Embed Size (px)
Citation preview

Eumusc.netProf. Loreto CarmonaInstituto de Salud Musculoesquelética, Madrid, España
Professor Anthony Woolf, eumusc.net coordinator

Model for Improvement using Plan-Do-Study-Act
(PDSA) cycles(Institute for Healthcare
Improvement)
Langley GL, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance (2nd edition). San Francisco: Jossey-Bass Publishers; 2009.

Measure to improve
Measure
Implement
Measure
Tune-up
Based on “The model for improved care” by Langley GL et al. ”The Improvement Guide: A Practical Approach to Enhancing Organizational Performance (2nd edition)”. San Francisco: Jossey-Bass Publishers; 2009.

Levels for improvement
Patient
Local
Country

Levels for improvement
Patient
Local
Country
Europe
country
local
Two ways
Europe
Country
Local
P
P
p
Local
P
P
p
Local
P
P
p
Country
Local
P
P
p
Local
P
P
p
Local
P
P
p
Country
Local
P
P
p
Local
P
P
p
Local
P
P
p

Two ways
Europe
Country
Local
P
P
p
Local
P
P
p
Local
P
P
p
Country
Local
P
P
p
Local
P
P
p
Local
P
P
p
Country
Local
P
P
p
Local
P
P
p
Local
P
P
p

Two ways
Europe
Country
Local
P
P
p
Local
P
P
p
Local
P
P
p
Country
Local
P
P
p
Local
P
P
p
Local
P
P
p
Country
Local
P
P
p
Local
P
P
p
Local
P
P
p
More homogeneousLess inequalities

The European Musculoskeletal Conditions Surveillance and Information Network
(eumusc.net)
• 3 year project to raise and harmonise quality of care and enable equity of care of RMD across the Member States.
• Developing and operationalising a relevant health surveillance and information system.
• €1.8 million project supported by:– the European Community (EC Community Action in the Field of
Health 2008-2013) – European League Against Rheumatism (EULAR)
• 22 organisations across 17 countries.

The Ambition
• The EUMUSC.NET project aimed to:– Increase the recognition of the importance of musculoskeletal
health. – Integrate musculoskeletal health policy with those of other
chronic diseases.– Gain priority for research and programmes that will lead to
better musculoskeletal health taking into account health inequalities.
– Increase the political salience of reducing the burden of RMD on both individuals and society.
– Promote the execution of evidence-based strategies.– Keep people at work despite their musculoskeletal condition.

The Approach
Establishment of standards of information,
accessible to patients, healthcare professionals
and policy informers
Organisation into a series of Work Packages
Outcome = recommendations to
improve the delivery of Standards of Care across the EU Member States

Eumusc.net work packages
Work Package 4• Led by Royal Cornwall Hospitals Trust
(UK)• The impact of RMD on
individuals and society
Work Package 5• Led by Medizinische Universität Wien
(AT)• Patient centred standards
of care for OA and RA across Europe
Work Package 6• Led by Lund University (SE)• Health Care Quality
Indicators
Work Package 7• Led by Diakonhjemmet Sykehus AS
(NO)• Barriers and facilitators to
the implementation of the selected standards of care
WP4 Musculoskeletal health measure
• An Atlas of the Burden of RMD across Europe. – Based on agreed indicators of musculoskeletal health.– Using an assessment tool so that standardised information can
be collected.– Results available directly on the web based information system. – Inequalities in outcomes across Member States can be
identified.
The aim, in the long term, would be for much of the relevant data to be collected routinely by integrating with health monitoring systems e.g. EHIS.
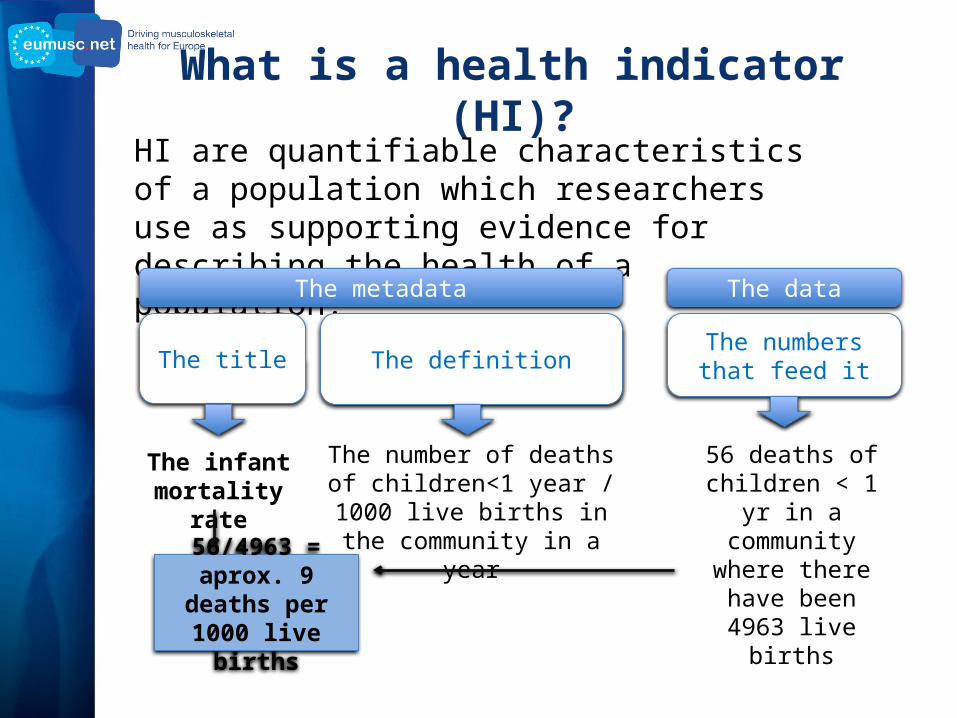
What is a health indicator (HI)?HI are quantifiable characteristics of a population which researchers use as supporting evidence for describing the health of a population.
The metadata The data
The title The definitionThe numbers that
feed it
The infant mortality rate
The number of deaths of children<1 year / 1000 live births
in the community in a year
56 deaths of children < 1 yr in a community where there have been 4963 live births56/4963 = aprox.
9 deaths per 1000 live births

How did we generate indicators? (Health and quality indicators)
Decide on domain• Structure – process – outcome
Propose specific figures that can be measured
Assess validity and agreement
Think-tank / consensus

Assess “validity”: 10 basic questions• What is being measured?• Why is being measured?• How is this indicator actually defined?• Who does it measure it?• When do we measure it?• Where do the data actually come from?• How accurate and complete will the data be?• Are there any caveats/warnings/problems?• Will it measure absolute numbers or proportions?• Are particular tests needed such as standardisation, or statistical
controls to test the meaning of the data and the variation they show?

The definition of HI (Web-based information system)
The assessment tool
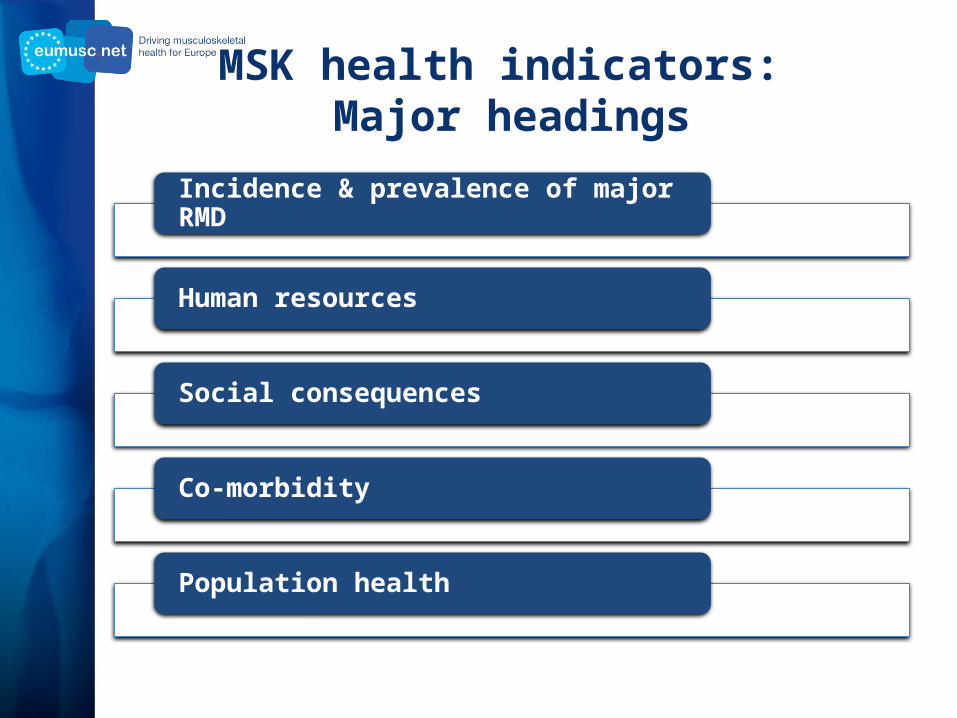
MSK health indicators: Major headings
Incidence & prevalence of major RMD
Human resources
Social consequences
Co-morbidity
Population health

Incidence & prevalence of major RMD
• Prevalence of (ever, doctor diagnosed, and doctor diagnosed in the past 12 months)– low back pain – neck disorder or defect (ever) – rheumatoid arthritis (ever) – osteoarthritis (ever) – osteoporosis (ever)
• Incidence of hip fracture

Others
• Number of surgeries – hip arthroplasty – knee arthroplasty
• Primary care visits related to musculoskeletal conditions • Number Orthopaedic surgeons per 100,000 inhabitants
• Work loss due to musculoskeletal conditions • Temporary work loss due to musculoskeletal conditions
• Obesity • Co-morbidity musculoskeletal condition and obesity • Physical activity

Sources of data
• Surveys– EHIS & EHIS based surveys– Eurobarometer Reports– Eurostat– Research driven
• Audits– WHO European Hospital Morbidity Data– OECD Health Data– National– Research driven
• National statistics– Agencies– Health ministries
Surveillance network

Musculoskeletal health is closely related to political decisions.
Will we ever know if we are improving the health of Europeans if we don’t measure?
Please, include indicators of musculoskeletal health in your routine data collection
Policies leading to ↑physical activity ↓obesity ↑research ↓barriers to
access best care ↑knowledge ↓work harms

Spain’s case: the National Strategy for RMD

Eumusc.net work packages
Work Package 4• Led by Royal Cornwall Hospitals Trust
(UK)• The impact of RMD on
individuals and society
Work Package 5• Led by Medizinische Universität Wien
(AT)• Patient centred standards
of care for OA and RA across Europe
Work Package 6• Led by Lund University (SE)• Health Care Quality
Indicators
Work Package 7• Led by Diakonhjemmet Sykehus AS
(NO)• Barriers and facilitators to
the implementation of the selected standards of care

Aims of WP5
• To develop user-focused Standards of Care (SOCs)
– for RA and OA – together with a patient
check-list– Use of national and
international guidelines as basis
• To translate into all EU languages
– the SOCs – and the check-list
Michaela Stoffer

WP5: Patient centred standards of care for OA and RA across Europe
SR on recommendations and guidelines in OA and RA
Selection and Evaluation of documents- using the AGREE criteria
Extracting all mentioned means and methods and recommendations
Informed discussion on the means/ methods/ recommendations and to formulate the user–focused SOC
WP5: Patient centred standards of care for OA and RA across Europe

Example: RA SOC
49 Interventions
link to Recommendations
7 Main Groups
16 Standards of Care

Example linking SOC RA 3 to Check List Question
•People with RA should receive a treatment plan developed individually between them and their clinician at each visit.
Standard of Care
•Have I received a treatment plan which includes explanation of my management, expected goals and outcomes and important contact details?
Check List

ARD publications
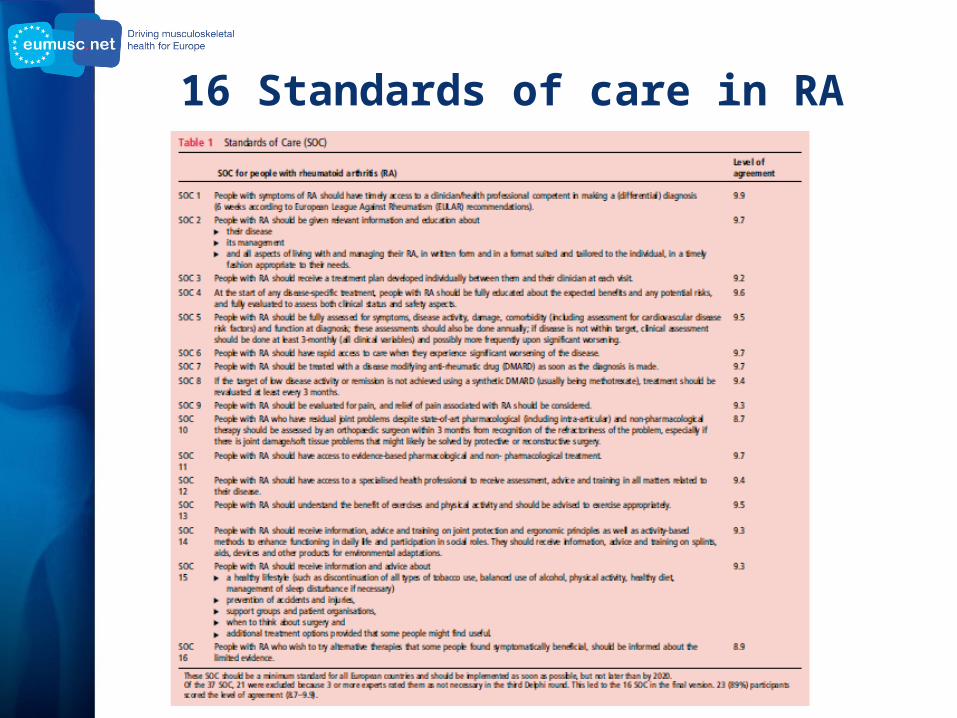
16 Standards of care in RA

16 item checklist for persons with RA

10 SOC for OA

10 item checklist for essential care in OA

Example of LIRE’s use of the SOC
checklists

Eumusc.net work packages
Work Package 4• Led by Royal Cornwall Hospitals Trust
(UK)• The impact of RMD on
individuals and society
Work Package 5• Led by Medizinische Universität Wien
(AT)• Patient centred standards
of care for OA and RA across Europe
Work Package 6• Led by Lund University (SE)• Health Care Quality
Indicators
Work Package 7• Led by Diakonhjemmet Sykehus AS
(NO)• Barriers and facilitators to
the implementation of the selected standards of care

WP6 Health Care Quality Indicators
SR on HQCI
Selection
Test
The eumusc.net SOCs for RA were
developed in parallel.
Prof. Ingemar Petterson

SR on HQCI
6 HQCI setsMainly process
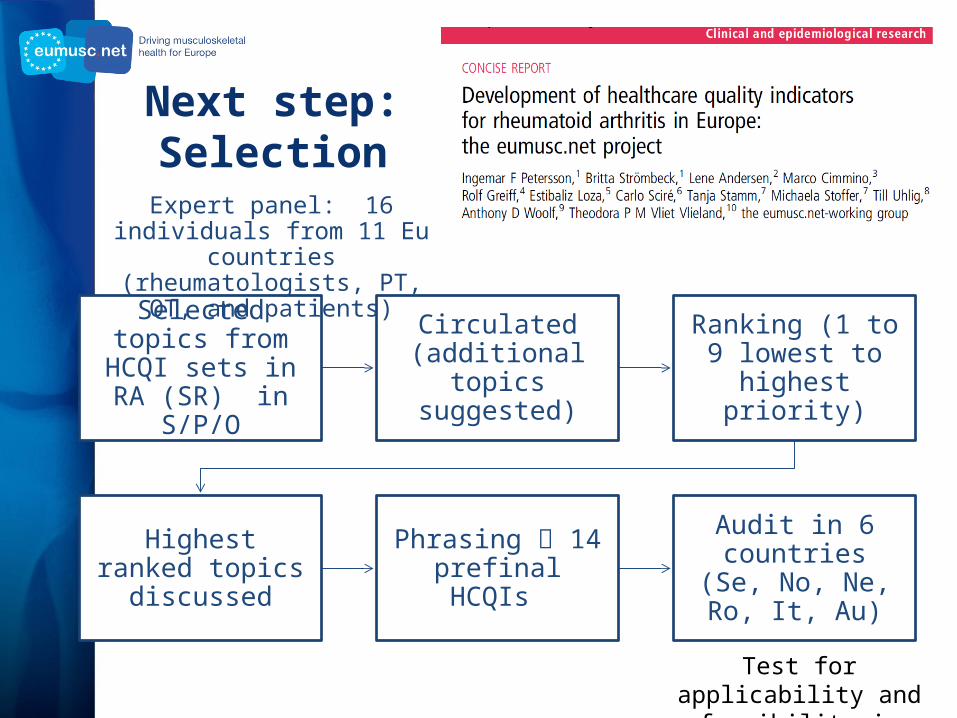
Next step: Selection
Selected topics from HCQI sets in RA (SR) in S/P/O
Circulated (additional topics
suggested)
Ranking (1 to 9 lowest to highest
priority)
Highest ranked topics discussed
Phrasing 14 prefinal HCQIs
Audit in 6 countries (Se, No, Ne, Ro, It,
Au)
Expert panel: 16 individuals from 11 Eu countries (rheumatologists,
PT, OT, and patients)
Test for applicability and feasibility in clinical practice

Example of 1 of the 14 HQCI

Results from the audit

Eumusc.net work packages
Work Package 4• Led by Royal Cornwall Hospitals Trust
(UK)• The impact of RMD on
individuals and society
Work Package 5• Led by Medizinische Universität Wien
(AT)• Patient centred standards
of care for OA and RA across Europe
Work Package 6• Led by Lund University (SE)• Health Care Quality
Indicators
Work Package 7• Led by Diakonhjemmet Sykehus AS
(NO)• Barriers and facilitators to
the implementation of the selected standards of care
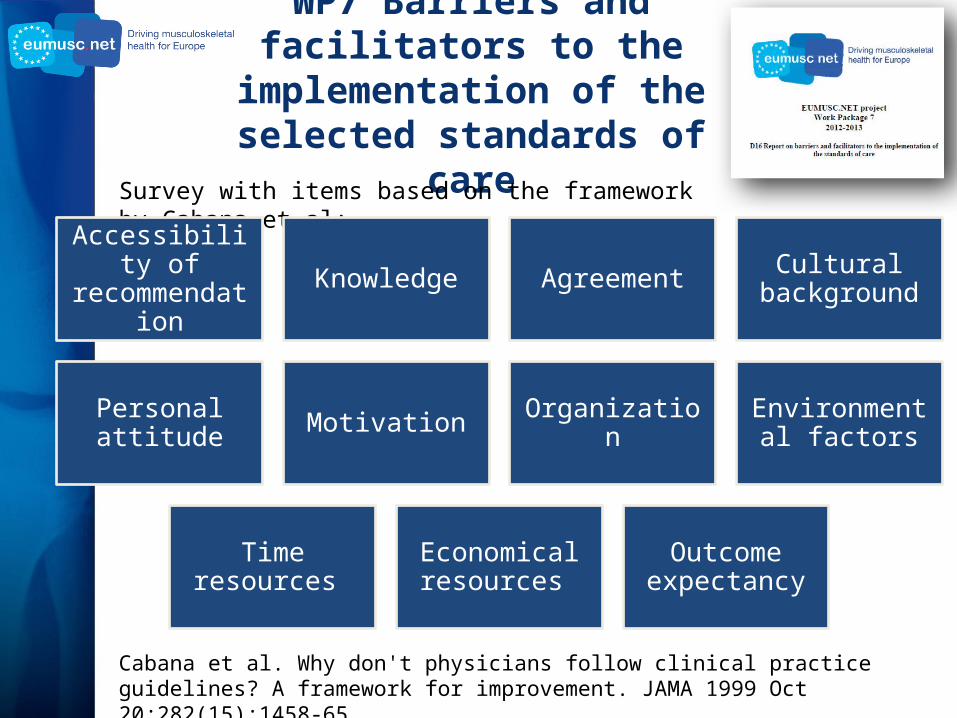
WP7 Barriers and facilitators to the implementation of the
selected standards of careSurvey with items based on the framework by Cabana et al:
Cabana et al. Why don't physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999 Oct 20;282(15):1458-65.
Accessibility of recommendation Knowledge Agreement Cultural
background
Personal attitude Motivation Organization Environmental factors
Time resources Economical resources
Outcome expectancy
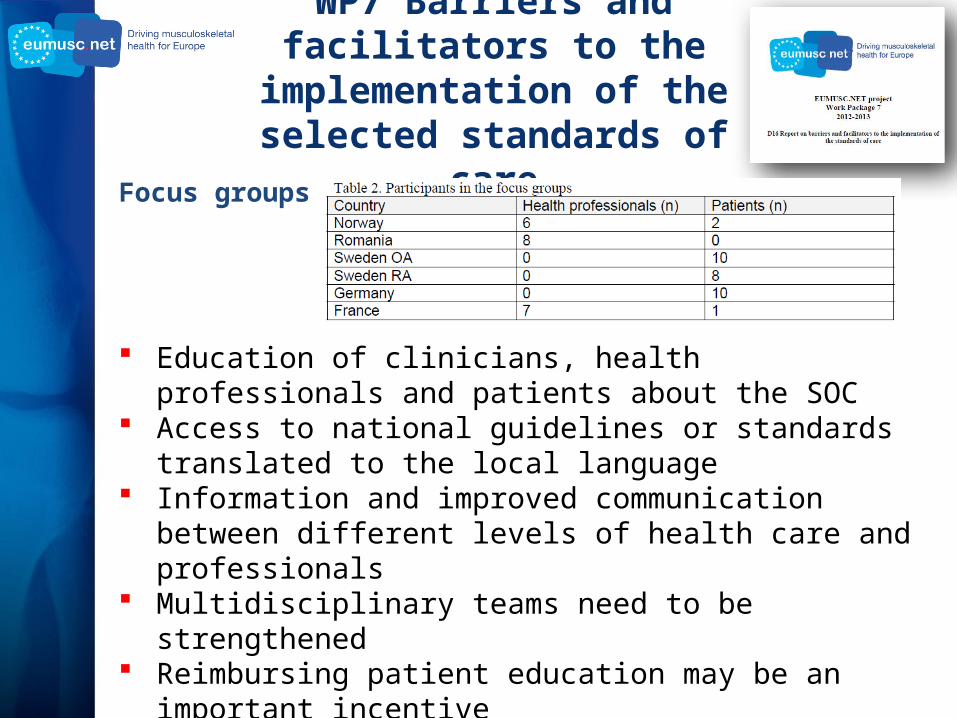
WP7 Barriers and facilitators to the implementation of the selected standards of care
Focus groups:
Education of clinicians, health professionals and patients about the SOC
Access to national guidelines or standards translated to the local language
Information and improved communication between different levels of health care and professionals
Multidisciplinary teams need to be strengthened Reimbursing patient education may be an important incentive Some health economic systems need to be changed to avoid
inequity of care

Good practice examples

Summary: Have we met our objectives?
• The EUMUSC.NET project aimed to:– Increase the recognition of the importance of musculoskeletal
health. – Integrate musculoskeletal health policy with those of other
chronic diseases.– Gain priority for research and programmes that will lead to
better musculoskeletal health taking into account health inequalities.
– Increase the political salience of reducing the burden of RMD on both individuals and society.
– Promote the execution of evidence-based strategies.– Keep people at work despite their musculoskeletal condition.

¡Muchas gracias!