Embed Size (px)
Citation preview

Centers for Disease Control and PreventionNational Center for Immunization and Respiratory Diseases
Centers for Disease Control and PreventionNational Center for Immunization and Respiratory Diseases
Centers for Disease Control and PreventionNational Center for Immunization and Respiratory Diseases
Centers for Disease Control and PreventionNational Center for Immunization and Respiratory Diseases
Photographs and images included in this presentation are licensed solely for CDC/NCIRD online and presentation use. No rights are implied or extended for use in printing or any use by other CDC CIOs or any external audiences.
November 4, 2017
Shannon Stokley, DrPH
Immunization Services Division
Centers for Disease Control and Prevention

SmallpoxPolio
DiphtheriaPertussisTetanusMeasles
1964 (6)Polio
DiphtheriaPertussisTetanusMeaslesRubellaMumps
1985 (7)
Polio
Diphtheria
Pertussis
Tetanus
Measles
Rubella
Mumps
Hib (infant)
HepB
HepA
Varicella
Pneumococcal
Influenza
Meningococcal
Rotavirus
HPV
PolioDiphtheriaPertussisTetanusMeaslesRubellaMumps
Hib (infant)HepB
Varicella
1995 (10)2017 (16)
Polio
Diphtheria
Pertussis
Tetanus
Measles
Rubella
Mumps
Hib (infant)
HepB
HepA
Varicella
Pneumococcal
Influenza
Meningococcal
Rotavirus
HPV
Number of Diseases Prevented by Vaccines Included in the Routine Child/Adolescent Immunization Schedule

Comparison of 20th Century Annual Morbidity and Current Morbidity: Vaccine-Preventable Diseases
Disease
20th Century
Annual Morbidity†
2015
Reported Cases † †
Percent
Decrease
Smallpox 29,005 0 100%
Diphtheria 21,053 0 100%
Measles 530,217 189 > 99%
Mumps 162,344 1,057 99%
Pertussis 200,752 18,166 91%
Polio (paralytic) 16,316 0 100%
Rubella 47,745 5 > 99%
Congenital Rubella Syndrome 152 1 99%
Tetanus 580 25 96%
Haemophilus influenzae 20,000 23* > 99%
† JAMA. 2007;298(18):2155-2163† † CDC. MMWR January 8, 2016/ 64(52);ND-923 – ND-940. (MMWR 2015 week 52 provisional data)
* Haemophilus influenzae type b (Hib) < 5 years of age. An additional 10 cases of Hib are estimated to
have occurred among the 211 reports of Hi (< 5 years of age) with unknown serotype.

CDC estimates that vaccination of children born between 1994 and 2016:
Prevent 381 million illnesses
Prevent 24.5 million hospitalizations
Help avoid 855,000 early deaths
Save nearly $360 billion in direct costs and $1.65 trillion in total society costs
Every dollar spent in childhood vaccination ultimately saves $10.10.
Childhood Immunization Provides Big SavingsVaccines for Children: 23 years of protecting America’s children
Updated March 2017 from previous article: Benefits from Immunization During the Vaccines for Children Program Era – United States, 1994-2013. MMWR. 25 April 2014

Vaccine Coverage among Children 19-35 Months, National Immunization Survey, United States, 1994-2016
0
10
20
30
40
50
60
70
80
90
1001
99
4
19
95
19
96
19
97
19
98
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
20
11
20
12
20
13
20
14
20
15
20
16
Pe
rce
nt
Vac
cin
ate
d
Year
MMR (1+)
DTP/DTaP (3+)
Polio (3+)
Hib (3+)
HepB (3+)
Varicella (1+)
PCV (4+)
Rotavirus
HepA (2+)
3+HepB
1+ Varicella4+ PCV 2+ HepA
Rotavirus
<1% of toddlers had received no vaccines

Completion of vaccination series by age, National Immunization Survey-Kindergarten (Oct, 2013 – Mar, 2014)
Smith et al. Vaccine. 2017;35:5346-5351.


0
10
20
30
40
50
60
70
80
90
100
2011-12 2012-13 2013-14 2014-15 2015-16 2016-17
Perc
ent
Median and Range* of Measles, Mumps, and Rubella Vaccine (MMR) Coverage, and Exemptions from Any Required Vaccination† among Kindergartners, United States, 2011-12 to 2016-17 School Years
Median MMR Coverage Median Exemption from Any Required Vaccination
Source: School Vaccination Assessment Program, 2011-12, 2012-13, 2013-14, 2014-15, 2015-16, and 2016-17; Available from: https://www.cdc.gov/vaccines/vaxview/index.html.Abbreviations: MMR = measles, mumps, and rubella vaccine.

53.8 54.7
43.1
55.8
86.589.9 90.5 88.6
0
20
40
60
80
100
DTaP Poliovirus MMR Varicella
Exempt Not Exempt
Vaccination coverage by exemption status, National Immunization Survey-Kindergarten (Oct, 2013 – Mar 2014)
Smith et al. Vaccine. 2017;35:5346-5351.
1.9% requested an exemption
95.6% of exempt children had receivedat least 1 dose of vaccine
Children with an exemption receivedan average of 21.8 vaccine doses
Children without an exemption receivedan average of 28.2 vaccine doses

Represents children who are attending kindergarten but do not have documentation of being vaccinated or requesting an exemption
Measles vaccination:– 90.9% vaccinated– 1.1% requested an exemption and unvaccinated– 0.3% provisionally enrolled/grace period and unvaccinated– 7.7% no documentation of vaccination or exemption
Vaccination coverage gap, National Immunization Survey-Kindergarten (Oct, 2013 – Mar 2014)
Smith et al. Vaccine. 2017;35:5346-5351.

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
D C E B P J U O Q T A F G R K I H N L M S
(Wei
ghte
d)
Perc
ent
State
Estimated Percent of Kindergartners with Documented Vaccination for MMR (MMR UTD), Exempt from MMR Vaccination (MMR Exempt), or in the Vaccination-Exemption Gap (VEG)
- Selected States, 2016-17 School Year
Vaccinated Exempt No documentation

10 Years of HPV Vaccination
0
10
20
30
40
50
60
70
80
90
100
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Pe
rce
nt
Vac
cin
ate
d
Survey Year
Tdap
MCV4
1 HPV girls
3 HPV girls
1 HPV boys
3 HPV boys
1 HPV girls &boys
88.0
82.2
65.1
56.0
43.0
31.5
60.4
*Source Walker, et al. MMWR; August 25, 2017 / 66(33);874–882

Number of HPV-Attributable Cancers Averted over 100 Years of 9-Valent HPV Vaccination Program
Estimates calculated using published model (Chesson et al, Hum Vaccin Immunother 2016), with modified coverage assumptions. Coverage levels shown (39.7%, 21.6%, and 80%) refer to coverage among ages 13-17. For females, the annual probability of vaccination in the current coverage scenario was modeled as 20.9% for age 12, 8.9% for ages 13 to 18, and 0.89% for ages 19 to 26. For males, these values were 10.5%, 4.4%, and 0.44% (through age 21), respectively. In the 80% coverage scenario, the annual probability of vaccination was 73.8% for age 12, 8.9% for ages 13 to 18, and 0.89% for those 19 and older (through age 21 for men and age 26 for women).
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
1,800,000
HPV cancers averted total (excluding herd immunity) HPV cancers averted total
Nu
mb
er o
f H
PV
-att
rib
uta
ble
can
cers
ave
rted
2014 coverage (Females 39.7%, Males 21.6%)
Higher male and female coverage (80%)
709,000
1.23 million
Total US population
1.56 million
1.27 million

How do we Communicate with Parents about Vaccines?

Examples of How We Use a Risk Communication Approach
Show empathy--we know parents want to protect their kids
Acknowledge both benefits and risks of vaccines
Cite facts and data whenever possible
Talk about what we don’t know
Give concrete action steps

Frame the Conversation Positively
Source: Opel et al. Pediatrics 2013; 132:1037
Observational study included 93 discussions about vaccines
74% of providers used a presumptive approach– “He’s due for three shots today”
26% used a participatory approach– “What would you like to do about shots?”
Bottom line: Presumptive approach had less parental resistance to immunizations (26% versus 83%)

HPV Vaccination: Announcement vs. Conversation
Will a “conversation” versus an “announcement” of vaccines recommended on the adolescent platform impact uptake?
Brewer NT, Hall ME, Malo TL, et al. Announcements Versus Conversations to Improve HPV Vaccination Coverage: A Randomized Trial. Pediatrics. 2017;139(1):e20161764

Structure of “announcement”
Child is due for 3 vaccines to be given today:
• mentioning the child’s age; • announcing the child is due for 3 vaccines
recommended for children this age, • placing HPV vaccine in the middle of list; and• Saying they will vaccinate today
Brewer NT, Hall ME, Malo TL, et al. Announcements Versus Conversations to Improve HPV Vaccination Coverage: A Randomized Trial. Pediatrics. 2017;139(1):e20161764

6.4
9.5
11.5
14.9
8.4
11.5
0
2
4
6
8
10
12
14
16
3 months 6 months
Pe
rce
nta
ge P
oin
t C
han
ge in
Co
vera
ge
Time Post-training
Control Announcement Conversation
“Announcement” improved HPV vaccine acceptance, compared to “conversation”
Brewer NT, Hall ME, Malo TL, et al. Announcements Versus Conversations to Improve HPV Vaccination Coverage: A Randomized Trial. Pediatrics. 2017;139(1):e20161764
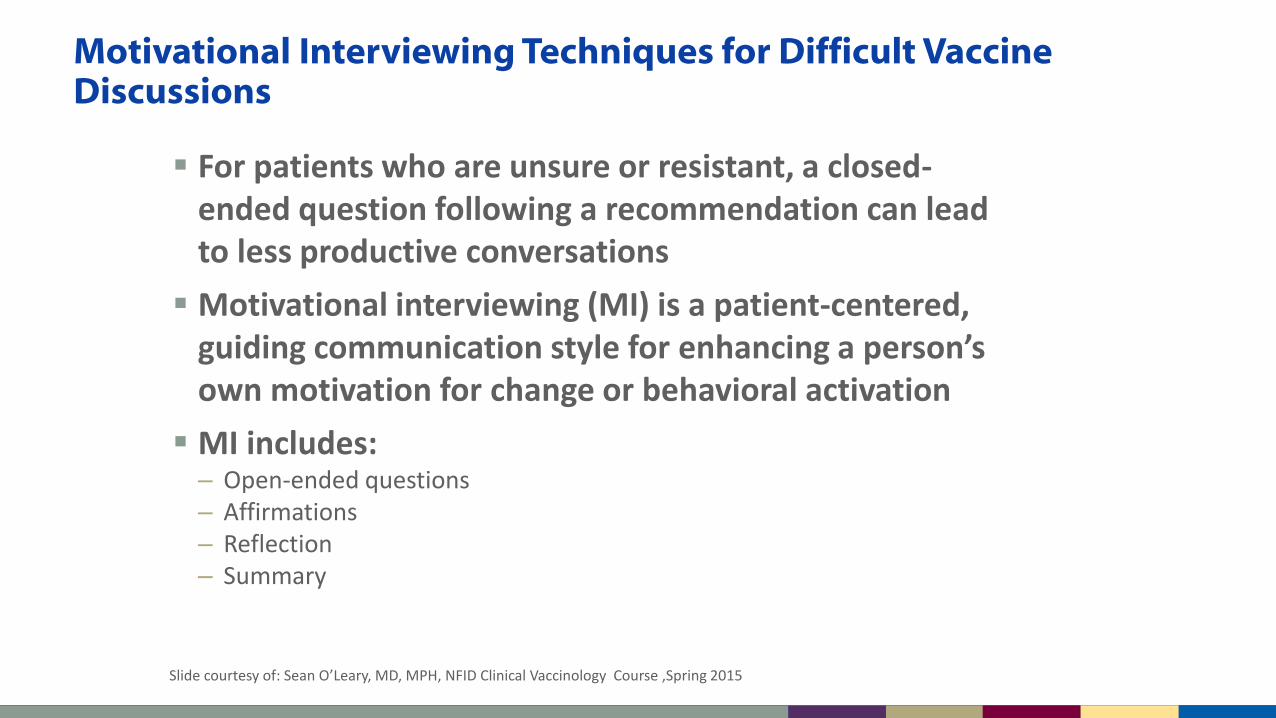
Motivational Interviewing Techniques for Difficult Vaccine Discussions
Slide courtesy of: Sean O’Leary, MD, MPH, NFID Clinical Vaccinology Course ,Spring 2015
For patients who are unsure or resistant, a closed-ended question following a recommendation can lead to less productive conversations
Motivational interviewing (MI) is a patient-centered, guiding communication style for enhancing a person’s own motivation for change or behavioral activation
MI includes:– Open-ended questions – Affirmations – Reflection – Summary

Some Parents Need Reassurance
Many parents simply accept this bundled recommendation
Some parents may be interested in vaccinating, yet still have questions. Interpret a question asthey need additional reassurance from YOU, the clinician they trust with their child’s health care
Ask parents about their main concern (be sure you are addressing their real concern)
Unpublished CDC data, 2013.

Want to See Experts Answering Questions?
www.vaccinateyourbaby.org/faq

#HowIRecommend

Provider Resources for Vaccine Conversations with Parents
Developed with partners AAP and AAFP
Based on formative research and reviewed regularly
Uses risk communication principles
Provides information for conversations on vaccines, vaccine safety, and vaccine preventable diseases
Includes supplemental resources for parents
www.cdc.gov/vaccines/conversations

Resources for Parents
www.cdc.gov/vaccines/partners/childhood/multimedia.html

Resources for Parents: If you Choose not to Vaccinate
For parents who are considering or have decided to delay or refuse recommended vaccines
Discusses:– Steps to take before or during an outbreak to
help protect their family and community– The importance of notifying healthcare
professionals that a child is not fully vaccinated
– Considerations when travelling
Main message: this is not a risk-free choice

For more information, contact CDC1-800-CDC-INFO (232-4636)TTY: 1-888-232-6348 www.cdc.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Photographs and images included in this presentation are licensed solely for CDC/NCIRD online and presentation use. No rights are implied or extended for use in printing or any use by other CDC CIOs or any external audiences.
Thank you!







![Types of vaccines 1 - First generation vaccines are whole-organism vaccines - either live and weakened, or killed forms. [1] Live, attenuated vaccines,](https://img.pdfslide.us/doc/110x75/56649e155503460f94afff0b/types-of-vaccines-1-first-generation-vaccines-are-whole-organism-vaccines.jpg)