Embed Size (px)
Citation preview

SUBMUCOUS LIGATIONOF
FISTULA TRACT (SLOFT)
Dr D.U.PathakMS FACRSI
Jabalpur (M.P) India

Development of Ano -Rectum

Development of Anus
• Hind gut fuses with proctodeum below to make anal canal
• Both carry different Blood , Lymphatic and nerve supply
• The mucosa above is columnar and becomes gradually stratified below• Two different cultures
meet each other

SURGICAL ANATOMY OF ANO RECTUM
• Anatomical anal canal is 2cms – Anal valves to anal verge
• Surgical anal canal is 4 cms Anal ring to anal verge

Surgical & Anatomical anal canal
• Surgical anal canal extends from Ano rectal ring to anal verge. It is 4 cms.
• Anatomical anal canal is only 2 cms from dentate line to anal verge.

Surgical anatomy of Ano-rectum

Ano rectal ring
• The deep fibres of external sphincteres and pubo rectalis sling form the upper end of Ano rectal margin and the ring

Dentate (Pectinate) line
• It is the junction of upper 2/3rds and lower one third of anal canal
• Fusion of hindgut and proctodeum
• Hence Endoderm above and Ectoderm below

Dentate line
• Blood supply is from superior rectal above and middle and inferior rectal below
• Nerve supply above is inferior hypogastric plexus conducting stretch and
• Inferior rectal nerves carrying pain to cut and burn through pudendal.
• Lymphatics below drain to inguinal and above to pararectal

Hilton’s line
• First landmark above the anal verge.
• More felt than seen – inter-sphincteric groove
• It is muco cutaneous junction
• Below is Keratinized stratified squamous epithelium
• Below it the lymphatic drainage is to inguinal nodes.

Pectin
• A small strip of 1 cm below the Dentate line and is called Pectin
• It is a transitional zone with cuboidal epithelium and no skin appendages
• Here the mucosa is very adherent to the surroundings hence abscesses are very painful
• Ischio rectal abscesses usually drain below this area• Below this the skin gradually thickens and
appendages develop near the verge

Anal verge
• Below the Hilton’s line• Distal collapsed rugous end of the anal canal • Surrounded by superficial anal sphincter• Transitional area of epithelium of the anal
canal and perianal skin

Sphincters
Internal• Pearly white condensed
circular smooth muscle fibres
• Extend from ano rectal junction all along the anal canal.
• Thickest - 3-5 mms at the verge
• Lower level than external• Autonomous nerve supply
External• Skeletal voluntary red
muscles, supplied by somatic nerve supply
• Divisions have no clinical significance, all merged

Surface landmarks

Anal glands
• Lie in the inter sphincteric and sub mucous planes
• Two to ten in number• Secrete lubricating
material in anus• Internal opening is in the
crypts at dentate line• Highly susceptible for
infection

Anal gland

Ano-rectal diseases

Crypto glandular infection
• The infection usually starts in the crypts• Common organisms are Staphylococci,
Streptococci, E coli or Proteus• Recently also anaerobes like Clostridium
Welchii and bacteroids• Sometimes mixed with tubercular

Sites of abscess

Spread of sepsis

Ano Rectal Fistula
• It is sequel of crypto glandular abscess• The infection is of anal gland• Anal glands are 6-8 in number• Their function is to lubricate the anal canal• All open at the dentate line

Location of Internal opening

Basic understanding
• The internal opening is always at the dentate line.
• High opening is usually Iatrogenic, other uncommon causes are tuberculosis and malignancy, rarely Crohns
• The usual pyogenic abscess can never perforate a normal rectal wall and create a high opening

Formation of fistula
• A crypto glandular abscess with inadequate drainage from the internal opening spreads in loose inter sphincteric planes and ultimately finds its way somewhere to drain out, making an external opening.
• The collections develop a protective wall around them, which becomes more firm, shrinks in size, takes a tubular shape to make a so called fistula tract.

Investigations
• To diagnose• To assess• To rule out• To know the synchronous problems• To follow up the progress of recovery

The best investigation remains …

If you don’t want to put your foot in rectum …

Fistulography

Conventional USG
• Readily available• Gives information about
the maturity of tract• Of more help when
combined with other imaging like fistulography
• Detects the hidden abscesses

Endo SonologyTrans sphincteric

Endo Sono - Horseshoe

MRI
• CT could not give proper information about the soft tissues
• It helps in 90% cases to localize the internal opening
• Helps in mapping , planning and projecting the prognosis.
• Worth in recurrent fistulae

Chest X Ray

Classification
• Vertical • Parks Simple, Inter
sphincteric and trans sphincteric.

Goodsal’s Rule

Extensions

Why do we classify an disease??
• To plan the treatment.• When the treatment is same you do not
bother for classification like – hernia.

Existing procedures
• Aim towards separate treatment for different types.
• The approach is from distal – external opening to proximal – internal opening
• Hence the knowledge of anatomy of the tract was compulsory

The Aim of treatment
• Control of sepsis
• Prevention of incontinence and recurrence
• Giving him less pain, morbidity and job loss

Existing methods
• Lay open • Seton• Kshar sutra• Cut and repair of the sphincter after excision
of the tract.• Fistula plug• VAAFT• LIFT

Lay open
• Big painful wound with long term recovery
• Makes the patient incontinent at least for flatus.
• Gives a bad scar and furrow.

Seton
• Painful long term cutting of the sphincter with pressure

Ksharsutra- Ayurvedic thread
• Chemical cutting with a formulation of fixed ph
• It is long term painful cutting with gradual healing at the same time
• Leaves behind a bad scar

Excision of the tract and
Primary repair of sphincter
• Needs high expertise• Associated with high incidence of
incontinence.

Fistula plug
• Very attractive choice for affluent class
• The zero morbidity way but associated with high recurrence rate

VAAFT
• It’s a high tech costly operation

LIFT
• Sound surgical principle • Low morbidity • No incontinence But• Difficult to learn, to do and to teach

Sub mucous Ligation Of Fistula Tract(SLOFT)
• Basic principle is of LIFT- ligation of the tract • In SLOFT -• It is more proximal• It is more superficial• Leaves behind a smaller stump of the proximal
tract

Submucosal Ligation Of Fistula Tract (SLOFT)
• The approach is anti grade – from internal opening to going distal – that too only for 2 cms.
• The tract as it emerges from internal opening is always straight and superficial
• As is goes distally it changes it’s course like a river• The distal coarse is unpredictable as regards its
curvatures and depth hence existing methods are not so easy and effective for elimination of the tract.

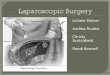
Schematic representation of SLOFT
Internal opening
Tract hooked
Dentate line

Instruments

Probing
• Probe is gently introduced to come out from internal opening
• Then it is bent and pulled out of the Anus.
Incision

Injection Xylocaine adrenaline
• This blanches the area and does hydro dissection around the tract
Muco- Cutaneous
Junction

Hooking the tract
• Incision is at the muco cutaneous junction
• The tract is hooked
• Here it is superficial.

Site of ligation
• It is Sub mucous and is medial to the internal sphincter

FAQ – How far from Internal opening?

Division of the Tract
Anus
Anus
Hooked tract
Tract transacted

Distal tract
• Cored out and sent for HPR .
Coring of external
tract
EAL near internal opening

Wound
• Can be Primarily closed

Fistula at 4-O clock

Fistula at 2-O clock

Multiple tracts – method is the same
Opening at 6-O clock
Opening at 2-O clock
Opening at 2-O clock
passing gas from scrotum
All the three tracts EAL done separately

Cored after SLOFT
All three external tracts
removed by coring
Healed in 20 days

Immediate post op picture
This patient had two tracts with one para rectal blind extension.

Post operative period
• Discharge in a day
• No post discharge dressings

Post op first morning can sit without pain

They are happy

Case -1- 091797-60854 Multiple tracts
• 45 yrs male came with recurrence after two operations in 2 ½ yrs.
• He came with • 1. impending rupture of
perianal abscess at 4-O clock
• 2.External opening at 2-O clock and
• 3. External opening at the base of scrotum from where he was passing flatus

Internal opening at 2-O clock
• Probe coming out of opening from 2-O clock
• SLOFT done

SLOFT
• SLOFT at 2-O clock

Internal opening at 4-O clock
• SLOFT at 4-O clock

Probe from scrotal opening
• Probe from scrotal opening

Internal opening 2-O clock
• SLOFT 2-O clock

Coring
• Coring done after confirmation of the ligation
• Wounds left open to heal

Healed in 20 days
• Patient did not come for follow up
• He had to be called on request and the wounds were seen to be healed in 20 days

Post op 3 weeks
• He had to be called for documentation because as such he had no problem

Case -2 - 097132-50531
• The post op picture• SLOFT hidden in the
anal verge• Pt did not come for
follow up as the wound healed and he had no problem
• Mr Kamlesh Jharia c/o Dr R.P.Gupta 097132-50531

Case-2-Inter sphincteric fistula-per op
• Per operative photo after SLOFT
• Hydrogen peroxide seen leaking through the peri-anal space

Case -3- 089323-09290Recurrent fistula
• 50 yrs/M controlled DM, came with recurrence of fistula .
• SLOFT done and distal abscess cavity marsupilised

Insertion of probe

Ligation

SLOFT

Abscess marsupilised

Post op 20 days-healing

Almost healed

Post op 2 monthssudden perianal abscess

Seton tied – superficial fistula

Abscess and rupture

Seton cut after 15 days under LA

Case-4- 078285-13112

Healed in 25 days

Post op 40 days - recurrence

Spontaneous rupture of abscess

Spontaneous healing

Case-5-093031-62144

Incision over probe

Indwelling probe

Tract hooked

Ligated and transacted

Probe in distal tract

Distal tract excised

Painless P/R next morning

Next morning

Post op 10th day

Healed

Post op visit

Case-6- 098273-71437Acute abscess fistula complex



• In spite of the acute and fragile tract, SLOFT could be done as the probe was indwelling and ano-rectum could be kept virgin

Healed within few days with intact anus

Case-8Internal opening not demonstrable

Had to core, shorten the tract and gently
negotiate with the probe to come inside the internal opening.



Follow up on request ( 094251-52818)

First put in cradle by Dr Radhakrishna Patta


First workshop at Mujaffarnagar

ReproducedDr Naveen Agrawal – 097603 36161

Recurrences ??
• Time only will tell the percentage but• They are bound to occur
Recurrence bothers the patient if
the procedure was either costly or the recovery was painful.


Seriously looking forward for long term resultsధన్య�వాదాలు�