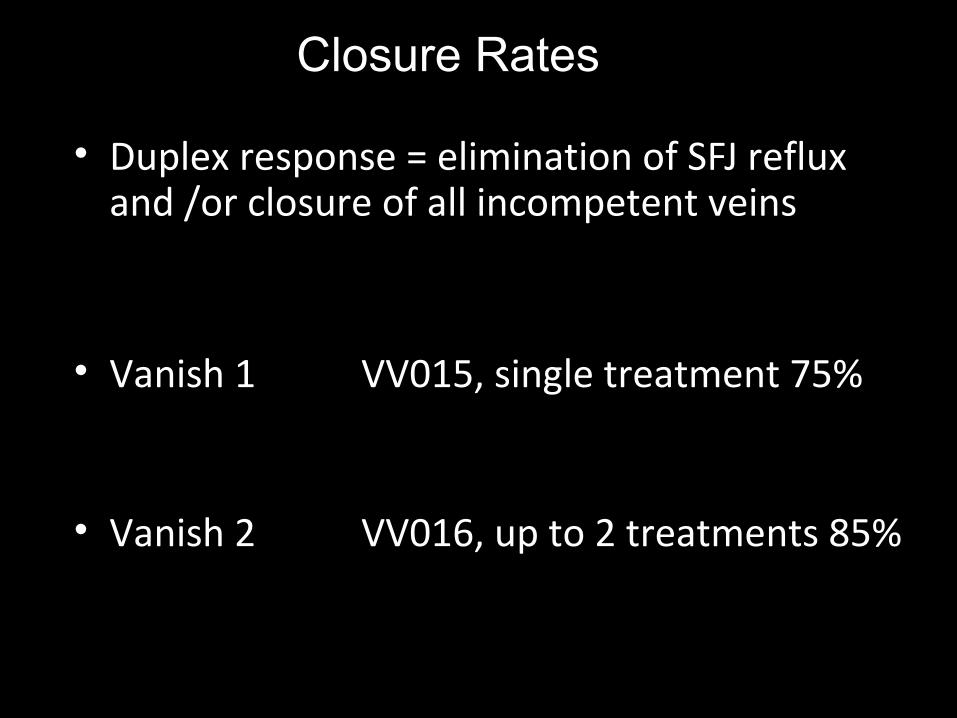
• Duplex response = elimination of SFJ reflux and /or closure of all incompetent veins
• Vanish 1 VV015, single treatment 75%
• Vanish 2 VV016, up to 2 treatments 85%
Closure Rates
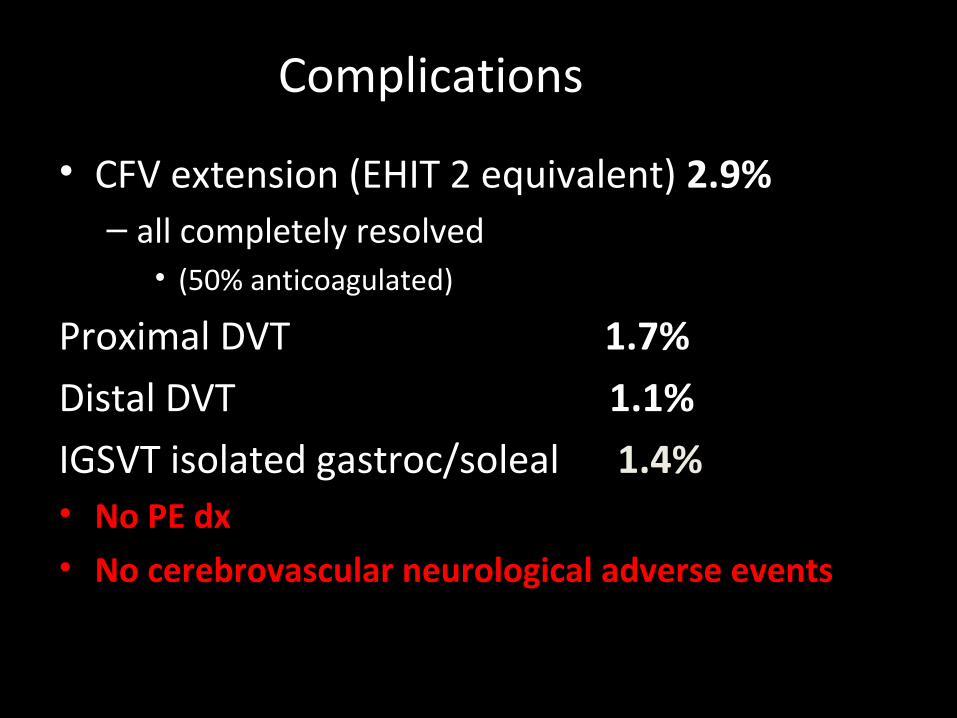
• CFV extension (EHIT 2 equivalent) 2.9%– all completely resolved
• (50% anticoagulated)
Proximal DVT 1.7%
Distal DVT 1.1%
IGSVT isolated gastroc/soleal 1.4%• No PE dx• No cerebrovascular neurological adverse events
Complications

MOCA:NTNT

Position: Wire 1 cm SFJ
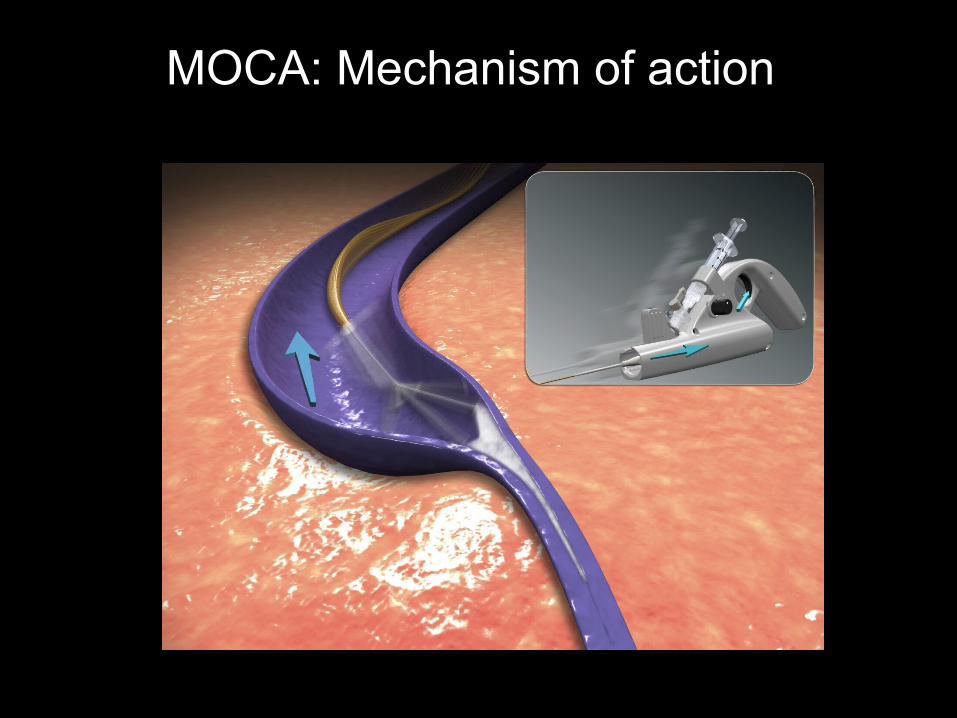
MOCA: Mechanism of action
Elias FIM: Clinical Trial 2/09*
• 30 limbs• GSV only (no SSV, VV, IPV)• 1 yr. follow up to complete trial• No tumescence or sedation
*Elias S, Raines JK. Mechanochemical tumescentless endovenous ablation: final results of the initial clinical trial.Phlebology 2012;27:67-72.
Completed Trial and Non Trial*
• All closed except 1st patient – btw 3-6mos
• 1 year – 29/30 (96%)
• 2 years– 27/28 (96%) ( 1 died, 1 lost F/U)
• >2 years non trial – 29/30 (96%) (random pts.) *Elias S, Lam YL, Wittens CHA. Mechanochemicalablation: status and results. Phlebology 2013 Supp. 1:28;10-14. .
CComplications
• No DVT
• No nerve injury
• No skin injury
• Bruising 3 pts. - 2° caught on vein wall

GSV Results: Dutch series
• 224 GSV’s
• 6 weeks – 182/185 (98% closed)
• 6 months – 40/42 (95% closed)
• No nerve/ skin injury/ DVT
Ramon RJP, van Eekeren MD et al. Endovenous mechanochemical ablation ofgreat saphenous vein incompetence using the ClariVein device: a safety study.J Endovasc Ther 2011; 18:328-334.
SSV: 50 pts
• 1 yr. – 94% occlusion
• VCSS – 3 to 1
• No DVT, no nerve injury
Boersma D, van Eekeren RRJP, Werson DAB, et al.Mechanochemical endovenous ablation of smallsaphenous vein insufficiency using the ClariVeindevice: One-year results of a prospective series. EJVES2012.
MOCA vs. RF
MOCA• 14 day pain – 8.6 (100)
• RTW – 3.3 days
• RT Activity – 1.2 days
• QoL - equal
RF• 14 day pain – 14.8 (100)
• RTW – 5.6 days
• RT Activity – 2.8 days
• QoL - equal
van Eekeren et al. Postoperative pain and early quality of life after radiofrequency ablation and mechanochemical endovenousablation of incompetent great saphenous veins. J VascSurg 2012.
MOCA:Contraindications
• GSV/SSV – post SVT
• Synechiae – can place but wire snags
• Large veins - >15mm. (19mm)
Summary: MOCA
• 15,000 cases worldwide (GSV/SSV/AAGSV)• > 90% occlusion rate – various intervals• QoL – improves as any successful EVA• DVT - < 1% worldwide• No nerve injury
V Block
• NTNT
• Endovenous SFJ ligation
• Dual syringe system to deliver sclerosant
• Results pending
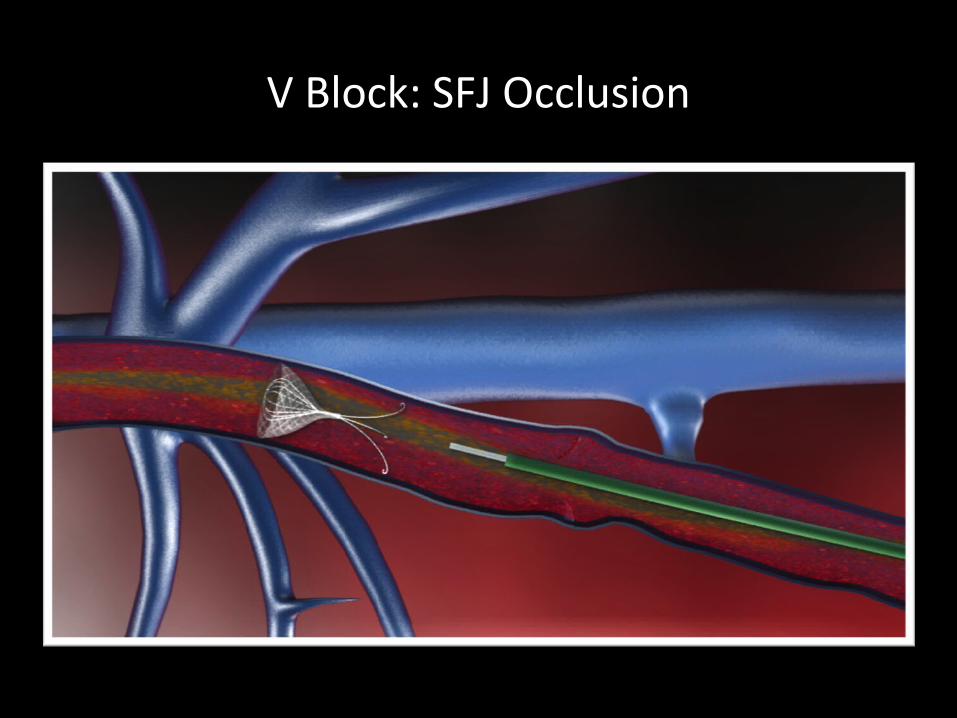
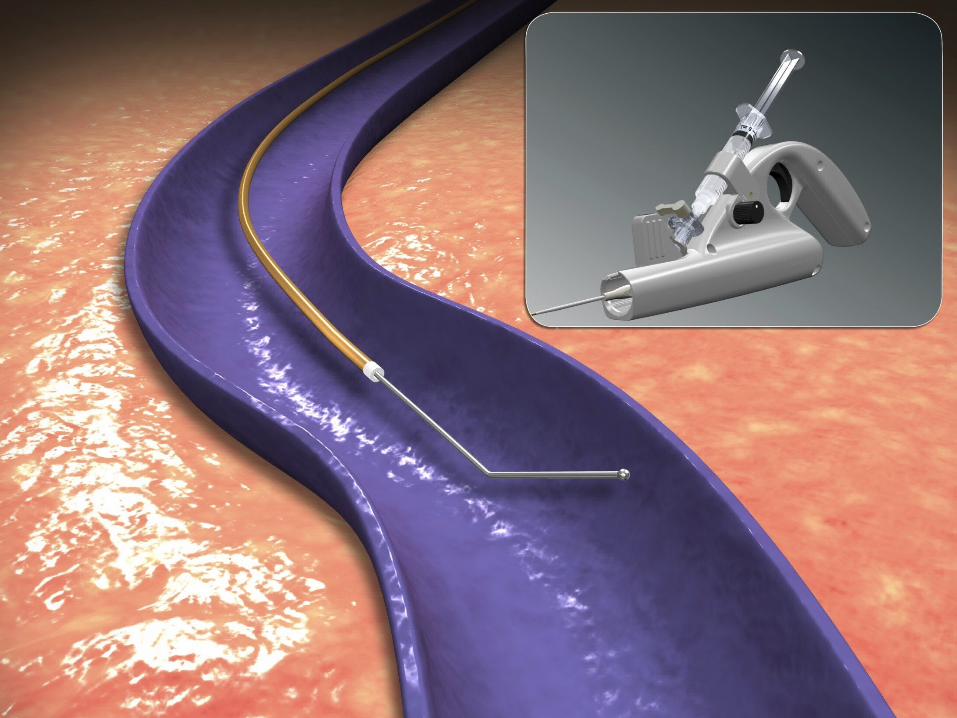
V Block: SFJ Occlusion
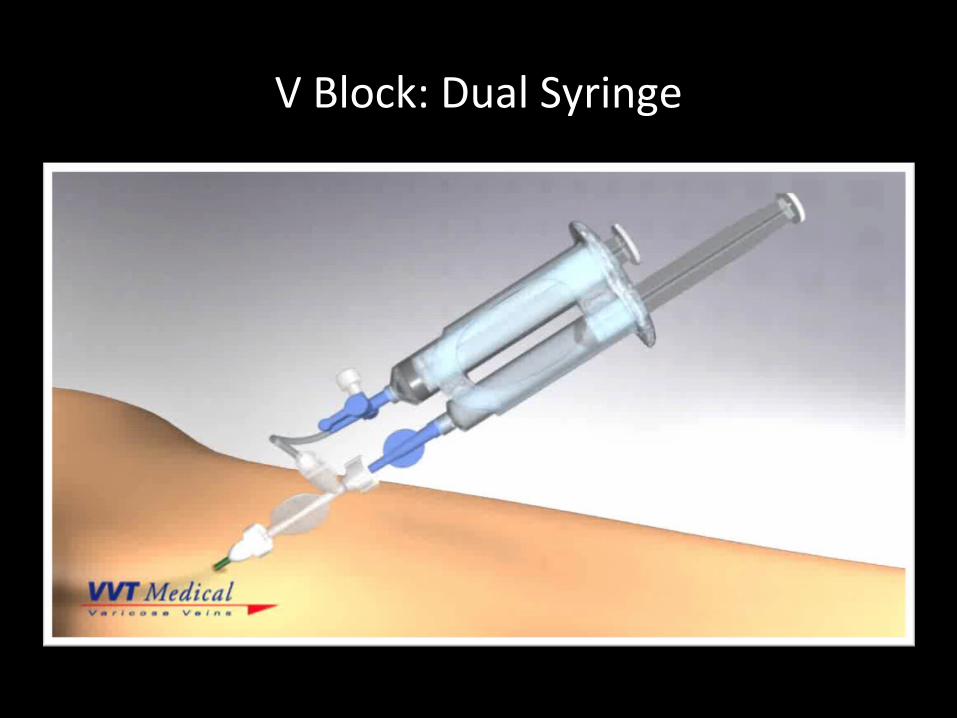
V Block: Dual Syringe
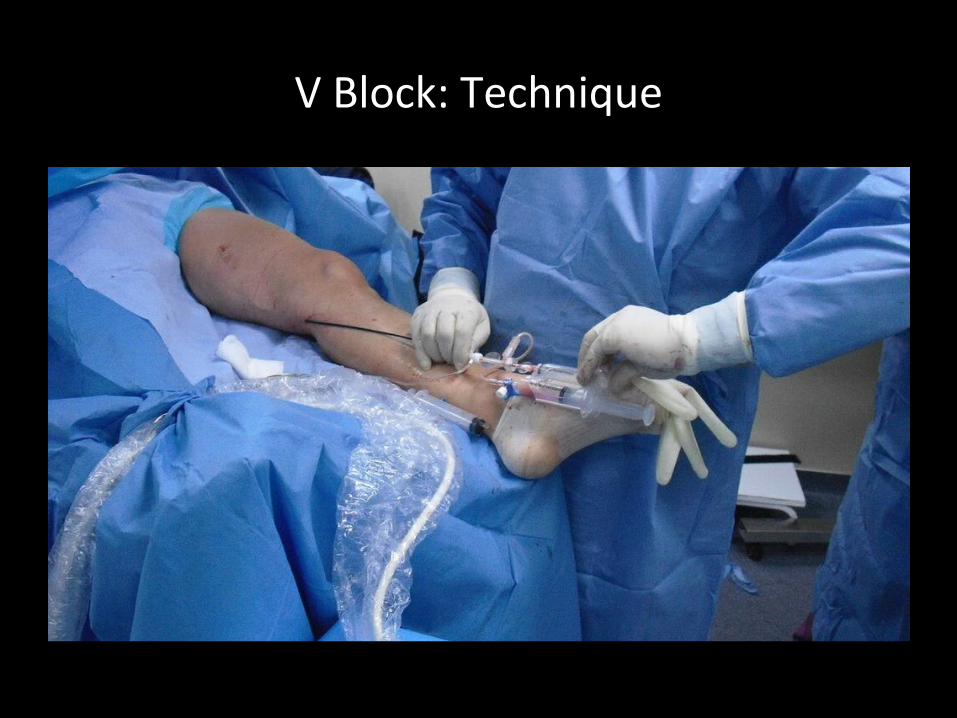
V Block: Technique
V Block: US Post insertion
NTNT: Special Considerations
• SSV, BK GSV, suprafascial – can go to malleolus
• C5 –C6 – retrograde tumescence hard to place
• Minimal nerve/skin injury
Summary: NTNT
• MOCA – 96% (>2yr)
• CAG – 93% (1yr)
• PEM – 85% (1yr)
• V Block – await results
Steam: TT
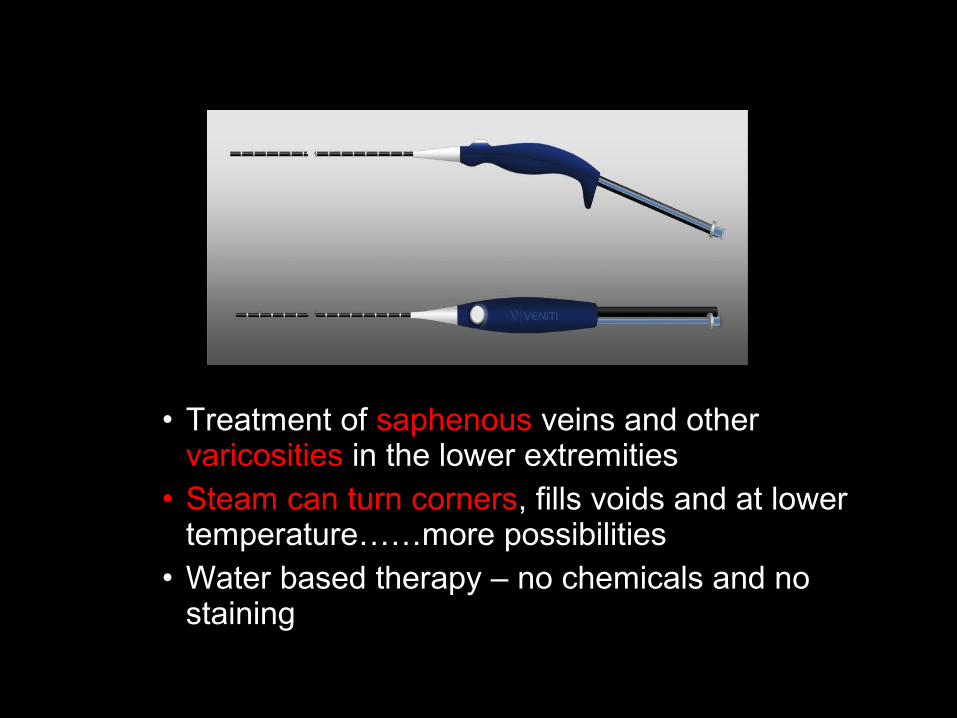
• Treatment of saphenous veins and other varicosities in the lower extremities
• Steam can turn corners, fills voids and at lower temperature……more possibilities
• Water based therapy – no chemicals and no staining
•SVS steam catheter (1.2 mm) -50% smaller than RFA (2.3 mm)
GSV, SSV, varicose veins, recurrences and venous malformations
Steam Catheter: TT
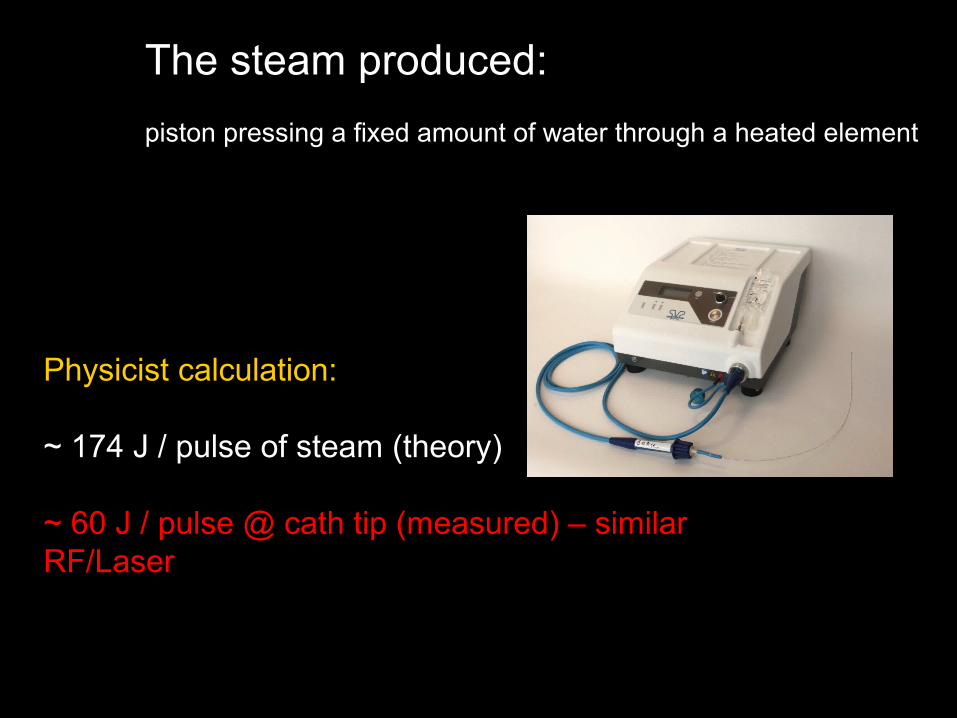
Physicist calculation:
~ 174 J / pulse of steam (theory)
~ 60 J / pulse @ cath tip (measured) – similar RF/Laser
The steam produced:
piston pressing a fixed amount of water through a heated element
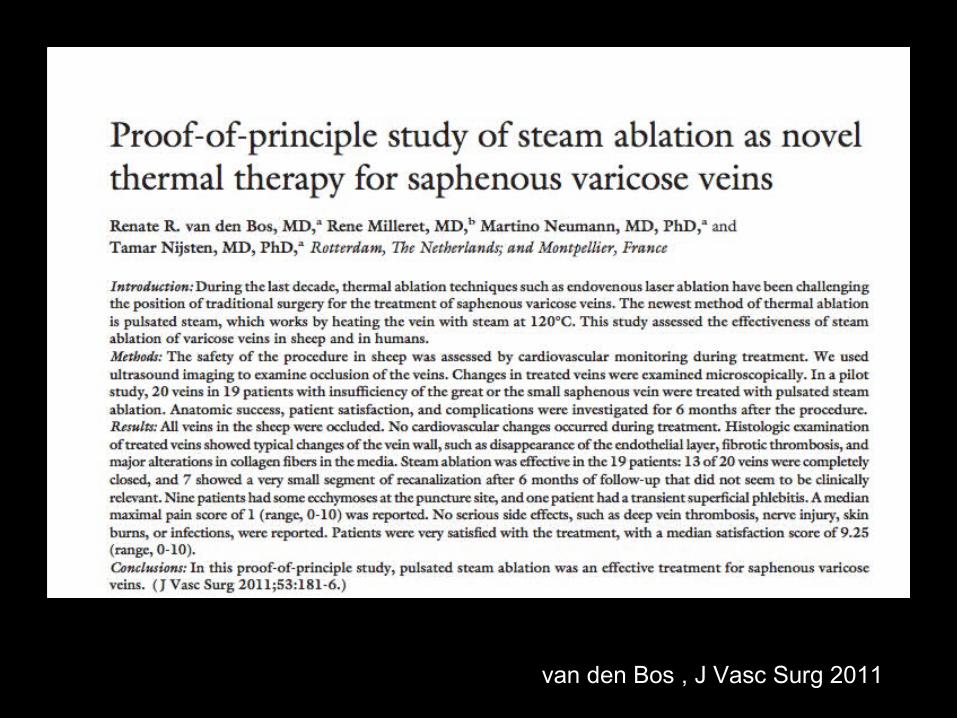
van den Bos , J Vasc Surg 2011
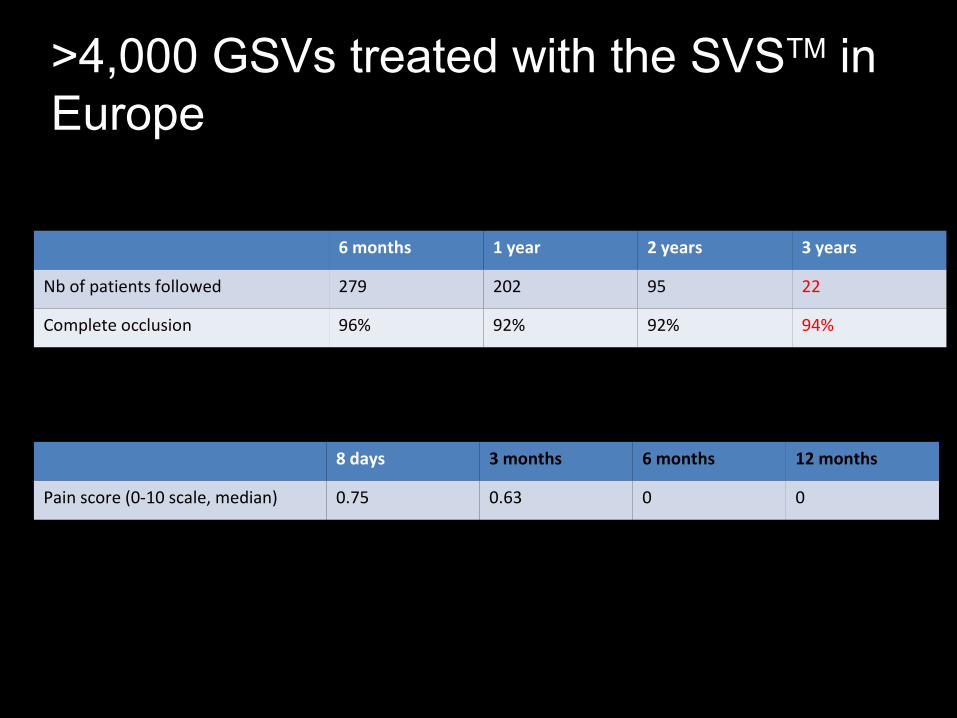
6 months 1 year 2 years 3 years
Nb of patients followed 279 202 95 22
Complete occlusion 96% 92% 92% 94%
8 days 3 months 6 months 12 months
Pain score (0-10 scale, median) 0.75 0.63 0 0
>4,000 GSVs treated with the SVSTM in Europe
NTNT vs. TT:Eliminating Tumescence Is The Future
•TT (Steam) – VV advantage (not GSV/SSV)•NTNT – nerve/skin risk less/patient comfort•Treat to malleolus/SSV•C5, C6 – tumescence difficult in lower leg•More complete treatment?•NTNT – The future (probably for 95% of GSV)
THE END
• All new technologies need to impact QoL
• Simplify procedure = better for pt. and MD
• Current new technology: eliminate tumescence
• Future new technology: completely non invasive
Vein disease is an incurable disease