Embed Size (px)
Citation preview
Transplantation for Light Chain (AL) and
Transthyreitin (TTR) Amyloidosis
Marc J. Semigran MD
Medical Director Heart Failure and Cardiac Transplantation
Massachusetts General Hospital
Associate Professor of Medicine
Harvard Medical School
Introduction
• Patients with cardiac amyloidosis due to either light chain
(AL) or transthyretin (ATTR) deposition presenting with
moderate or greater heart failure have a median survival of
6-8 months.
• Orthotopic heart transplant (OHT), followed by autologous
stem cell transplantation (ASCT) for AL amyloidosis and
often by orthotopic liver transplant (OLT) for ATTR
amyloidosis, have proven successful in small studies.
• Rapid progression of cardiac amyloidosis, particularly AL, as
well as the limited number of donor hearts, mandates that
we understand patient characteristics and treatments that
will lead to the best possible clinical outcomes. This can
provide insight into the timing of referral.
Introduction
Therefore, ten transplant centers in the US and Europe
agreed to pool their patient data for analysis:
Massachusetts General Hosp, NY Presbyterian Med. Ctr.
Houston Methodist Hosp. Stanford U. Med. Ctr.
University of Padova Newark-Beth Israel Med. Ctr.
Boston U Med. Ctr. Cedars-Sinai Med. Ctr.
Cleveland Clinic UC: San Francisco
Methods
• Patients with AL and ATTR amyloidosis undergoing serial
OHT/ASCT (for AL), or either isolated OHT or OHT/OLT (for
ATTR) between 1998-2014 were identified at each of 10
collaborating institutions in the US & Europe.
• Demographic and clinical characteristics, including measures
of both cardiac and extracardiac manifestations of
amyloidosis were entered into the Research Electronic Data
Capture (REDCap) online clinical data registry.
• For patients with AL amyloidosis, clinical characteristics for
patients waitlisted for transplantation who died prior to
receiving a donor organ and those who survived to OHT
were compared.

Methods
• Survival after OHT in AL and ATTR amyloidosis patients
was compared with a contemporaneous age-matched
population of patients with restrictive cardiomyopathy
reported to the Scientific Registry of Transplant Recipients
(SRTR).
• Univariate and multivariate analysis, using Cox regression,
were used to identify predictors of waitlist mortality in AL
amyloidosis patients, and post transplant survival in AL and
ATTR patients.
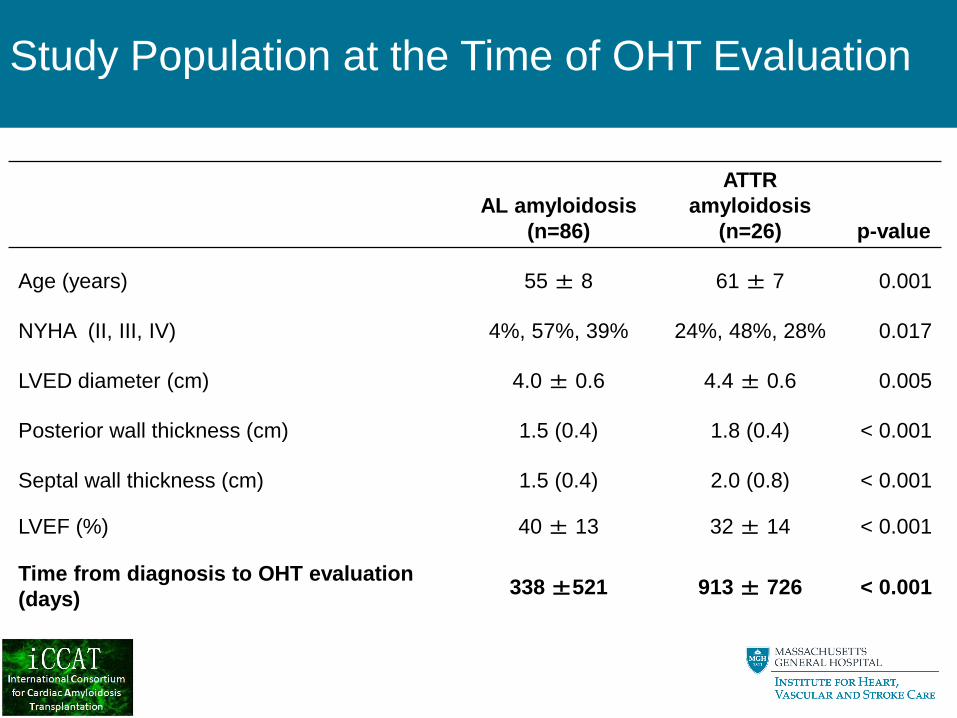
AL amyloidosis
(n=86)
ATTR
amyloidosis
(n=26) p-value
Age (years) 55 ± 8 61 ± 7 0.001
NYHA (II, III, IV) 4%, 57%, 39% 24%, 48%, 28% 0.017
LVED diameter (cm) 4.0 ± 0.6 4.4 ± 0.6 0.005
Posterior wall thickness (cm) 1.5 (0.4) 1.8 (0.4) < 0.001
Septal wall thickness (cm) 1.5 (0.4) 2.0 (0.8) < 0.001
LVEF (%) 40 ± 13 32 ± 14 < 0.001
Time from diagnosis to OHT evaluation
(days) 338 ±521 913 ± 726
< 0.001
Study Population at the Time of OHT Evaluation
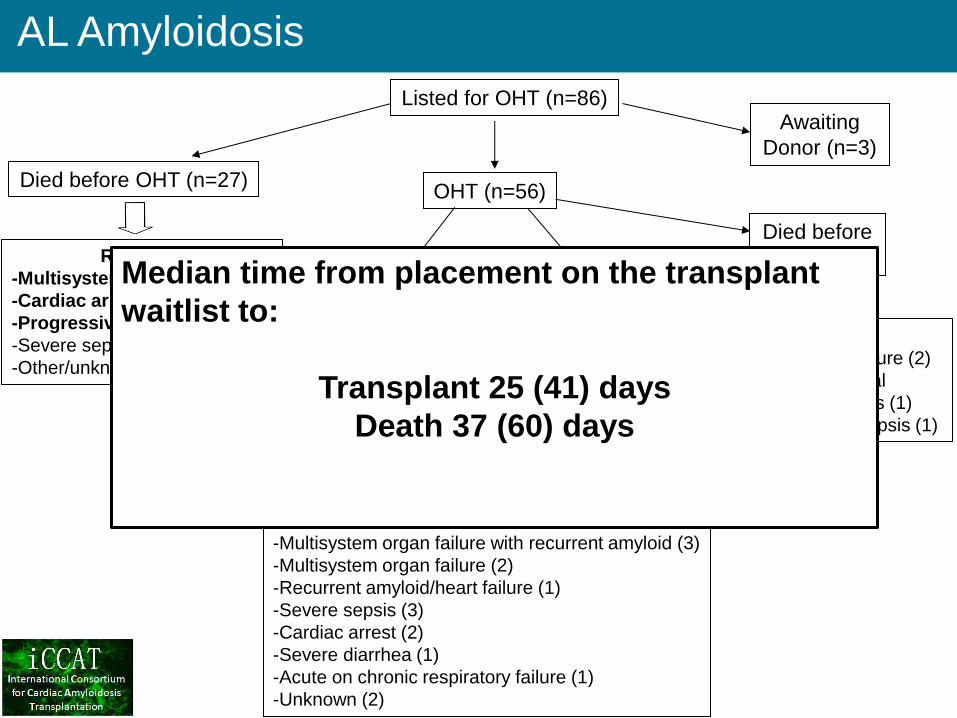
OHT (n=56)
Listed for OHT (n=86)
OHT + ASCT
(n=42)
Died before OHT (n=27)
Reasons:
-Multisystem organ failure (6)
-Cardiac arrest (11)
-Progressive CHF (6)
-Severe sepsis (3)
-Other/unknown (1)
Reasons:
-Multisystem organ failure (2)
-Severe gastrointestinal
hemorrhage and sepsis (1)
-Respiratory failure/ sepsis (1)
Awaiting
Donor (n=3)
Died before
ASCT (n=4)
Died after
ASCT (n=15) Alive at follow-
up (n=27)
Alive, no ASCT
(n=10) -awaiting ASCT (2)
-received chemo (4)
AL Amyloidosis
Reasons:
-Multisystem organ failure with recurrent amyloid (3)
-Multisystem organ failure (2)
-Recurrent amyloid/heart failure (1)
-Severe sepsis (3)
-Cardiac arrest (2)
-Severe diarrhea (1)
-Acute on chronic respiratory failure (1)
-Unknown (2)
Median time from placement on the transplant
waitlist to:
Transplant 25 (41) days
Death 37 (60) days
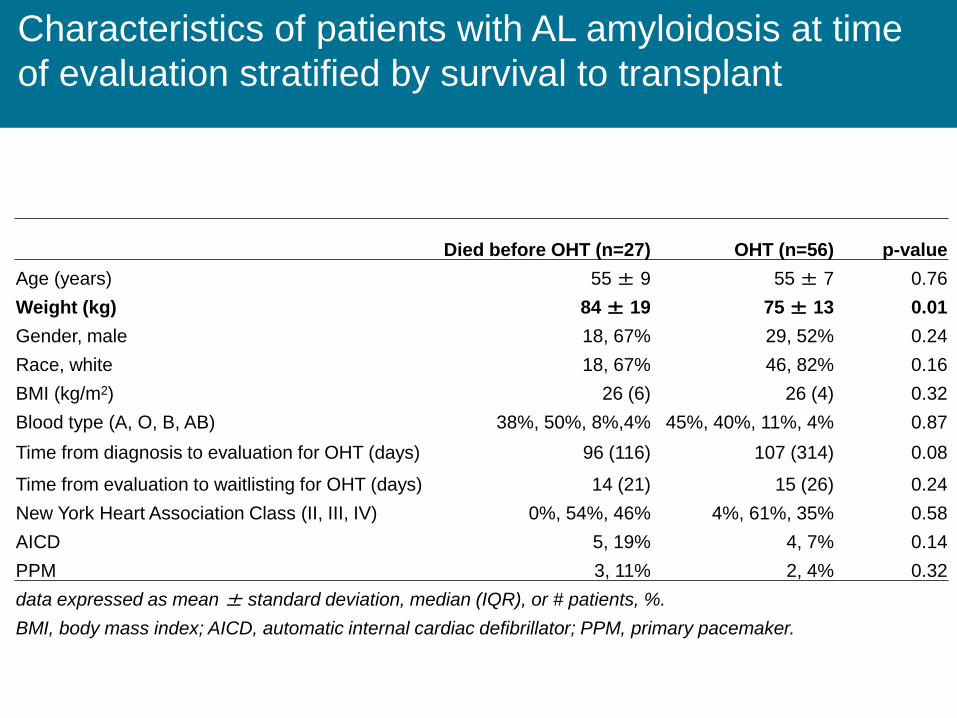
Characteristics of patients with AL amyloidosis at time
of evaluation stratified by survival to transplant
Died before OHT (n=27) OHT (n=56) p-value
Age (years) 55 ± 9 55 ± 7 0.76
Weight (kg) 84 ± 19 75 ± 13 0.01
Gender, male 18, 67% 29, 52% 0.24
Race, white 18, 67% 46, 82% 0.16
BMI (kg/m2) 26 (6) 26 (4) 0.32
Blood type (A, O, B, AB) 38%, 50%, 8%,4% 45%, 40%, 11%, 4% 0.87
Time from diagnosis to evaluation for OHT (days) 96 (116) 107 (314) 0.08
Time from evaluation to waitlisting for OHT (days) 14 (21) 15 (26) 0.24
New York Heart Association Class (II, III, IV) 0%, 54%, 46% 4%, 61%, 35% 0.58
AICD 5, 19% 4, 7% 0.14
PPM 3, 11% 2, 4% 0.32
data expressed as mean ± standard deviation, median (IQR), or # patients, %.
BMI, body mass index; AICD, automatic internal cardiac defibrillator; PPM, primary pacemaker.
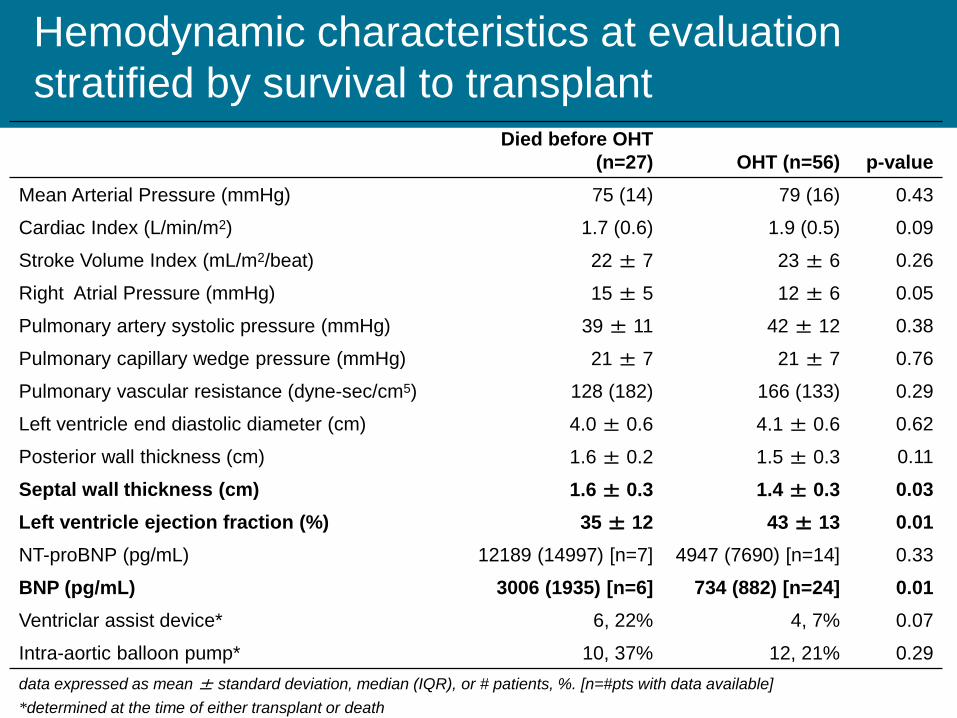
Hemodynamic characteristics at evaluation
stratified by survival to transplant
Died before OHT
(n=27) OHT (n=56) p-value
Mean Arterial Pressure (mmHg) 75 (14) 79 (16) 0.43
Cardiac Index (L/min/m2) 1.7 (0.6) 1.9 (0.5) 0.09
Stroke Volume Index (mL/m2/beat) 22 ± 7 23 ± 6 0.26
Right Atrial Pressure (mmHg) 15 ± 5 12 ± 6 0.05
Pulmonary artery systolic pressure (mmHg) 39 ± 11 42 ± 12 0.38
Pulmonary capillary wedge pressure (mmHg) 21 ± 7 21 ± 7 0.76
Pulmonary vascular resistance (dyne-sec/cm5) 128 (182) 166 (133) 0.29
Left ventricle end diastolic diameter (cm) 4.0 ± 0.6 4.1 ± 0.6 0.62
Posterior wall thickness (cm) 1.6 ± 0.2 1.5 ± 0.3 0.11
Septal wall thickness (cm) 1.6 ± 0.3 1.4 ± 0.3 0.03
Left ventricle ejection fraction (%) 35 ± 12 43 ± 13 0.01
NT-proBNP (pg/mL) 12189 (14997) [n=7] 4947 (7690) [n=14] 0.33
BNP (pg/mL) 3006 (1935) [n=6] 734 (882) [n=24] 0.01
Ventriclar assist device* 6, 22% 4, 7% 0.07
Intra-aortic balloon pump* 10, 37% 12, 21% 0.29
data expressed as mean ± standard deviation, median (IQR), or # patients, %. [n=#pts with data available]
*determined at the time of either transplant or death
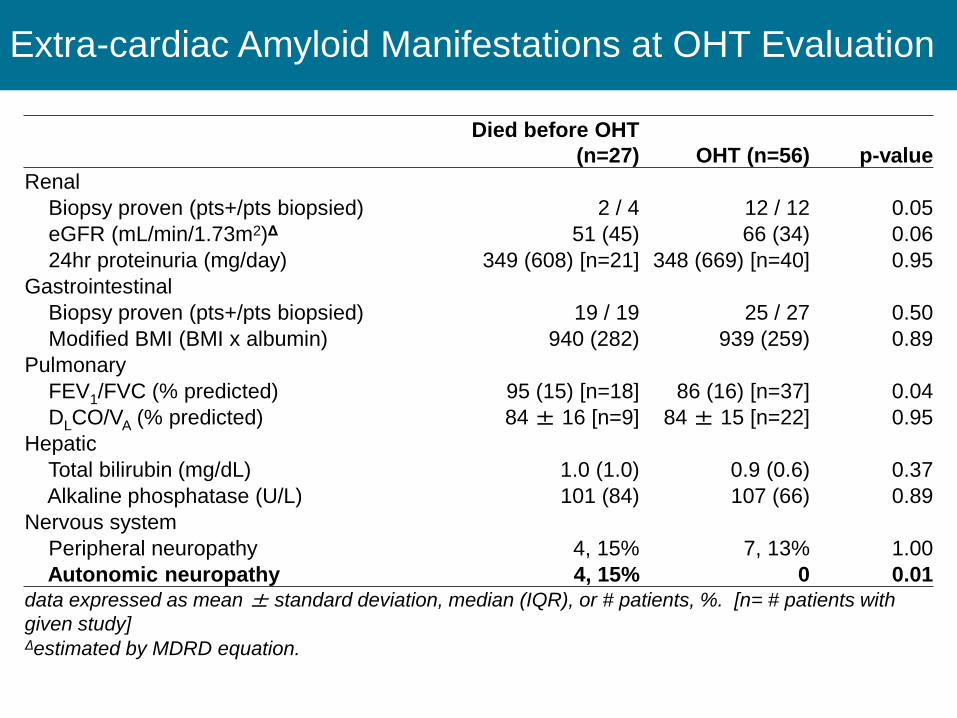
Extra-cardiac Amyloid Manifestations at OHT Evaluation
Died before OHT
(n=27) OHT (n=56) p-value
Renal
Biopsy proven (pts+/pts biopsied) 2 / 4 12 / 12 0.05
eGFR (mL/min/1.73m2)Δ 51 (45) 66 (34) 0.06
24hr proteinuria (mg/day) 349 (608) [n=21] 348 (669) [n=40] 0.95
Gastrointestinal
Biopsy proven (pts+/pts biopsied) 19 / 19 25 / 27 0.50
Modified BMI (BMI x albumin) 940 (282) 939 (259) 0.89
Pulmonary
FEV1/FVC (% predicted) 95 (15) [n=18] 86 (16) [n=37] 0.04
DLCO/VA (% predicted) 84 ± 16 [n=9] 84 ± 15 [n=22] 0.95
Hepatic
Total bilirubin (mg/dL) 1.0 (1.0) 0.9 (0.6) 0.37
Alkaline phosphatase (U/L) 101 (84) 107 (66) 0.89
Nervous system
Peripheral neuropathy 4, 15% 7, 13% 1.00
Autonomic neuropathy 4, 15% 0 0.01
data expressed as mean ± standard deviation, median (IQR), or # patients, %. [n= # patients with
given study] Δestimated by MDRD equation.
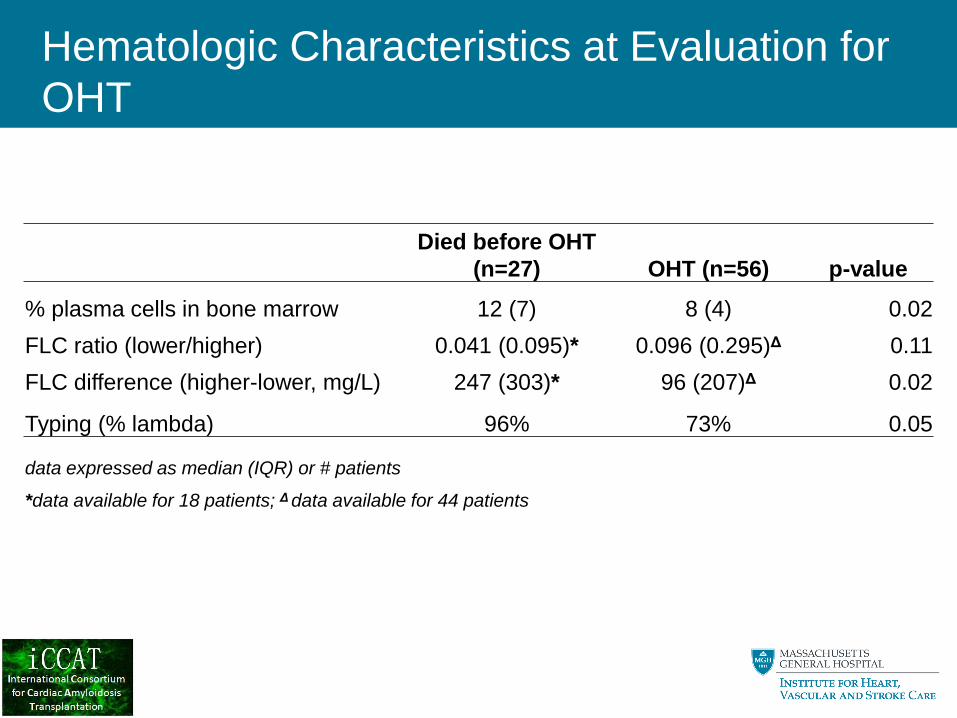
Hematologic Characteristics at Evaluation for
OHT
Died before OHT
(n=27) OHT (n=56) p-value
% plasma cells in bone marrow 12 (7) 8 (4) 0.02
FLC ratio (lower/higher) 0.041 (0.095)* 0.096 (0.295)Δ 0.11
FLC difference (higher-lower, mg/L) 247 (303)* 96 (207)Δ 0.02
Typing (% lambda) 96% 73% 0.05
data expressed as median (IQR) or # patients
*data available for 18 patients; Δ data available for 44 patients
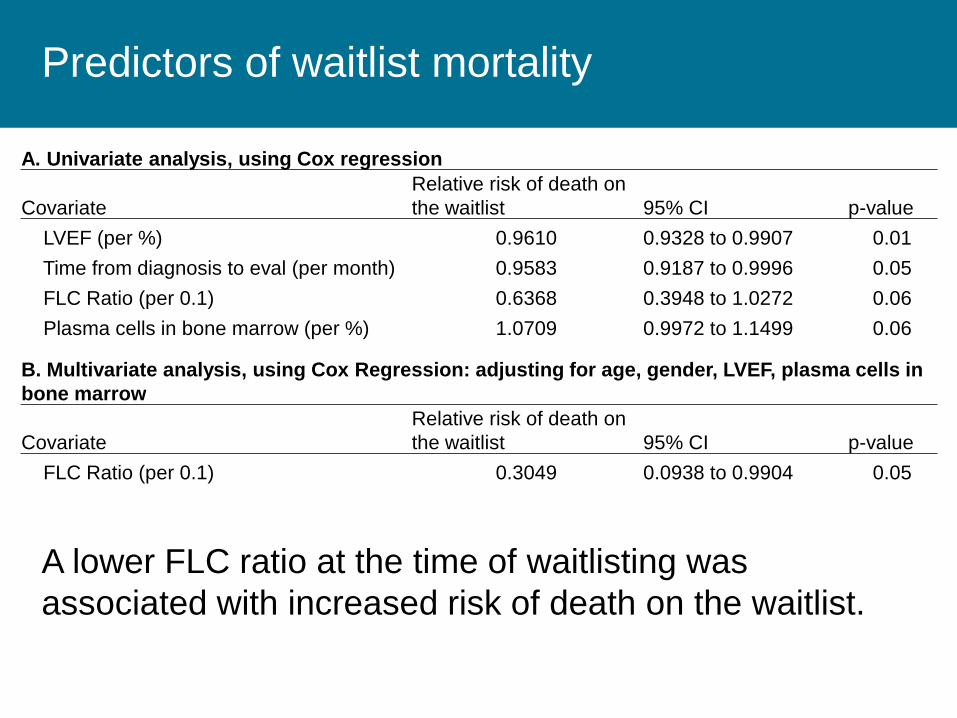
Predictors of waitlist mortality
A. Univariate analysis, using Cox regression
Covariate
Relative risk of death on
the waitlist 95% CI p-value
LVEF (per %) 0.9610 0.9328 to 0.9907 0.01
Time from diagnosis to eval (per month) 0.9583 0.9187 to 0.9996 0.05
FLC Ratio (per 0.1) 0.6368 0.3948 to 1.0272 0.06
Plasma cells in bone marrow (per %) 1.0709 0.9972 to 1.1499 0.06
B. Multivariate analysis, using Cox Regression: adjusting for age, gender, LVEF, plasma cells in
bone marrow
Covariate
Relative risk of death on
the waitlist 95% CI p-value
FLC Ratio (per 0.1) 0.3049 0.0938 to 0.9904 0.05
A lower FLC ratio at the time of waitlisting was
associated with increased risk of death on the waitlist.
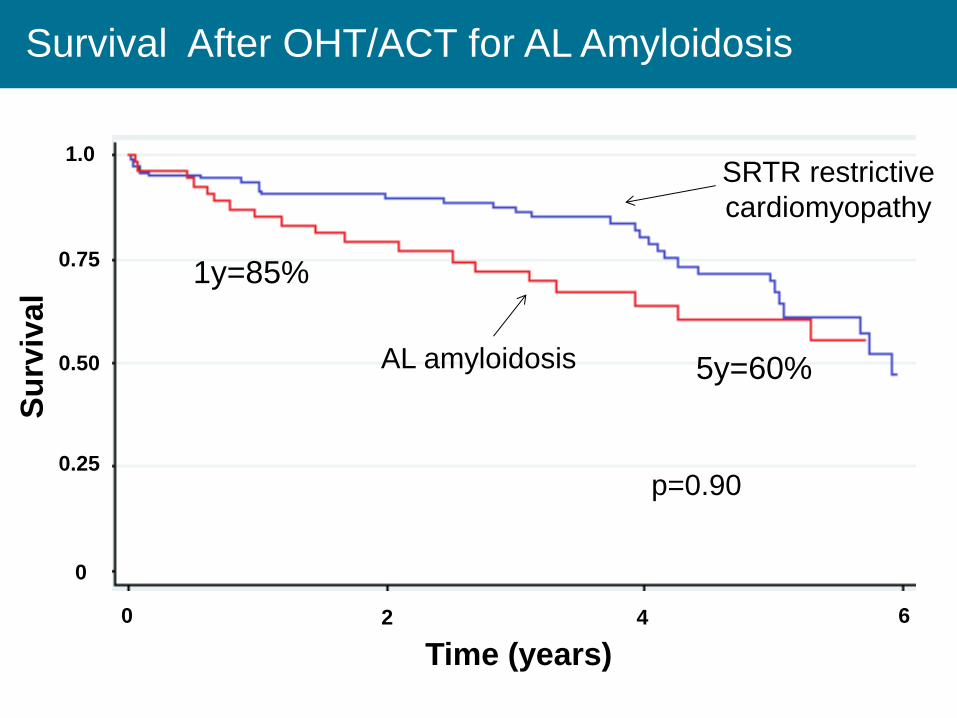
Survival After OHT/ACT for AL Amyloidosis
SRTR restrictive
cardiomyopathy
AL amyloidosis
Time (years)
Su
rviv
al
1.0
0.50
0.25
0
0.75
0 2 4 6
p=0.90
1y=85%
5y=60%
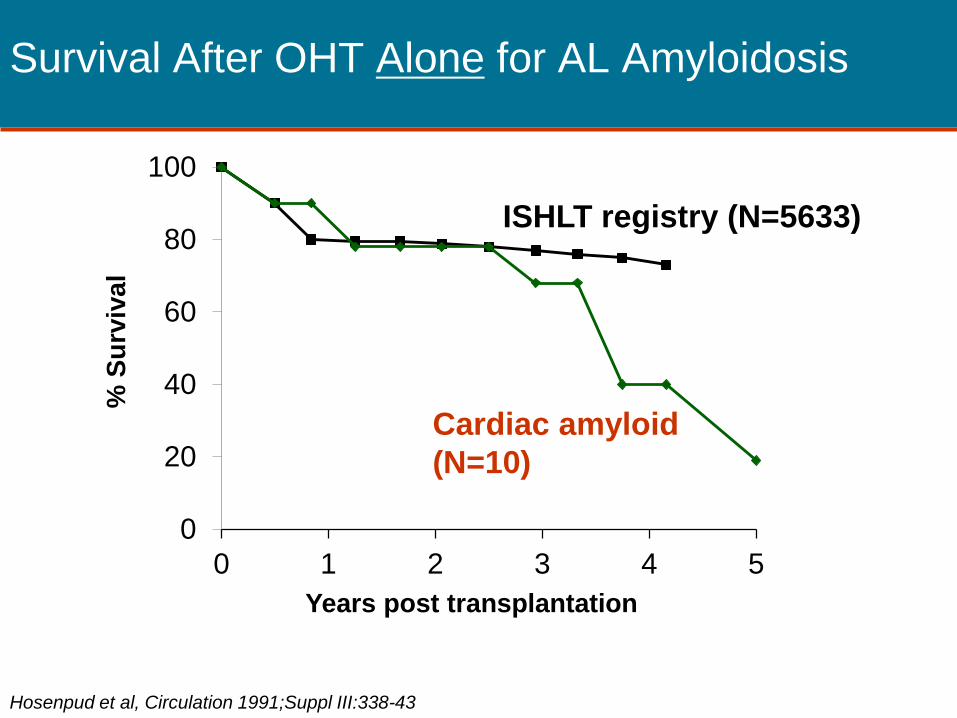
Survival After OHT Alone for AL Amyloidosis
0
20
40
60
80
100
0 1 2 3 4 5
% S
urv
ival
Years post transplantation
Cardiac amyloid
(N=10)
ISHLT registry (N=5633)
Hosenpud et al, Circulation 1991;Suppl III:338-43
15
• No clinical characteristics assessed at the time of evaluation
for OHT were found to predict survival after transplant in AL
amyloidosis patients
• Of patients not treated with chemotherapy prior to OHT
(n=38), the cardiac recurrence rate was 29%.
• Of patients receiving chemotherapy prior to OHT (n=18),
none had recurrence of amyloid in the allograft heart post-
transplant (p=0.01).
Predictors of survival after OHT
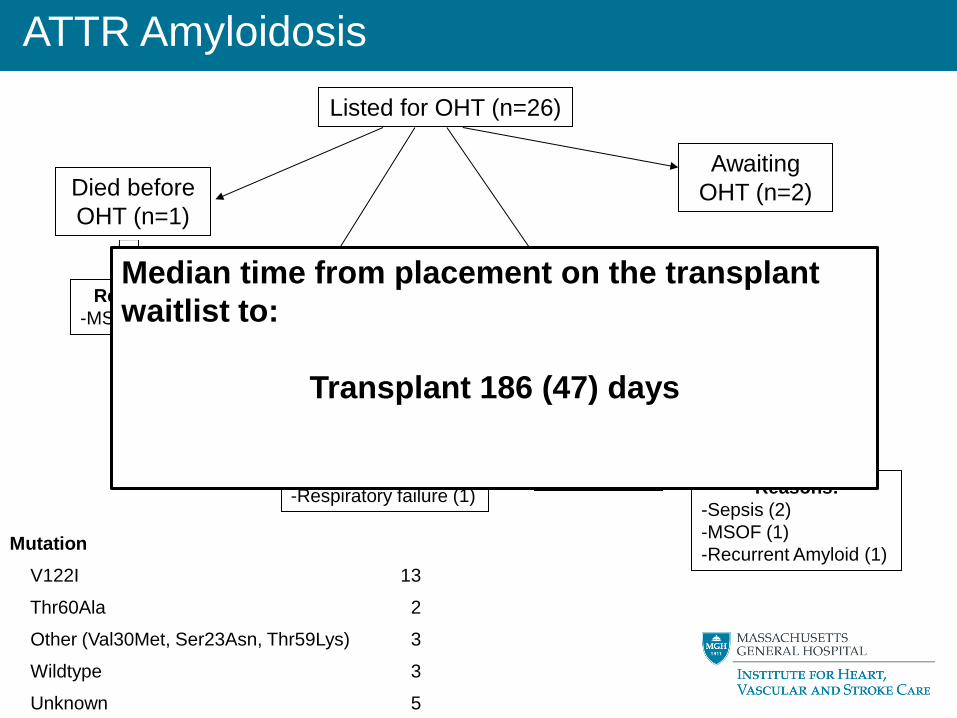
OHT only (n=16)
Listed for OHT (n=26)
Died (n=2) Alive at
follow-up
(n=14)
Died before
OHT (n=1)
Awaiting
OHT (n=2)
Reason:
-MSOF
Reasons:
-Sepsis (1)
-Respiratory failure (1)
OHT + OLT (n=7) -sequential (4)
-concurrent (3)
Died (n=4)
Reasons:
-Sepsis (2)
-MSOF (1)
-Recurrent Amyloid (1)
Alive at
follow-up
(n=3)
ATTR Amyloidosis
Mutation
V122I 13
Thr60Ala 2
Other (Val30Met, Ser23Asn, Thr59Lys) 3
Wildtype 3
Unknown 5
Median time from placement on the transplant
waitlist to:
Transplant 186 (47) days
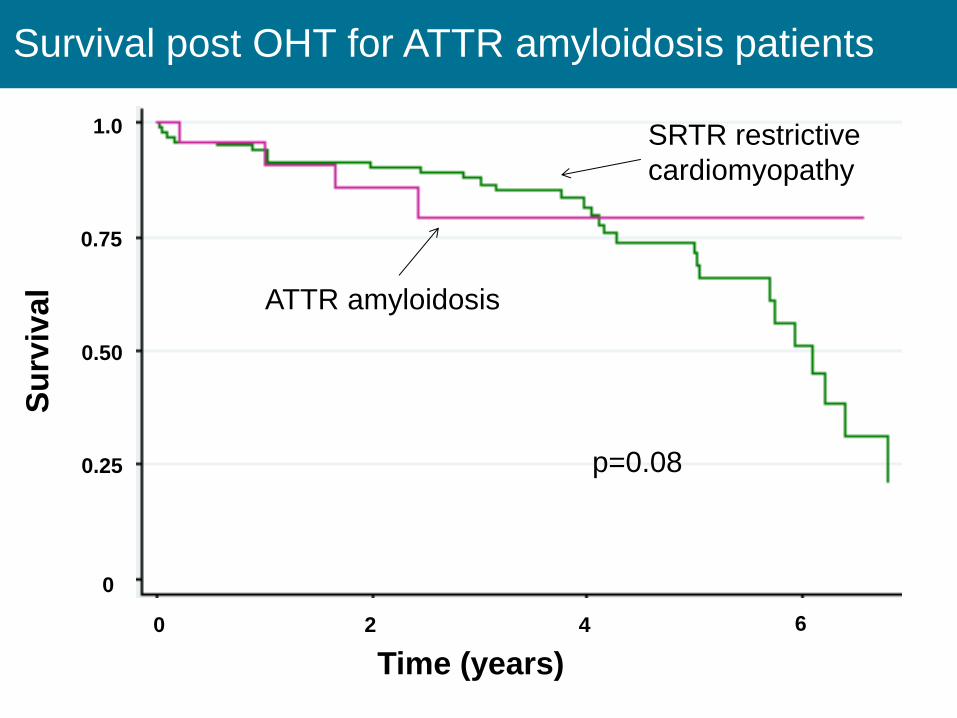
Survival post OHT for ATTR amyloidosis patients
ATTR amyloidosis
SRTR restrictive
cardiomyopathy
1.0
0.75
0.50
0.25
0
Su
rviv
al
Time (years)
2 0 4 6
p=0.08
Summary
1. The rapid progression of AL cardiac amyloidosis is shown by
the significant mortality of patients while awaiting OHT.
2. For AL amyloidosis, those that died while waiting for a donor
heart had higher weight, lower LVEF, and more advanced
hematologic parameters than those that survived to OHT.
3. Cardiac recurrence of amyloid post-transplant occurred in
19% of patients undergoing OHT. No patients treated with
chemotherapy prior to OHT had cardiac recurrence.
4. Survival after heart transplant for either AL or ATTR amyloid
patients is no different than contemporaneous age-matched
groups from the SRTR.
Conclusion
• Orthotopic heart transplant, followed by ASCT for AL and often OLT for ATTR, are appropriate options in the treatment of patients presenting with advanced heart failure due to cardiac amyloidosis. Cardiologists need to diagnose and treat or refer these patients.
• Decreased survival on the transplant waitlist suggests that high-risk AL patients with greater LV wall thickness, depressed LVEF, lower FLC ratio, and λ subtype should be rapidly referred and evaluated for OHT/ASCT.

THANKS!
Alvarez-Munoz J Patel J
Baran D Sarswat N
Cordero A Selby, V
Estep JD Seldin D
Feltrin G Stone JR
Hanna M Tabtabai S
Maurer M Witteles R
Niehaus E, Zucker M

21

AL
Amyloidosis
ATTR
Amyloidosis
Restrictive
Cardiomyopathy*
N 86 26 206
Age (years) 55 ± 8 61 ± 7 55 ± 6
Weight (kg) 77 ± 15 86 ± 23 79 ± 6
Gender, male 48 (56%) 14 (54%) 128 (62%)
Race, white 67 (78%) 12 (46%)
BMI (kg/m2) 26 ± 5 28 ± 8 24 ± 3.0
Time from listing to OHT or death
(days) 57± 72 186 ± 329
Study Population at the Time of OHT Evaluation
*Data obtained at time of transplant

Su
rviv
al
Survival after transplantation
Post-op RRT (n=8)
No post-op RRT (n=46)
Post-op RRT= renal replacement therapy initiated during index transplant hospitalization
Time from OHT to last follow-up/death (years)
5 2 3 4 1 0
0
0.25
0.50
0.75
1.0
Survival post OHT for patients requiring post-op RRT
Log-rank test: p<0.0001