Embed Size (px)
Citation preview

HEALTH SCENARIO IN SRI LANKA
Dr.Bharat k
MPH 2014
PADMASHREE SCHOOL OF PUBLIC HEALTH. BANGALORE
Introduction:
Sri Lanka is an island country located off the southern coast of India. Sri Lanka is surrounded by the Indian Ocean, Gulf of Mannar, the Palk Strait, and lies in the vicinity of India and Maldives.
The geography of Sri Lanka includes coastal plains in the north and hills and mountains in the interior.
The government system is a republic. The chief of state and head of government is the President.
Sri Lanka is a member of Bay of Bengal Initiative for MultiSectoral Technical and Economic Cooperation (BIMSTEC) and the South Asian Association for Regional Cooperation (SAARC).


Basic Facts about Sri Lanka:
Total Land Area: 65,610 KM2
Total Population: 20.48 million (2013)
GDP per capita, PPP (current international $): $9,736(2013)
Life expectancy at birth (2012): 71(MALE)/78(FEMALE)
Total expenditure on Health Per Capita(Int $ 2012): 189
Total Expenditure on Health as % of GDP(2012): 3.2
Country Risk Ranking: C
Infant Mortality Rate: 14.35/1000 LB
Maternal Mortality Rate : 23 / 10,000 live births
Under five mortality rate:12.9/1000
Access to Sanitation: 72.6%
Maternal Malnutrition: 48%
Current use of contraception :70% (**rising teenage pregnancies in HSZ)
Total fertility rate(total births per woman): 2.3 (2010)
Immunization coverage :80.7% (under 5 years with a health card)
Hospital Beds: 3.6/1000 Beds
Doctors: 2300 persons/Doctor
Nurses: 826persons /staff nurse
Global Competitiveness Report: 4.218 (65 out of 148)
Adult Literacy Rate: 92.3
Source: Health System Assessment in North and East of Sri Lanka, WHO, Sri Lanka 2012 extracted from Annual Health Bulletin 1999, 2000 and statistical Health book NEP 2000, DHS survey 2001
HEALTH SECTOR IN SRI LANKA Sri Lanka has achieved a commendable health status measured in terms of
traditional health indices in relation to its Gross Domestic Product (GDP).
Sri Lanka provides free universal healthcare.
One of the few countries in the world with free healthcare and education, both of which have been national priorities for decades.
Both the Government and Private sector have been rapidly building and improving infrastructure, quality of services and human capital base in the healthcare sector.
Sri Lanka has a unique healthcare system where one can go directly to the hospital (government or private), to the family GP or directly see a specialist – with no reference from a 3rd party.
HOSPITAL SYSTEM:
Government hospitals have been the primary mode by which modern medical treatment has been made available to people in rural areas.
OPD facilities are readily available in public (general) hospitals situated in major towns and cities, with laboratory and radiology facilities common in most.
Widely anything can be dealt with in the teaching hospitals in Colombo, Colombo South, Colombo North, Kandy/ Peradeniya, Galle (Karapitiya Hospital) and Jaffna.
For emergencies, especially accidents, it is highly recommended to go directly to General hospital accident services as they are equipped with the staff and facilities to handle emergencies.
In most cases of serious accidents, private hospitals refer patients to General hospitals. This is mostly due to the high investment in equipment and staff training in the public healthcare sector.
Many new private hospitals have been opened across the country due to rising income of people and demand for private healthcare.

WHO Ranking: The World’s Health Systems
Sri Lanka-76
France-1
Singapore-6
USA -37
India- 112
Pakistan-122
China-144
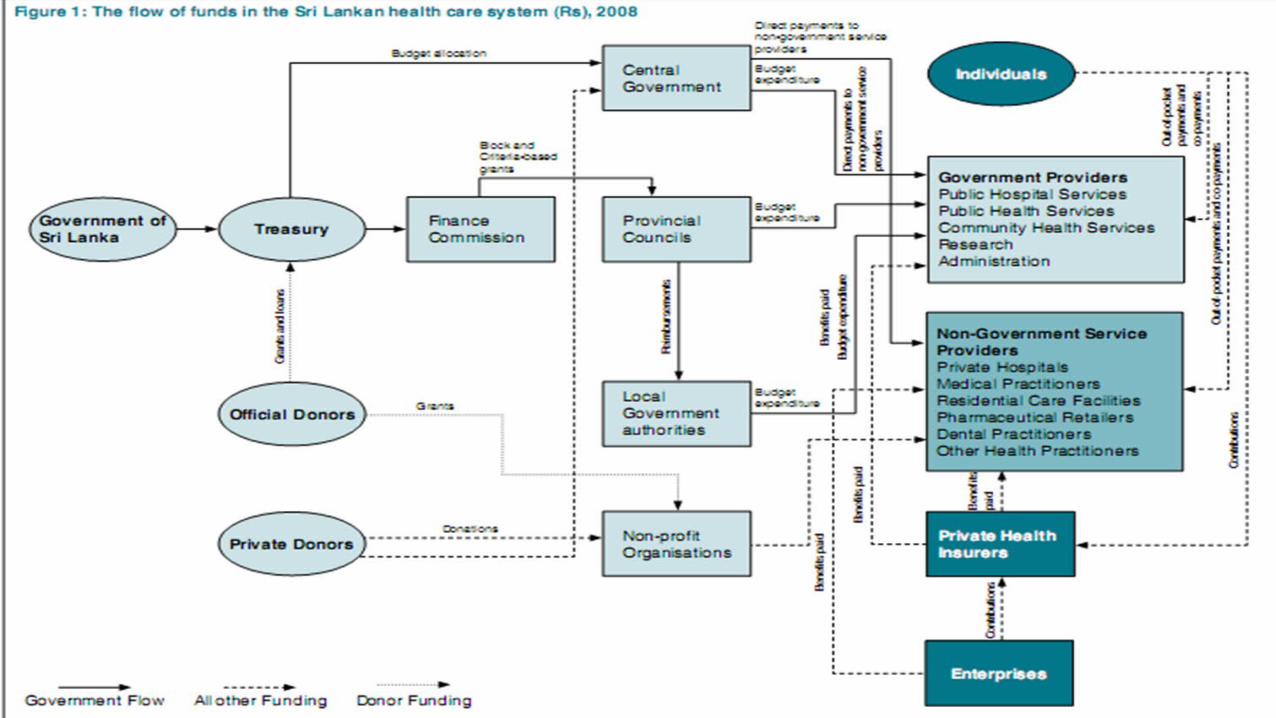
HEALTH EXPENDITURE
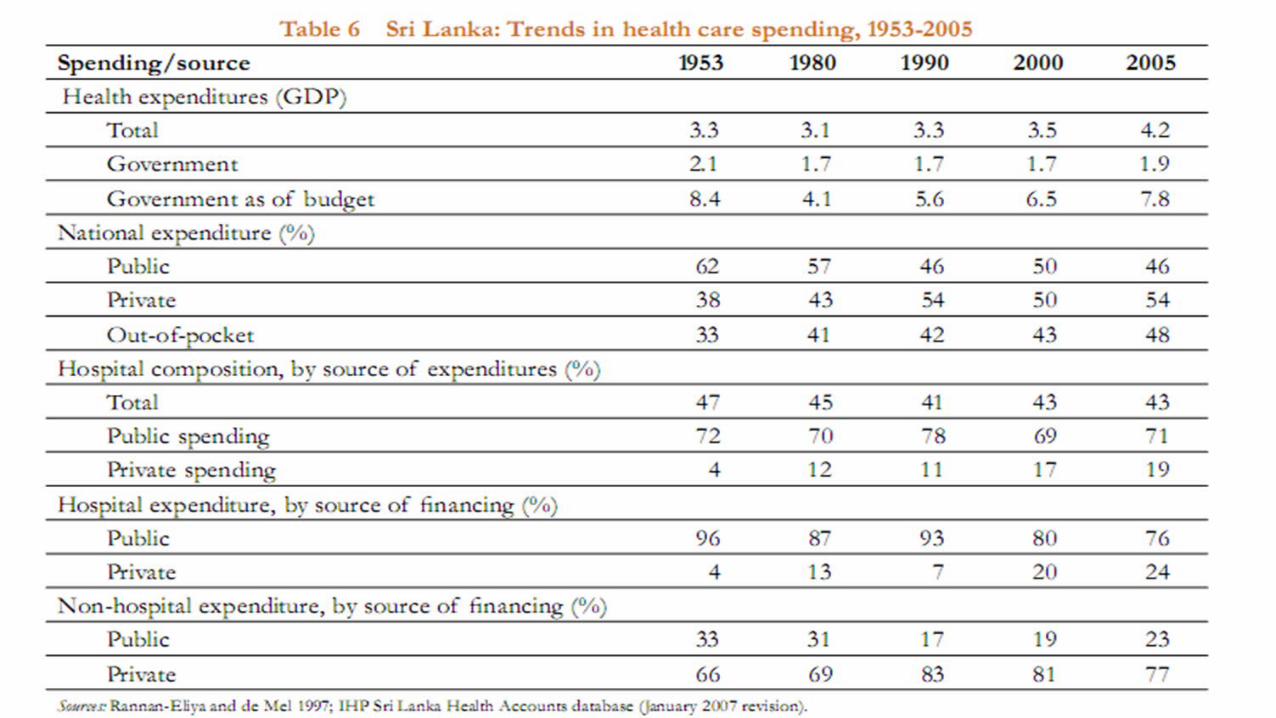
Total health expenditure, driven mostly by private spending, has increased since the early 1990s.
Contribution from the Government to the total health expenditure was 45.8% in 2009, while the contribution from the private sector was 54.2%
The government health expenditure as a percentage of total government expenditure was 4.9% in 2007, which is a decrease of over half from the 7.2% recorded in 2006. It is increasingly evident that private sector financing has become more prominent over time
Most private spending is for outpatient care and for purchasing medicines, but the share of hospital spending in private outlays has increased.(partly because of expanded delivery of outpatient services by private hospitals and partly because of the increased availability of private insurance.)
Health services account for 8 percent of government budgetary spending.
Private financing is mostly out-of-pocket spending by households, with smaller contributions from employers and insurance.
Spending by non-governmental organizations (NGOs) is small.
Government expenditures have concentrated on hospitals since the health reforms of the 1930s, directed primarily at increasing equity in access and improving risk protection.
Hospital spending accounted for about 70 percent of government recurrent spending in the 1950s, and the share has changed little since then .
until recently more than 85 percent of hospital spending was by government, while more than 80 percent of nonhospital and outpatient care spending was financed privately
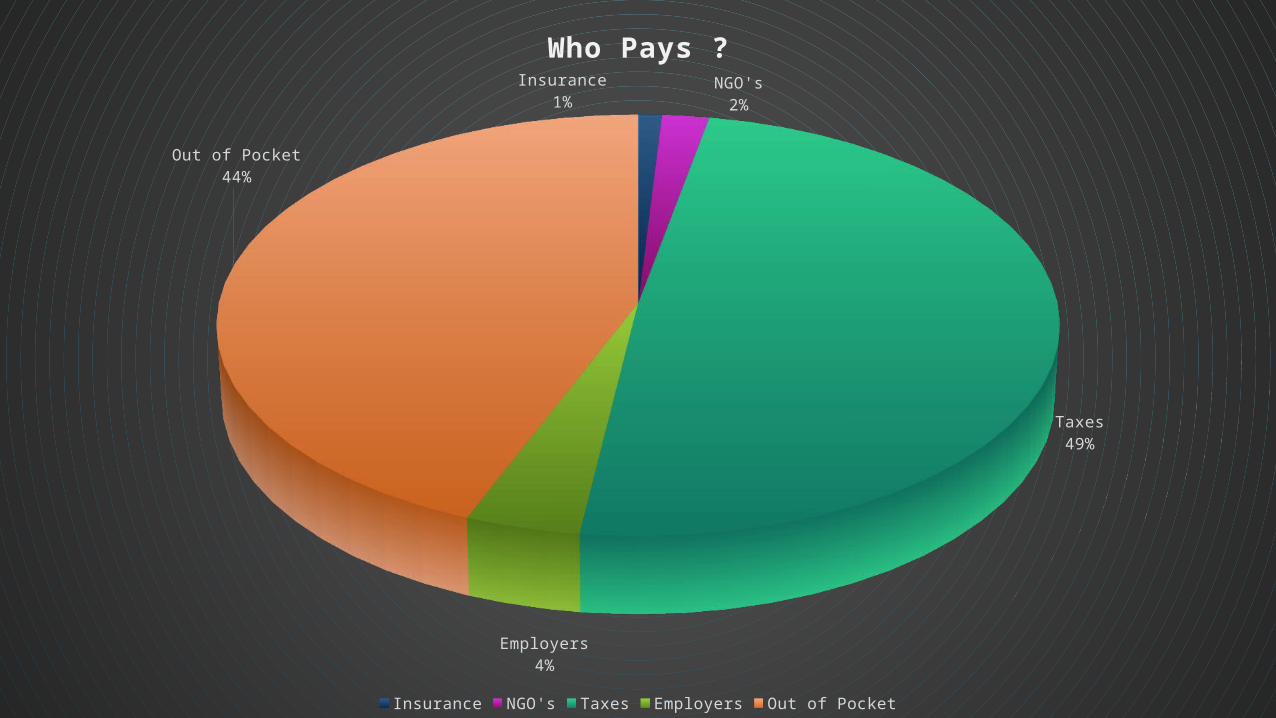
Insurance1%
NGO's2%
Taxes49%
Employers4%
Out of Pocket44%
Who Pays ?
Insurance NGO's Taxes Employers Out of Pocket
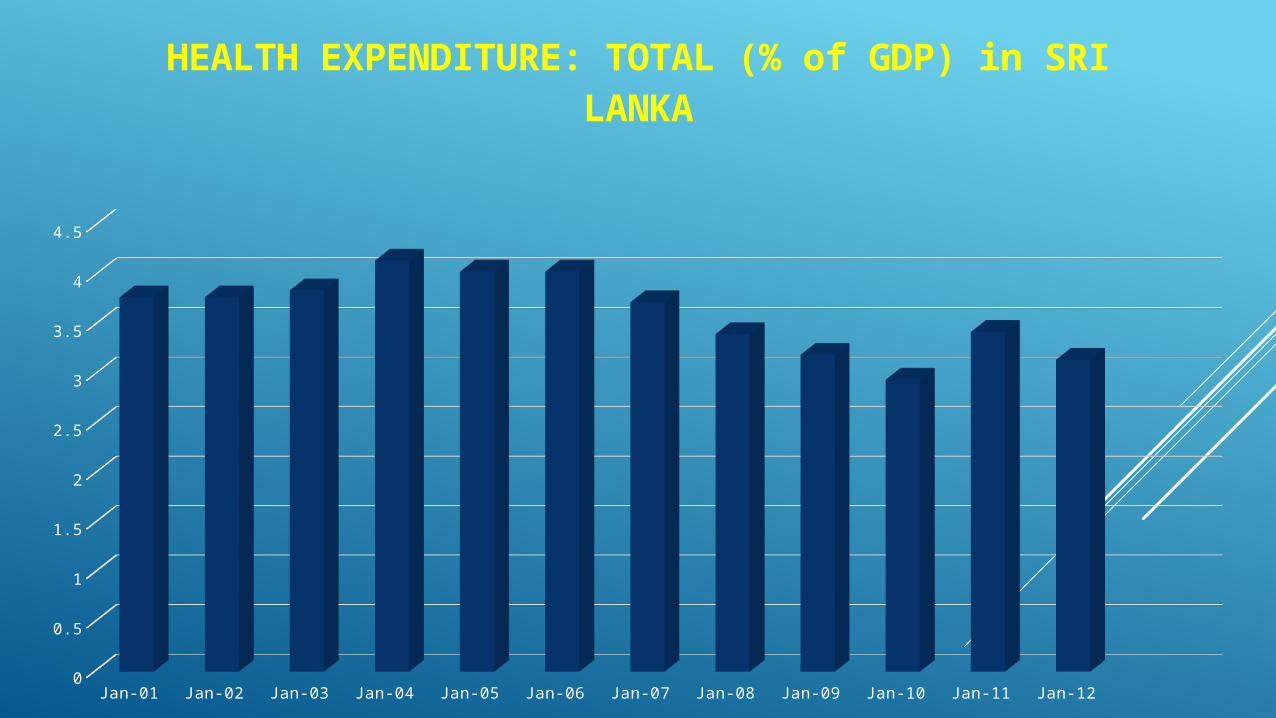
Jan-01 Jan-02 Jan-03 Jan-04 Jan-05 Jan-06 Jan-07 Jan-08 Jan-09 Jan-10 Jan-11 Jan-120
0.5
1
1.5
2
2.5
3
3.5
4
4.5
HEALTH EXPENDITURE: TOTAL (% of GDP) in SRI LANKA
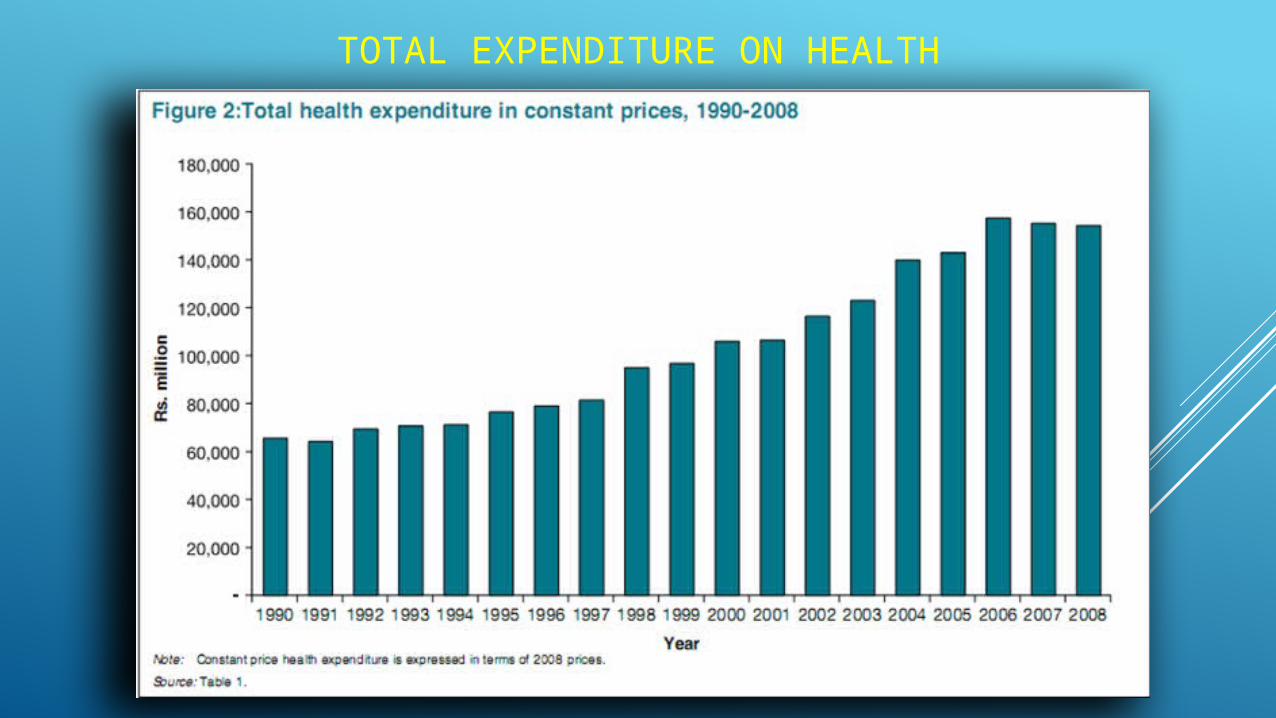
TOTAL EXPENDITURE ON HEALTH
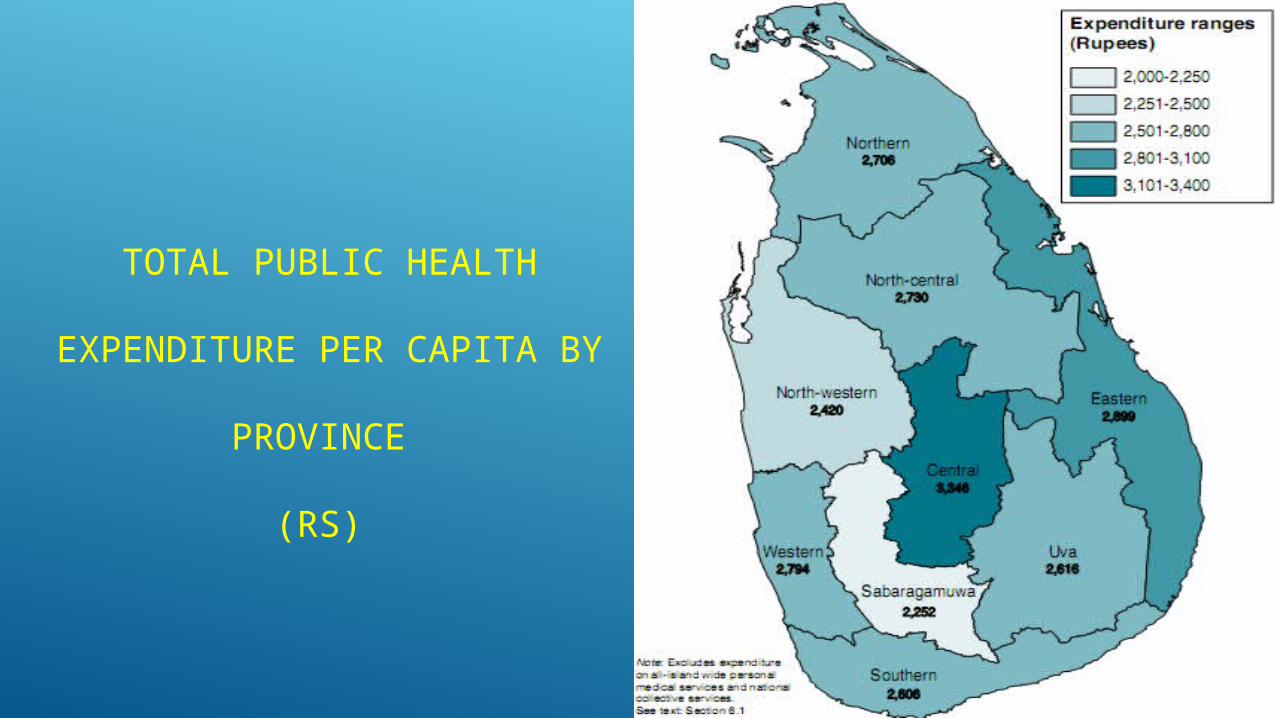
TOTAL PUBLIC HEALTH
EXPENDITURE PER CAPITA BY
PROVINCE
(RS)
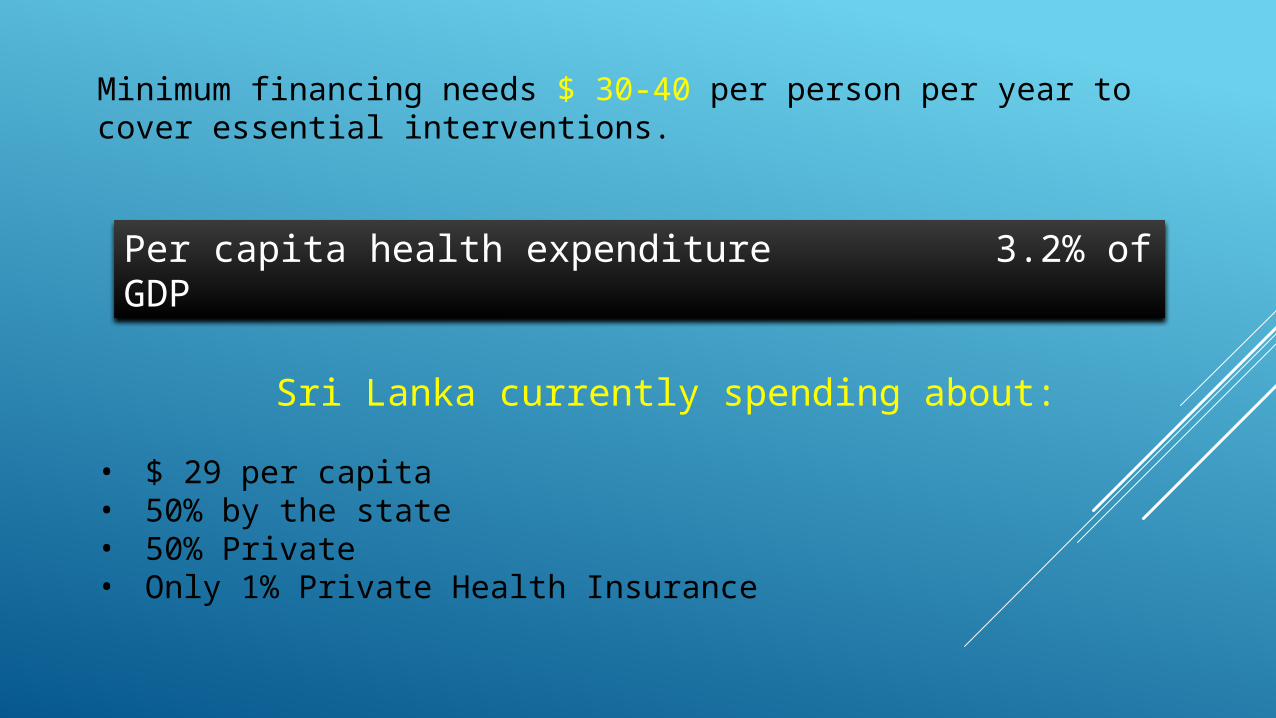
Minimum financing needs $ 30-40 per person per year to cover essential interventions.
Sri Lanka currently spending about:
• $ 29 per capita• 50% by the state • 50% Private• Only 1% Private Health Insurance
Per capita health expenditure 3.2% of GDP
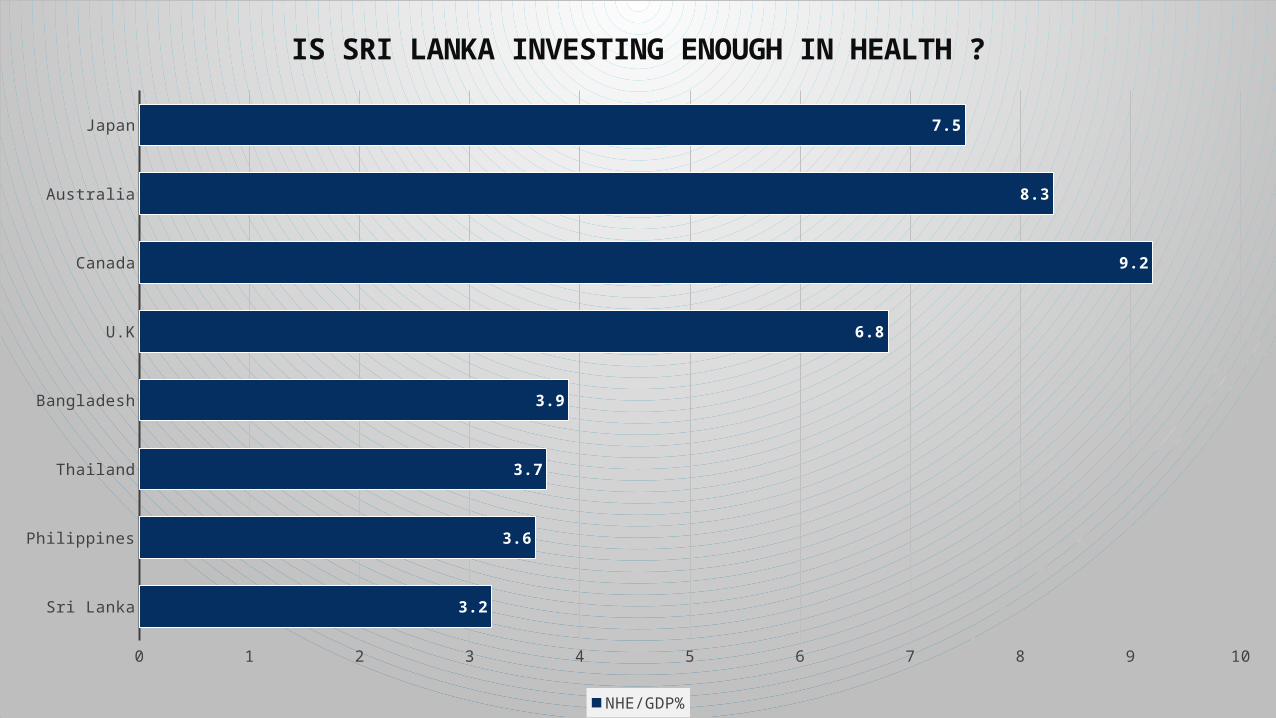
Sri Lanka
Philippines
Thailand
Bangladesh
U.K
Canada
Australia
Japan
0 1 2 3 4 5 6 7 8 9 10
3.2
3.6
3.7
3.9
6.8
9.2
8.3
7.5
IS SRI LANKA INVESTING ENOUGH IN HEALTH ?
NHE/GDP%
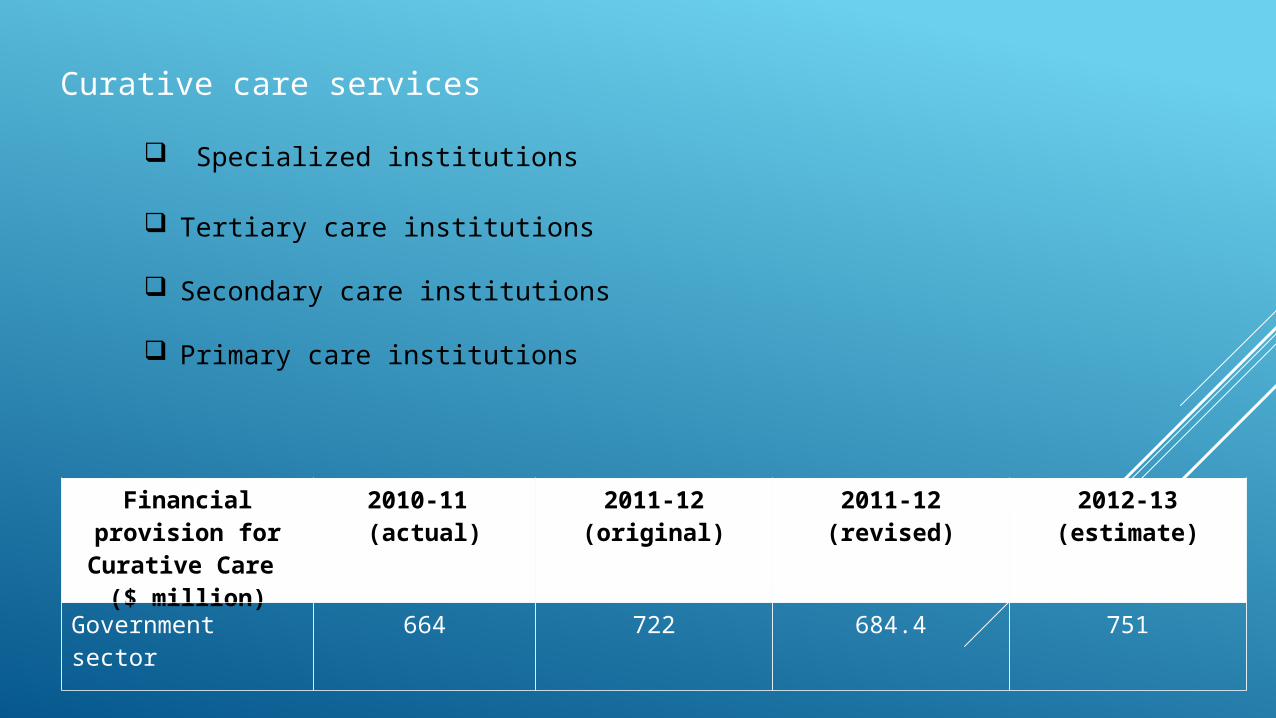
Curative care services
Specialized institutions
Tertiary care institutions
Secondary care institutions
Primary care institutions
Financial provision for
Curative Care ($ million)
2010-11 (actual)
2011-12(original)
2011-12(revised)
2012-13(estimate)
Government sector 664 722 684.4 751
One of the curative care aim is to provide specialized outpatient treatment for various illnesses.
BCG vaccinations
specialized outpatient clinics DTB and Chest
Dermatology
HIV/AIDS:
Specialized outpatient clinics provide curative services to patients with tuberculosis (TB) and chest diseases, skin diseases or human immunodeficiency virus (HIV) infection.
Dental treatment cases :
Dental service is provided to hospital patients, emergency cases and groups with special oral healthcare needs
key performance measures in respect of
curative care
PREVENTIVE HEALTH SERVICES
• Maternal and Child Health
• School Health
• Well-women services
• Family Planning
• Environment Health
• Occupational Health
• Prevention and control of communicable diseases
• Prevention and control of NCD
• Active ageing
• Mental Health well being
• Health Promotion
• Oral health care
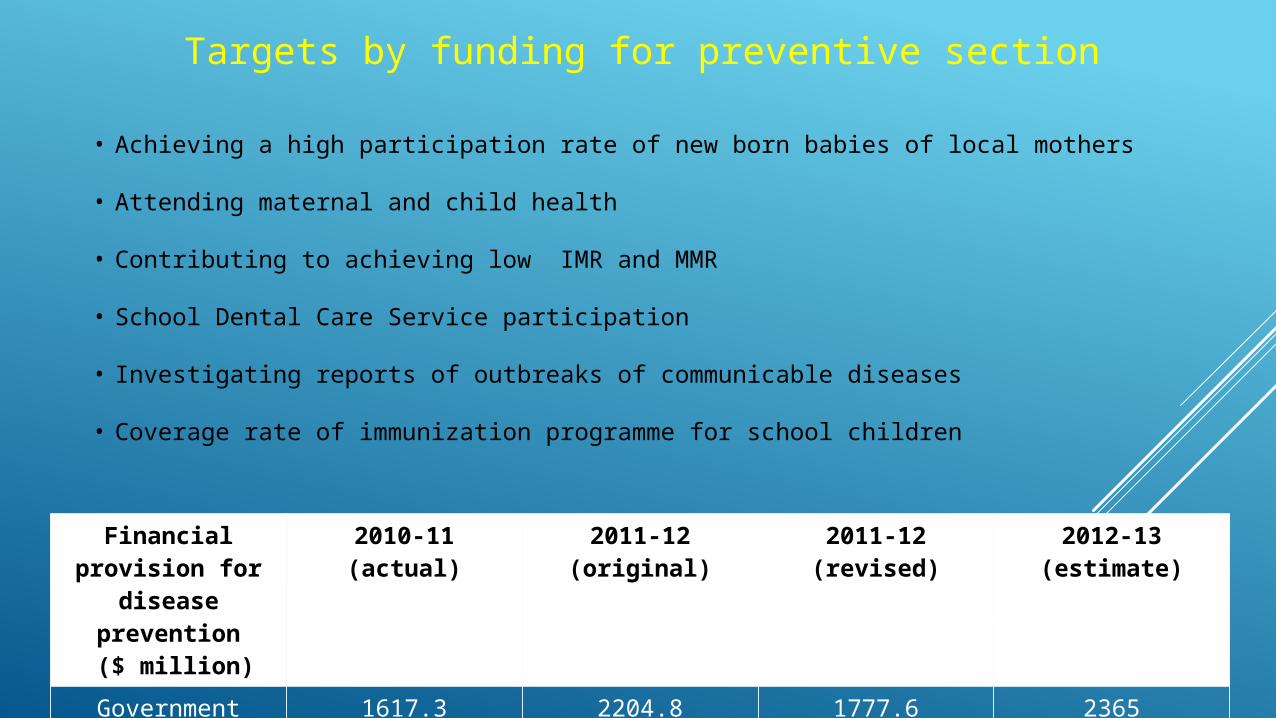
Financial provision for
disease prevention ($ million)
2010-11(actual)
2011-12(original)
2011-12(revised)
2012-13(estimate)
Government sector
1617.3 2204.8 1777.6 2365
Targets by funding for preventive section
• Achieving a high participation rate of new born babies of local mothers
• Attending maternal and child health
• Contributing to achieving low IMR and MMR
• School Dental Care Service participation
• Investigating reports of outbreaks of communicable diseases
• Coverage rate of immunization programme for school children
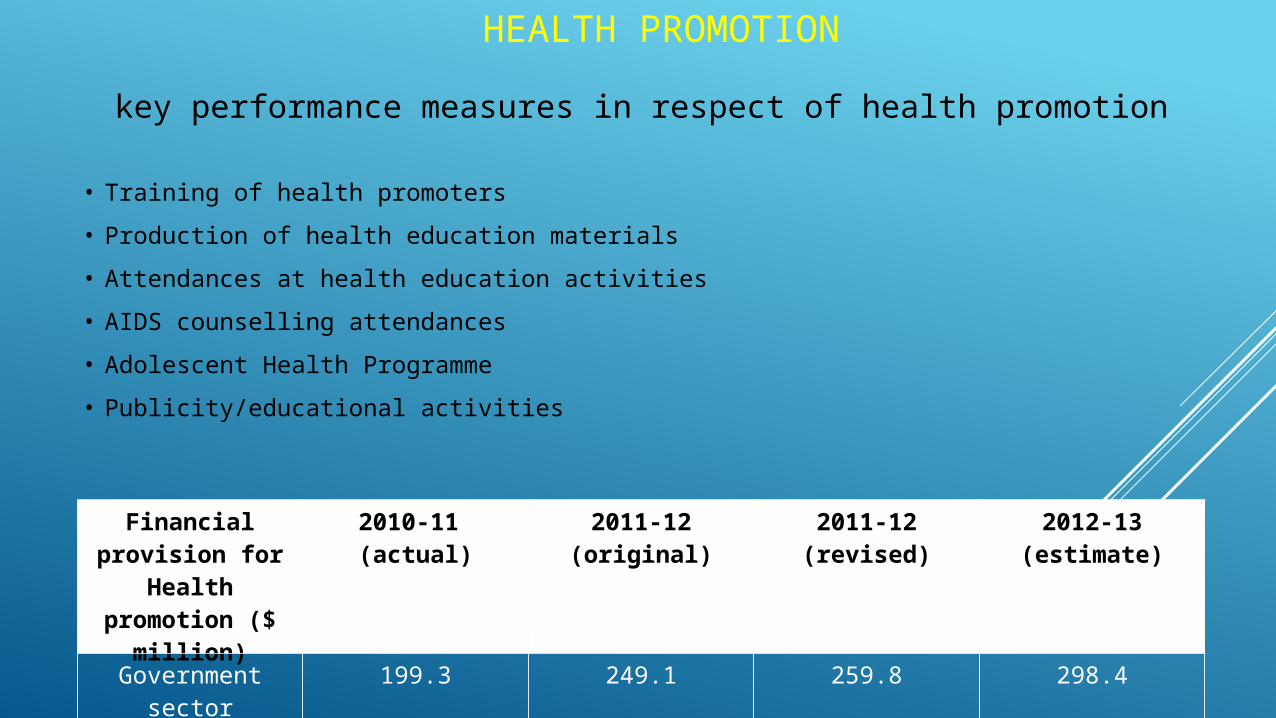
HEALTH PROMOTION
key performance measures in respect of health promotion
• Training of health promoters
• Production of health education materials
• Attendances at health education activities
• AIDS counselling attendances
• Adolescent Health Programme
• Publicity/educational activities
Financial provision for
Health promotion ($
million)
2010-11 (actual)
2011-12(original)
2011-12(revised)
2012-13(estimate)
Government sector
199.3 249.1 259.8 298.4
SPECIAL CAMPAIGNS
Respiratory Disease Control Unit
STD HIV/AIDS Control Program
Rabies Control activities
Malaria Control Program
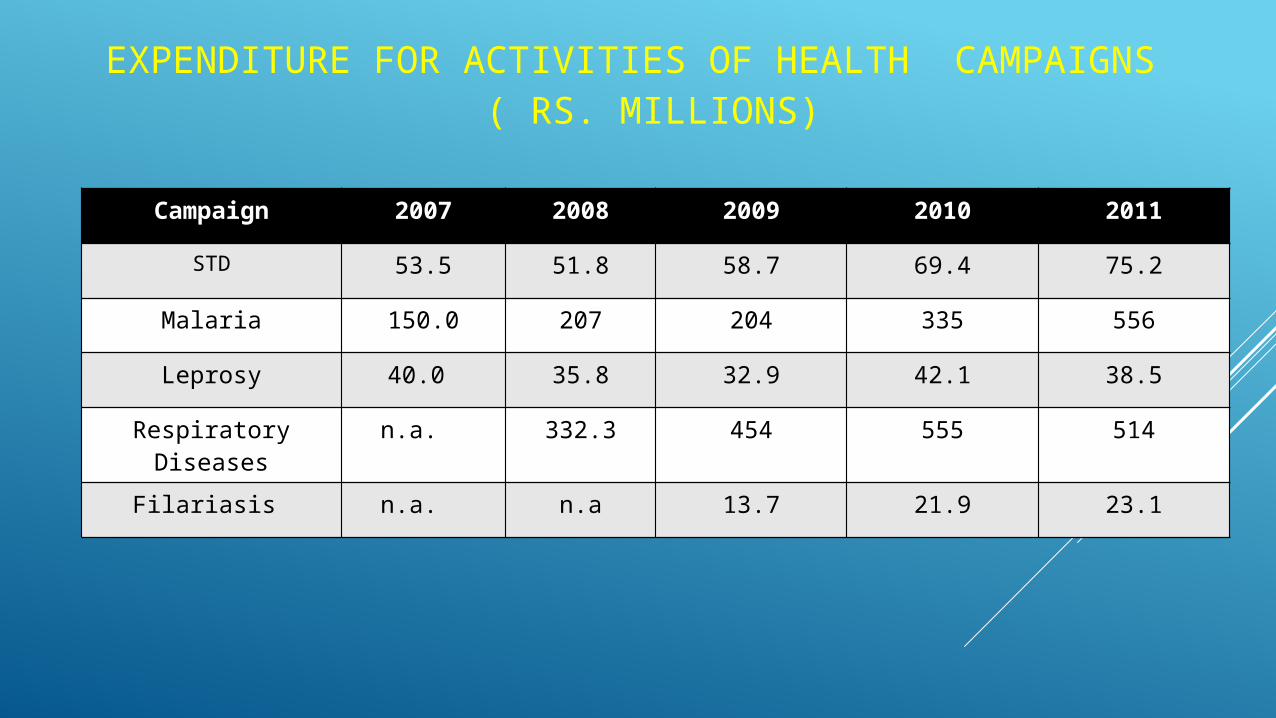
Campaign 2007 2008 2009 2010 2011
STD 53.5 51.8 58.7 69.4 75.2
Malaria 150.0 207 204 335 556
Leprosy 40.0 35.8 32.9 42.1 38.5
Respiratory Diseases
n.a. 332.3 454 555 514
Filariasis n.a. n.a 13.7 21.9 23.1
EXPENDITURE FOR ACTIVITIES OF HEALTH CAMPAIGNS ( RS. MILLIONS)
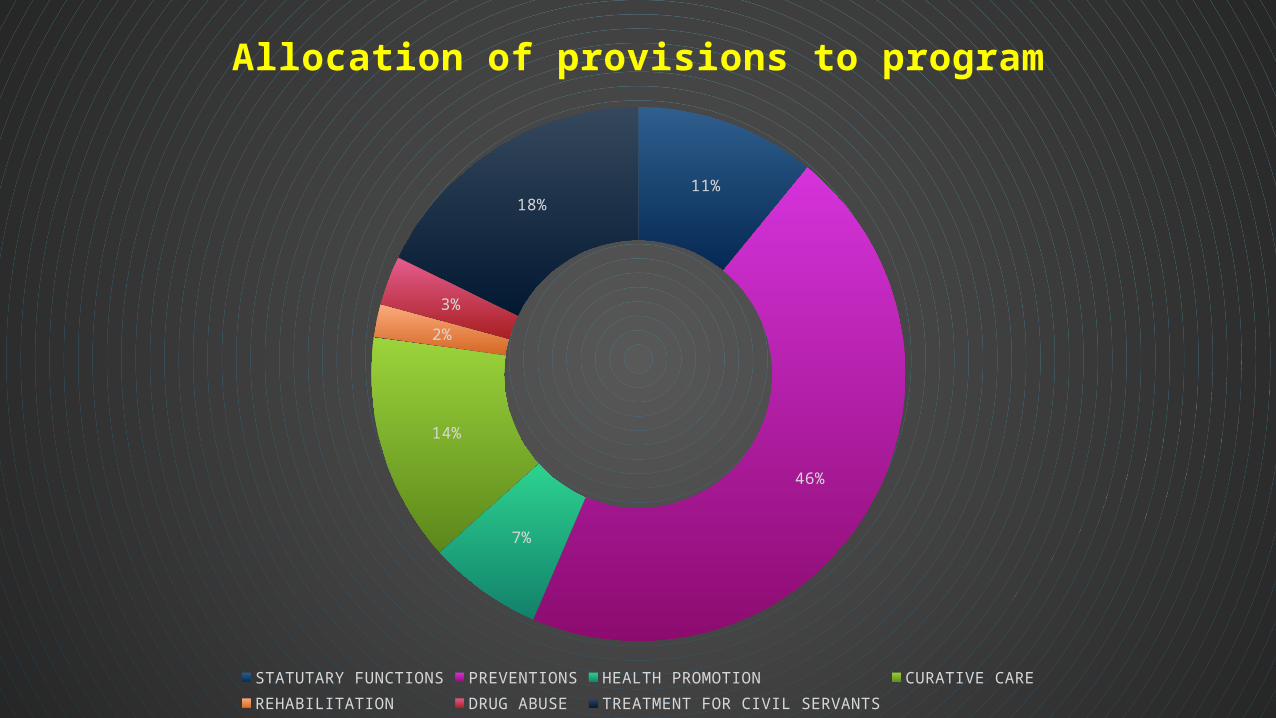
11%
46%
7%
14%
2%
3%
18%
Allocation of provisions to program
STATUTARY FUNCTIONS PREVENTIONS HEALTH PROMOTION CURATIVE CAREREHABILITATION DRUG ABUSE TREATMENT FOR CIVIL SERVANTS
Malnutrition
Rapid increase in non communicable diseases
Violence and injuries (intentional and unintentional)
Malaria, TB, dengue and filariasis
The above-mentioned problems are compounded for the poor population, with an estimated 25% of the population below the ‘national’ poverty line and 7% on less than one dollar/day.
PROBLEMS
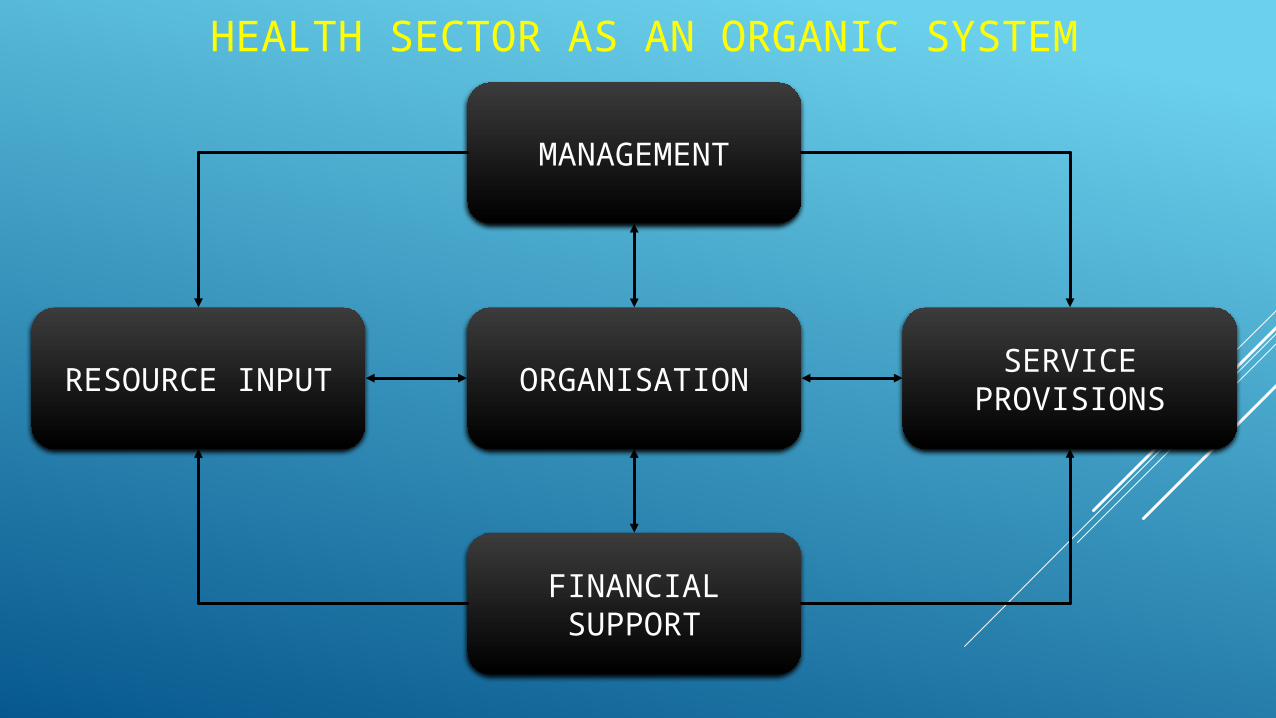
MANAGEMENT
ORGANISATION
FINANCIAL SUPPORT
RESOURCE INPUTSERVICE
PROVISIONS
HEALTH SECTOR AS AN ORGANIC SYSTEM
Ampara
Anuradhapura
Moneragala
Kurunegala
Badulla
Puttalam
Ratnapura
Matale
Galle
Kandy
Polonnaruwa
Mullaitivu
Mannar
Batticaloa
Kegalle
Vavuniya
Hambantota
Trincomalee
Kalutara
Matara
GampahaNuwara
Eliya
Kilinochchi
Jaffna
Colombo
53.2
26.9
30.1
19.0
53.7
32.9
30.6
38.0
26.3
23.6
21.3
45.8
25.3
95.1
13.3
17.7
30.9
38.5
57.1
33.8
35.5
2.2
113.1
23.5
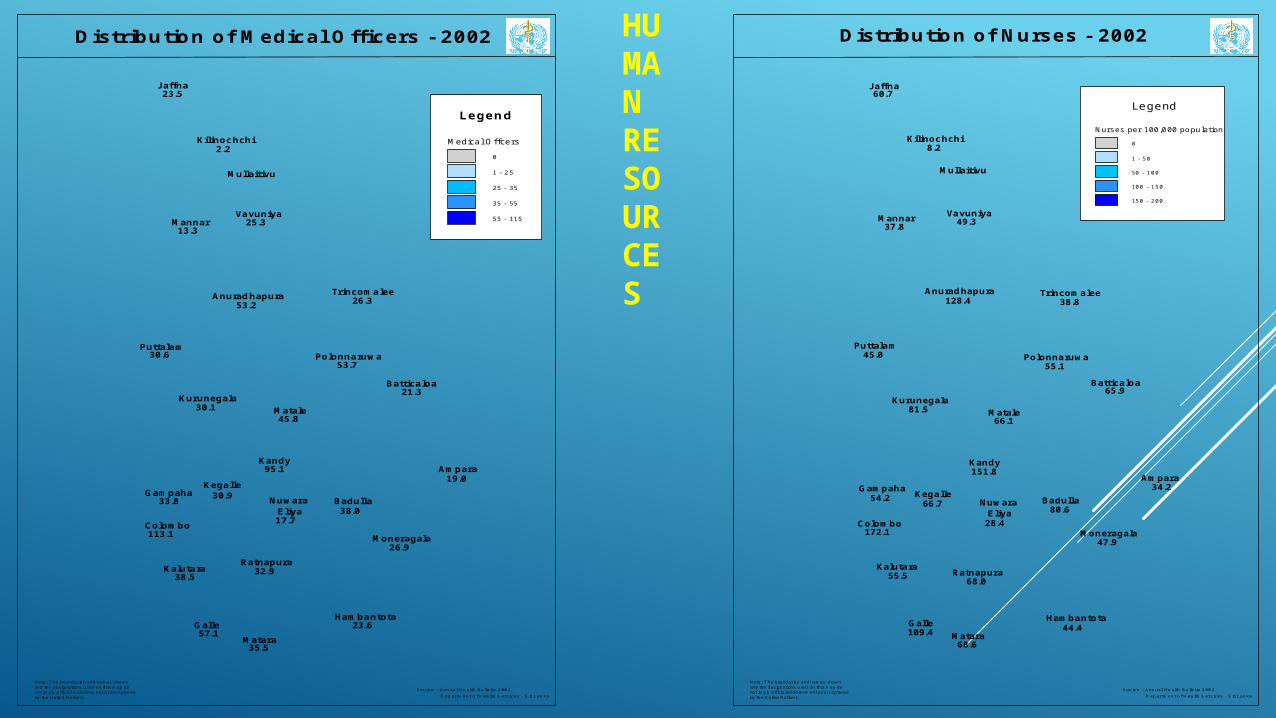
Medical Offcers
0
1 - 25
25 - 35
35 - 55
55 - 115
Legend
Distribution of Medical Officers - 2002
Note : The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptanceby the United Nations.
Source : Annual Health Bulletin 2002 Department of Health Services - Sri Lanka
Ampara
Anuradhapura
Moneragala
Kurunegala
Badulla
Puttalam
Ratnapura
Galle
Matale
Kandy
Mullaitivu
Polonnaruwa
Mannar
Batticaloa
Kegalle
Vavuniya
Hambantota
Trincomalee
Kalutara
Matara
Gampaha
Nuwara Eliya
Kilinochchi
Jaffna
Colombo
128.4
47.9
81.5
34.2
55.1
68.0
45.0
80.6
38.8
44.4
65.9
66.1
49.337.8
28.4
151.8
66.7
55.5
109.4
54.2
68.6
8.2
172.1
60.7
Distribution of Nurses - 2002
Nurses per 100,000 population
0
1 - 50
50 - 100
100 - 150
150 - 200
Legend
Source : Annual Health Bulletin 2002 Department of Health Services - Sri Lanka
Note : The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptanceby the United Nations.
HUMAN RESOURCES
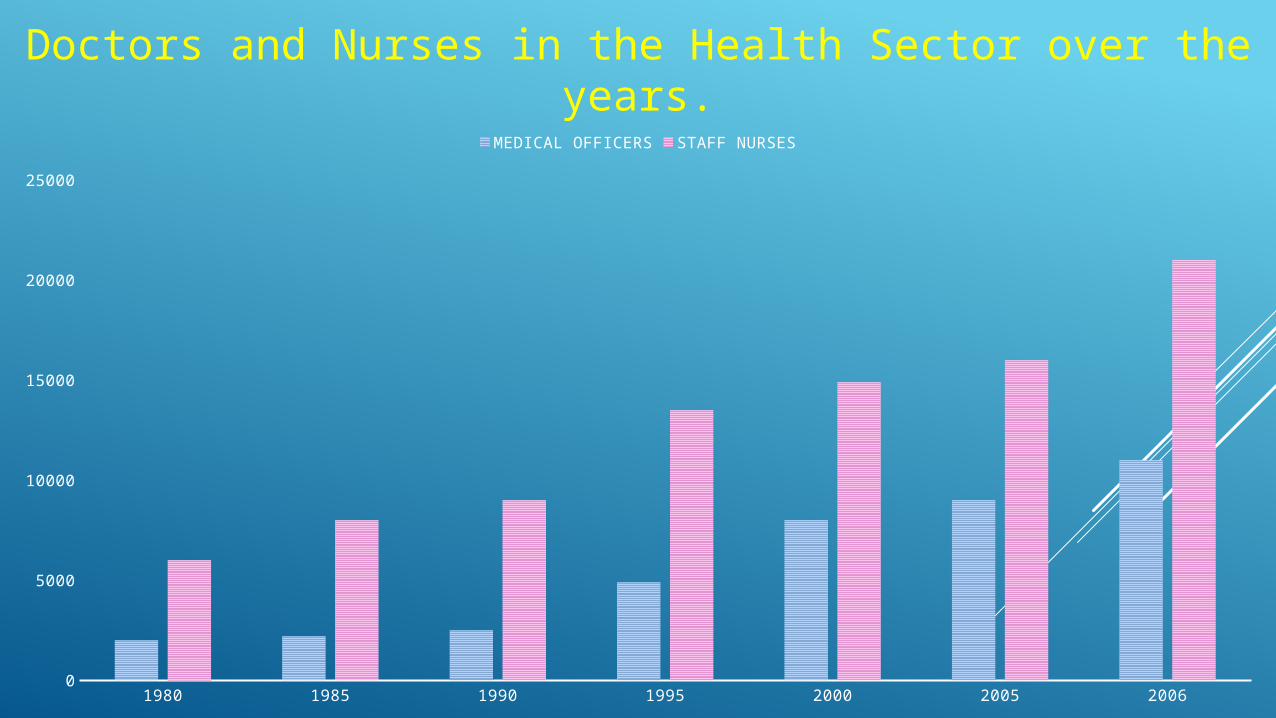
1980 1985 1990 1995 2000 2005 20060
5000
10000
15000
20000
25000
MEDICAL OFFICERS STAFF NURSES
Doctors and Nurses in the Health Sector over the years.
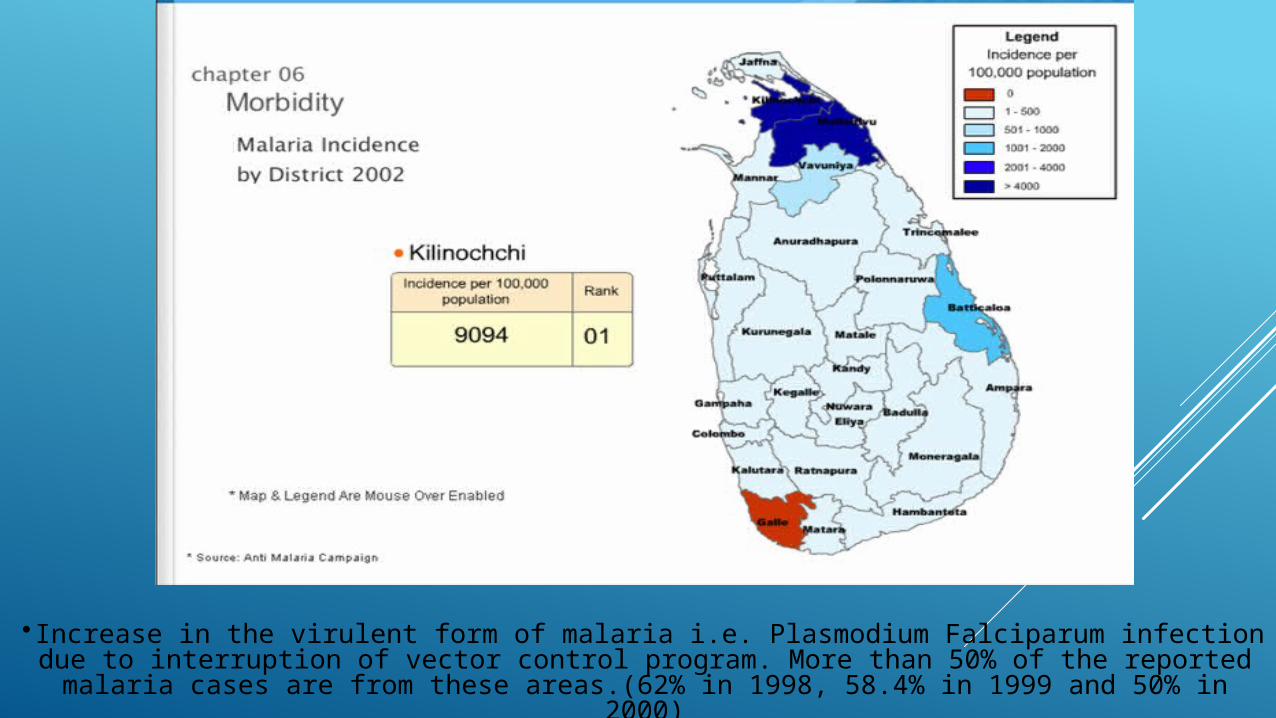
• Increase in the virulent form of malaria i.e. Plasmodium Falciparum infection due to interruption of vector control program. More than 50% of the reported malaria cases are
from these areas.(62% in 1998, 58.4% in 1999 and 50% in 2000)
Mental Health and Psychosocial wellbeing – Often taking the low priority
A mental health needs assessment concentrating on those living in the ‘welfare centres’ who had been suffering from the combined effects of trauma and poverty in the District of Vavuniya had shown : -
High numbers of attempted suicides, alcohol abuse, domestic violence, grief, suspicion and a sense of ‘learnt helplessness’,
A breakdown in normal social support networks,
Appalling living conditions and lack of services,
Total absence of psychosocial support services,
97% had lost their homes and property,
87% had constant feeling of insecurity 63% had suicidal thoughts,
66% had bad memories of displacement, death of a family member, witnessing people being burnt alive in their homes etc.
INCIDENCE OF CANCER
Jaffna district has the highest incidence of cancer in Sri Lanka
Incidence of cancer among the males in Jaffna district is double that of the average for Sri Lanka
Analysis by ethnic groups the incidence is
Tamils 108 per 100,000 population
Sinhalese 91 per 100,000 population
Muslims 57 per 100,000 population
[Ref: Panabokke R G. (1984) The Geographical Pathology of Malignant tumors in Sri Lanka. Ceylon Medical Journal. 2:4;211-15.]
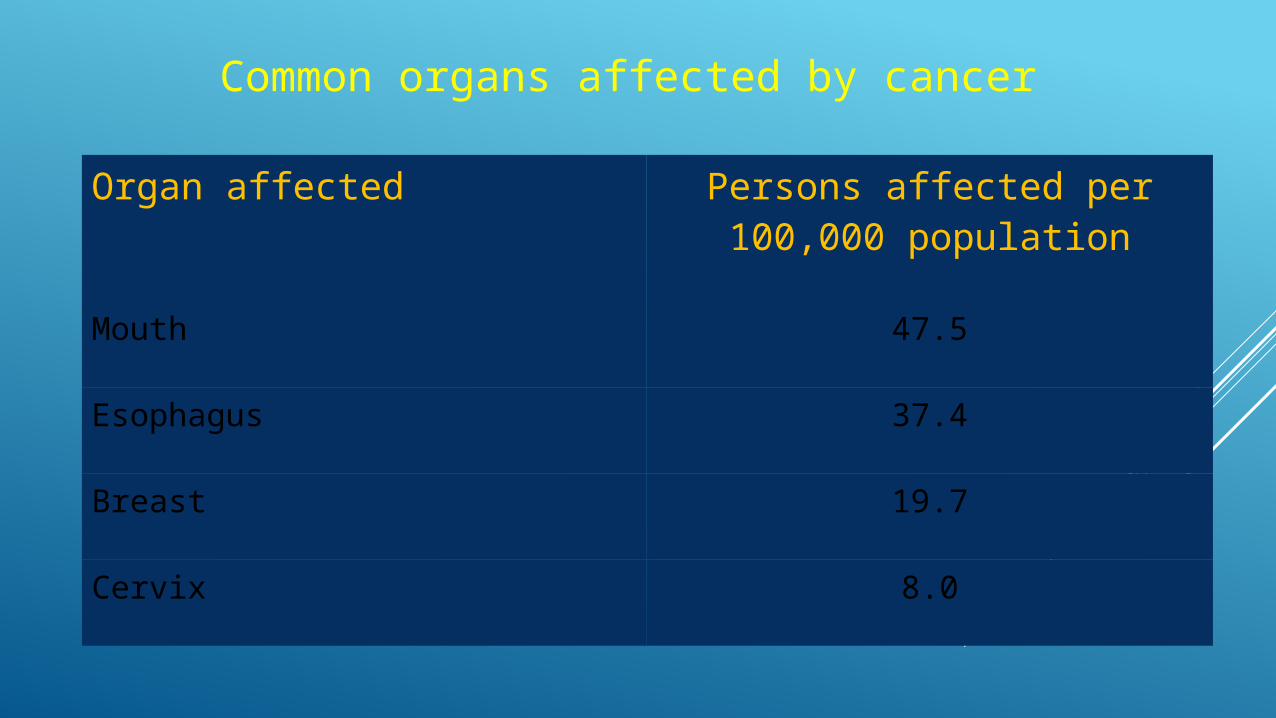
Organ affected Persons affected per 100,000 population
Mouth 47.5
Esophagus 37.4
Breast 19.7
Cervix 8.0
Common organs affected by cancer
PLANNING ISSUES & CHALLENGES
Required Policy Framework and Guiding Principles
1: Responding to Epidemiology (Service and System)
In order to meet the epidemiological changes, reorientation of the health care services and their delivery system is a must. This can be derived from the following three principles:
• Principle 1: Prioritisation and Characterisation of Disease (Communicable/Non Communicable)
• Principle 2: Exploration and Development of New Strategy
• Principle 3: Linking and Integrating Services and Systems
2: Responding to Patient’s Expectation (Culture and Care)
Not only through the global awakening of patient’s right and equity, but also by looking at the characteristics of the disease itself, patient participation and satisfaction bears greater importance in the success of treatment. Greater efforts are needed in educating patients as well as health service providers to make better choices. This calls for reorientation of people’s cultural norm on the health care in association with the following principles:
• Principle 1: Improvement of “Quality and Safety”
• Principle 2: Securing of “Patient Right”
• Principle 3: Enhancement of “Client Satisfaction”
3: Responding to Efficacy of the System (Mission and Management)
Reorientation of the health sector organisation, management and information systems is required to respond to efficacy of the system. In the changing situation, it must reframe the entire management system to:
• Principle 1: Be Accountable
• Principle 2: Be Flexible
• Principle 3: Be Efficient
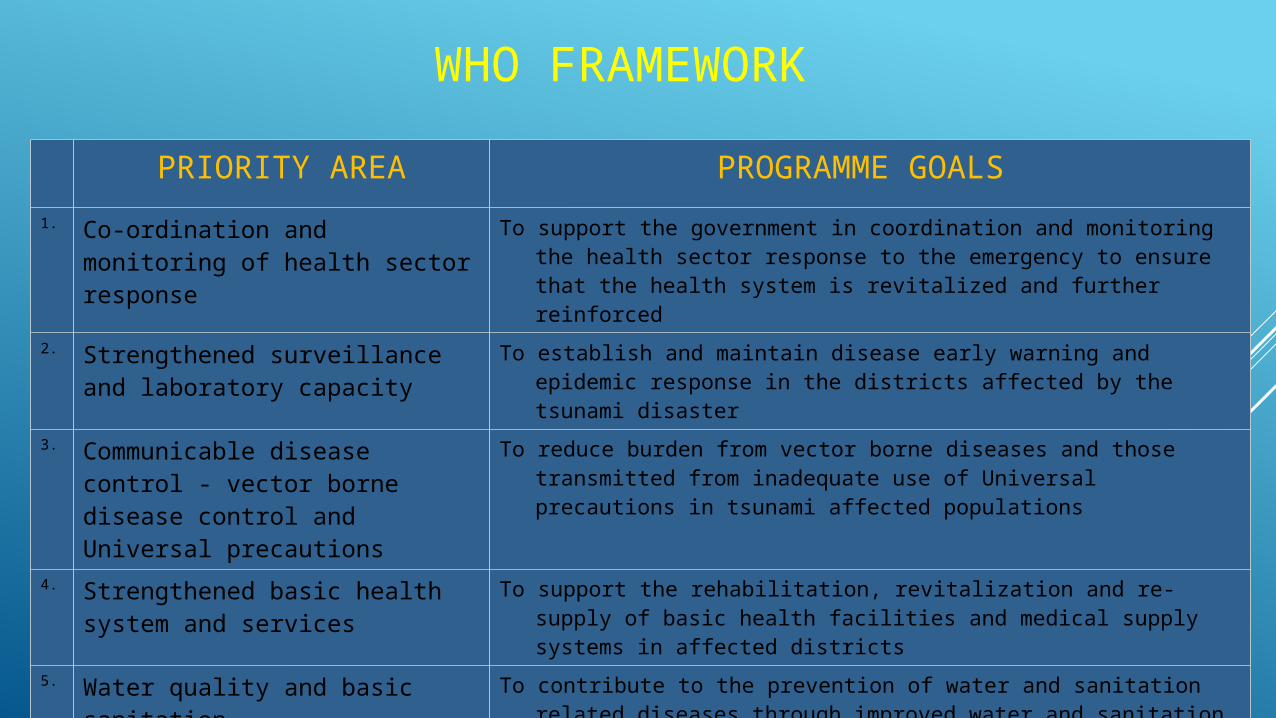
WHO FRAMEWORK
PRIORITY AREA PROGRAMME GOALS
1. Co-ordination and monitoring of health sector response
To support the government in coordination and monitoring the health sector response to the emergency to ensure that the health system is revitalized and further reinforced
2. Strengthened surveillance and laboratory capacity
To establish and maintain disease early warning and epidemic response in the districts affected by the tsunami disaster
3. Communicable disease control - vector borne disease control and Universal precautions
To reduce burden from vector borne diseases and those transmitted from inadequate use of Universal precautions in tsunami affected populations
4. Strengthened basic health system and services
To support the rehabilitation, revitalization and re-supply of basic health facilities and medical supply systems in affected districts
5. Water quality and basic sanitation To contribute to the prevention of water and sanitation related diseases through improved water and sanitation services and their effective use
6. Psychosocial and mental health support
To provide immediate psychosocial mental health assistance to the population affected by the tsunami and to strengthen the mental health system

Sri Lanka Health Accounts, National Health Expenditure,1990-2008
Annual health bulletin 2007
Progress Review, Ministry of Healthcare & Nutrition
Sri Lanka: “Good Practice“ in Expanding Health Care Coverage by Ravi P. Rannan-Eliya & Lankani Sikurajapathy
http://www.tradingeconomics.com/sri-lanka/
Health System Assessment in North and East of Sri Lanka, WHO, Sri Lanka 2012
Annual Health Bulletin 1999, 2000
statistical Health book NEP 2000, DHS survey 2001
www.google.com
WHO.SriLanka
THANK YOU