Embed Size (px)
Citation preview

Revolutionizing the Fight Against Cancers and Infectious Diseases
Dr. J. Joseph Kim PRESIDENT & CEO NASDAQ: INO
It’s All About the T-Cells

Forward Looking Statement
Our commentary and responses to your questions may contain forward-looking statements, including comments concerning clinical trials and product development programs, evaluation of potential opportunities, the level of corporate expenditures, the assessment of Inovio’s technology by potential corporate partners, capital market conditions, timing of events, cash consumption and other subjects. Information concerning factors that could cause actual results to differ materially from those set forth in our Annual Report on Form 10-K for the year ended December 31, 2013, our Form 10-Q for the quarter ended September 30, 2014, and other regulatory filings from time to time.
2

A Highly Compelling Weapon: T Cells
Cytotoxic T lymphocyte
T cell
Target cell
3
A Highly Compelling Weapon: T Cells
Cytotoxic T lymphocyte
T cell
Target cell
4
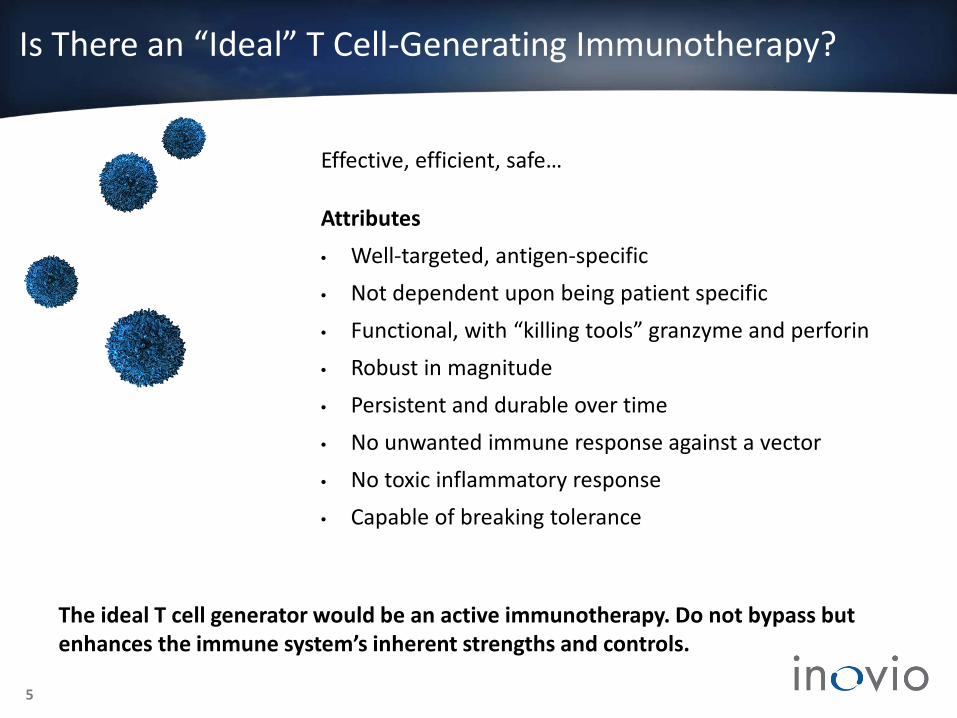
Is There an “Ideal” T Cell-Generating Immunotherapy?
Effective, efficient, safe…
Attributes • Well-targeted, antigen-specific • Not dependent upon being patient specific • Functional, with “killing tools” granzyme and perforin • Robust in magnitude • Persistent and durable over time • No unwanted immune response against a vector • No toxic inflammatory response • Capable of breaking tolerance
The ideal T cell generator would be an active immunotherapy. Do not bypass but enhances the immune system’s inherent strengths and controls.
5

Inovio Active DNA Immunotherapies: It’s All About the T Cells
IT’S ALL ABOUT THE T CELLS
Identify pertinent disease-specific antigen(s)
Encode DNA plasmid with genetic code for antigen
Deliver plasmids into cells in the body (in vivo), enabling them to produce antigen
T cells eliminate cells displaying disease-specific antigen
Immune system activates antigen-specific T cells
6
Effective, efficient, safe in vivo T cell activation

7
• Activate disease-specific CD8+ killer T cells and antibodies
Antigen targeting immunotherapies &
vaccines
• Enhance immune response activation • Impact durability of immune responses • Drive immune responses to sites of infection
Immune activators
• Simplified design, product stability, better manufacturing, dosing, and cost effectiveness
• Rapidly activates sufficient quantities of specific antibodies
Monoclonal antibodies
(DNA-based)
DNA Immunotherapy Platform: Multiple Applications
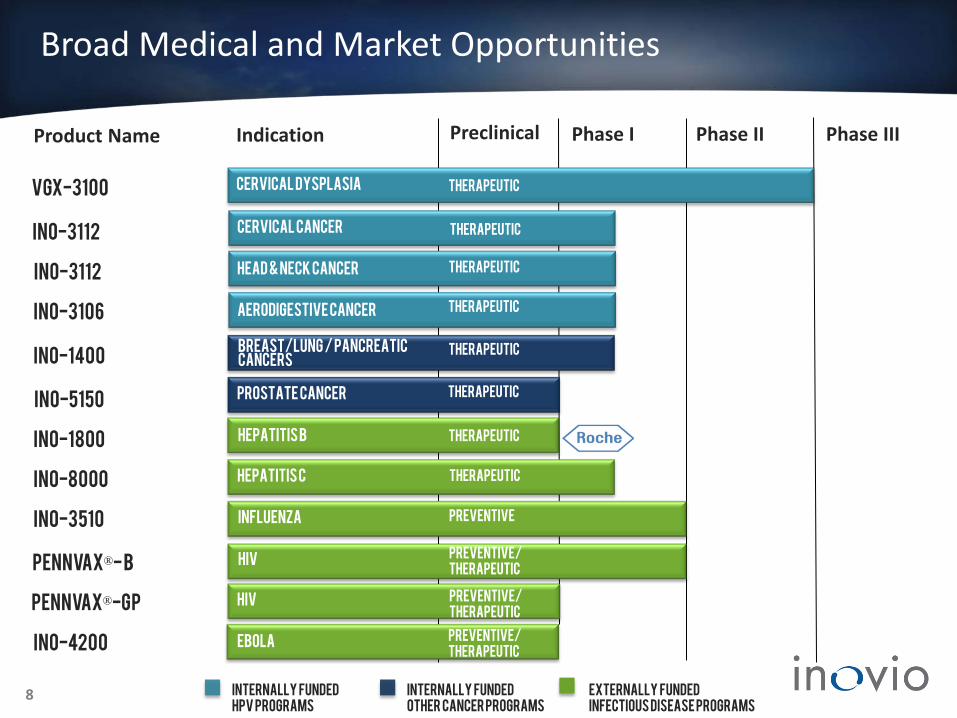
Broad Medical and Market Opportunities
Product Name
INTERNALLY FUNDED OTHER Cancer Programs
Indication Preclinical Phase I Phase II
Vgx-3100
Ino-5150
Ino-1400
EXTERNALLY FUNDED Infectious Disease Programs
Ino-3510
ino-1800
Phase III
8
INO-3112
INO-3112
Hepatitis B Therapeutic
influenza
Breast/lung / Pancreatic cancers
Therapeutic
Prostate cancer Therapeutic
Head & Neck Cancer Therapeutic
Cervical Cancer Therapeutic
Cervical dysplasia
Therapeutic
Preventive/ Therapeutic
Ebola
Aerodigestive Cancer Therapeutic
INO-3106
INO-4200
Preventive
INTERNALLY FUNDED HPV programs
Pennvax®- B hiv
Pennvax®-GP hiv
Preventive/ Therapeutic Preventive/ Therapeutic
Ino-8000 Hepatitis C Therapeutic
9
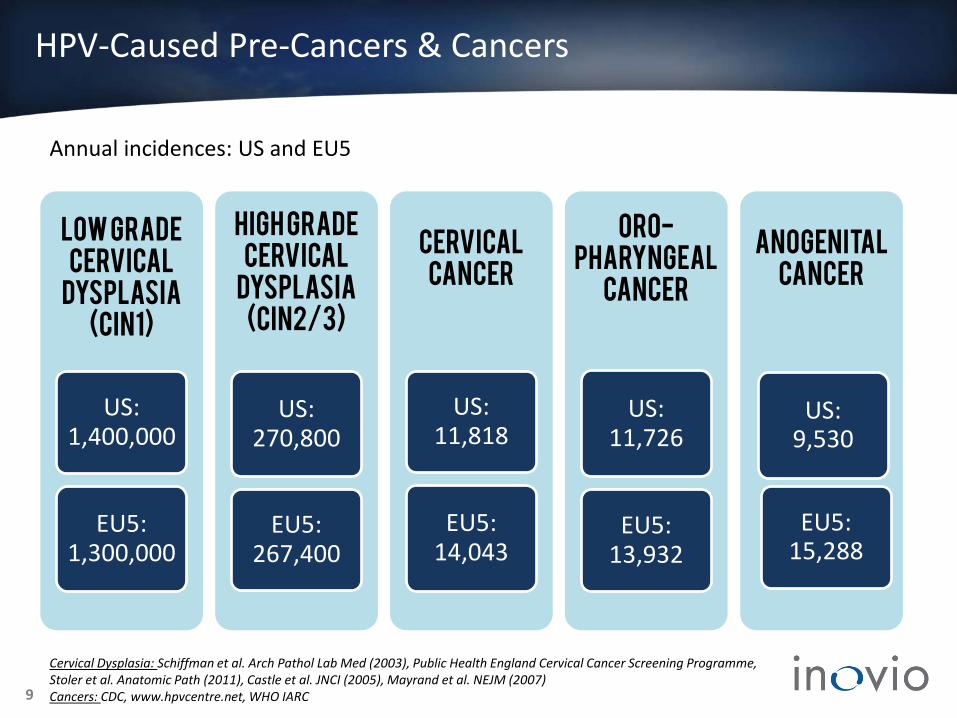
Cervical Dysplasia: Schiffman et al. Arch Pathol Lab Med (2003), Public Health England Cervical Cancer Screening Programme, Stoler et al. Anatomic Path (2011), Castle et al. JNCI (2005), Mayrand et al. NEJM (2007) Cancers: CDC, www.hpvcentre.net, WHO IARC
LOW GRADE
CERVICAL DYSPLASIA
(CIN1)
US: 1,400,000
EU5: 1,300,000
HIGH GRADE
CERVICAL DYSPLASIA
(CIN2/3)
US: 270,800
EU5: 267,400
CERVICAL CANCER
US: 11,818
EU5: 14,043
ORO-PHARYNGEAL
CANCER
US: 11,726
EU5: 13,932
Anogenital cancer
Annual incidences: US and EU5
HPV-Caused Pre-Cancers & Cancers
US: 9,530
EU5: 15,288

10
Normal Cervical Intraepithelial Neoplasia
(CIN3) Invasive Cancer
If untreated, moderate/severe cervical dysplasia (CIN2/3) may progress to invasive cancer
Preventing Cervical Cancers: New Market Opportunity
11
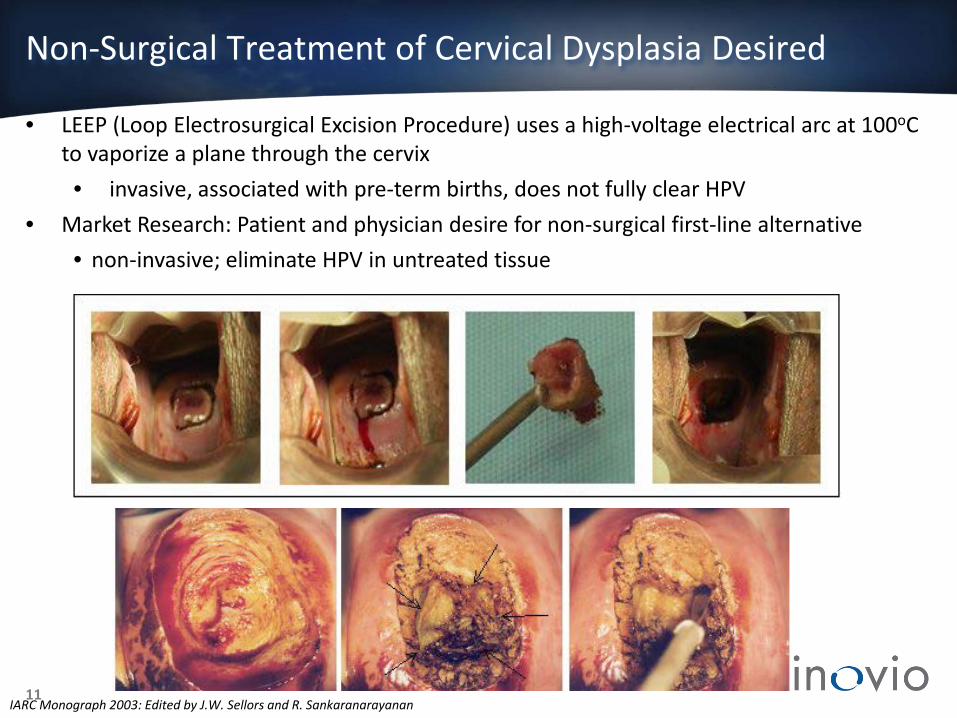
Non-Surgical Treatment of Cervical Dysplasia Desired
IARC Monograph 2003: Edited by J.W. Sellors and R. Sankaranarayanan
• LEEP (Loop Electrosurgical Excision Procedure) uses a high-voltage electrical arc at 100oC to vaporize a plane through the cervix • invasive, associated with pre-term births, does not fully clear HPV
• Market Research: Patient and physician desire for non-surgical first-line alternative • non-invasive; eliminate HPV in untreated tissue

Phase II: Study Design
• 148 subjects: 19-55 year old females with high-grade cervical dysplasia (CIN2/3)
• HPV 16 and/or 18 positive • 6 mg VGX-3100 or placebo(IM followed by EP)
at weeks 0, 4, and 12
Placebo-Controlled, Randomized, Double
Blind
• Regression of CIN2/3 to CIN1 or normal at six months post third dose (Week 36) Primary Endpoint
• Regression of CIN2/3 to CIN1 or normal and • Clearance of HPV 16 and/or 18 genotype
detected during screen Secondary Endpoint
12

0
10
20
30
40
50
60
Phase II: Regression of Cervical Lesions to CIN 1 or Normal
Pre-Specified 1° Endpoint: Histopathologic Regression to CIN1 or Normal
30.6% (11/36)
Statistically significant difference (p=0.017; strata-adjusted)
Post-Hoc Analysis: Regression to Normal
0
10
20
30
40
50
60
40.2% (43/107)
16.7% (6/36)
Perc
ent
VGX-3100 Placebo VGX-3100 Placebo Statistically significant difference
(p=0.006; strata-adjusted)
Overall Histopathologic Regression Incidence Per-Protocol Population (N=143)
13
49.5% (53/107)
Perc
ent

Phase II: Clinically Significant Efficacy; Achieves Endpoints
49.5% (53/107)
30.6% (11/36)
Histopathologic Regression to CIN1 or Normal AND Virological Clearance (HPV16 or 18) (n=143)
0
10
20
30
40
50
60
40.2% (43/107)
14.3% (5/35)
Perc
ent
VGX-3100 Placebo
Statistically significant difference (p=0.001; strata-adjusted)
14

*Statistically significant; bars are 95% CI. IFN = interferon. .
IFN-γ ELISpot Analysis
VGX-3100 Generates HPV-16 and HPV-18 T Cell Responses
15
800
600
400
200
0 0 5 10 15 20 25 30 35 40
Study Week
VGX-
3100
Spe
cific
T C
ells
(S
FU/1
06 PBM
Cs A
bove
Bas
elin
e)
* * * *
VGX-3100 Placebo
Treatment at wks 0, 4 & 12
N= 140 .

CD8 T Cells Clear Virus and Lesions in Cervical Tissue: Placebo W
eek
0: C
IN3
path
olog
y
IHC Staining: HPV
Wee
k 36
: CIN
3 pa
thol
ogy
IHC Staining: CD8 16

CD8 T Cells Clear Virus and Lesions in Cervical Tissue: VGX-3100 Treated Patients
Wee
k 0:
CIN
3 pa
thol
ogy
IHC Staining: HPV
Wee
k 36
: No
sign
ifica
nt
path
olog
y
IHC Staining: CD8 17

Powerful Impact of Successful VGX-3100 Phase II Efficacy Data
VGX-3100 is a non-surgical option for the treatment of CIN2/3
Simple 3 monthly injections generated CD8 Killer T cells
Measured in blood
Observed in cervical tissues (tissue infiltrating T cells)
Direct correlation found between CD8 T cells and efficacy
Demonstrated phase 2 efficacy and safety
Regressed disease to normal
Cleared virus which caused the disease
Disease regression - expand into other HPV-caused diseases
Other anti-cancer therapies (lung, breast, pancreas, prostate)
HPV clearance – antiviral therapies (HBV, HCV, HIV)
18

VGX-3100: Next Steps
EXPANSION OF HPV PROGRAM TO RELATED CANCERS AND PRE-CANCERS • Cervical cancer (Ph I/IIa initiated) • Head & neck (Ph I/IIa initiated)
• Anogenital cancers • VIN, PIN
PREPARING SCIENTIFIC PAPER FOR PEER REVIEW • Completing immunological analysis to characterize T cell subsets.
Phase II data adds to phase I data, which was extensively characterized (Bagarazzi, et al. Sci Transl Med 2012)
• Manuscript being prepared for submission
PHASE III PLANNING FOR EARLY 2016 LAUNCH • Clinical and regulatory • Scale up immunotherapy production • Market research
• Supply chain strategy • EP device production • Pricing & reimbursement
19

HPV-Associated Cancer Studies Enrolling: INO-3112
Phase I/IIa’s: INO-3112 (VGX-3100 + IL-12 DNA immune activator); HPV 16/ 18 related disease
Cervical Cancer • 20 women with cervical carcinoma • Safety, tolerability, immunogenicity • Cervical histology • Treat after chemoradiation
Head & Neck Squamous Cell Carcinoma • 20 men/women • Safety, tolerability, immunogenicity • Anti-tumor effects & progression free
survival • Arm #1: treat before/after tumor resection • Arm #2: treat after chemoradiation
20

hTERT-Associated Cancers: INO-1400
• Antigen: human telomerase reverse transcriptase (hTERT), associated with cancer cell survival; overexpressed in 85% of cancers - potential “universal” cancer therapy
• +/- IL-12 DNA immune activator
• Phase I: 54 patients with breast, lung, or pancreatic cancers
• Safety, tolerability, immunogenicity
• Anti-tumor effects and progression free survival
• Trial launched: 4Q 2014
21
• Multi-antigen: HBV clades A & C surface antigens & HBV core antigens
• +/- IL-12 DNA immune activator • Phase I/IIa: patients with chronic HBV
infection • Safety, tolerability, immunogenicity • Trial initiation: 1H 2015 • Trial initiation will trigger milestone
payment from Roche
22
Hepatitis B: INO-1800

anthrax Louis Pasteur
Peter Kies CFO • Ernst & Young
• Experience with growth companies
Mark L. Bagarazzi, MD CMO • Clinical research experience incl. Merck
• Led clinical/regulatory for shingles and rotavirus vaccines; DNA vaccine expert
J.Joseph Kim, PhD President & CEO
• Decades of biotechnology/ pharma management
• Merck: hepatitis A and B vaccines manufacturing; HIV
vaccine (Ad5) R&D
Niranjan Y. Sardesai, PhD COO
• Extensive biotech management and product development
experience
• Led diagnostics development for mesothelioma, bladder
cancer, and ovarian cancer for Fujirebio Diagnostics
Management
23

anthrax J.Joseph Kim, PhD • President & CEO, Inovio
Adel Mahmoud, PhD • Professor, Princeton University
• Former President, Merck Vaccines
• Responsible for Gardasil®, Zostavax®, Proquad® and Rotateq®
Morton Collins, PhD • General Partner, Battelle Ventures and Innovations Valley Partners
Simon X. Benito • Former Senior Vice President,
Merck Vaccine Division
Angel Cabrera, PhD • President, George Mason
University
• Former President, Thunderbird School of Global Management
Avtar Dhillon, MD Chairman, BOD
• Former President & CEO, Inovio Biomedical
Board of Directors
24

anthrax Louis Pasteur
Stanley A. Plotkin, MD • Developed rubella and rabies vaccines
• Oversaw Sanofi flu vaccine
• Emeritus Professor, Wistar Institute & University of Pennsylvania
Philip Greenberg, MD • Expert in T cell immunology
• Head, Immunology Program, Fred Hutchinson Cancer Research Center
25
Anthony W. Ford-Hutchinson, PhD
• Former SVP, Vaccines R&D, Merck
• Oversaw development: Singulair®, Januvia®, Gardasil®, Zostavax®,
Proquad® and Rotateq®
David B. Weiner, PhD Chairman
•“Father of DNA vaccines”
• Dept. of Pathology & Laboratory Medicine, University of Pennsylvania
Scientific Advisory Board

Financial Information
Cash, cash equivalents & short-term investments2 $ 100.9 M
Debt2 0 M
Cash runway 4Q 2017
Shares outstanding2 60.5 M
Recent share price1 $8.23
Market cap1 $ 497.9 M
NASDAQ: INO
1Feb 5, 2015 2Sep 30, 2014 3 From Q3 20142
26
Insider buying3 > $2.75M

INTERNALLY FUNDED EXTERNALLY FUNDED
Ino-1400 4Q 2014 Initiated phase I
Breast, Lung, And Pancreatic Cancer
Vgx-3100 2016 Initiate phase III Cervical dysplasia
27
Value Drivers
INO-3112 2015 Report interim data
Head & Neck and Cervical Cancer
Ino-8000 2015 Report interim phase I data
Hepatitis C
Ino-1800 1H 2015 Initiate phase I/IIa
Hepatitis B
Ebola 1H 2015 Initiate phase I INO-4200
Ino-5150 1H 2015 Initiate phase I
Prostate cancer
PennVAX®
1H 2015 Initiate PENNVAX-GP phase I HIV

Best-in-class immune
responses to fight cancers
and infectious diseases
Targeting broad range of billion dollar disease
markets
Breakthrough in vivo T cell generating platform
Validating partnership with Roche
Lead product met phase II
efficacy endpoints
Investor Highlights
28

Revolutionizing the Fight Against Cancers and Infectious Diseases
It’s All About the T-Cells

Strain 1
Strain X
Strain 2
Antigen Y
Antigen Y Antigen Y
T Cells by Design: Antigen-Specific, Optimized, Best-in-Class
30
Identify gene sequence of selected antigen(s) from chosen strains/variants of the virus/cancer
Synthetically create optimal consensus gene sequence for the selected antigen – PATENTABLE

Insert SynCon® gene sequence for selected antigen into DNA plasmid.
SYNCON® DNA
Antigen consensus
sequence
DNA Plasmid
Designed to Break Tolerance or Provide Universal Protection
31
SynCon DNA plasmid ready to manufacture.

Electroporation Delivery Plays a Vital Role
32

SynCon®+ Electroporation: Significant Antigen Expression
Ref: Sardesai & Weiner Curr. Opin. Immunol. 2011
• 1000x increase in cellular uptake and antigen production/ expression
• >500 patents globally
Intramuscular Intradermal
33

Inovio Beats Previous Gold Standard for T Cell Generation DNA/Electroporation vs Merck Ad5 Viral Vector (Non-Human Primates)
SIV Model: UPenn/Merck/Inovio Assay: Data Co-Published
T Cell ELISpot Assay T Cell Proliferation Assay
DNA + EP Ad5 DNA + EP Ad5
Ref: Hirao et al. Molecular Therapy, August 2010
Flow Cytometry Assay
34
Ad5 DNA + EP Ad5 DNA + EP
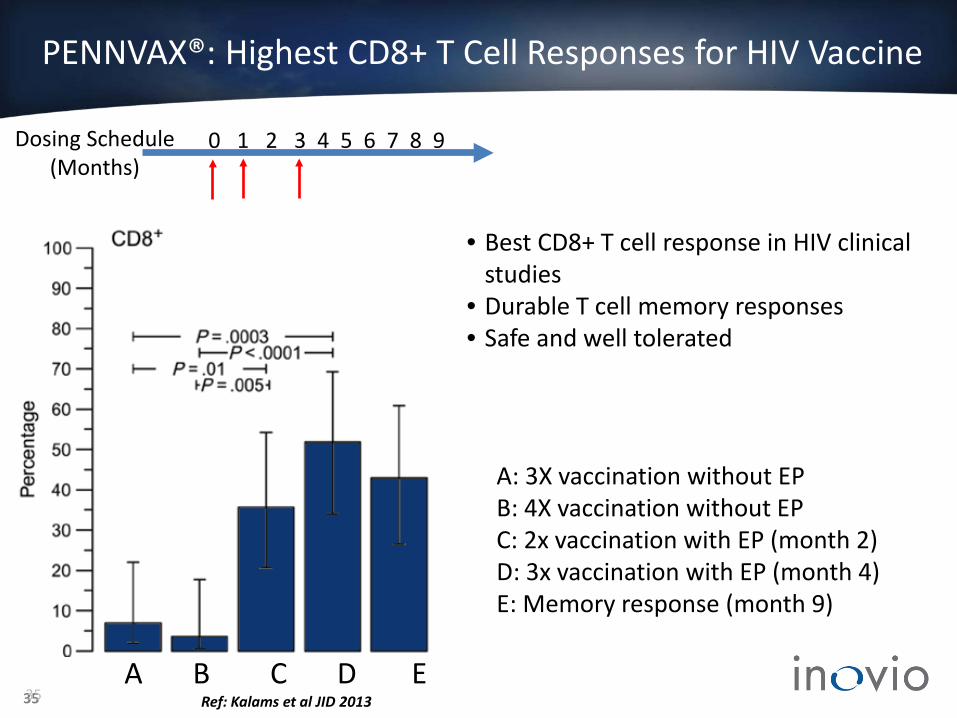
PENNVAX®: Highest CD8+ T Cell Responses for HIV Vaccine
Ref: Kalams et al JID 2013 35
A: 3X vaccination without EP B: 4X vaccination without EP C: 2x vaccination with EP (month 2) D: 3x vaccination with EP (month 4) E: Memory response (month 9)
A B C D E
• Best CD8+ T cell response in HIV clinical studies
• Durable T cell memory responses • Safe and well tolerated
0 1 2 3 4 5 6 7 8 9 Dosing Schedule (Months)
35

VGX-3100 is a non-surgical option for the treatment of HPV-specific high-grade cervical dysplasia (CIN2/3)
Combination HPV16/18 E6/E7 DNA immunotherapy (two DNA plasmids delivered simultaneously via IM injection followed by short electrical pulses)
Capitalizes on Inovio’s ability to drive the body’s own immune system to seek and destroy pre-cancerous cells
Treatment with VGX-3100 results in histopathological regression of CIN2/3 and clearance of HPV in a placebo-controlled Phase II study
Opportunity to position VGX-3100 in the gynecologist’s office in lieu of watchful waiting or LEEP
Estimated potential market of $600 MM
36

HPV 16 E6 HPV 16 E7
VGX-3100: HPV16,18 E6/E7 Immunotherapy
37
*Deletions or mutations important for p53 binding and degradation
Mutations in Rb binding site
pCon18E6E7
IgELS Endoproteolytic cleavage site
* * *
pCon16E6E7
HPV 18 E6 HPV 18 E7
IgELS Endoproteolytic cleavage site
* * *

Phase I summary: VGX-3100 is safe, tolerable and generates antigen-specific cellular responses
Bagarazzi et al., Sci Transl Med. (2012)
Safety: IM injection of VGX-3100 + CELLECTRA® EP – Well tolerated – No discontinuations, related SAEs, or grade 3 or 4 AEs Tolerability: Measured by visual analog scale (VAS) – Moderate pain (mean VAS score of 6 out of 10) experienced immediately after
injection; dissipates rapidly after 10 minutes
Immunogenicity: – High titers of antibody against all four antigens (ELISA, Western Blot)
– Antigen-specific cellular responses to HPV 16 and 18 E6/E7 (IFN-γ ELISpot)
– Cytotoxic T-lymphocyte (CTL) phenotype (Granzyme B/perforin release assay)
– No effect of pre-existing Treg cells – Primarily effector memory phenotype
38

Combined Cohorts Individual Dose Cohorts
VGX-3100 Induces Robust and Durable T Cell Responses
Bagarazzi, Yan, Morrow et al. Sci Transl Med 4, 155ra138 (2012)
• 14/18 (78%) subjects responded to at least one antigen • 13/18 (72%) responded to at least two antigens • 9/18 (50%) responded to all four antigens
39
ELISpot Assay
0 1 2 3 4 5 6 7 8 9 Dosing Schedule (Months)

Bagarazzi, Yan, Morrow et al, Science Trans. Med. (2012)
HPV16-, HPV18-Specific IFN-γ Production
Multi-parameter flow cytometry: CD4, CD8 activation phenotype
40

HPV16-, HPV18-Specific CD107a, Granzyme B, Perforin
Bagarazzi, Yan, Morrow et al, Science Trans. Med. (2012)
CD8 cytolytic phenotype
41

VGX-3100 Flow Cytometry – Functional Killing Assays
Inovio Confidential Bagarazzi, Yan, Morrow et al. Sci Transl Med 4, 155ra138 (2012)
Quantitative Assay
Qualitative Assay
• Patient pre-VGX-3100 PBMC are targets, post-VGX-3100 PBMC are effectors • Quantitative - PBMC added irrespective of Ag-specific CD8 frequency • Qualitative - PBMC normalized to account for Ag-specific CD8 frequency • Measure granzyme B delivery to targets
42

Phase II: Study Timeline
Wk 6 -10 weeks to -1day (begins at initial biopsy)
S
Wk 2
Day 0
E
Wk 4 Wk 12
Wk 14 Wk 24 Wk 62 Wk 88
DC
Wk 36
Histopathology
Wk 40
21-month protocol • 3-month (0, 4, 12 week) regimen • +6 months to primary endpoint • +12 months long-term follow-up
DC = discharge; E = enrollment; S = screening; Wk = week. Data on file, Inovio. 43

INO-1400: Potential Universal Cancer Therapy Targeting hTERT (overexpressed in 85% of cancers)
Yan J et al., Cancer Immunol Res. (2013) 44
Dharmapuri et al., Mol Ther. (2009)
T-cell generation: older generation DNA vaccine and electroporation device
SynCon® T-cell generation with CELLECTRA® electroporation device





























