Embed Size (px)
Citation preview

Speaker : Werner Schierschmidt
Title : Human Factors in a Safety Management System –
Breaking the Chain

High risk products
High cost products
Safety is a must
Quality is not negotiable
Failure is not an option
Tightly controlled requirements
SMS in Aerospace and Defence

SAA Boeing 707 (Namibia) 1968
Tenerife Disaster (KLM 747 – PanAm 747) 1977
JAL Boeing 747 1980
Aloha Airlines Boeing 737 1988
British Airways Flight 5390 1990
Examples of Accidents

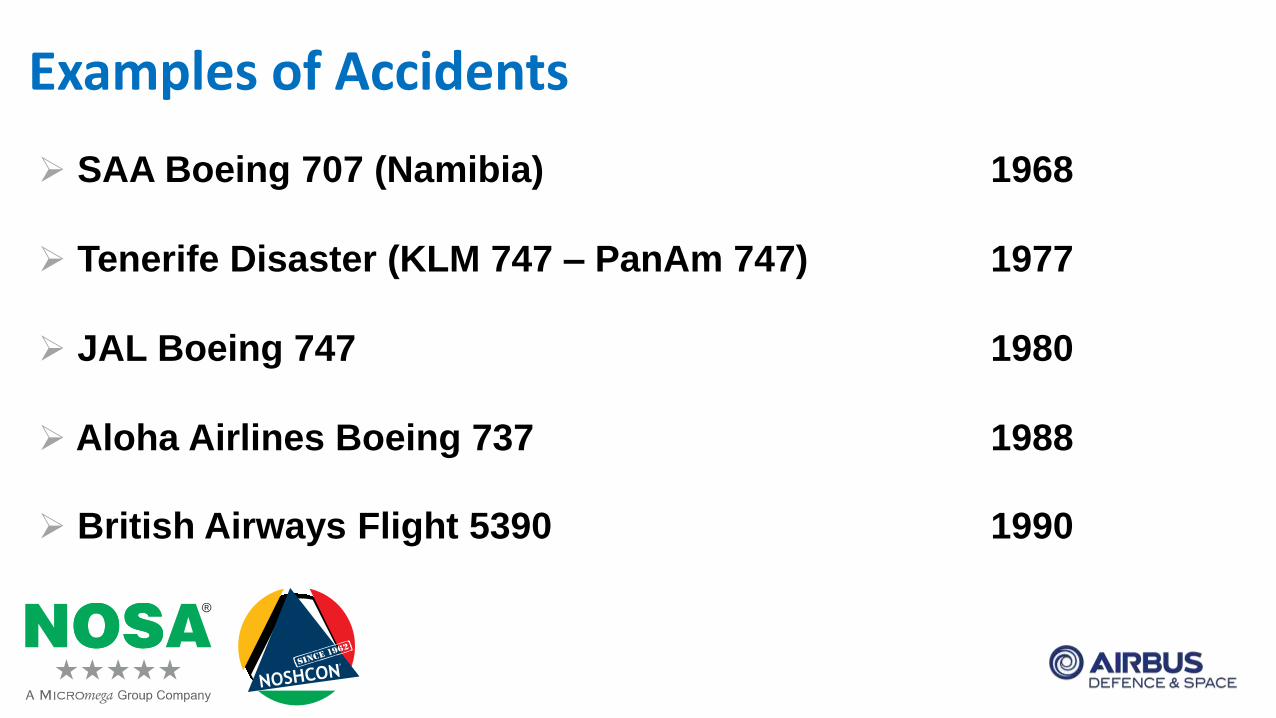
Why are there still Accidents?
60
40
20
30
20
10
1960 1970 1980 1990 2000 2010
Traffic Growth
Accidents per year
Traffic Growth
Accidents per year
Accid
en
ts p
er y
ear
Mil
lio
ns o
f d
ep
art
ure
s
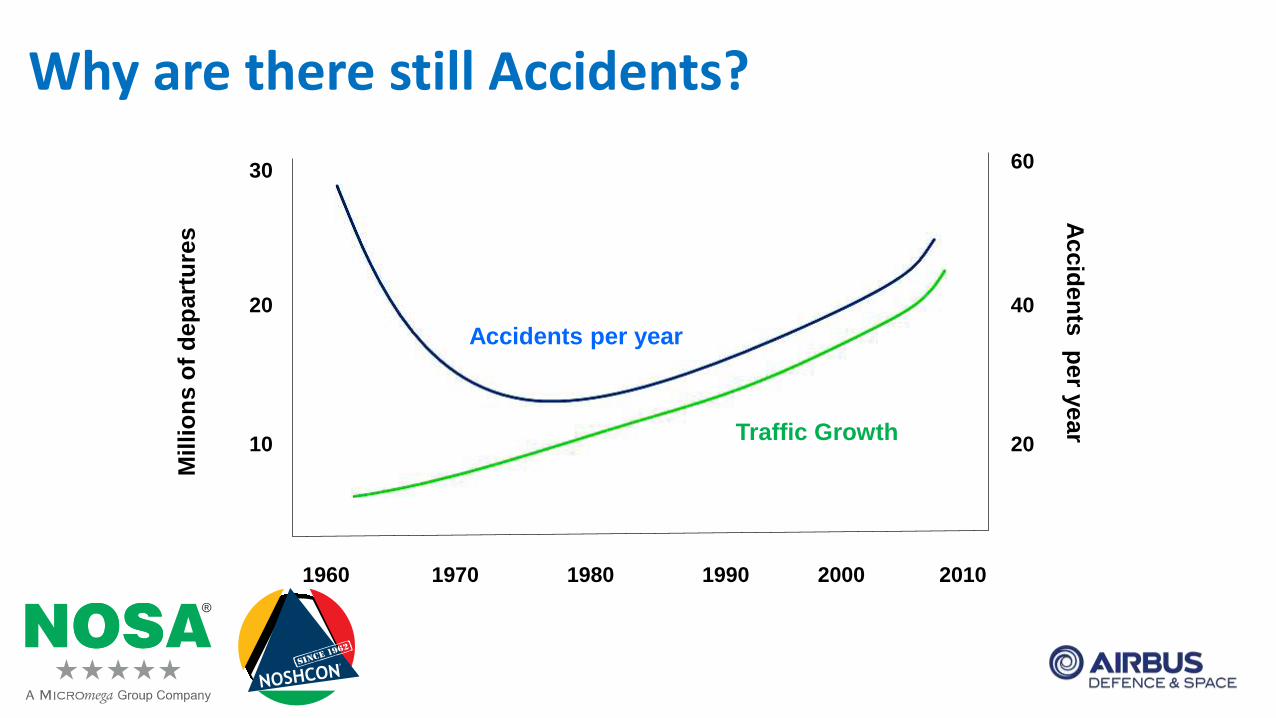
Wicken’s Information Processing
Receptors
and
Sensory
Memory
Stores
Attentional
MechanismPerception
Working
MemoryResponse
Long-term
Memory
Motor
Programmes
Ignore it
Respond to it
Consider it
Remember it
Activate other processing
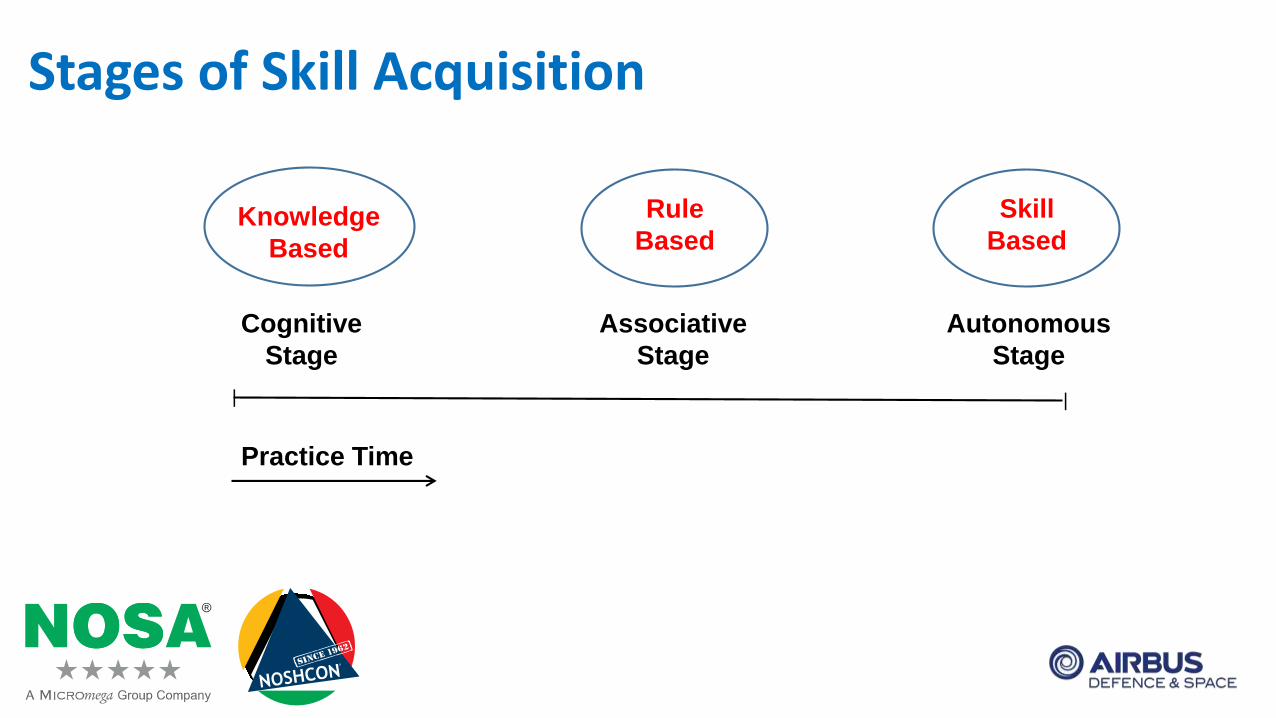
Stages of Skill Acquisition
Cognitive
Stage
Associative
Stage
Autonomous
Stage
Knowledge
Based
Rule
Based
Skill
Based
Practice Time
||
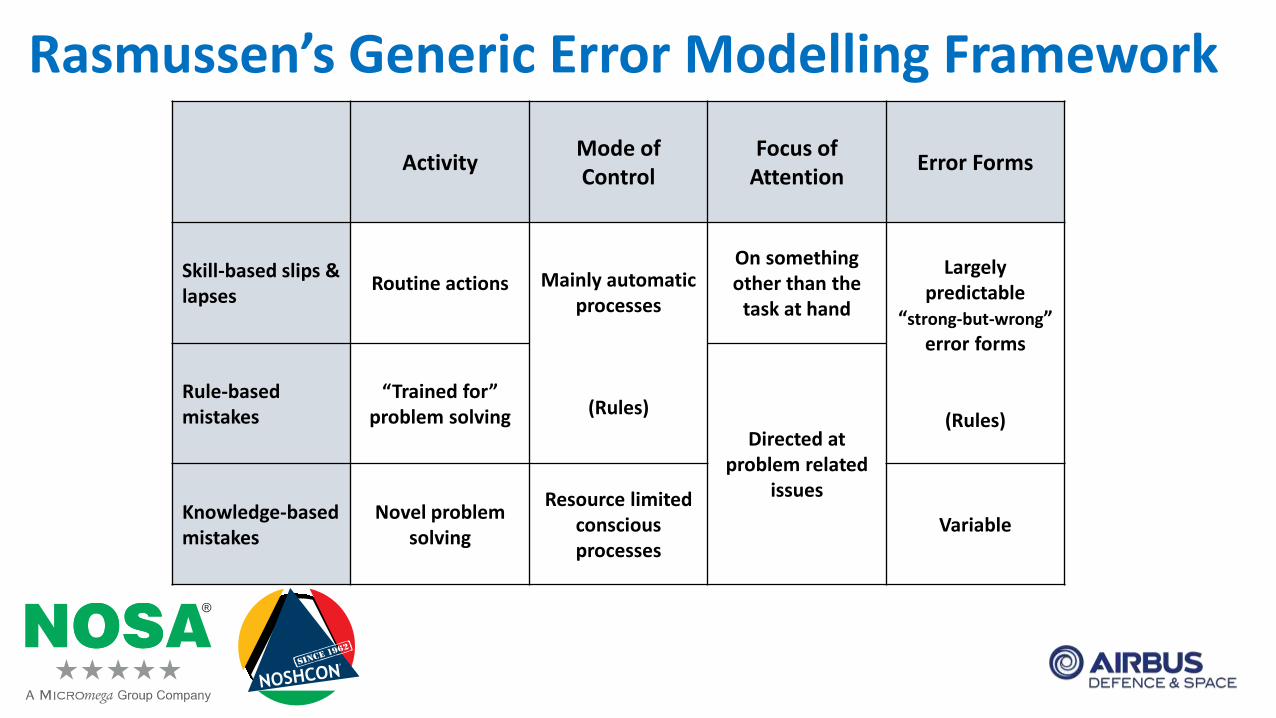
Rasmussen’s Generic Error Modelling Framework
ActivityMode of Control
Focus of Attention
Error Forms
Skill-based slips & lapses
Routine actions Mainly automatic processes
(Rules)
On something other than the
task at hand
Largely predictable
“strong-but-wrong” error forms
(Rules)
Rule-based mistakes
“Trained for” problem solving
Directed at problem related
issuesKnowledge-based mistakes
Novel problem solving
Resource limited consciousprocesses
Variable

Competence
Skills Knowledge
Attitude
Error Mistake
Violation
Competence
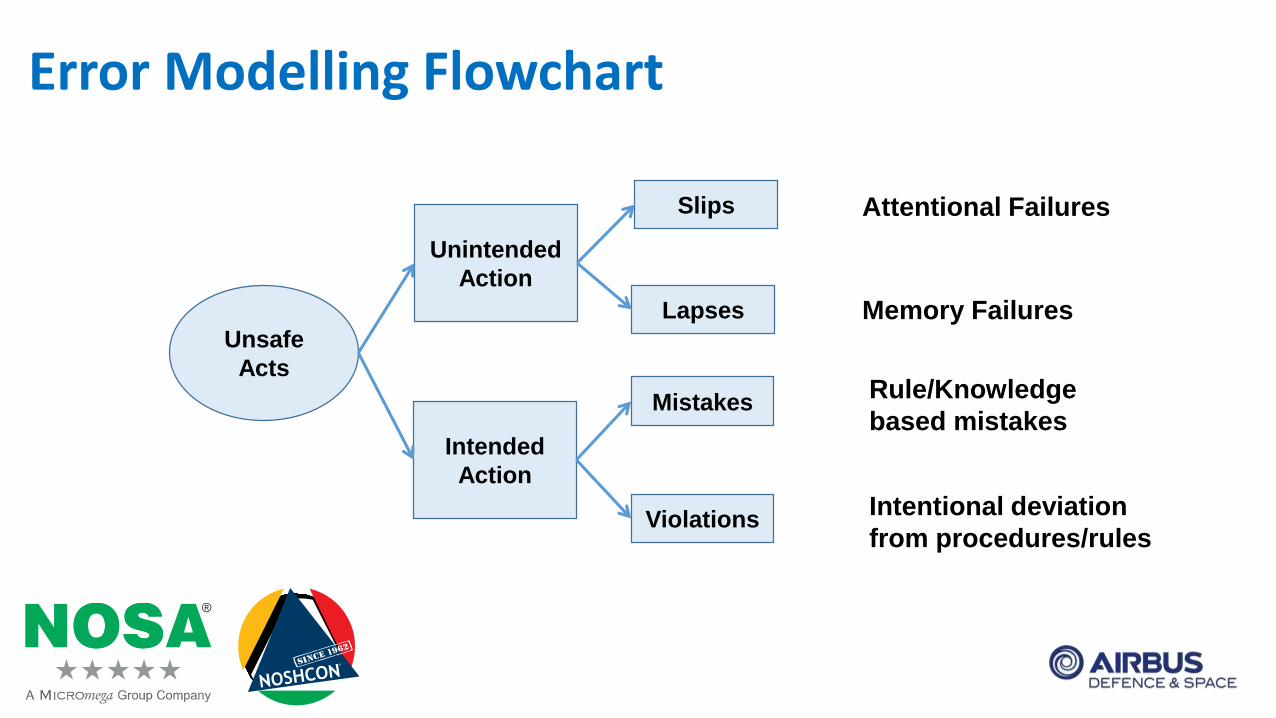
Error Modelling Flowchart
Unsafe
Acts
Unintended
Action
Intended
Action
Slips
Lapses
Mistakes
Violations
Attentional Failures
Memory Failures
Rule/Knowledge
based mistakes
Intentional deviation
from procedures/rules
Routine Violations
Situational Violations
Optimising Violations (for “kicks or a laugh”, i.e. personal gain)
Types of Violations
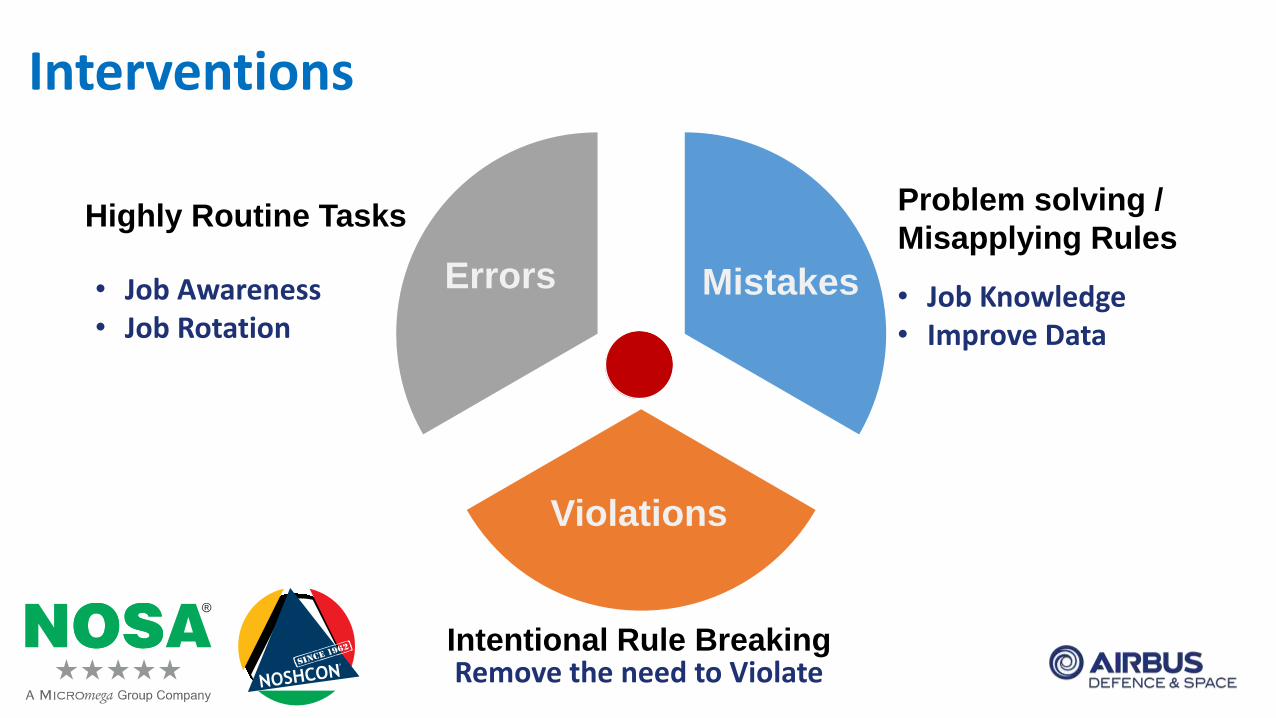
Interventions
Errors Mistakes
Violations
Highly Routine TasksProblem solving /
Misapplying Rules
Intentional Rule Breaking
• Job Awareness• Job Rotation
• Job Knowledge• Improve Data
Remove the need to Violate

Organizational Factors
Situational Factors
People Factors
Performance Shaping Factors
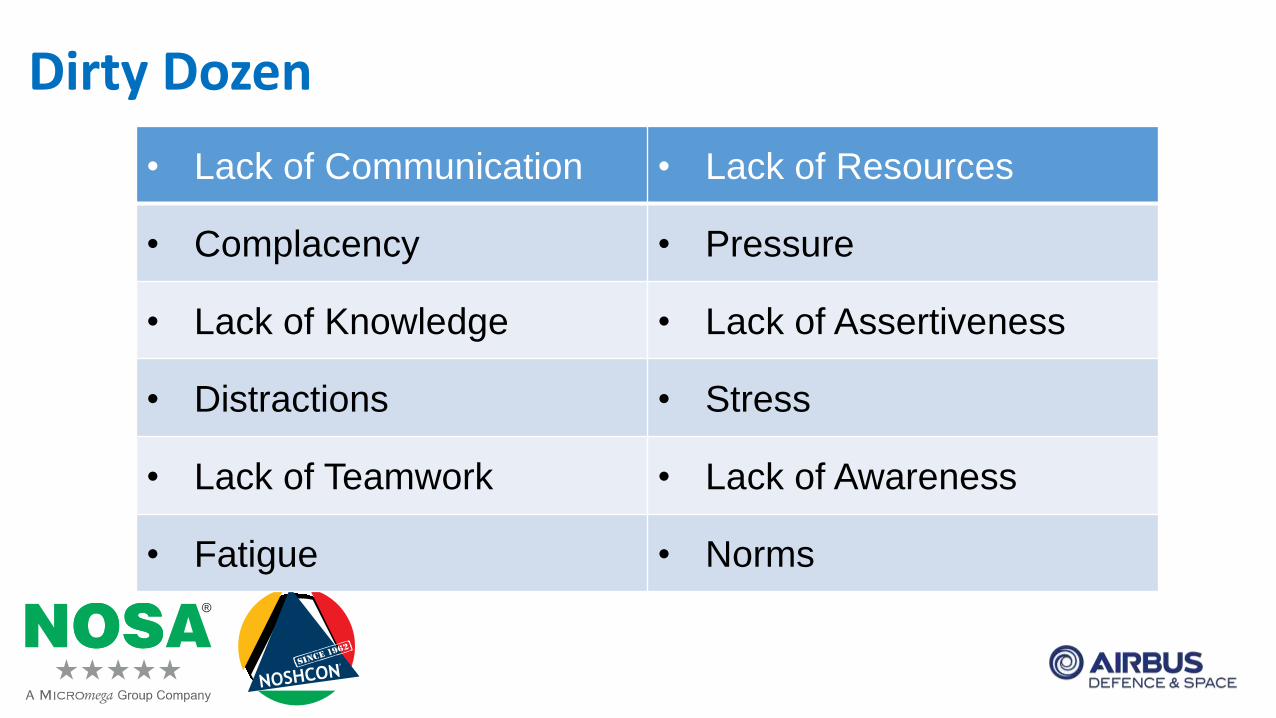
Dirty Dozen
• Lack of Communication • Lack of Resources
• Complacency • Pressure
• Lack of Knowledge • Lack of Assertiveness
• Distractions • Stress
• Lack of Teamwork • Lack of Awareness
• Fatigue • Norms

Hazard Management
Hazard
OwnersOk to Go
Control
Owners
EventHazard
ReportsDatabase
SAG
SRB
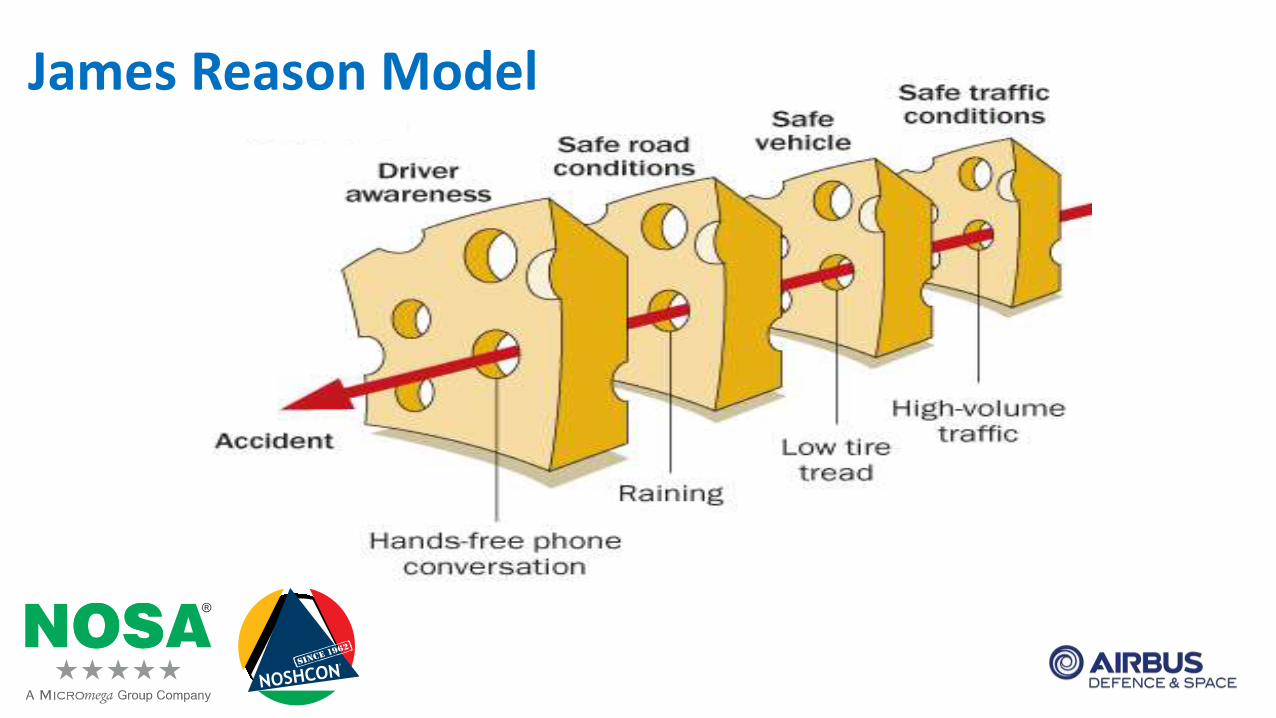
James Reason Model

Incidents / Accidents
600 Unsafe
Acts
1 Fatal Accident
10 Non-fatal Accidents
30 Reportable Incidences
In Aviation:
Human Factors
contributes to
80 - 85%
Blame
Loosing face
Do not think the event is significant, i.e.: near miss – no outcome
Always been like this in the past – status quo
Too hard to get things changed – learned helplessness
Why do we not report?
Beliefs:
Professionals will make mistakes
Professionals will develop unhealthy norms
Expectation that system safety will improve
Duties:
To raise your hand and say: “I made a mistake”
To resist the growth of “at-risk” behaviour
To absolutely avoid reckless conduct
Just Culture (not a “Blame-Free Culture”)

Reactive Safety Management
Investigation of accidents and incidents
Based upon the notion of waiting until something breaks to fix it
Most appropriate for:
o Situations involving failures in technology
o Unusual events
Types of Safety Management Systems
Proactive Safety Management
Mandatory and voluntary reporting systems, safety audits and surveys
Based upon the notion that system failures can be minimised by:
o Identifying safety risks within the system before it fails
o Taking the necessary actions to reduce such safety risks
Types of Safety Management Systems (cont.)
Predictive Safety Management
Confidential reporting, data analysis, normal operations monitoring
Based upon the notion that Safety Management is best accomplished by
looking for trouble
Aggressively seek information from a variety of resources
Types of Safety Management Systems (cont.)
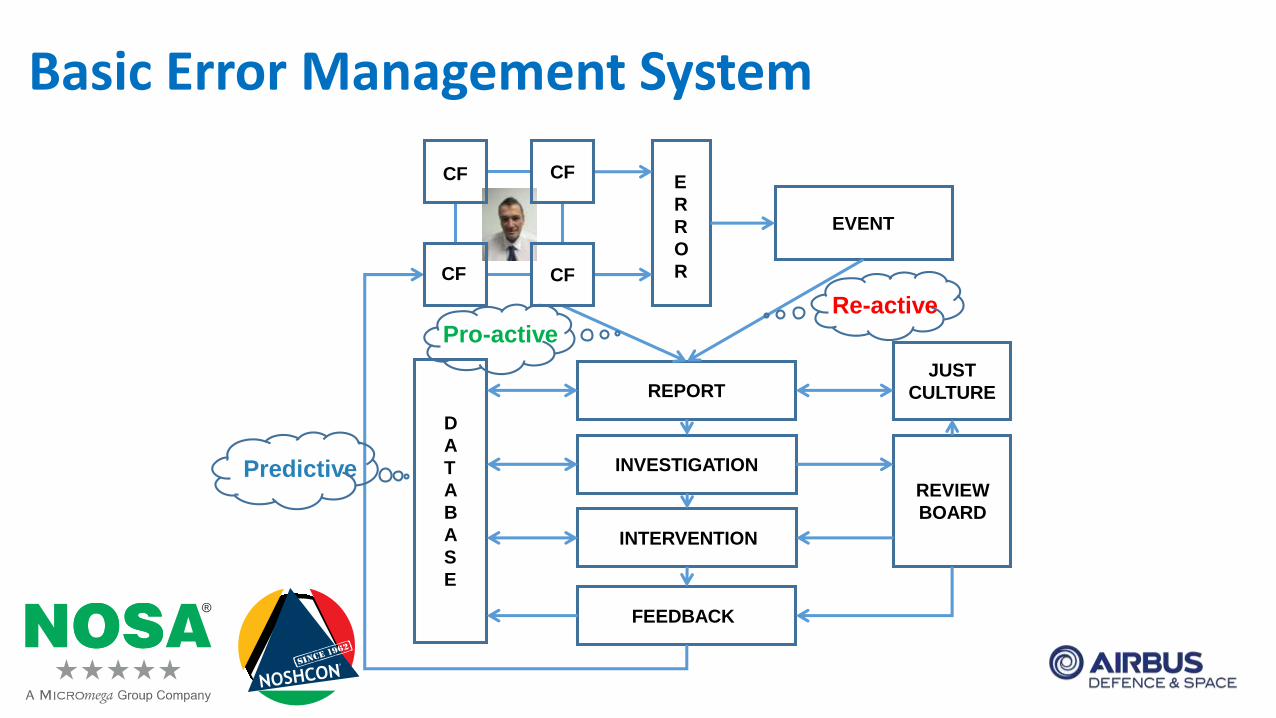
Basic Error Management System
CF
CF CF
CF
E
R
R
O
R
EVENT
REPORT
INVESTIGATION
INTERVENTION
FEEDBACK
D
A
T
A
B
A
S
E
REVIEW
BOARD
JUST
CULTURE
Re-active
Pro-active
Predictive
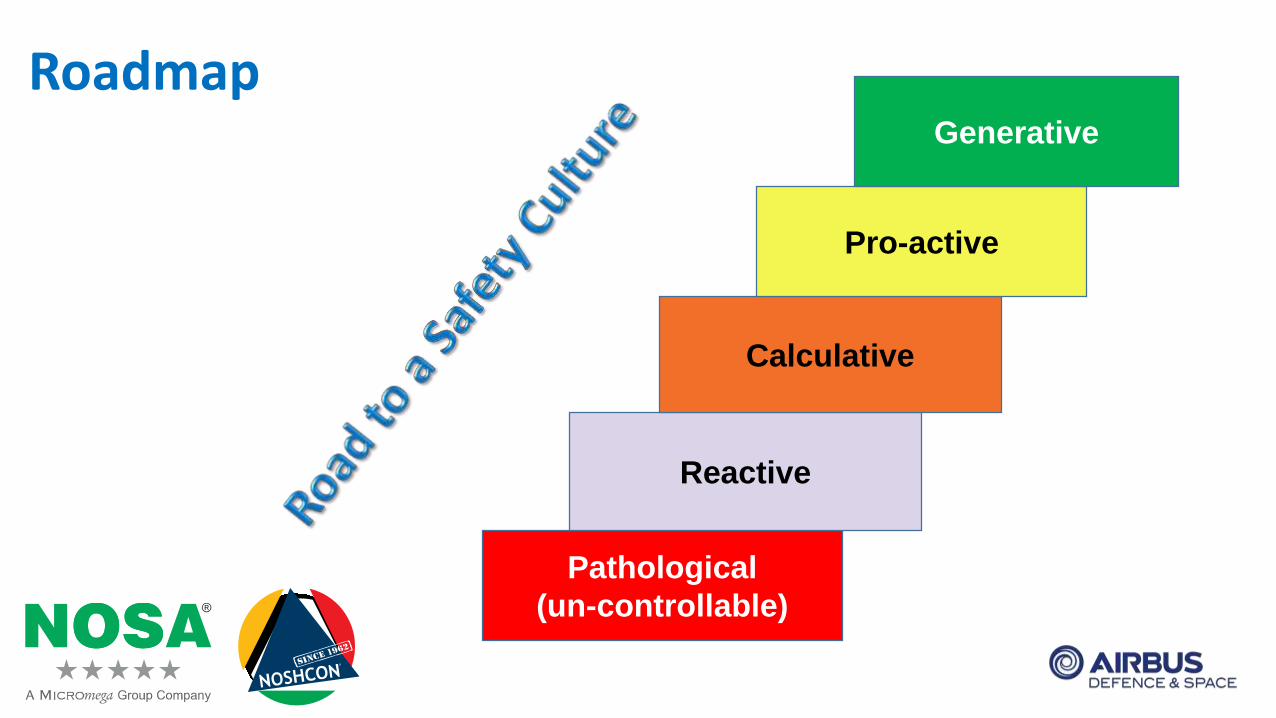
Roadmap
Pathological
(un-controllable)
Reactive
Calculative
Pro-active
Generative
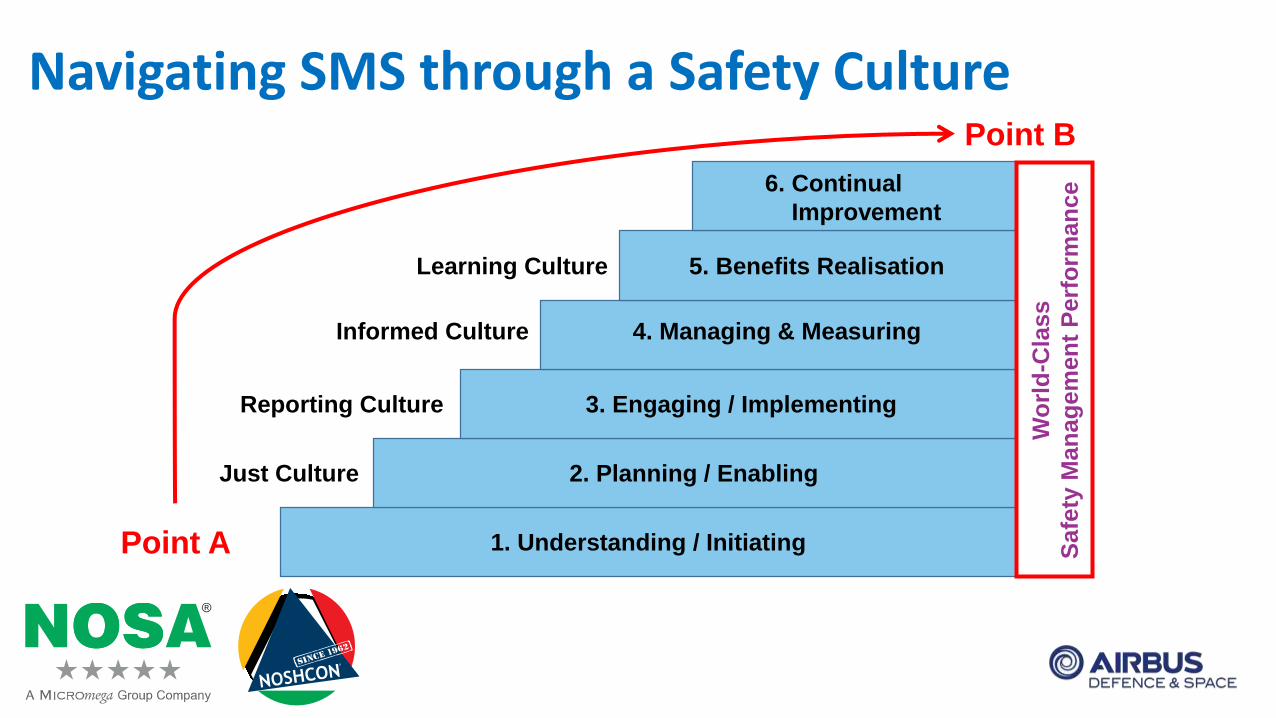
Navigating SMS through a Safety Culture
Just Culture
Reporting Culture
Informed Culture
Learning Culture
1. Understanding / Initiating
2. Planning / Enabling
3. Engaging / Implementing
4. Managing & Measuring
5. Benefits Realisation
6. Continual
Improvement
Wo
rld
-Cla
ss
Safe
ty M
an
ag
em
en
t P
erf
orm
an
ce
Point A
Point B
Humans are the strongest Link
Humans want to stick to their
Habits and Norms, they do not
like to break links in chains

Breaking the Chain
A successful Human Factors and SMS
programme is all about breaking links
in future accident chains

Thank you for your attention !
Safety is a Journey
Enjoy the Ride
![Converged Storage, Wishful Thinking & Realitycloudscaling.com/assets/pdf/cloudscaling_whitepaper_converged_st… · inimitable Werner Vogels, CTO of Amazon [@werner]. Werner focuses](https://img.pdfslide.us/doc/110x75/5f46e8be3e118e38f36b60e4/converged-storage-wishful-thinking-inimitable-werner-vogels-cto-of-amazon.jpg)