Embed Size (px)
Citation preview
NEGLECTED TROPICAL DISEASES CONTROL PROGRAM
STRATEGIC COMMUNICATION FOR PREVENTION AND CONTROL
2012-2017
2
Table of Content Strategy Summary ........................................................................................................................................ 3
1. BACKGROUND INFORMATION ......................................................................................................... 4
1.1 NTD in Tanzania: Burden of Diseases ......................................................................................... 4
1.2 NTD Strategic Plan (2012-2017) Vision, Mission and Goal ........................................................ 6
1.2.1 Vision .......................................................................................................................................... 6
1.2.2 Mission ........................................................................................................................................ 6
1.2.3 Goal ............................................................................................................................................. 6
1.3 Strategic Priorities and Objectives ..................................................................................................... 7
2. STRATEGIC COMMUNICATION FOR NTD CONTROL ................................................................... 8
2.1 BCC Strategy Goal and Objectives .................................................................................................... 8
2.1.1 Goal ............................................................................................................................................. 8
2.1.2 Objectives ............................................................................................................................. 8
2.2 Understanding the audience ............................................................................................................... 8
3. GENERIC MESSAGES AND SUGGESTED STRATEGIES ................................................................ 9
3.1 Sanitation and Hygiene messages and suggested strategies ............................................................. 10
3.2 Advocacy and Behavior Change ...................................................................................................... 12
4. DESCRIPTION OF STRATEGIES ....................................................................................................... 14
5. VISUALS AND TRAINING MANUALS ............................................................................................ 15
6. MONITORING AND EVALUATION PLAN ...................................................................................... 15
3
Strategy Summary Situation Analysis
Purpose Enhancing knowledge and intensify community engagement in prevention and control of NTD
Health Issue Presence of parasitic infections that are widespread in the country Context Strengthen advocacy, visibility and profile of NTD control initiative
Desired Change Enhanced knowledge, changed attitude and practice with regard to NTDs prevention and control/elimination
Communication strategy
Audience Primary: Children, communities (both men and women) Secondary: Health workers, community leaders, policy makers and media
Behavioral Objectives To increase knowledge, skills, practice related to prevention and control/elimination of NTDs and adherence/compliance to MDA
Strategic approach Focused on interpersonal communication (IPC); mass media (radio, TV); folk media; outdoor branding; social networks
Key messages Focus – sanitation and hygiene, MDA Channel and tools IPC, print materials, visual & audio Management of the strategy Timeline 2012 to 2017 Monitoring and Evaluation Tracking results Progress monitoring, annual monitoring, outcome measure
4
1. BACKGROUND INFORMATION 1.1 NTD in Tanzania: Burden of Diseases
Neglected Tropical Diseases (NTDs) are a devastating burden for the people of Tanzania and are prevalent throughout the country, though certain areas of the country face more severe burdens than others due to geographic and environmental conditions. The country is endemic with five preventive chemotherapy diseases namely, Schistosomiasis, Lymphatic Filariasis, Onchocerciasis, Trachoma, and the soil-transmitted helminths (Hookworm, Ascariasis, And Trichuriasis). Such high prevalence rates of multiple NTDs increase the risk for co-infection with two or more diseases, a phenomenon that leads to more severe health consequences. Mothers and children are disproportionately affected by NTDs, leading to increased maternal morbidity and mortality, poor pregnancy outcomes, and impairment of childhood development. NTDs also exacerbate under-nutrition, a condition affecting the majority of children in the developing world. The nutritional losses caused by NTDs result in 1 in 3 Tanzanian children being underweight for their age and almost 1 in 2 suffering obviously stunted growth.
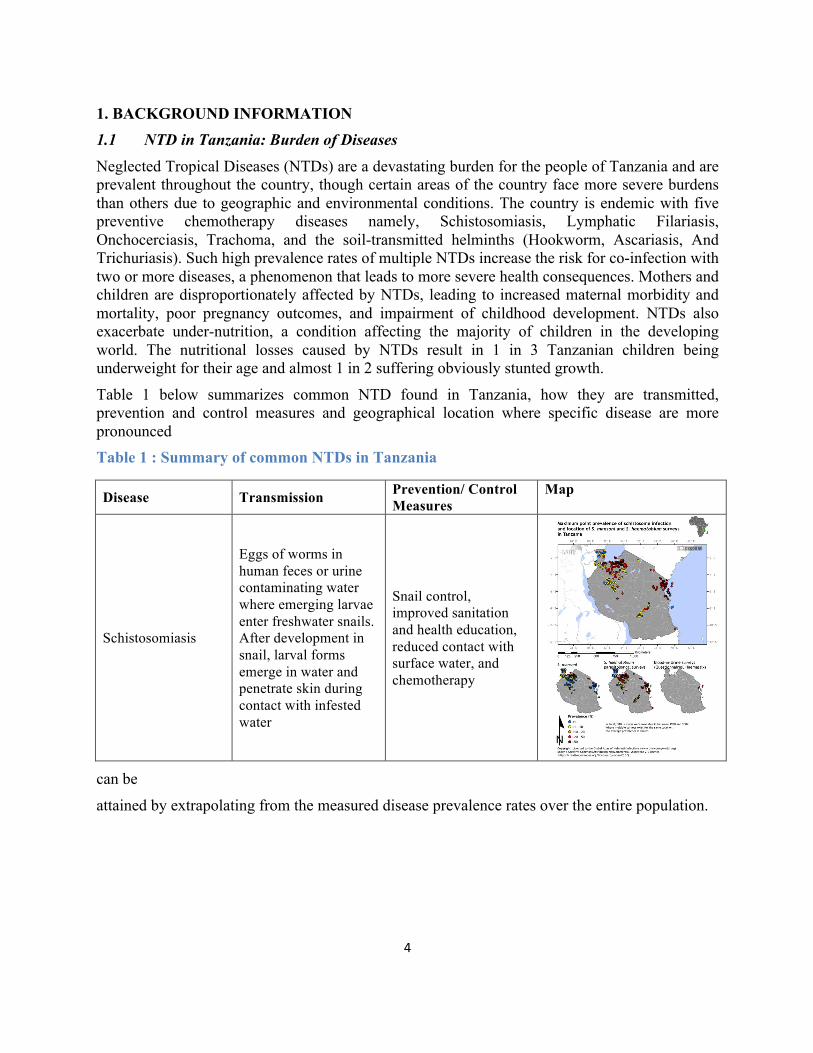
Table 1 below summarizes common NTD found in Tanzania, how they are transmitted, prevention and control measures and geographical location where specific disease are more pronounced Table 1 : Summary of common NTDs in Tanzania
Disease Transmission Prevention/ Control Measures
Map
Schistosomiasis
Eggs of worms in human feces or urine contaminating water where emerging larvae enter freshwater snails. After development in snail, larval forms emerge in water and penetrate skin during contact with infested water
Snail control, improved sanitation and health education, reduced contact with surface water, and chemotherapy
can be
attained by extrapolating from the measured disease prevalence rates over the entire population.
5
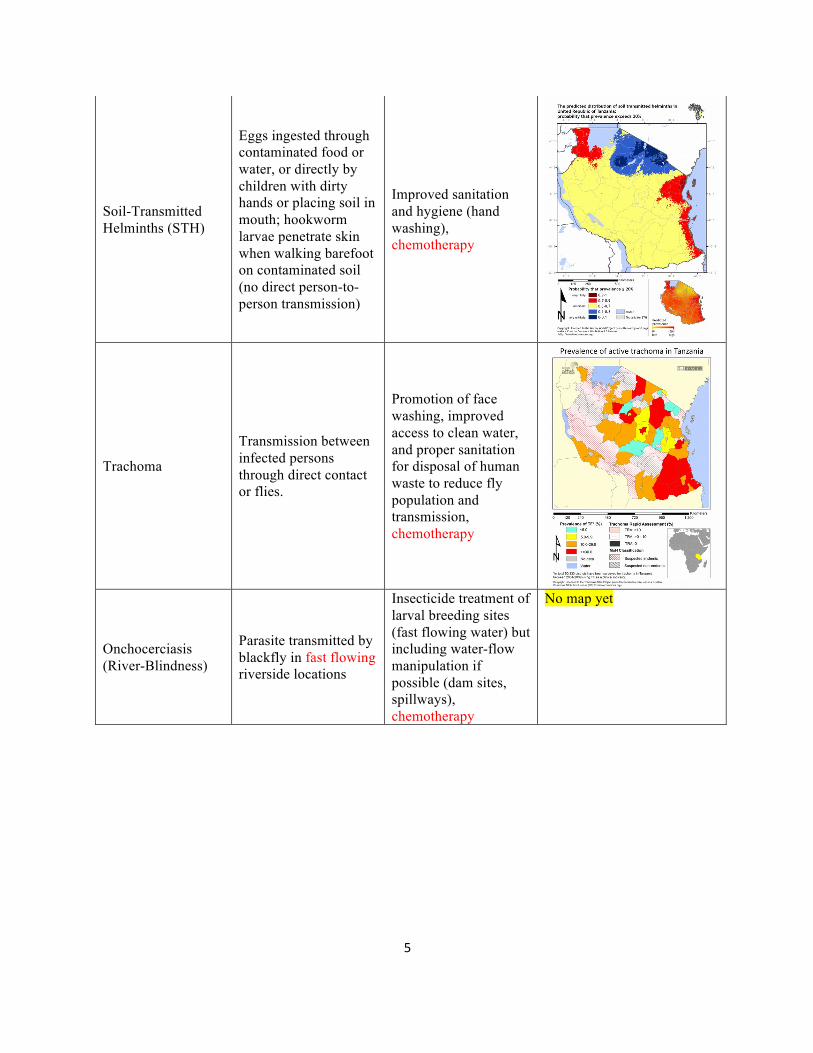
Soil-Transmitted Helminths (STH)
Eggs ingested through contaminated food or water, or directly by children with dirty hands or placing soil in mouth; hookworm larvae penetrate skin when walking barefoot on contaminated soil (no direct person-to-person transmission)
Improved sanitation and hygiene (hand washing), chemotherapy
Trachoma
Transmission between infected persons through direct contact or flies.
Promotion of face washing, improved access to clean water, and proper sanitation for disposal of human waste to reduce fly population and transmission, chemotherapy
Onchocerciasis (River-Blindness)
Parasite transmitted by blackfly in fast flowing riverside locations
Insecticide treatment of larval breeding sites (fast flowing water) but including water-flow manipulation if possible (dam sites, spillways), chemotherapy
No map yet
6
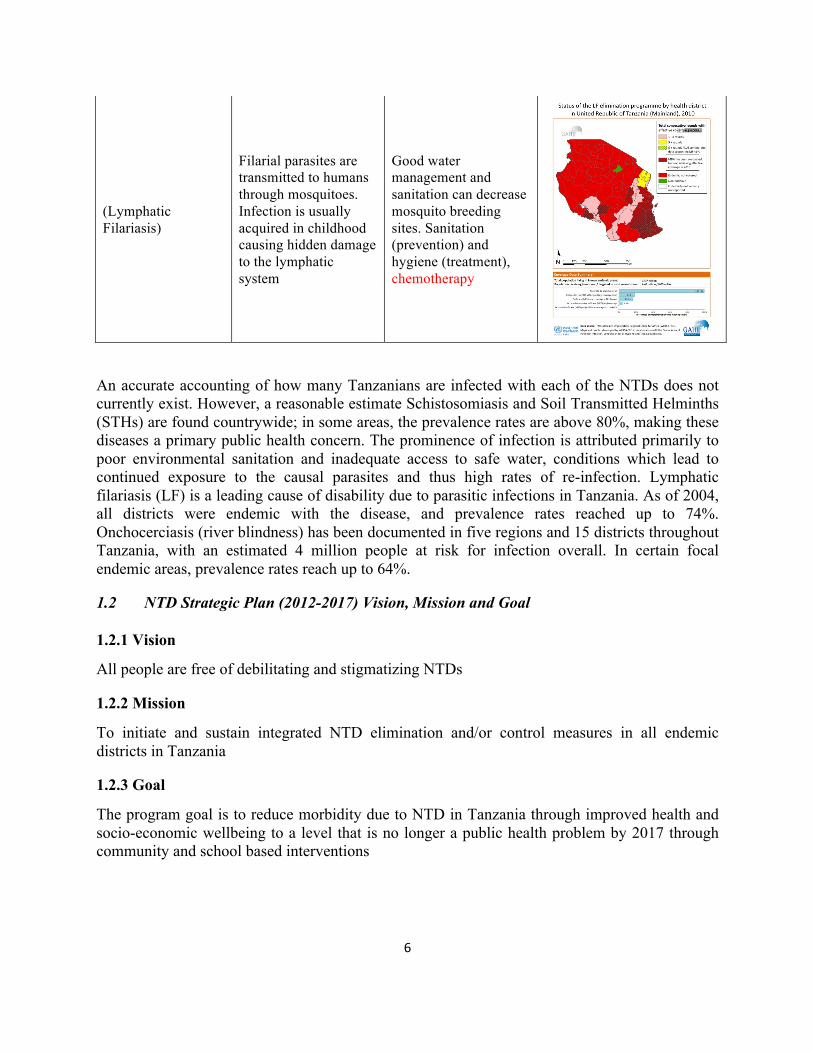
(Lymphatic Filariasis)
Filarial parasites are transmitted to humans through mosquitoes. Infection is usually acquired in childhood causing hidden damage to the lymphatic system
Good water management and sanitation can decrease mosquito breeding sites. Sanitation (prevention) and hygiene (treatment), chemotherapy
An accurate accounting of how many Tanzanians are infected with each of the NTDs does not currently exist. However, a reasonable estimate Schistosomiasis and Soil Transmitted Helminths (STHs) are found countrywide; in some areas, the prevalence rates are above 80%, making these diseases a primary public health concern. The prominence of infection is attributed primarily to poor environmental sanitation and inadequate access to safe water, conditions which lead to continued exposure to the causal parasites and thus high rates of re-infection. Lymphatic filariasis (LF) is a leading cause of disability due to parasitic infections in Tanzania. As of 2004, all districts were endemic with the disease, and prevalence rates reached up to 74%. Onchocerciasis (river blindness) has been documented in five regions and 15 districts throughout Tanzania, with an estimated 4 million people at risk for infection overall. In certain focal endemic areas, prevalence rates reach up to 64%.
1.2 NTD Strategic Plan (2012-2017) Vision, Mission and Goal
1.2.1 Vision
All people are free of debilitating and stigmatizing NTDs
1.2.2 Mission
To initiate and sustain integrated NTD elimination and/or control measures in all endemic districts in Tanzania
1.2.3 Goal
The program goal is to reduce morbidity due to NTD in Tanzania through improved health and socio-economic wellbeing to a level that is no longer a public health problem by 2017 through community and school based interventions
7
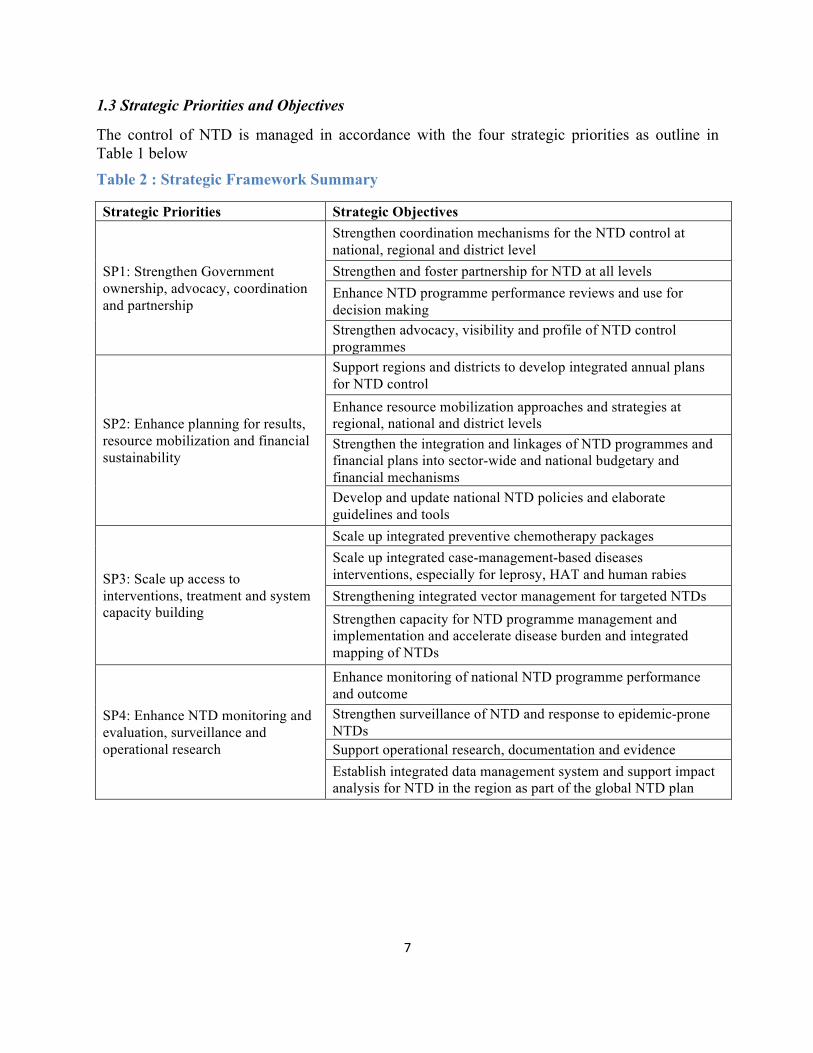
1.3 Strategic Priorities and Objectives
The control of NTD is managed in accordance with the four strategic priorities as outline in Table 1 below Table 2 : Strategic Framework Summary
Strategic Priorities Strategic Objectives
SP1: Strengthen Government ownership, advocacy, coordination and partnership
Strengthen coordination mechanisms for the NTD control at national, regional and district level Strengthen and foster partnership for NTD at all levels Enhance NTD programme performance reviews and use for decision making Strengthen advocacy, visibility and profile of NTD control programmes
SP2: Enhance planning for results, resource mobilization and financial sustainability
Support regions and districts to develop integrated annual plans for NTD control Enhance resource mobilization approaches and strategies at regional, national and district levels Strengthen the integration and linkages of NTD programmes and financial plans into sector-wide and national budgetary and financial mechanisms Develop and update national NTD policies and elaborate guidelines and tools
SP3: Scale up access to interventions, treatment and system capacity building
Scale up integrated preventive chemotherapy packages Scale up integrated case-management-based diseases interventions, especially for leprosy, HAT and human rabies Strengthening integrated vector management for targeted NTDs Strengthen capacity for NTD programme management and implementation and accelerate disease burden and integrated mapping of NTDs
SP4: Enhance NTD monitoring and evaluation, surveillance and operational research
Enhance monitoring of national NTD programme performance and outcome Strengthen surveillance of NTD and response to epidemic-prone NTDs Support operational research, documentation and evidence Establish integrated data management system and support impact analysis for NTD in the region as part of the global NTD plan
8
2. STRATEGIC COMMUNICATION FOR NTD CONTROL
2.1 BCC Strategy Goal and Objectives
2.1.1 Goal
In line with NTD Strategic Master Plan (2012 - 2017), the goal of the BCC strategy is to provide a framework for guiding NTD BCC actors and implementing partners for a well coordinated and sustained communication for strengthened advocacy, visibility and profile of NTD control programmes as well as creating awareness about NTD in Tanzania.
2.1.2 Objectives
1. To guide advocacy efforts aimed at political leaders, decision makers, private sector partners and community leaders in order to raise NTD profile and ensure increased resource allocation at all levels.
2. To ensure consistent and standardized messages among all partners in NTD interventions. 3. To provide a framework to guide the development and implementation of strategic,
evidence-based BCC interventions. 4. To create platform and forum for BCC partners to harmonize and coordinate NTD BCC
activities implemented by different partners in Tanzania
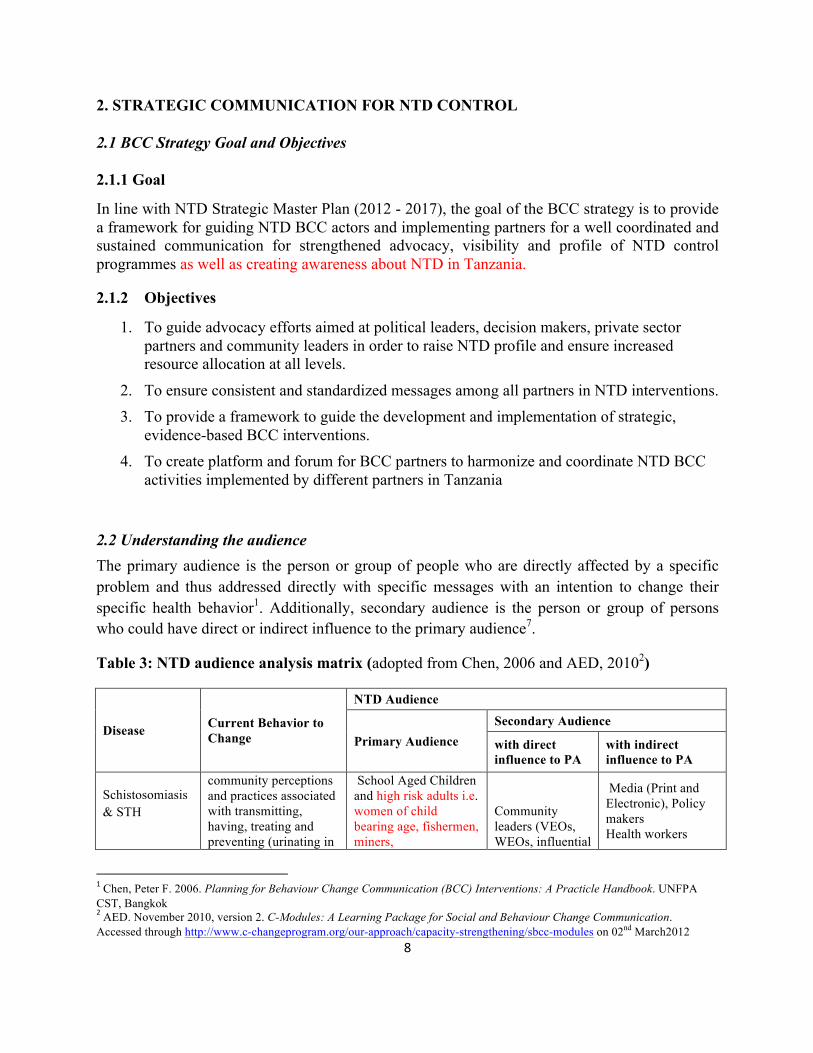
2.2 Understanding the audience The primary audience is the person or group of people who are directly affected by a specific problem and thus addressed directly with specific messages with an intention to change their specific health behavior1. Additionally, secondary audience is the person or group of persons who could have direct or indirect influence to the primary audience7.
Table 3: NTD audience analysis matrix (adopted from Chen, 2006 and AED, 20102)
Disease Current Behavior to Change
NTD Audience
Primary Audience Secondary Audience
with direct influence to PA
with indirect influence to PA
Schistosomiasis & STH
community perceptions and practices associated with transmitting, having, treating and preventing (urinating in
School Aged Children and high risk adults i.e. women of child bearing age, fishermen, miners,
Community leaders (VEOs, WEOs, influential
Media (Print and Electronic), Policy makers Health workers
1 Chen, Peter F. 2006. Planning for Behaviour Change Communication (BCC) Interventions: A Practicle Handbook. UNFPA CST, Bangkok 2 AED. November 2010, version 2. C-Modules: A Learning Package for Social and Behaviour Change Communication. Accessed through http://www.c-changeprogram.org/our-approach/capacity-strengthening/sbcc-modules on 02nd March2012
9
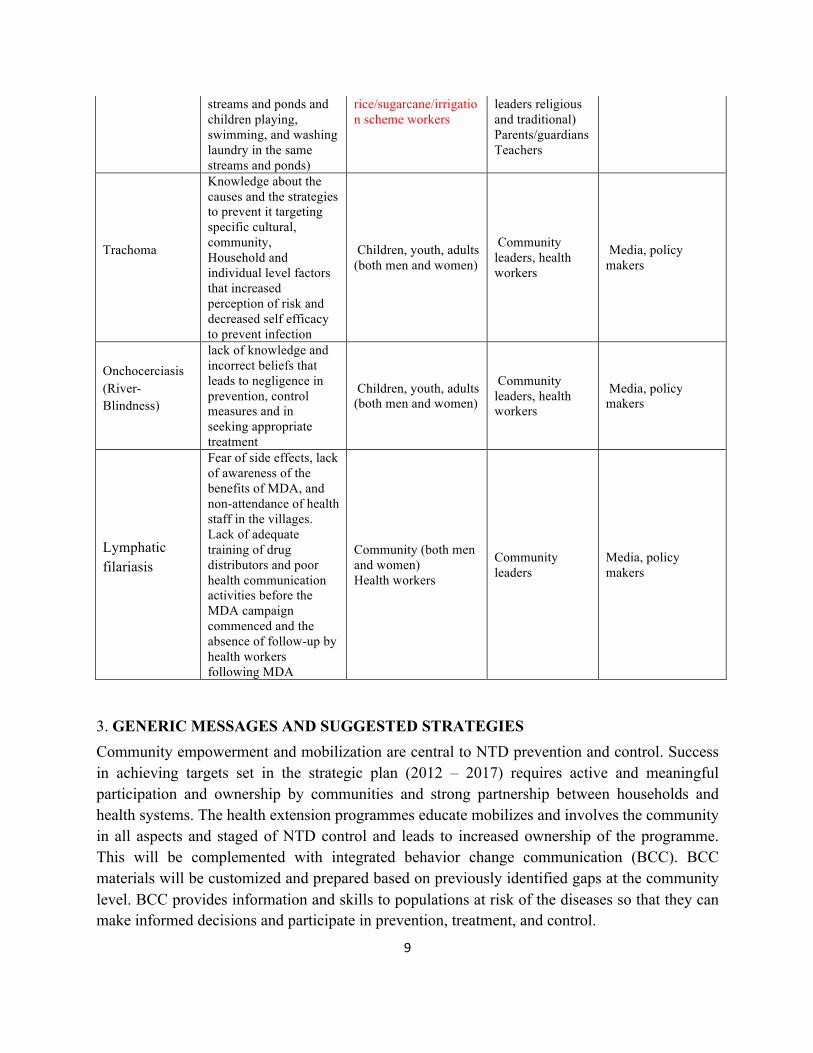
streams and ponds and children playing, swimming, and washing laundry in the same streams and ponds)
rice/sugarcane/irrigation scheme workers
leaders religious and traditional) Parents/guardians Teachers
Trachoma
Knowledge about the causes and the strategies to prevent it targeting specific cultural, community, Household and individual level factors that increased perception of risk and decreased self efficacy to prevent infection
Children, youth, adults (both men and women)
Community leaders, health workers
Media, policy makers
Onchocerciasis (River-Blindness)
lack of knowledge and incorrect beliefs that leads to negligence in prevention, control measures and in seeking appropriate treatment
Children, youth, adults (both men and women)
Community leaders, health workers
Media, policy makers
Lymphatic filariasis
Fear of side effects, lack of awareness of the benefits of MDA, and non-attendance of health staff in the villages. Lack of adequate training of drug distributors and poor health communication activities before the MDA campaign commenced and the absence of follow-up by health workers following MDA
Community (both men and women) Health workers
Community leaders
Media, policy makers
3. GENERIC MESSAGES AND SUGGESTED STRATEGIES Community empowerment and mobilization are central to NTD prevention and control. Success in achieving targets set in the strategic plan (2012 – 2017) requires active and meaningful participation and ownership by communities and strong partnership between households and health systems. The health extension programmes educate mobilizes and involves the community in all aspects and staged of NTD control and leads to increased ownership of the programme. This will be complemented with integrated behavior change communication (BCC). BCC materials will be customized and prepared based on previously identified gaps at the community level. BCC provides information and skills to populations at risk of the diseases so that they can make informed decisions and participate in prevention, treatment, and control.
10
In particular, IEC/BCC raises community awareness about the signs and symptoms of the diseases, encourages early treatment-seeking behavior and treatment compliance, and creates demand for and increases the utilization of services. The overall goal of the BCC is to increase community understanding, mobilize resources and guarantee the sustainable results. This is done through a variety of media and channels including mass media (especially radio), interpersonal communication (especially from health extension workers), participatory communication (including community dialogue) and social mobilization (particularly during distribution campaigns).
This section shows behavior or generic message, target audience, additional information and arguments to convince people to adopt the recommended behavior, and suggested strategies to promote this behavior. The section is divided into two sub-sections, 1) focusing on NTDs whose main strategy is improvement of sanitation and hygiene infrastructure and appropriate health-seeking behavior and 2) focus on advocacy and behavior change
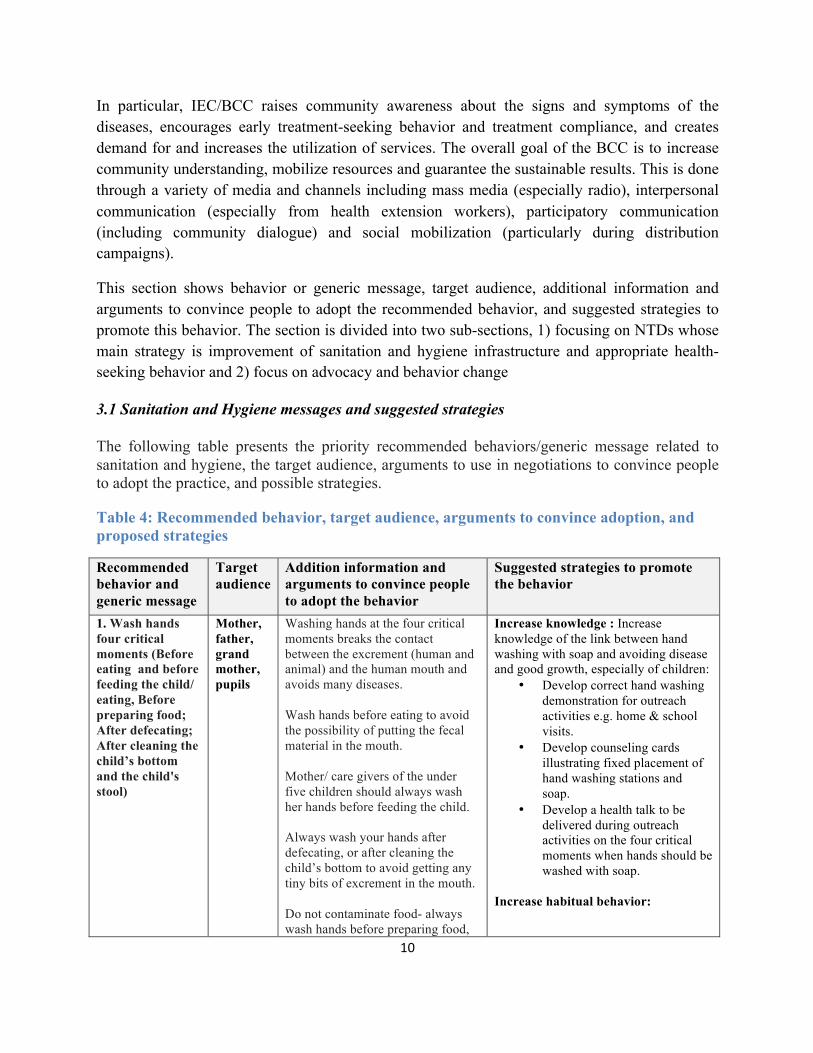
3.1 Sanitation and Hygiene messages and suggested strategies
The following table presents the priority recommended behaviors/generic message related to sanitation and hygiene, the target audience, arguments to use in negotiations to convince people to adopt the practice, and possible strategies.
Table 4: Recommended behavior, target audience, arguments to convince adoption, and proposed strategies
Recommended behavior and generic message
Target audience
Addition information and arguments to convince people to adopt the behavior
Suggested strategies to promote the behavior
1. Wash hands four critical moments (Before eating and before feeding the child/ eating, Before preparing food; After defecating; After cleaning the child’s bottom and the child's stool)
Mother, father, grand mother, pupils
Washing hands at the four critical moments breaks the contact between the excrement (human and animal) and the human mouth and avoids many diseases. Wash hands before eating to avoid the possibility of putting the fecal material in the mouth. Mother/ care givers of the under five children should always wash her hands before feeding the child. Always wash your hands after defecating, or after cleaning the child’s bottom to avoid getting any tiny bits of excrement in the mouth. Do not contaminate food- always wash hands before preparing food,
Increase knowledge : Increase knowledge of the link between hand washing with soap and avoiding disease and good growth, especially of children:
• Develop correct hand washing demonstration for outreach activities e.g. home & school visits.
• Develop counseling cards illustrating fixed placement of hand washing stations and soap.
• Develop a health talk to be delivered during outreach activities on the four critical moments when hands should be washed with soap.
Increase habitual behavior:
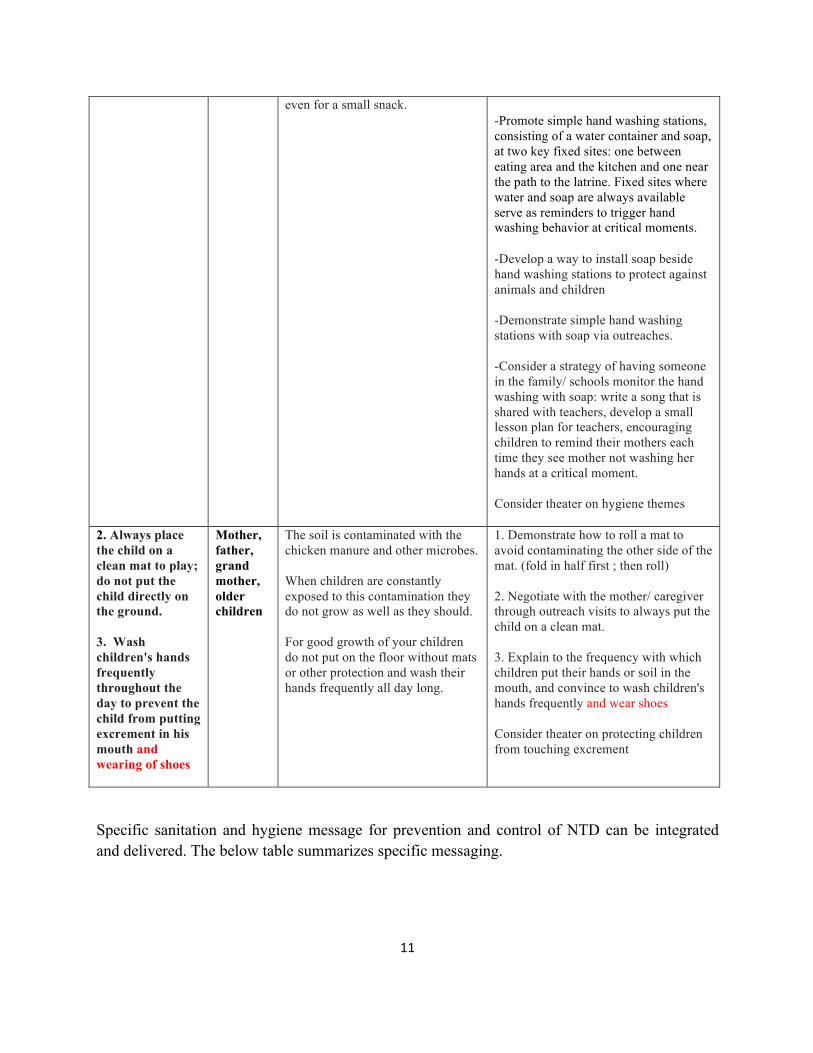
11
even for a small snack. -Promote simple hand washing stations,
consisting of a water container and soap, at two key fixed sites: one between eating area and the kitchen and one near the path to the latrine. Fixed sites where water and soap are always available serve as reminders to trigger hand washing behavior at critical moments.
-Develop a way to install soap beside hand washing stations to protect against animals and children -Demonstrate simple hand washing stations with soap via outreaches. -Consider a strategy of having someone in the family/ schools monitor the hand washing with soap: write a song that is shared with teachers, develop a small lesson plan for teachers, encouraging children to remind their mothers each time they see mother not washing her hands at a critical moment. Consider theater on hygiene themes
2. Always place the child on a clean mat to play; do not put the child directly on the ground. 3. Wash children's hands frequently throughout the day to prevent the child from putting excrement in his mouth and wearing of shoes
Mother, father, grand mother, older children
The soil is contaminated with the chicken manure and other microbes. When children are constantly exposed to this contamination they do not grow as well as they should. For good growth of your children do not put on the floor without mats or other protection and wash their hands frequently all day long.
1. Demonstrate how to roll a mat to avoid contaminating the other side of the mat. (fold in half first ; then roll) 2. Negotiate with the mother/ caregiver through outreach visits to always put the child on a clean mat. 3. Explain to the frequency with which children put their hands or soil in the mouth, and convince to wash children's hands frequently and wear shoes Consider theater on protecting children from touching excrement
Specific sanitation and hygiene message for prevention and control of NTD can be integrated and delivered. The below table summarizes specific messaging.
12
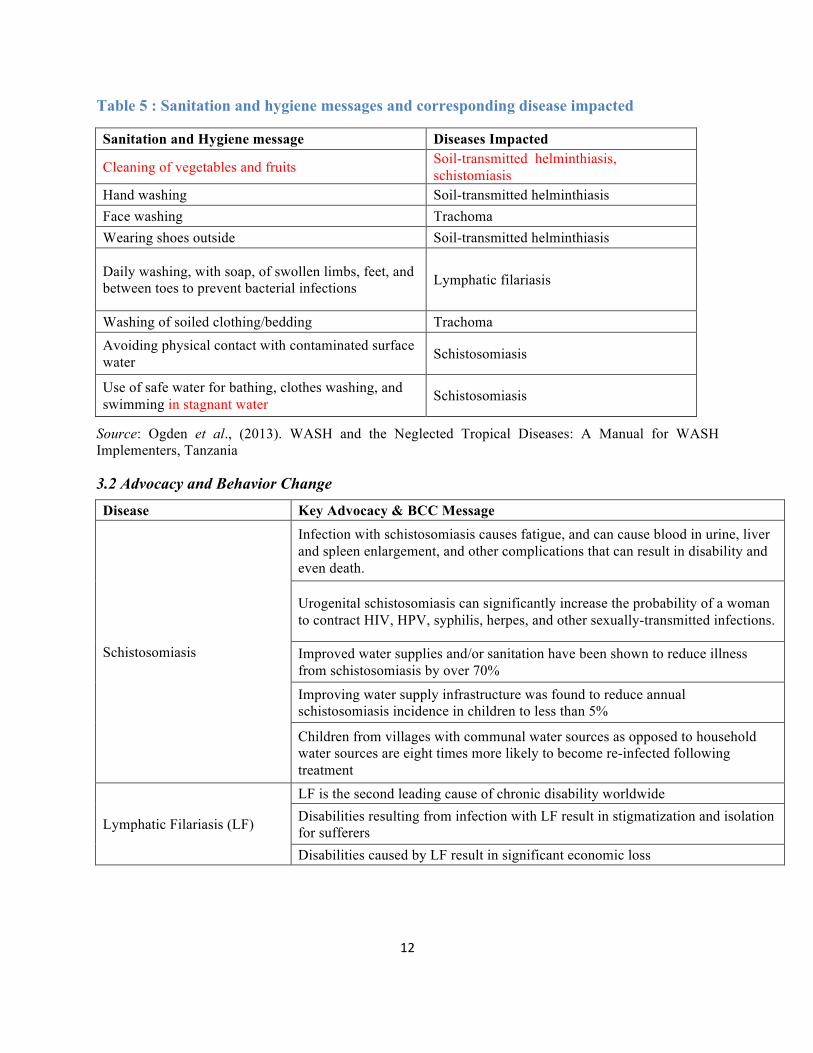
Table 5 : Sanitation and hygiene messages and corresponding disease impacted
Sanitation and Hygiene message Diseases Impacted
Cleaning of vegetables and fruits Soil-transmitted helminthiasis, schistomiasis
Hand washing Soil-transmitted helminthiasis Face washing Trachoma Wearing shoes outside Soil-transmitted helminthiasis
Daily washing, with soap, of swollen limbs, feet, and between toes to prevent bacterial infections Lymphatic filariasis
Washing of soiled clothing/bedding Trachoma Avoiding physical contact with contaminated surface water Schistosomiasis
Use of safe water for bathing, clothes washing, and swimming in stagnant water Schistosomiasis
Source: Ogden et al., (2013). WASH and the Neglected Tropical Diseases: A Manual for WASH Implementers, Tanzania
3.2 Advocacy and Behavior Change
Disease Key Advocacy & BCC Message
Schistosomiasis
Infection with schistosomiasis causes fatigue, and can cause blood in urine, liver and spleen enlargement, and other complications that can result in disability and even death.
Urogenital schistosomiasis can significantly increase the probability of a woman to contract HIV, HPV, syphilis, herpes, and other sexually-transmitted infections.
Improved water supplies and/or sanitation have been shown to reduce illness from schistosomiasis by over 70%
Improving water supply infrastructure was found to reduce annual schistosomiasis incidence in children to less than 5%
Children from villages with communal water sources as opposed to household water sources are eight times more likely to become re-infected following treatment
Lymphatic Filariasis (LF)
LF is the second leading cause of chronic disability worldwide Disabilities resulting from infection with LF result in stigmatization and isolation for sufferers Disabilities caused by LF result in significant economic loss

13
Hygiene plays a critical role in decreasing disability caused by advanced stages of LF. Foot washing with soap helps to manage the debilitating swelling of the limbs (lymphedema) by reducing the frequency of painful secondary bacterial infections in affected limbs
Management of wastewater, cesspits and septic tanks, as well as covering water containers, treating water bodies, and other interventions can help prevent breeding of mosquitoes that spread the disease
Trachoma
Trachoma is the world’s leading cause of preventable blindness Nearly 1.2 million people in Tanzania are irreversibly blind as a result of trachoma Infection with trachoma results from poor hygiene and sanitation
Trachoma infection can be prevented through increased facial cleanliness with soap and clean water and improved sanitation. Facial cleanliness means that an individual having a clean face and no visible ocular discharge. Facial cleanliness has been used as a proxy indicator for the activity of face washing.
Facial cleanliness is associated with over 60% reduction in risk of active trachoma and reduction in risk of infection with the bacteria that causes trachoma.
People with latrines have over 15% reduction in risk of active trachoma and over 50% reduction in risk of infection with the bacteria that causes trachoma.
Improved water supplies and/or sanitation reduce illness from trachoma for over 25%.
Soil-transmitted helminthiasis (STH)
Improved water supplies and/or sanitation have been shown to reduce illness from one of the STH worms and roundworm Wearing shoes reduces hookworm infection Combined sanitation availability and use reduce the infection Access to a household latrine is associated with a greater than 40% reduced risk of infection with roundworm and whipworm
Hand washing with soap at critical times, such as after defecation and before eating, can reduce risk of infection with all three STH species by greater than 30%
Households that have piped water access have a markedly reduced risk of infection, though this may be related to other sanitation and hygiene practices as a result of having a water source close to home
Onchocerciasis
Onchocerciasis is the second leading cause of blindness of infectious origin. Over time, inflammatory responses to microfilariae lead to sensitivity to light, diminished vision, and eventually blindness
Infected patients develop severe dermatitis, which causes intense itching. The skin becomes swollen, thickened, and eventually loses pigment, a disfiguring condition called “lizard skin.”
14
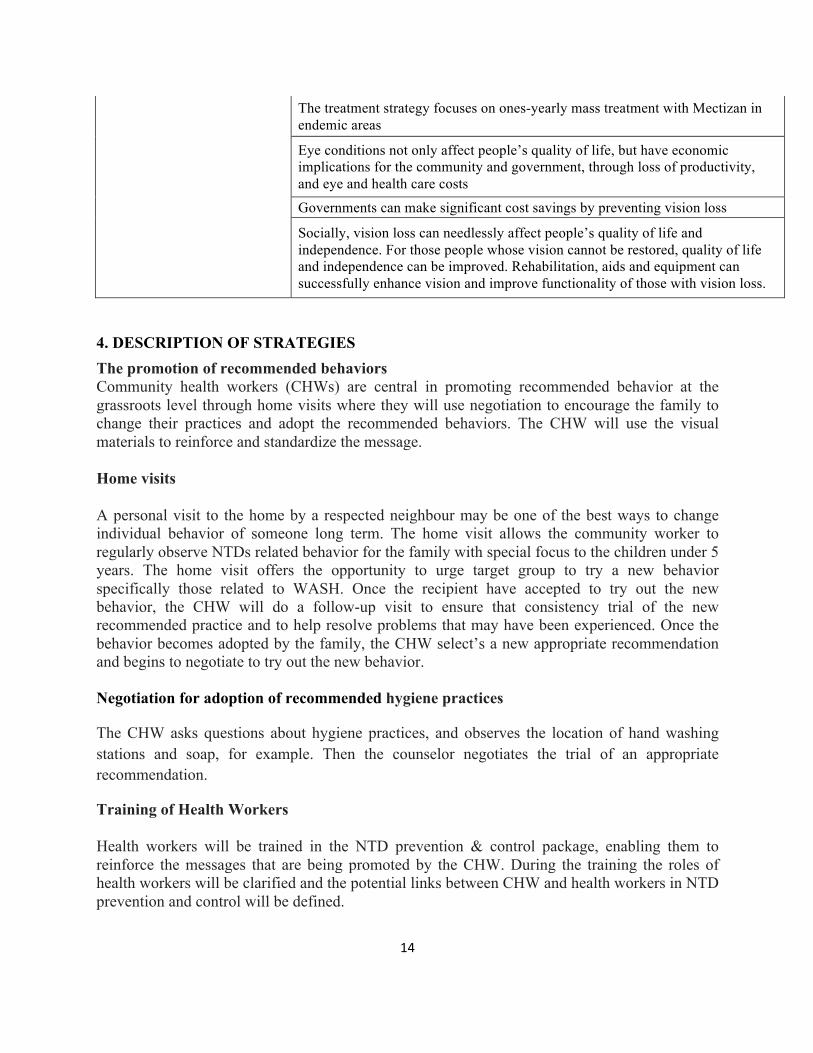
The treatment strategy focuses on ones-yearly mass treatment with Mectizan in endemic areas
Eye conditions not only affect people’s quality of life, but have economic implications for the community and government, through loss of productivity, and eye and health care costs
Governments can make significant cost savings by preventing vision loss
Socially, vision loss can needlessly affect people’s quality of life and independence. For those people whose vision cannot be restored, quality of life and independence can be improved. Rehabilitation, aids and equipment can successfully enhance vision and improve functionality of those with vision loss.
4. DESCRIPTION OF STRATEGIES The promotion of recommended behaviors Community health workers (CHWs) are central in promoting recommended behavior at the grassroots level through home visits where they will use negotiation to encourage the family to change their practices and adopt the recommended behaviors. The CHW will use the visual materials to reinforce and standardize the message. Home visits A personal visit to the home by a respected neighbour may be one of the best ways to change individual behavior of someone long term. The home visit allows the community worker to regularly observe NTDs related behavior for the family with special focus to the children under 5 years. The home visit offers the opportunity to urge target group to try a new behavior specifically those related to WASH. Once the recipient have accepted to try out the new behavior, the CHW will do a follow-up visit to ensure that consistency trial of the new recommended practice and to help resolve problems that may have been experienced. Once the behavior becomes adopted by the family, the CHW select’s a new appropriate recommendation and begins to negotiate to try out the new behavior. Negotiation for adoption of recommended hygiene practices
The CHW asks questions about hygiene practices, and observes the location of hand washing stations and soap, for example. Then the counselor negotiates the trial of an appropriate recommendation.
Training of Health Workers Health workers will be trained in the NTD prevention & control package, enabling them to reinforce the messages that are being promoted by the CHW. During the training the roles of health workers will be clarified and the potential links between CHW and health workers in NTD prevention and control will be defined.

15
Hygiene strategies Strategies will promote hygiene through demonstrations and negotiation during home visits, talks and demonstrations at model farm sites and use of counseling cards. Theater sketches will be considered as a very effective way of introducing somewhat embarrassing subjects to the discussion. Training of Teachers School teachers (head teacher and health teacher) will be trained in NTD prevention enabling them to promote school-based hygiene, sanitation, and de-worming treatment compliance. Theater Using drama is a very effective way of introducing new practices and getting people to consider that the new practices might work for them. Radio & TV Radio spots and interactive program can be very effective in introducing new concepts and new practices. This channel has wider coverage and reach thus key in promoting easy to adopt behavior like turn out during mass drug distribution, face washing and causes of NTDs in general.
5. VISUALS AND TRAINING MANUALS Communicating NTD prevention and control requires training manuals and visual materials to be developed and/or adopted. A dedicated team will need to examine each materials developed to see if it covers the message for each recommended behavior and if it is sufficient and can be easily adopted. If no materials exist, then new cards will have to be developed for each concept or recommended behavior.
6. MONITORING AND EVALUATION PLAN Monitoring the implementation of activities will concentrate on tracking the process and output indicators to ensure that activities are being implemented as intended. Monitoring shall be an ongoing process guided by a set of tools including, but not limited to, a monitoring checklist. Evaluation, on the other hand, would be conducted on a periodic basis to determine whether or not the objectives have been reached. Evaluation shall measure outcome indicators, including but not limited to message recall, changes in attitude and or intentions, and behavior. Data for evaluation shall come from small-scale, community-based surveys or other special data collection activities. The indicators identified in this document are process and outcome indicators, which are pertinent to the realization of the behavioral objectives.

16
Coverage of communication activities will be measured (numerator: number of schools/ regions/ districts/ wards/villages where at least one activity was carried out, denominator: targeted number of schools/ regions/ districts/ wards/ villages in the implementation area). Knowledge, attitudes and practices will be measured to assess the effectiveness of the communication activities. Other performance indicators that will measure the performance of communication activities will include program coverage, epidemiological coverage, geographical coverage and school coverage.