Embed Size (px)
Citation preview

1
Dental Contract Reform Programme
Prototype Welcome events
Summer 2016, London and Leeds
2
Housekeeping
• There is no fire alarm planned today. If the alarm goes
off please evacuate, follow security staff instructions
and assemble outside building
• Toilets are across core 2 lift lobby
• Please turn phones to silent or vibrate
3
Agenda
• Update from dental contract reform
programme
• Prototype evaluation
• Post go-live feedback
• Making it work for you (refreshment break within
this session)
• Meet your programme support team
• Close

4
Dental Contract ReformPrototype Welcome Event
Summer 2016, London and Leeds
5
Thank you
• Thank you for your participation in the dental contract
reform programme
• This is an exciting time for contract reform and your
continued support is appreciated and valued
• Pathway approach remains at the heart of reform
• Aim of today is to:
• Provide you with an overview of where we are
• To get feedback
• Support you to understand and use the data you
need to manage your contract
• Opportunity to network and share learning
6
Changes at the Department
• New Minister for dentistry – David Mowat,
Parliamentary Under Secretary of State for
Community Health and Care.
• New Senior Civil Servant Graeme Tunbridge with
responsibility for dentistry
• BUT cross party support for dental contract reform
continues.
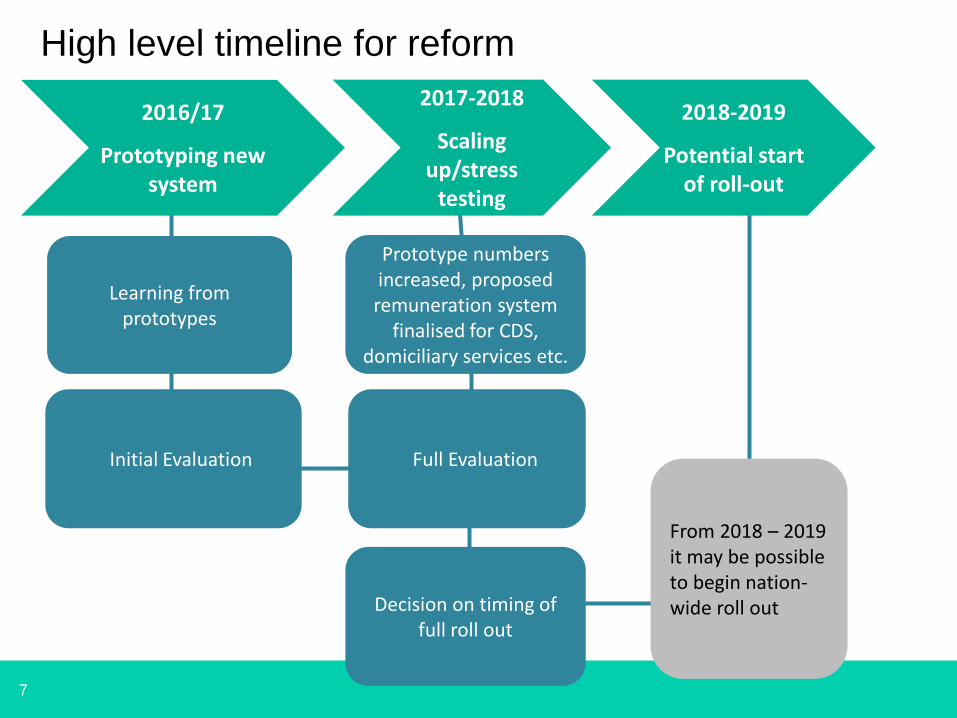
7
From 2018 – 2019 it may be possible to begin nation-wide roll out
Prototype numbers increased, proposed remuneration system
finalised for CDS, domiciliary services etc.
Learning from prototypes
2016/17
Prototyping new system
2017-2018
Scaling up/stress
testing
2018-2019
Potential start of roll-out
High level timeline for reform
Initial Evaluation
Decision on timing of full roll out
Full Evaluation
8
What are the characteristics of the
prototypes?
• Total of 82 prototypes
– 79 high street
– 3 Community Dental Services
– 21 new sites (ex UDA)
– 58 former pilots
• Of the 79 high street practices
– 40 Blend A ( 29 former pilot 11 new prototypes)
– 39 Blend B (29 former pilot 10 new prototypes)
9
How will we measure success of the
prototype approach?
We will be looking to capture 3 high level measures of
success before any new system can be rolled out:
1. Appropriate, high quality care: we will measure
outcomes (tooth decay and gum disease) and
treatment volumes to check appropriate care has
been delivered
2. Access: the prototype approach will need to be able
to provide care for at least the same number of
patients as the current system
3. Value for money: Care to patients can be delivered
within the existing dental budget
10
Programme support
• Throughout the session today you will
hear from the programme about your vital
role in prototyping
• To support this role, we will be setting out
how we will continue to work with you,
including regular contact from the
programme, visits and future events.
11
Communication plans
• Over the coming year we will be engaging
more widely with the dental and local
health communities
• This will include a bulletin highlighting the
work of the dental contract reform
programme
• Prototypes will also receive a regular
bulletin which you will hear about later
12
Evaluation of Prototyping
Summer 2016, London and Leeds
13
Evaluation – pilot practices
Pilot stage of contract reform had two evidence and learning reports
• Report 1 found:
– the pathway was having the desired effect, i.e. disease risk was
being consistently captured, communicated to patients and
managed;
– Survey responses of patients were positive; and
– The arrangements made clinical sense to dentists
• Report 2 found:
– Reinforcing the early findings report, net shift in risk from red
towards amber or green;
– Particular improvement in periodontal disease with a reduction
in disease prevalence “when measured at a level which would
generally be considered moderate but clinically problematic”
14
Evaluation – prototype practice
• Working group overseeing the work
– Chaired by Eric Rooney, deputy CDO
– Representatives from BDA and CQC
• Key themes
– Quality and appropriateness of care;
– Improvements in oral health;
– Access and accessibility
– Value for money
– Sustainability for roll out
15
Evaluation – prototype practice
• Quality and appropriateness of care
– Patients getting the treatment they need
– Compliance with the pathway / all bits of the pathway
adding value
– Professional satisfaction with the approach
– Patient journey / resources going to patients with the
highest need
• Oral Health
– Were the improvements seen at the pilot stage
maintained / improved further
16
Evaluation – prototype practice
• Access and accessibility
– Can practices provide care to the same number of
patients
– Are patients able to get an appointment (both new
patients and existing patients)
• Value for money
– Can the reformed contract be delivered within the
same financial budget
17
Evaluation – prototype practice
• Sustainability for roll out
– Is it scalable?
– Does it work for all practice types?
– What tweaks are required?
– Does the contract structure have the flexibility to
evolve over time?
18
Evaluation of Prototyping(Table top exercise)
19
Evaluation – table top exercise
Introduction
• The analysis to support the evaluation will take
a number of forms:
– Quantitative analysis (based on data)
– Qualitative analysis (getting people’s views)
– One way to conduct the qualitative analysis is to use
a structured questionnaire
– We would use the structured questionnaire at
practice visits or ask practice team to complete online
20
Evaluation – table top exercise
• What themes should the structured
questionnaire cover?
– Views on the remuneration mechanism
– Views on the pathway
– Views on the need for skill mix
– Views on flexibility / rigidity to deliver care
– What else?
21
Post go-live feedback
Summer 2016, London and Leeds
22
Post go-live feedback
• 58 former pilots, 21 new prototypes and 3 CDS make up prototype practices
• Since February the programme have completed 68* calls with prototype providers
• Purpose of calls was to provide structured post go live support to providers and business managers and obtain feedback on how prototyping was going.
• Commenced with the prototype practices new to the reform programme
• Moved to former pilot practices who were now prototypes
*CDS practices were not included at this time / small number outstanding
23
Process
• Calls were with practice owners / principals
and their business managers
• Commissioners were invited
• As well as general feedback there were a
number of areas covered including pathway,
software, remuneration and training
• For practices new to the programme only, the
call also included the pathway and a clinician
joined those calls.
24
What you told us
We asked you how prototyping had gone?
• There was consensus of support across both former pilots and the new prototypes for the clinical pathway and how this enabled clinicians to practice their dentistry, the use of extended practice team approach and focus on behaviour change of patients (and staff)
• New prototypes were broadly positive about activity + capitation, teams were still learning and adapting to new way of working
• Former pilots had more concerns about reintroduction of activity and, for some, their capitation targets
25
Clinical pathway
• All prototypes
– Use of skill mix to support delivery of pathway remains a positive approach
– Some concerns around meeting needs of differing patient populations within the current model
– Practices understood need to keep appointment lengths as short as clinically required and new majority of prototypes were working towards this from an early stage
26
Clinical Pathway ctd
• New prototypes– Majority had fully understood pathway approach and
all were positive about the benefit to patients
– Still early for these practices who are adapting to the pathway and the clinical approaches to managing individual patient needs
• Former pilots– Most practices have not made significant changes to
the way they practise dentistry as a prototype practice OHA/Rs continue to vary considerably in length.
– Some concerned that compensating for reduced treatment need (where patient’s oral health has improved) by increasing numbers of patients under capitation will not be easy.
27
Practice Management
• New prototypes
– Practices were getting used to how to run their
appointment books within prototyping such as
zoning and managing length of appointments
– Practices were considering how best to
implement skill mix to support pathway delivery
– There was some concerns about waiting times
lengthening but practices felt this would come
down again as they become more confident in the
pathway approach
28
Practice management ctd
• All prototypes– Majority of practices confirmed that patients were
accepting of the fair processing notice, there were some questions from a small minority of patients but generally were able to deal with these in practice
– Practices had taken steps to ensure all their patients had seen the notice with reception and clinical staff highlighting and laminated copies also being available in the waiting areas
– Early issues with supply chain of leaflets and prototype paperwork had been resolved
29
Performer contract
• New prototypes
– Mixed response, some were waiting to see how prototyping progressed in practice, others had already made changes, some were not looking to make changes at this time
– Where changes were made there were different approaches taken using BDA model, Code, or their own versions
• Former pilots
– As above, some practices have introduced activity measures into contracts, some capitation and some both. Again have used a variety of models
30
Software support systems
• New prototypes– No major issues raised regarding change over to prototype
software
• Former pilots– Greater level of concern from some former pilots, with particular
focus on slowness or clunkiness of systems
– These issues were generally being resolved in reasonable timeframe
• All prototypes– There had been positive feed back about their relationship with
and support received from their software companies, but this had depended on the individual practice issues and concerns
– Some practices reported good support and training from their software companies
31
Transmissions
• All prototypes
– Under a third of practices reported some issues with transmissions
– These included reported issues with slowness of transmissions and high levels of error messages and the impact this had on the practice
– For a few practices there were specific transmission issues which were being resolved directly with software companies
32
Assurance Framework
• All prototypes
– Practices were made aware of the framework
and were keen to understand what the
elements were to be included
– There was some concern from new
prototypes around a patient experience due to
the lengthening of waiting times
33
Remuneration model
• All prototypes
– The majority of practices felt they were
comfortable with the remuneration model and
had felt well supported with the training,
individual calls and web materials
– Where specific issues were raised these were
picked up outside of the calls
– Where practices needed support was in
accessing data
34
Portal reports• New prototypes
– At time of calls reports were only just becoming available on the system for practices to access
• Former pilots– High level of concern regarding access to timely
information to be able to monitor and manage contracts.
– Many would like software systems to support monitoring of capitation and UDA levels directly within software systems
– Many had missed communications on how to access portal reports in temporary home (pilot portal)
– For those who had been able to access reports they had further questions regarding what the data was showing them and how to interpret it

35
Support and Training
• All prototypes– Practices were happy to have a practice visit if they were
chosen for one
– Practices had felt comfortable being able to train their staff using materials made available
– 50/50 split response in whether practices had access to or had used the training material available on the website
– Practices were interested in idea of topic based webinars but would need more information and was mixed response as to whether these should be held at lunchtime or after surgery
– A number of former pilots had missed the more hands on programme presence and more frequent events provided under the pilot programme
36
Summary
• Programme would like to thank practices again for their time in participating in the post go-live calls
• Has the feedback you have heard today resonate with you and your experience?
• Is there any other feedback you would like to give the programme in relation to your experience of prototyping
37
Making it work for you
Summer 2016, London and Leeds
38
What we will cover in this session
• Introduction to the assurance framework
• Where to find your prototype reports
• What prototype reports are available
• Understanding your current position using the reports available
• Update on year-end
• Help and support available
39
Introduction to the assurance
framework• Programme has produced a Dental Assurance Framework
(DAF) for prototype practices, with input from Commissioners and the National Steering Group
• Currently finalising publication via NHS England’s gateway process
• Format of the framework has been based on the DAF for UDA practices, incorporating the four framework indicators:
1. Delivery
2. Patient Safety
3. Patient experience
4. Quality / clinical effectiveness
40
Introduction to the assurance
framework (2)• Set out the process for assurance:
– What is required
– By whom
– Timescales
• Reports to support assurance
– What is available / when
– How to access
– Interpretation
• Considerations for practices if you are experiencing problems with patient numbers and UDA delivery
41
Introduction to the assurance
framework (3)
• Focus of version 1 for 2016/17 is the delivery
domain
• Dental Assurance Framework for Prototypes will be
developed during 16/17 to include clinical indicators
and incorporate any learning from the prototypes
• Publication for Commissioners will be via the
regional bulletin and Prototypes will be notified by
the Programme
42
Where to find your prototype
reports• Prototype reports have a temporary home on the
pilot portal
• https://pilot.nhsbsadental.nhs.uk/portal2/
• Each user will have their own username and password to access this website
• The exact location of these reports varies depending on whether you were a former pilot or former UDA practice
43
Where to find your prototype reports
(2)
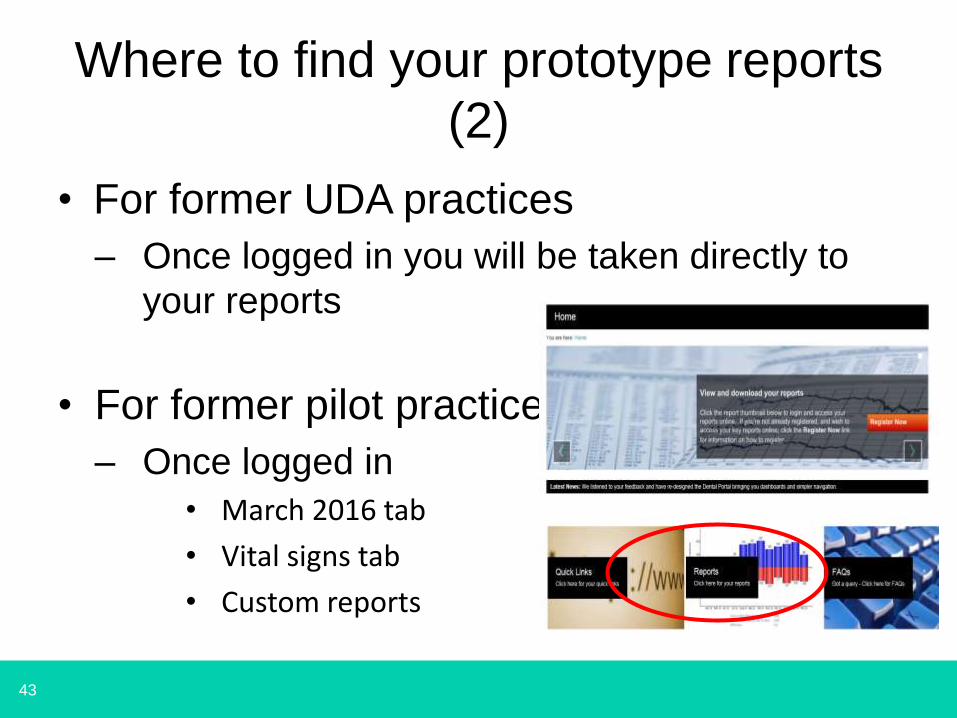
• For former UDA practices
– Once logged in you will be taken directly to
your reports
• For former pilot practices
– Once logged in
• March 2016 tab
• Vital signs tab
• Custom reports
44
Where to find your prototype reports (3)
• No access for performers to their
individual information via pilot portal
• Permanent home for prototype reports will
be within Compass
• Planned date for move to Compass is
August 2016
45
Prototype reports available • A suite of eight reports are produced for prototype
practices each month
• Reports are published in the first full week following month-end– July reports will be available to practices by week ending
5 August 2016
• There is a cut off date for data included in the monthly reports: – Appointment data: 22nd of each month
– FP17 data: This varies slightly each month and the schedule programme for 2016 is available via NHSBSA: http://www.nhsbsa.nhs.uk/i/DentalServices/Schedule_programme_2016.pdf. For July reports the scheduling date is 19 July 2016
46
Prototype reports available (2)
1. Capitation remuneration report
2. Capitation and activity report – performer level
3. Capitated patient list – details
4. Capitated patient list – summary by performer
5. Imminent lapsers – details
6. Imminent lapsers – summary by performer
7. Joiners and leavers – details
8. Joiners and leavers – summary by performer

47
Understanding your current position using the reports
available
48
In your table groups
• Review the example report pack available to discuss
– Which reports do you use to assess overall position of the practice?
– Which other reports do you use regularly, and why?
– Do you have any queries / questions about these reports?
– Are there any other reports / information you would find useful?
49
Understanding your current
position• Key reports:
• Capitation remuneration report‒ Summary of the actual patient numbers on the
capitated patient list against the expected patient numbers for 2016/17 (CECP) and the prototype UDAs delivered against the expected minimum activity level for 2016/17 (EMA)
• Capitation and activity report performer level‒ Performer-level breakdown of the number of
capitated patients and the number of prototype UDAs delivered, as reported on the capitation remuneration report
50
Common questions
51
What triggers capitation?
• A new patient joins the practice patient list when they
attend for an oral health assessment (OHA)
• They will remain on this list for a period of three years
unless they attend for NHS treatment elsewhere, except
where the patient attended another practice for urgent,
referral and charge exempt treatment. In these cases the
patient remains on your practice list
52
What triggers capitation? (2)
• The capitation period is refreshed each time NHSBSA receives notification of the following trigger events:
• Appointment data (DPMS)‒ Any OHA / R appointment
• FP17s‒ Band 1 course of treatment (non-referral, non-urgent)
‒ Band 1a (interim care) course of treatment
‒ Band 2 course of treatment (non-referral)
‒ Band 3 course of treatment (non-referral)

53
What data should we be
transmitting?
• There are two sources of data used to record and update prototype reports:‒ Appointment data (DPMS)
‒ FP17s
• Both data sources should be submitted on a regular basis:‒ Appointment data – we recommend this is done daily.
This data must be submitted within seven calendar days
‒ FP17s – we recommend these are submitted as soon as the course of treatment is complete and no later than two months after the course of treatment is complete
54
Can I transfer a patient list from
one performer to another?
• The facility for “bulk transfers” will be introduced for prototype practices
• This will allow the transfer of a patient list from one performer to another
– The full patient list has to transfer
– Transfers can only be made between performers of the same type, i.e you cannot move patients from a DFT to performer
• An online form will be completed to request a transfer
• Guidance note on how to do this will be issued
55
What is the transitional allowance?
• This applies to former pilots only
• It is an allowance to recognise the change in rule set for counting capitated patients between the pilot and prototype phase
• The calculation is undertaken individually for each former pilot practice
• The allowance (if applicable) is shown section 1 of the capitation remuneration report
56
What is the difference between
scheduled UDAs and completed UDA?
• Scheduled UDAs
‒ Total number of UDAs reported on FP17s received by NHS BSA between the previous cut-off date and the current schedule cut-off
‒ Therefore the June 2016 figure is those UDA received between 18 May and 13 June 2016
‒ This will exclude those FP17s transmitted outside the two-month rule
57
What is the difference between scheduled
UDAs and completed UDA? (2)
• Completed UDAs:
‒ Total number of UDAs reported on FP17s received by NHS BSA allocated to the month in which the treatment was completed
‒ Therefore the June 2016 figure is those UDA completed between 1 June and 13 June 2016
‒ This will exclude those FP17s transmitted outside the two-month rule
58
Relationship between patient
numbers and activity
• As part of their individual prototype
agreement each practice has:
‒ Expected patient list (CECP)
‒ Expected minimum activity level (EMA)
• However, there is the ability within the
prototype agreement to exchange activity
for patient numbers
59
Relationship between patient
numbers and activity (2)
• Practices can over-deliver on patient numbers to compensate for any under-delivery against activity
• If patient numbers are less than or equal to 100% of expected numbers, then any adjustment relating to activity delivery will be capped at a maximum of 100%
• If patient numbers are more than 100% of the expected level, then any adjustment relating to activity delivery will be capped at the same percentage as the achieved level for patient numbers

60
Update on year-end
61
Year-end 2015/16
• Year-end process for 2015/16 is underway
• The dental contract reform programme is working with local offices to calculate individual positions
• Calculation will vary depending on when you commenced as a prototype and also what system you were operating under prior to prototype arrangements
• NHS England will write to individual practices setting out the calculations and any financial adjustment / carry forward (if applicable)
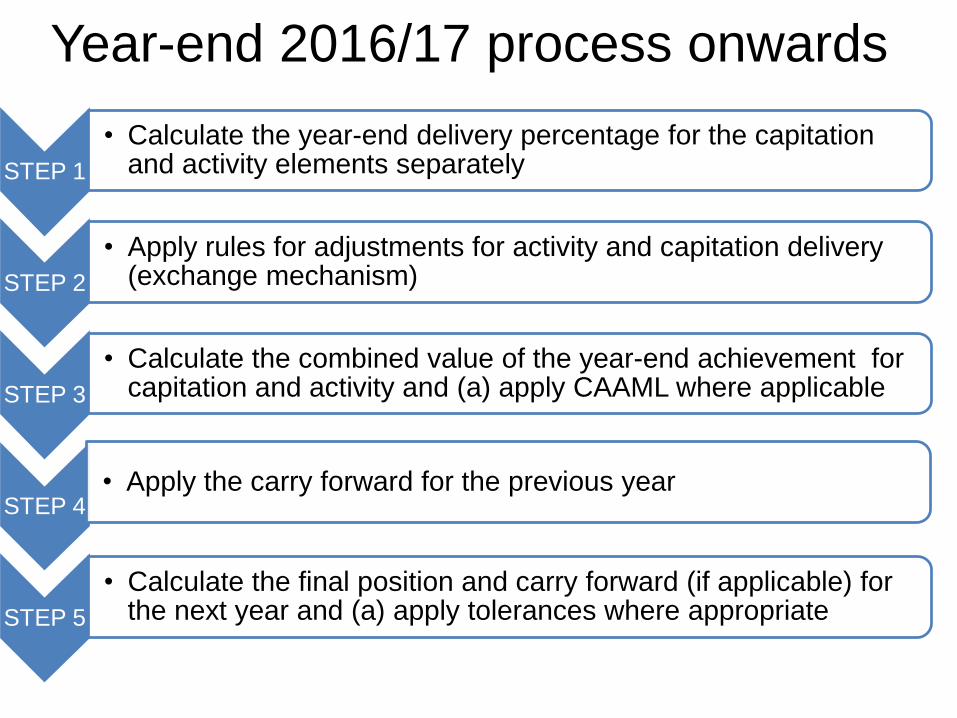
Year-end 2016/17 process onwards
STEP 1
• Calculate the year-end delivery percentage for the capitation and activity elements separately
STEP 2
• Apply rules for adjustments for activity and capitation delivery (exchange mechanism)
STEP 3
• Calculate the combined value of the year-end achievement for capitation and activity and (a) apply CAAML where applicable
STEP 4• Apply the carry forward for the previous year
STEP 5
• Calculate the final position and carry forward (if applicable) for the next year and (a) apply tolerances where appropriate
63
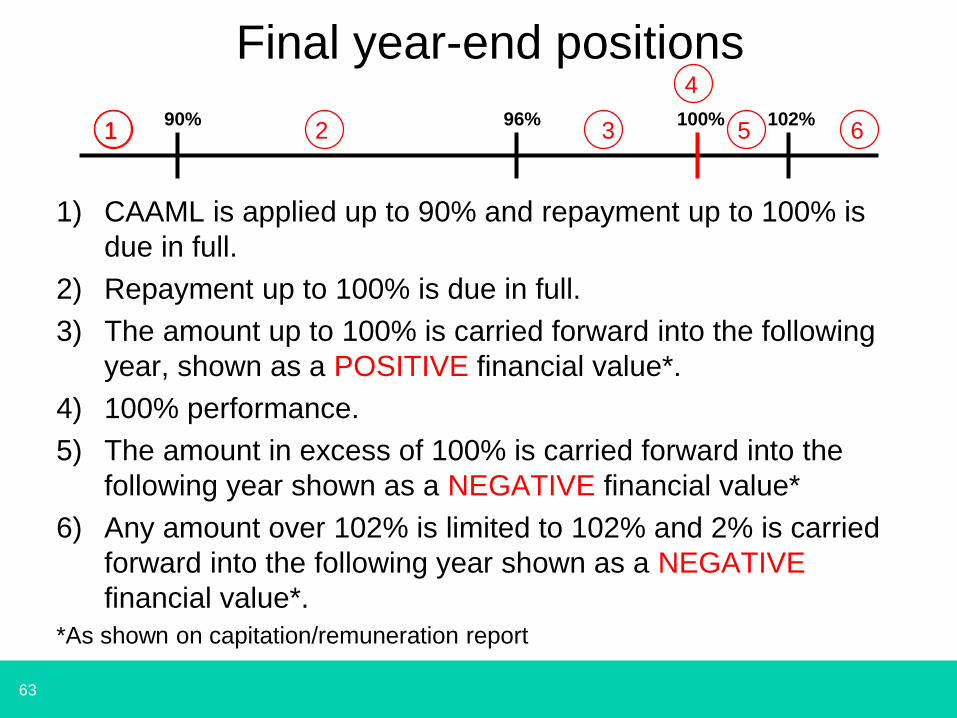
Final year-end positions
100%90% 96% 102%1 2 3 5 6
1) CAAML is applied up to 90% and repayment up to 100% is
due in full.
2) Repayment up to 100% is due in full.
3) The amount up to 100% is carried forward into the following
year, shown as a POSITIVE financial value*.
4) 100% performance.
5) The amount in excess of 100% is carried forward into the
following year shown as a NEGATIVE financial value*
6) Any amount over 102% is limited to 102% and 2% is carried
forward into the following year shown as a NEGATIVE
financial value*.
*As shown on capitation/remuneration report
1
4

64
Help and support
65
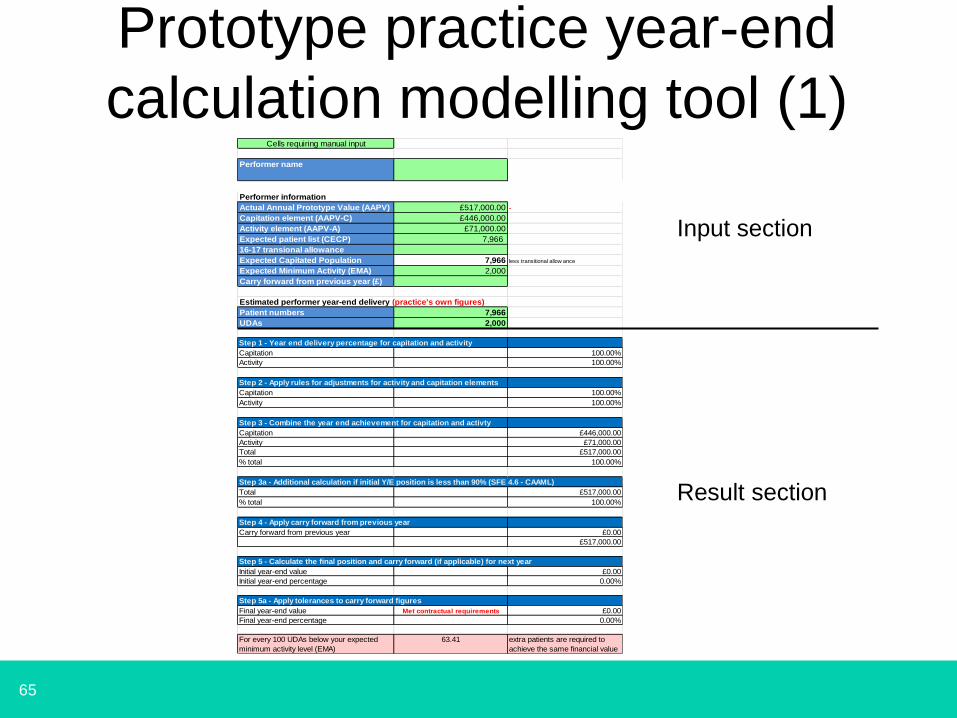
Cells requiring manual input
Performer name
Performer information
Actual Annual Prototype Value (AAPV) £517,000.00 -
Capitation element (AAPV-C) £446,000.00
Activity element (AAPV-A) £71,000.00
Expected patient list (CECP) 7,966
16-17 transional allowance
Expected Capitated Population 7,966 less transitional allow ance
Expected Minimum Activity (EMA) 2,000
Carry forward from previous year (£)
Estimated performer year-end delivery (practice's own figures)
Patient numbers 7,966
UDAs 2,000
Step 1 - Year end delivery percentage for capitation and activity
Capitation 100.00%
Activity 100.00%
Step 2 - Apply rules for adjustments for activity and capitation elements
Capitation 100.00%
Activity 100.00%
Step 3 - Combine the year end achievement for capitation and activty
Capitation £446,000.00
Activity £71,000.00
Total £517,000.00
% total 100.00%
Step 3a - Additional calculation if initial Y/E position is less than 90% (SFE 4.6 - CAAML)
Total £517,000.00
% total 100.00%
Step 4 - Apply carry forward from previous year
Carry forward from previous year £0.00
£517,000.00
Step 5 - Calculate the final position and carry forward (if applicable) for next year
Initial year-end value £0.00
Initial year-end percentage 0.00%
Step 5a - Apply tolerances to carry forward figures
Final year-end value Met contractual requirements £0.00
Final year-end percentage 0.00%
For every 100 UDAs below your expected
minimum activity level (EMA)
63.41 extra patients are required to
achieve the same financial value
Prototype practice year-end
calculation modelling tool (1)
Input section
Result section
66
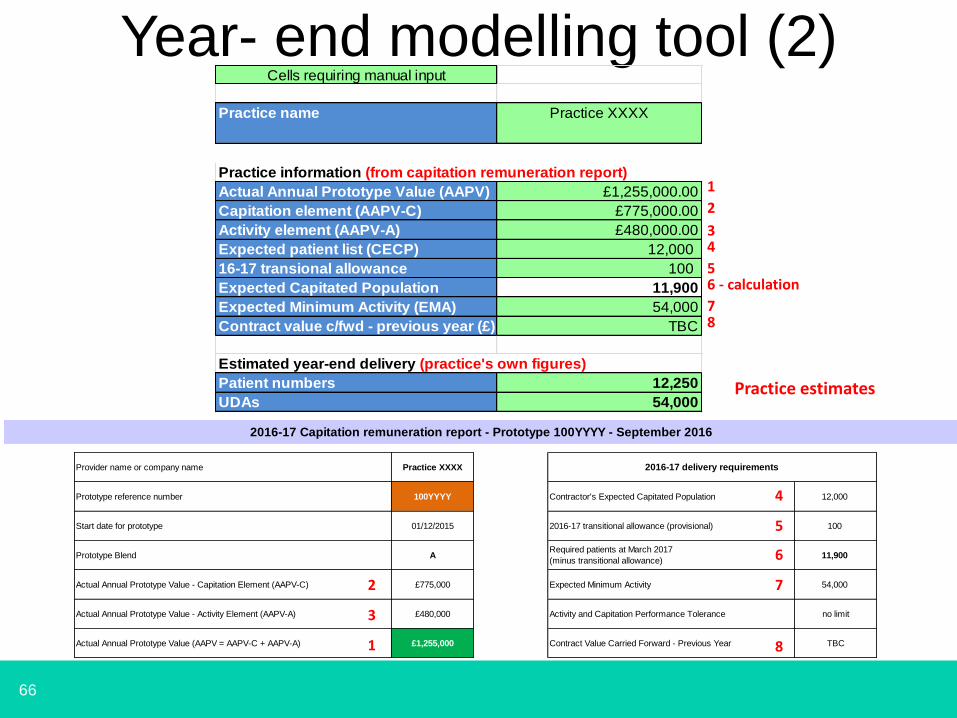
Year- end modelling tool (2)
Provider name or company name Practice XXXX
Prototype reference number 100YYYY 12,000
Start date for prototype 01/12/2015 100
Prototype Blend A 11,900
Actual Annual Prototype Value - Capitation Element (AAPV-C) £775,000 54,000
Actual Annual Prototype Value - Activity Element (AAPV-A) £480,000 no limit
Actual Annual Prototype Value (AAPV = AAPV-C + AAPV-A) £1,255,000 TBC
2016-17 Capitation remuneration report - Prototype 100YYYY - September 2016
2016-17 delivery requirements
Contractor's Expected Capitated Population
2016-17 transitional allowance (provisional)
Required patients at March 2017
(minus transitional allowance)
Expected Minimum Activity
Activity and Capitation Performance Tolerance
Contract Value Carried Forward - Previous Year1
2
3
4
5
6
7
8
1
2
3
56 - calculation
78
4
Cells requiring manual input
Practice name Practice XXXX
Practice information (from capitation remuneration report)
Actual Annual Prototype Value (AAPV) £1,255,000.00
Capitation element (AAPV-C) £775,000.00
Activity element (AAPV-A) £480,000.00
Expected patient list (CECP) 12,000
16-17 transional allowance 100
Expected Capitated Population 11,900
Expected Minimum Activity (EMA) 54,000
Contract value c/fwd - previous year (£) TBC
Estimated year-end delivery (practice's own figures)
Patient numbers 12,250
UDAs 54,000Practice estimates
67
Year-end modelling tool (3)Steps to be carried out:-
1) Input the appropriate data into the identified cells using
the data in the capitation remuneration report.
2) Input your own practice estimates for activity and
capitation.
3) Review the results.
4) Redo (2) above using different figures.
5) Review the results.
6) Redo (2) above using different figures.
7) Review the results
8) ………………………………….
It is a modelling tool
68
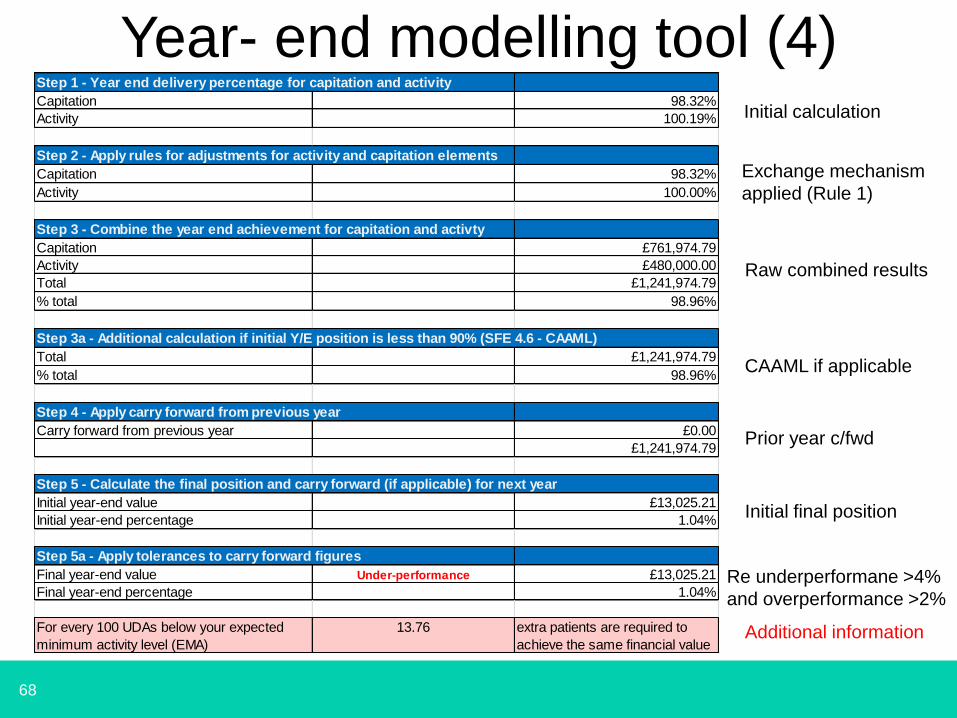
Year- end modelling tool (4)
Exchange mechanism
applied (Rule 1)
Additional information
Initial calculation
Raw combined results
CAAML if applicable
Step 1 - Year end delivery percentage for capitation and activity
Capitation 98.32%
Activity 100.19%
Step 2 - Apply rules for adjustments for activity and capitation elements
Capitation 98.32%
Activity 100.00%
Step 3 - Combine the year end achievement for capitation and activty
Capitation £761,974.79
Activity £480,000.00
Total £1,241,974.79
% total 98.96%
Step 3a - Additional calculation if initial Y/E position is less than 90% (SFE 4.6 - CAAML)
Total £1,241,974.79
% total 98.96%
Step 4 - Apply carry forward from previous year
Carry forward from previous year £0.00
£1,241,974.79
Step 5 - Calculate the final position and carry forward (if applicable) for next year
Initial year-end value £13,025.21
Initial year-end percentage 1.04%
Step 5a - Apply tolerances to carry forward figures
Final year-end value Under-performance £13,025.21
Final year-end percentage 1.04%
For every 100 UDAs below your expected
minimum activity level (EMA)
13.76 extra patients are required to
achieve the same financial value
Prior year c/fwd
Re underperformane >4%
and overperformance >2%
Initial final position
69
In your table groups
• Review the modelling tool examples showing the 6 potential year-end positions in conjunction with the 5 year-end steps– Is the information easy to understand?
– Can you follow the 5 steps?
– Will this tool be useful to you in trying to establish what the impact of your estimated year-end position might be?
– Is there any other information that you need?
– Is the ability to input individual performer data useful?
– What other comments do you have about it?
70
Answering your questions
online support
• Dental contract reform website
• http://www.pcc-cic.org.uk/resources/dental-contract-reform
71
Answering your questions online support
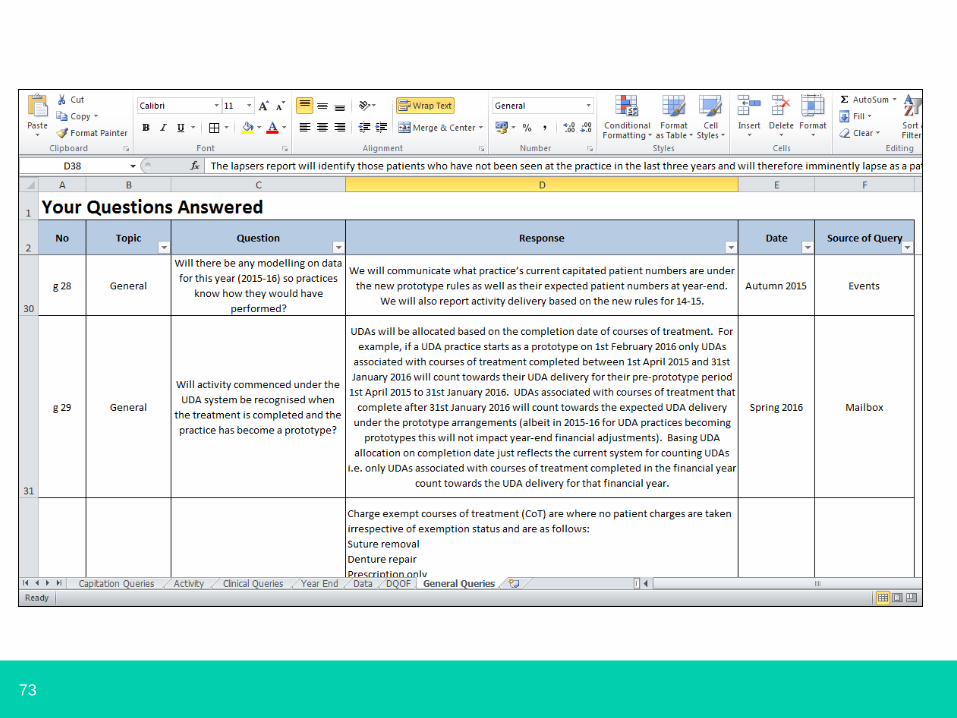
• Sections available:
• Remuneration
• Clinical philosophy
• Making it work clinically
• Making it work in practice
• Contract management
• Your questions answered
72
73
74
Answering your questions
direct support
• Inbox
• Helpdesk
https://helpdesk.pcc-cic.org.uk
75
Any questions?

76
Meet your support team
Summer 2016, London and Leeds
77
Keeping in touch
• Part of the support going forward will be
regular but informal telephone calls with
members of programme support team
• Calls will be every 4-6 weeks
• Supported by a team
• But please don’t wait if there is an urgent
query
78
Open discussion
79
Summary, next steps and close
Summer 2016, London and Leeds
80
Our support for you
• Webpages
• Help desk
• Inbox
• Newsletters
• Buddies
• Future Support
– Keeping in touch calls
– Mid year 1:1 sessions
– Engagement events
– Practice Visits
81
Newsletters
• Monthly news round-up
Summary of key messages and
communication with prototypes
• DCR news
Publication for wider dental profession
and health economies raising
awareness of dental contract reform
82
Helping each other
• 25 prototype practices buddied with 24 ex pilot
practices
• Aim is to provide practices new to reform with;
– Advice from experience
– Support for admin staff
– A sounding board for ideas
83
Future support
• Keeping in touch calls
• Mid year 1:1 sessions
• Engagement events
• Practice visits
84
And finally…..
THANK YOU





























