Embed Size (px)
Citation preview
Improving Access to Seven Day Services Event
NHS England Greater Manchester
& Lancashire Region
Wednesday, 25th June 2015, 09:30 – 2.30pm
Lion of Vienna Suite, Macron Stadium, Bolton
NHS Improving Quality and NHS England

Chair’s Welcome and Introduction
Dr Raj Patel, Medical Director NHSE Greater Manchester &
Lancashire
NHS Improving Quality and NHS England
7 Day Services across
Greater Man & Lanc
Dr Raj Patel,
Regional Medical
Director (Greater
Manchester &
Lancashire
NHSE – Our Business Plan
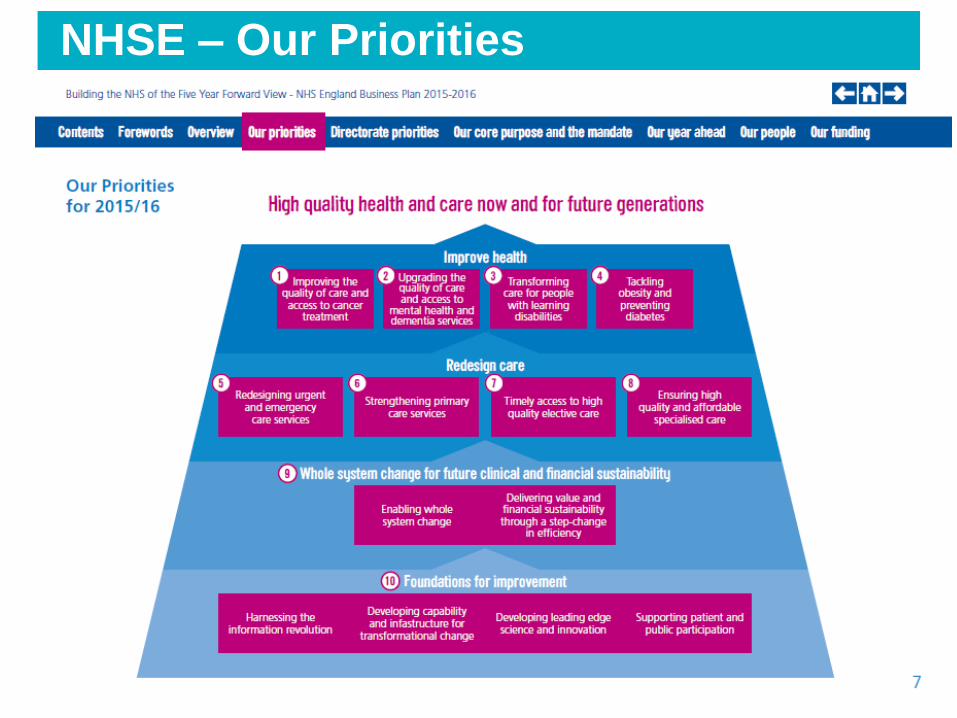
NHSE – Our Priorities
NHS | Presentation to [XXXX Company] | [Type Date] 5
NHS | Presentation to [XXXX Company] | [Type Date] 6
“ At the end of last year, the research company Dr Foster found mortality rates rose by 10%
at weekends. Other studies have shown similar correlations.
” BBC News, Health
Five day service model not meeting
patient needs or expectations.
7
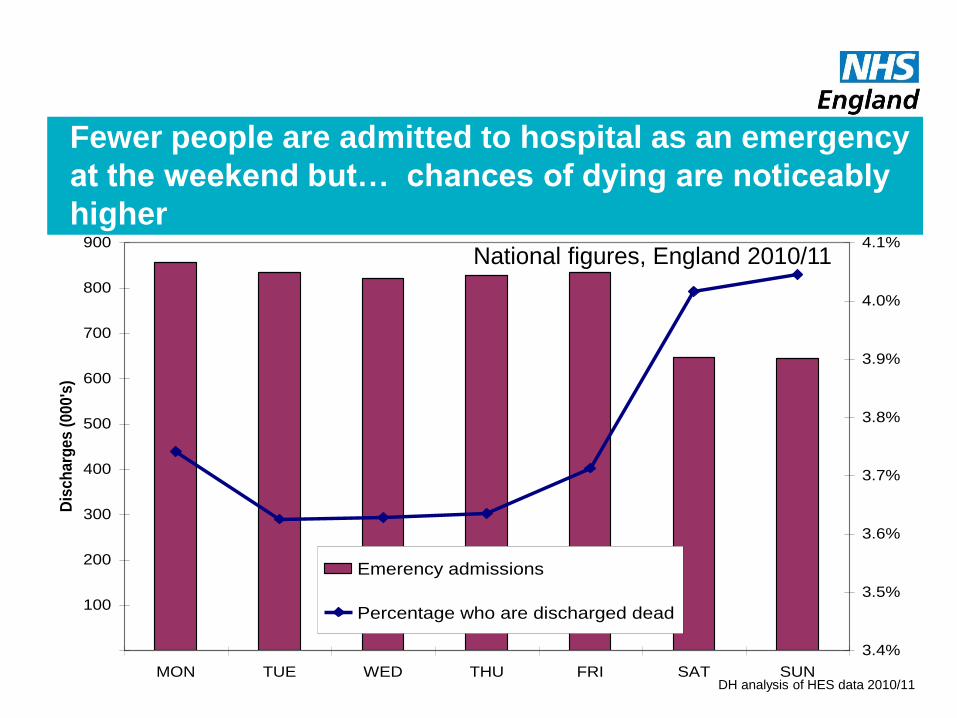
Fewer people are admitted to hospital as an emergency
at the weekend but… chances of dying are noticeably
higher
100
200
300
400
500
600
700
800
900
MON TUE WED THU FRI SAT SUN
Dis
ch
arg
es
(0
00
's)
3.4%
3.5%
3.6%
3.7%
3.8%
3.9%
4.0%
4.1%
Emerency admissions
Percentage who are discharged dead
DH analysis of HES data 2010/11
National figures, England 2010/11
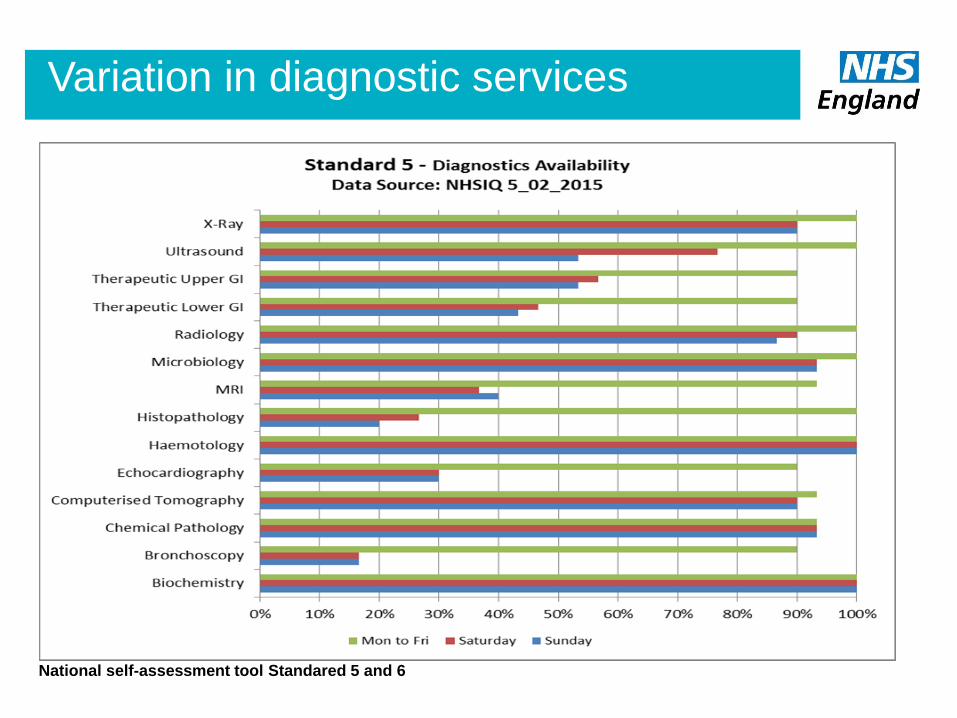
Variation in diagnostic services
National self-assessment tool Standared 5 and 6
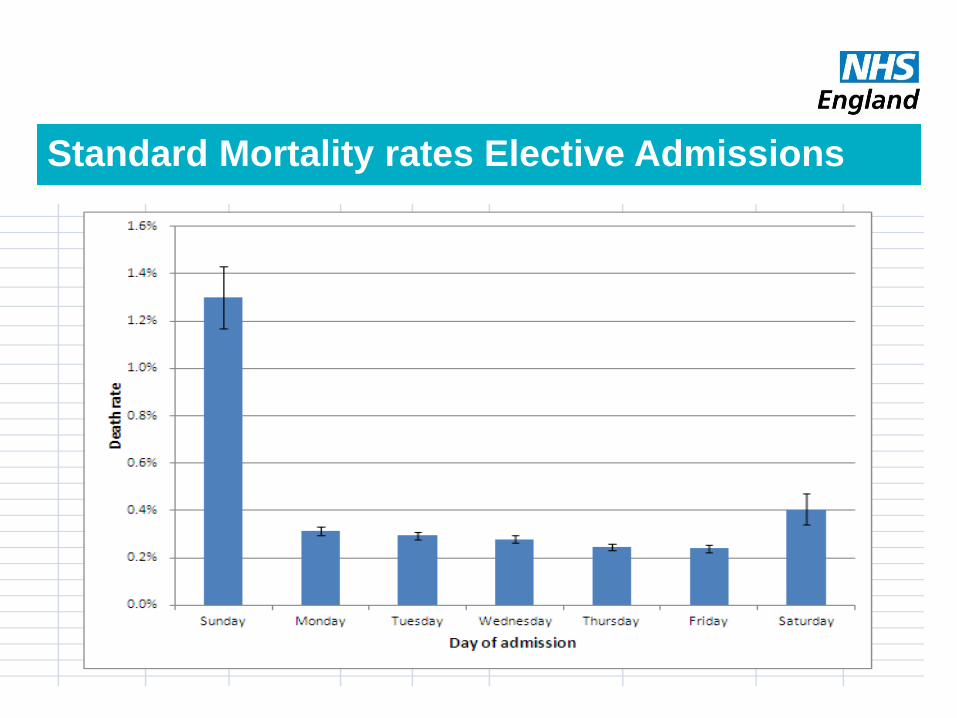
Standard Mortality rates Elective Admissions
“The NHS will move towards
routine services being available
seven days a week. This is
essential to offer a much more
patient-focused service and also
offers
the opportunity to improve
clinical outcomes”
Ten Clinical Standards describing
minimum standards of care patients
should expect to receive seven days a
week.
“This change will
be difficult - but it
is the right thing
to do.”
Sir Bruce Keogh,
National Medical Director NHS England
Time for Change
12

7Day Services –
The 10 Clinical Standards
Patient
Experience
Time to first
consultant
review
MDT
Review
Shift
Handovers
Transfer to
community
and Primary
and social
care
Mental
Health
Quality
Improvement Diagnostics
On-going
review
Intervention
/Key services
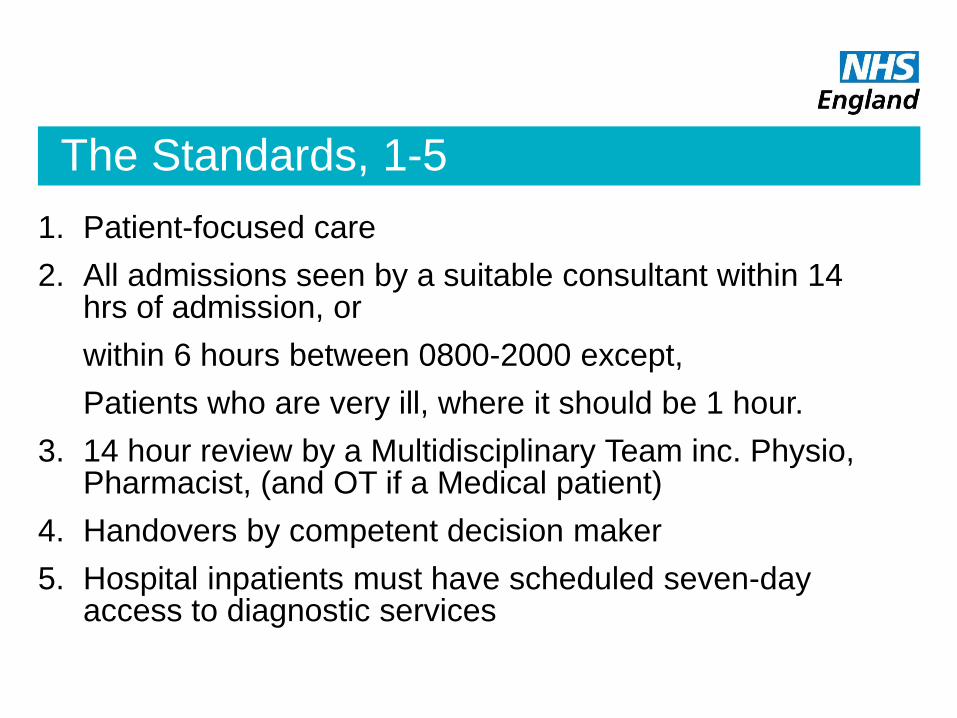
The Standards, 1-5
1. Patient-focused care
2. All admissions seen by a suitable consultant within 14 hrs of admission, or
within 6 hours between 0800-2000 except,
Patients who are very ill, where it should be 1 hour.
3. 14 hour review by a Multidisciplinary Team inc. Physio, Pharmacist, (and OT if a Medical patient)
4. Handovers by competent decision maker
5. Hospital inpatients must have scheduled seven-day access to diagnostic services
The Standards, 6-8
6. Hospital inpatients must have timely 24 hour access, seven days a week, to consultant-directed interventions
7. Where a mental health need is identified following an acute admission the patient must be assessed by psychiatric liaison within the appropriate timescales, 24 hours a day, seven days a week:
1 hour- Emergency, 14 hours Urgent
8. Once transferred from the acute area of the hospital to a general ward patients should be reviewed during a consultant-delivered ward round at least once every 24 hours, seven days a week, unless “not necessary”
The Standards, 9-10
9. Support services, both in the hospital and in primary, community and mental health settings must be available seven days a week
10. All those involved in the delivery of acute care must participate in the review of patient outcomes to drive care quality improvement. The duties, working hours and supervision of trainees in all healthcare professions must be consistent with the delivery of high-quality, safe patient care, seven days a week.
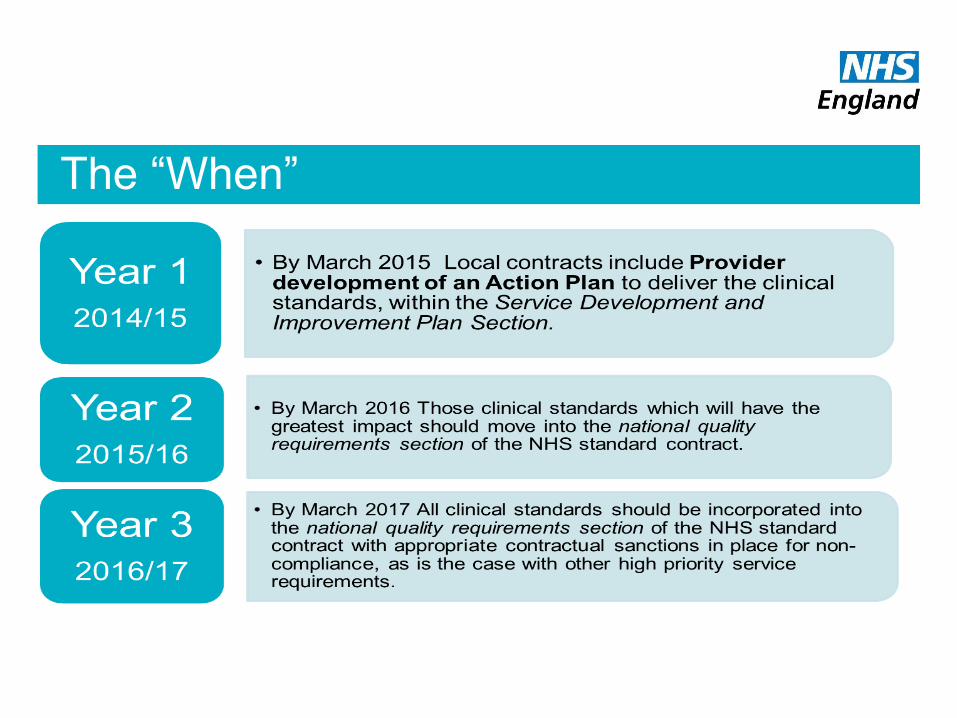
The “When”

Working together to support seven day
services
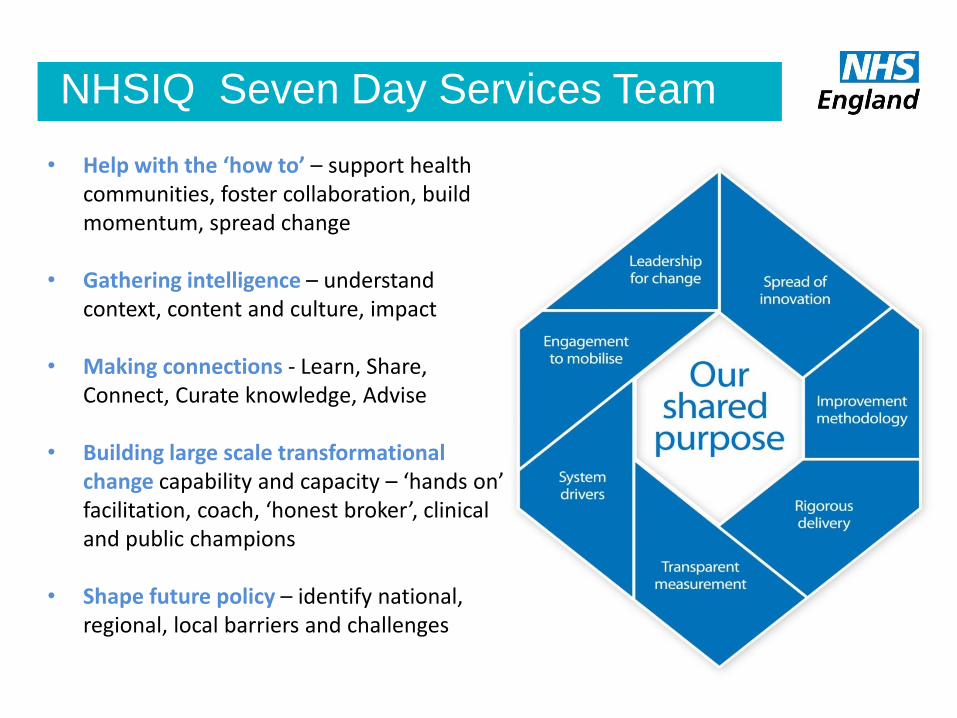
NHSIQ Seven Day Services Team
• Help with the ‘how to’ – support health communities, foster collaboration, build momentum, spread change
• Gathering intelligence – understand context, content and culture, impact
• Making connections - Learn, Share, Connect, Curate knowledge, Advise
• Building large scale transformational change capability and capacity – ‘hands on’ facilitation, coach, ‘honest broker’, clinical and public champions
• Shape future policy – identify national, regional, local barriers and challenges
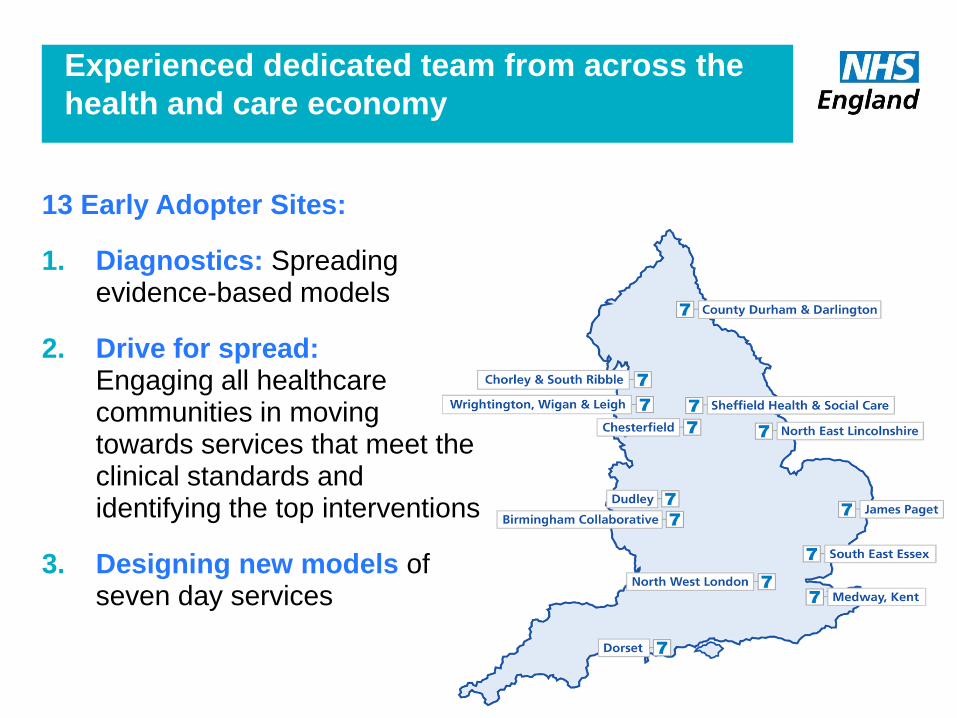
Experienced dedicated team from across the
health and care economy
13 Early Adopter Sites:
1. Diagnostics: Spreading evidence-based models
2. Drive for spread: Engaging all healthcare communities in moving towards services that meet the clinical standards and identifying the top interventions
3. Designing new models of seven day services
Have you completed your 7DS self-assessment?
• On-line self-assessment tool to measure progress
• Enables you to baseline your current level of service provision as a local health community
• Find out how your are progressing towards meeting the clinical standards and service provision
• Recent Updates:
Review your progress and benchmark yourself against others and create reports
To access the Seven Day Self Assessment tool, register http://www.7daysat.nhs.uk/
7 Day Self Assessment Tool (7DSAT)
Online Self-Assessment Tool
Multiple Users
Easy to Register
Baseline current service provision
Covers Local Health Economy (LHE) provision
Brings data together
Links to useful information
sources
FAQs
Access Support
Measure progress of services &
Clinical Standards
New tools:
Benchmark yourself against others
http://www.7daysat.nhs.uk/
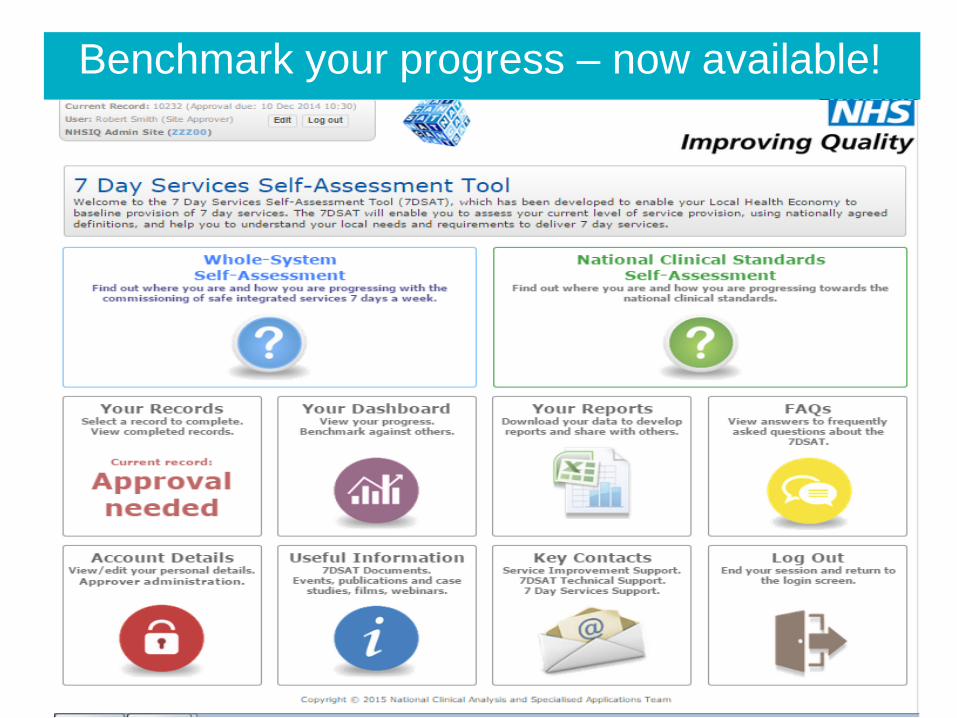
Benchmark your progress – now available!
7 Day Services SAT & Digest Survey
• Opportunity to have an introduction to this today:
• rolling presentation on screen and laptops for hands-on experience
• Primary Research – interviews and online survey – we need your input – to be launched in June
• Let us know if you would like to take part.
• Speak to your 7 Day Services Facilitator on your tables today!
NHS | Presentation to [XXXX Company] | [Type Date] 24
The weekend effect! - Easy Metric
Interactive Session – Key Pad Voting
Where we are now with the Challenge of 7 Day Services implementation …
NHS Improving Quality and NHS England
You will need your keypad to respond to questions in this session
When prompted press the key of your choice
A green light will flash to confirm your choice
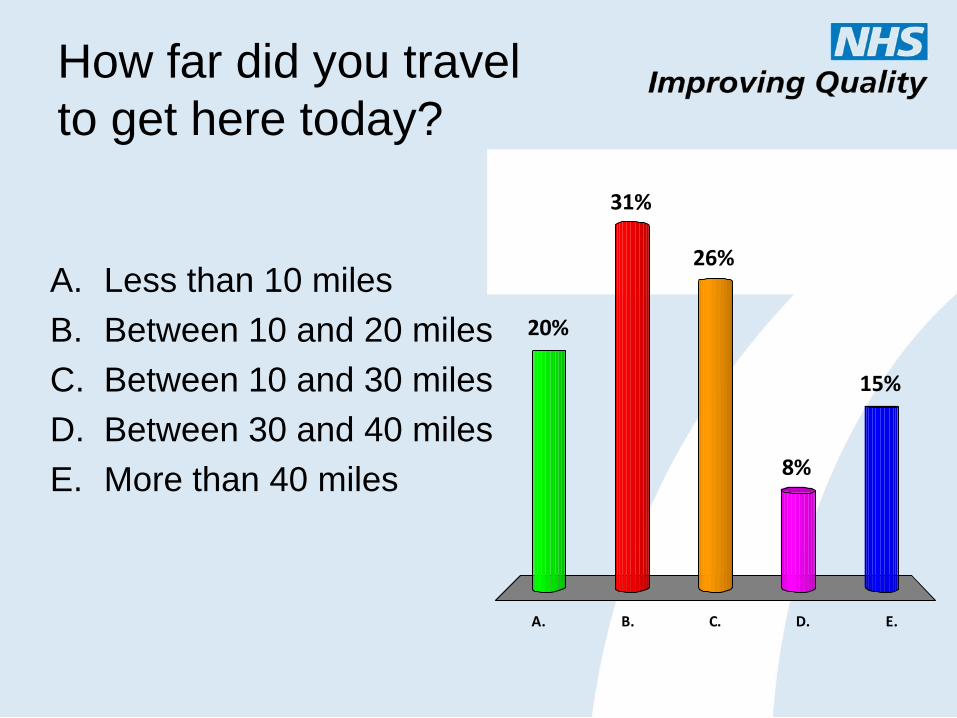
How far did you travel
to get here today?
A. B. C. D. E.
20%
31%
15%
8%
26%A. Less than 10 miles
B. Between 10 and 20 miles
C. Between 10 and 30 miles
D. Between 30 and 40 miles
E. More than 40 miles
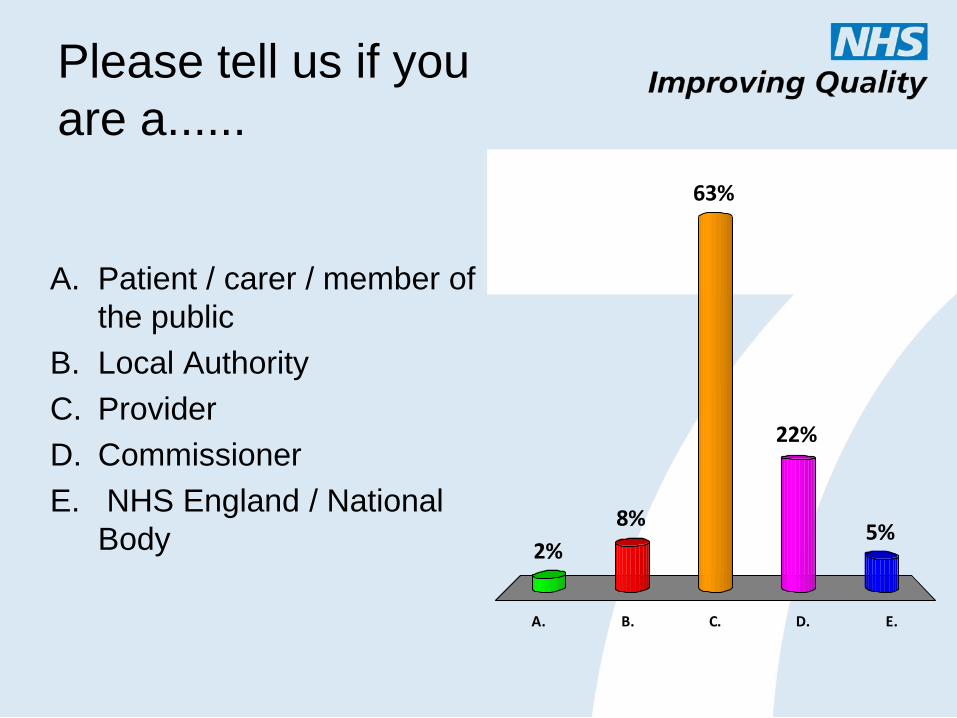
Please tell us if you
are a......
A. B. C. D. E.
2%
8%5%
22%
63%
A. Patient / carer / member of
the public
B. Local Authority
C. Provider
D. Commissioner
E. NHS England / National
Body
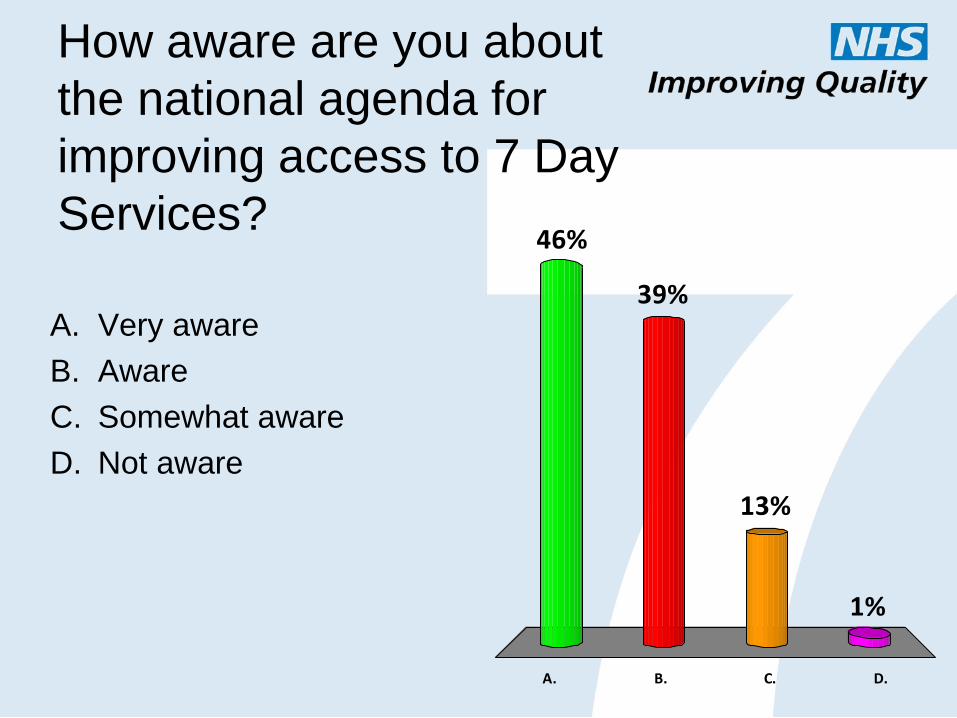
How aware are you about
the national agenda for
improving access to 7 Day
Services?
A. B. C. D.
46%
1%
13%
39%A. Very aware
B. Aware
C. Somewhat aware
D. Not aware
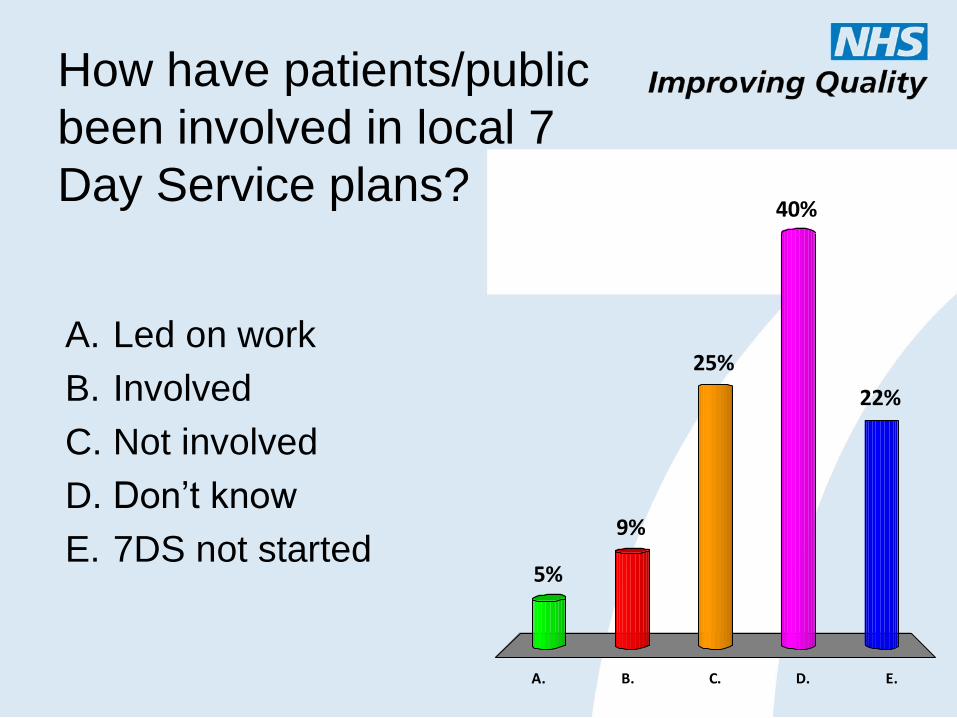
How have patients/public
been involved in local 7
Day Service plans?
A. B. C. D. E.
5%
9%
22%
40%
25%A. Led on work
B. Involved
C. Not involved
D. Don’t know
E. 7DS not started
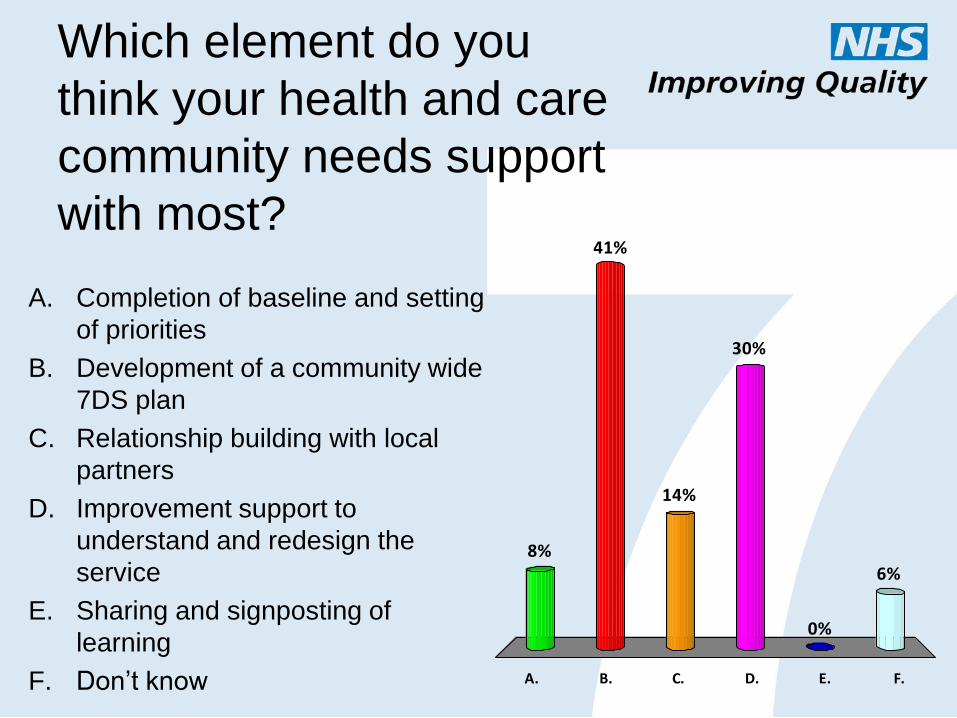
Which element do you
think your health and care
community needs support
with most?
A. B. C. D. E. F.
8%
41%
6%
0%
30%
14%
A. Completion of baseline and setting
of priorities
B. Development of a community wide
7DS plan
C. Relationship building with local
partners
D. Improvement support to
understand and redesign the
service
E. Sharing and signposting of
learning
F. Don’t know
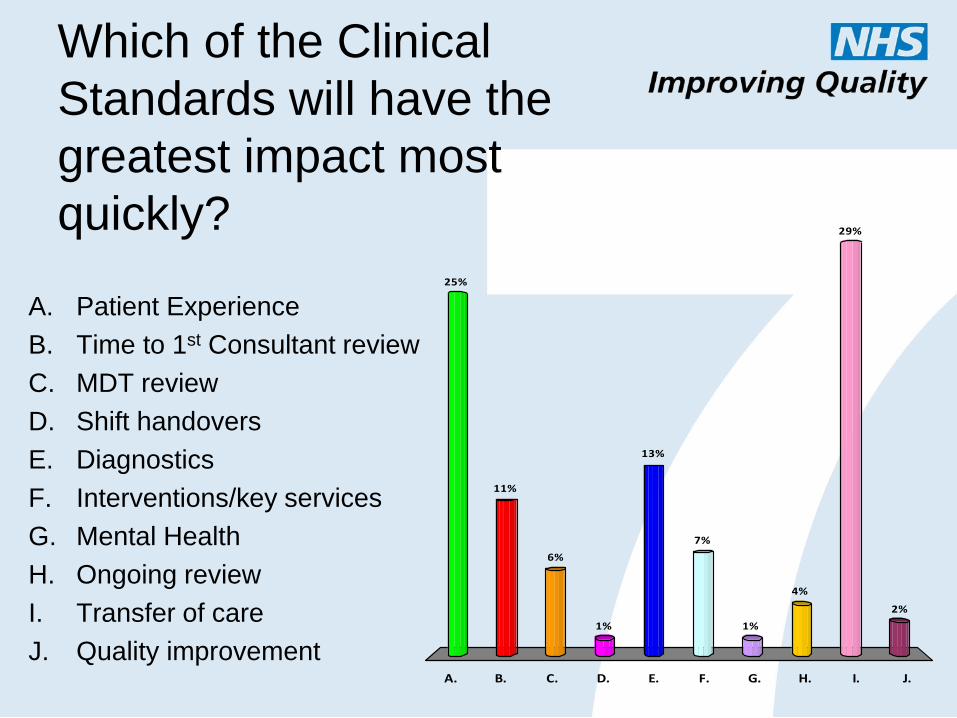
Which of the Clinical
Standards will have the
greatest impact most
quickly?
A. B. C. D. E. F. G. H. I. J.
25%
11%
6%
1%
2%
29%
4%
1%
7%
13%
A. Patient Experience
B. Time to 1st Consultant review
C. MDT review
D. Shift handovers
E. Diagnostics
F. Interventions/key services
G. Mental Health
H. Ongoing review
I. Transfer of care
J. Quality improvement
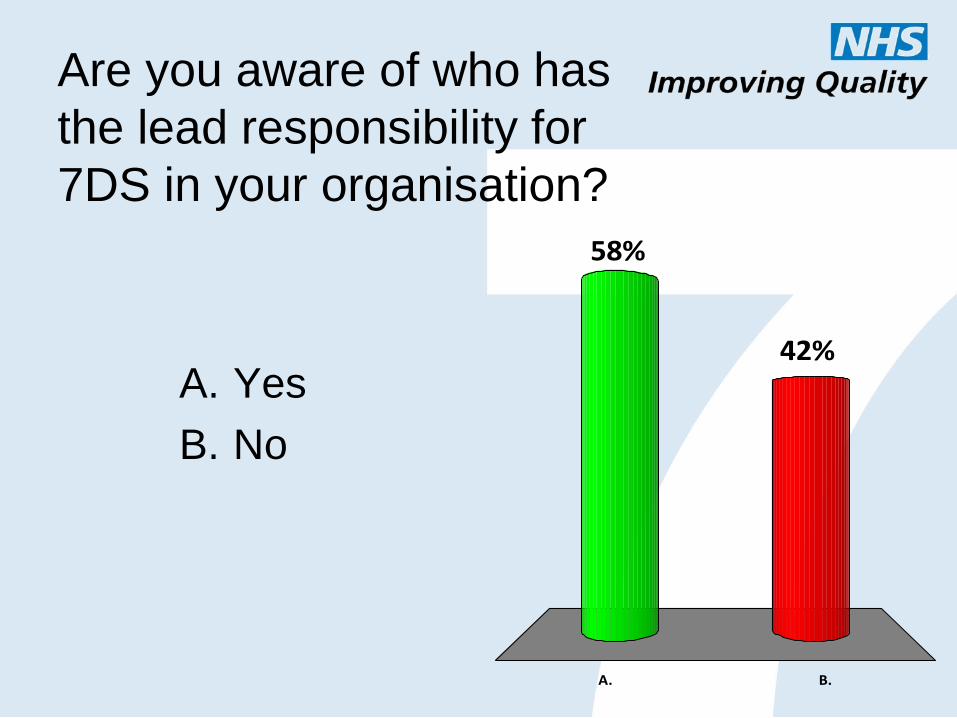
Are you aware of who has
the lead responsibility for
7DS in your organisation?
A. B.
42%
58%
A. Yes
B. No
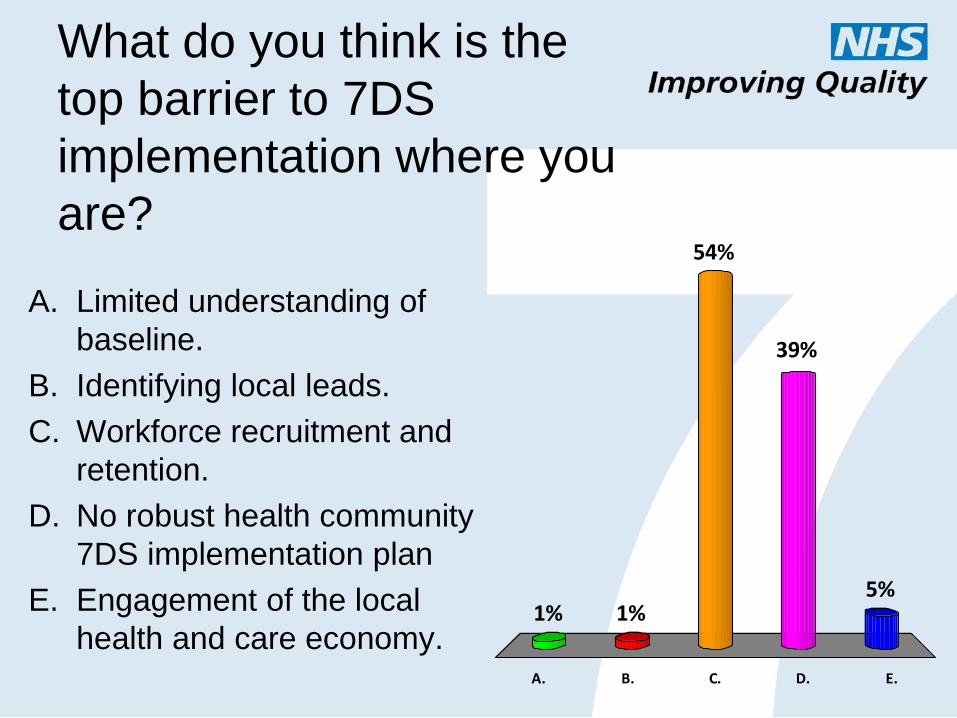
What do you think is the
top barrier to 7DS
implementation where you
are?
A. B. C. D. E.
1% 1%5%
39%
54%
A. Limited understanding of
baseline.
B. Identifying local leads.
C. Workforce recruitment and
retention.
D. No robust health community
7DS implementation plan
E. Engagement of the local
health and care economy.
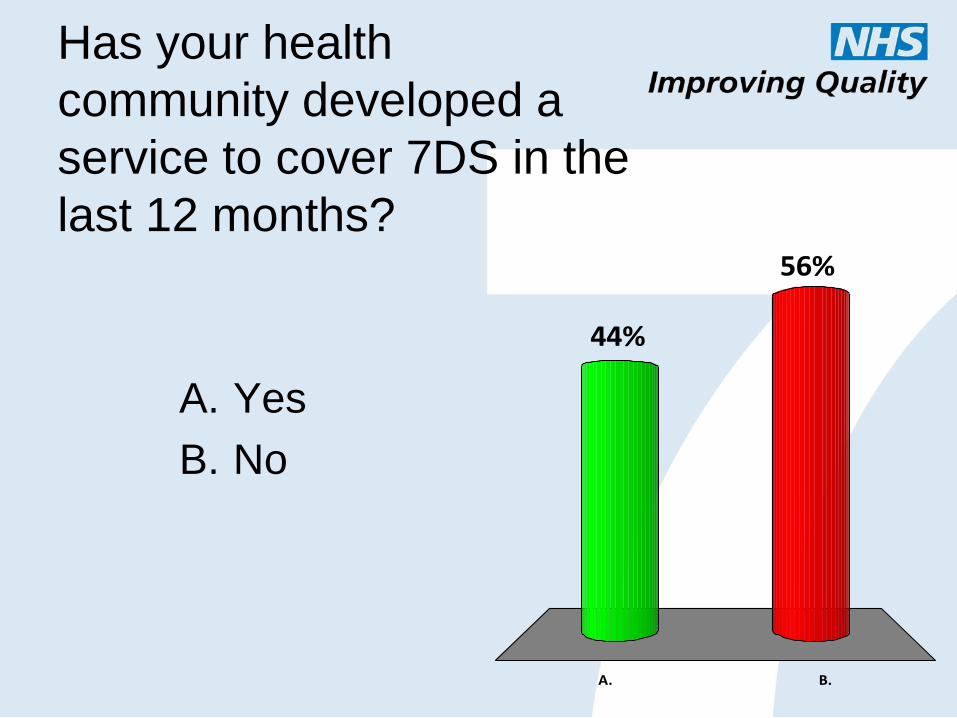
Has your health
community developed a
service to cover 7DS in the
last 12 months?
A. B.
56%
44%
A. Yes
B. No
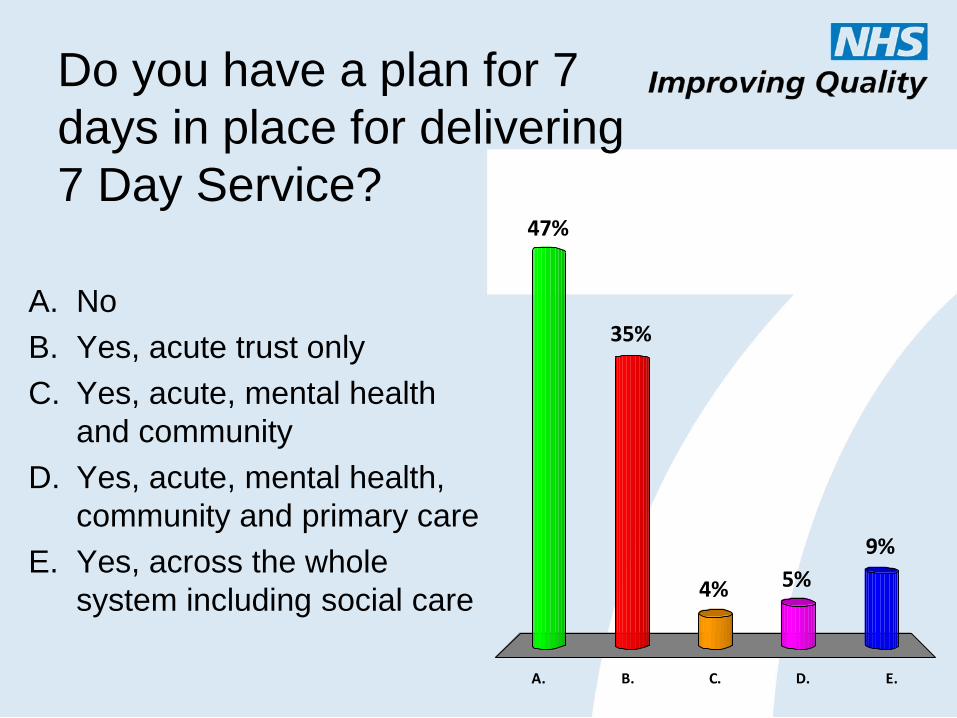
Do you have a plan for 7
days in place for delivering
7 Day Service?
A. B. C. D. E.
47%
35%
9%
5%4%
A. No
B. Yes, acute trust only
C. Yes, acute, mental health
and community
D. Yes, acute, mental health,
community and primary care
E. Yes, across the whole
system including social care

Dr Sanjay Arya, Divisional Medical Director, Division of
Medicine, Wrightington, Wigan & Leigh NHS FT
Wrightington, Wigan & Leigh’s experience of delivering 7 Day Services
NHS Improving Quality and NHS England
Dr Sanjay Arya MBBS (Hons), FRCP (London), FRCP (Glasgow) Consultant Interventional Cardiologist Divisional Medical Director, Division of Medicine Wrightington, Wigan & Leigh NHS Foundation Trust Clinical Lead for Heart Failure, AQuA, North West
25th June 2015
7 Day services at WWL – successes and challenges
Improving Access to Seven Day Services Event
‘‘Patients who are admitted to hospital believe that they are entering a place of safety, where they, their families and carers, have a right to believe that they will receive the best possible care’’.
‘‘Yet there is evidence to the contrary. Patients who are unwell, or
become acutely unwell in hospital, may receive suboptimal care’’
Dr Mary Armitage, Guideline Development Group Chair Acutely ill patients in hospital Royal College of Physicians
Avoidable Weekend Mortality in Hospitals
Patients and family expect that the NHS will provide safe and high
quality service consistently seven days a week
....there is a variation in care depending upon time of the day and
the day of the week
Patients admitted to hospital at weekend have a lower
chance of survival: Fact or Fiction ?
Increased risk of death associated with weekend acute admissions
for ruptured AAA, Acute epiglottitis and Pulmonary embolism (Bell CM et all: New England J Med 2001)
Increased risk of death associated with weekend acute admissions
for acute Myocardial infarction and acute kidney injury: (Kostis WJ et al: New England J Med 2007)
(James MT et all: J Am Soc Nephrol 2010)
Stroke patients have a 20% greater risk of dying if admitted over
a weekend (Palmer W L et al: Dying for the weekend - the association between day of
hosp presentation and the quality and safety of stroke care)

Where there is a 7 day service, there is no observed difference in
mortality rates in the week and at weekend (Bell M et all: The New England journal of Medicine 345:9) (Schmulewitz L et all: Clinical medicine Nov 2005)
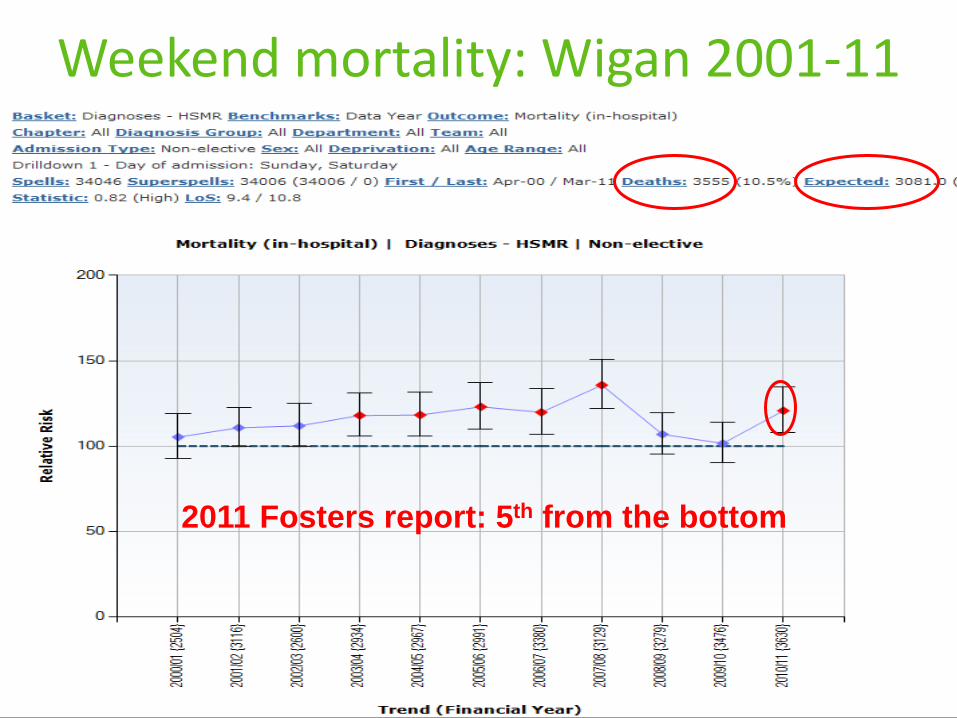
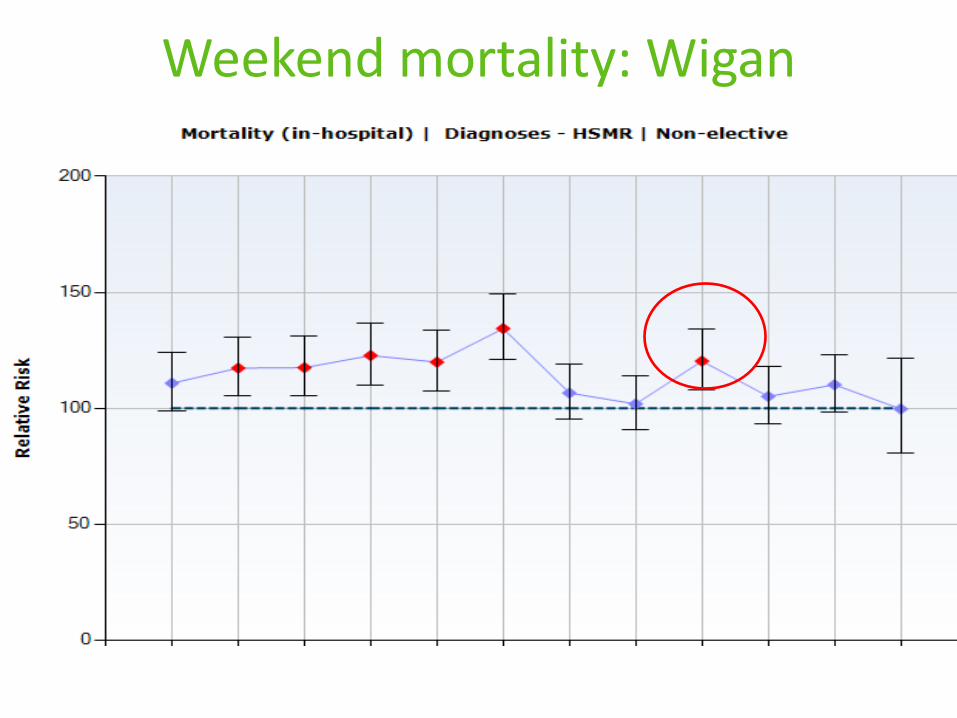
Weekend mortality: Wigan 2001-11
2011 Fosters report: 5th from the bottom
Why is there a ‘Weekend Effect’ ??
Why do patients admitted to hospital at weekend have
a lower chance of survival ?
Why is there an increased risk of death associated with
Weekend emergency admissions? (Aylin P et all: Qual Saf Health Care 2010)
Pre-Hospital factors
Hospital factors
Patient factors
The whole health community needs to address the problem of
increased mortality over the weekend
•Engaged clinicians (medical,nursing,physio,OT) and managers
•Developed leadership: Divisional Director & 4 Clinical Directors
•Involved everyone: Martin Farrier’s weekly mortality data:
There should be a 7 day access to all aspects of care:
Medical, Nursing, Diagnostics, Palliative care, GPs, Social services
• CoE Consultants in the community – supporting GPs
• Engaged Nursing / Care homes – advanced care planning
• Improved end-of-life care for terminally ill patients
Is there a solution? Wigan experience
Why are there more deaths? ‘Weekend Effect’
Increased Consultant presence: Cost effective / Reduces mortality
• Recruited 3 more A&E and 3 more MAU consultants
• Increased presence of Consultants on A&E, MAU and Medical
wards on weekends and bank holidays
Is there a solution? Wigan experience
Why are there more deaths? ‘Weekend Effect’
Right patient Right ward, beyond the first 24 hours of admission
•Specialists felt engaged, valued & comfortable in managing patients
•Improved patient pathway / journey / care bundles
Support services will also need to adopt 7 day working practice if
the full benefits of 7 day Consultant service are to be realised
•Increased presence of Physio, OT and Social services over
weekends and bank holidays
•Increased availability of diagnostics/therapeutics over weekends
and bank holidays (Radiology, Endoscopy, Pacing)
Is there a solution? Wigan experience
Why are there more deaths? ‘Weekend Effect’
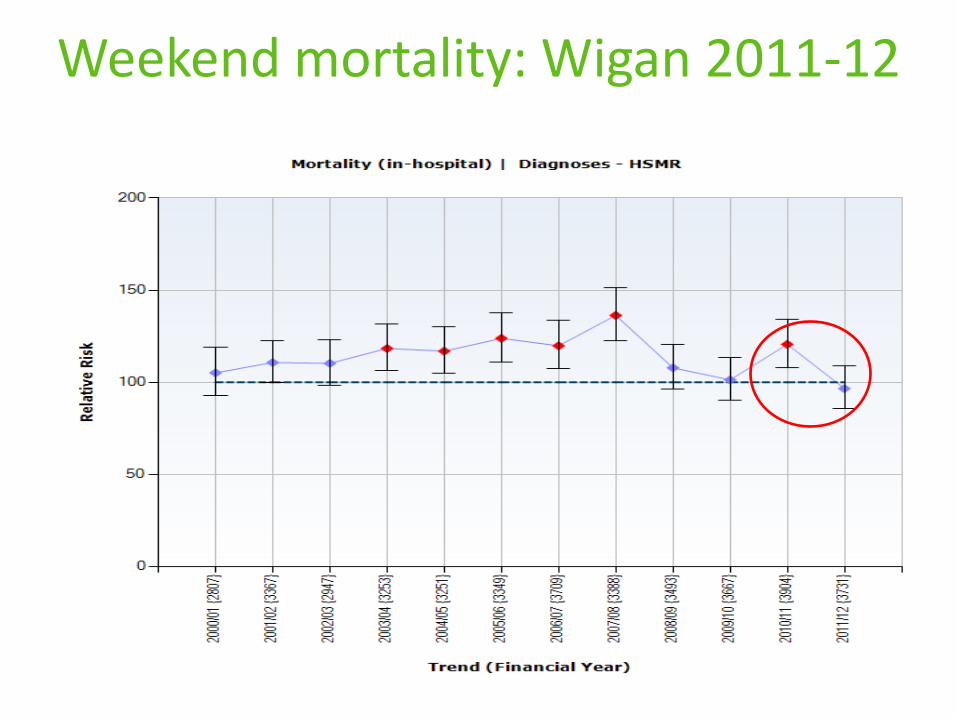
Weekend mortality: Wigan 2011-12
Weekend mortality: Wigan
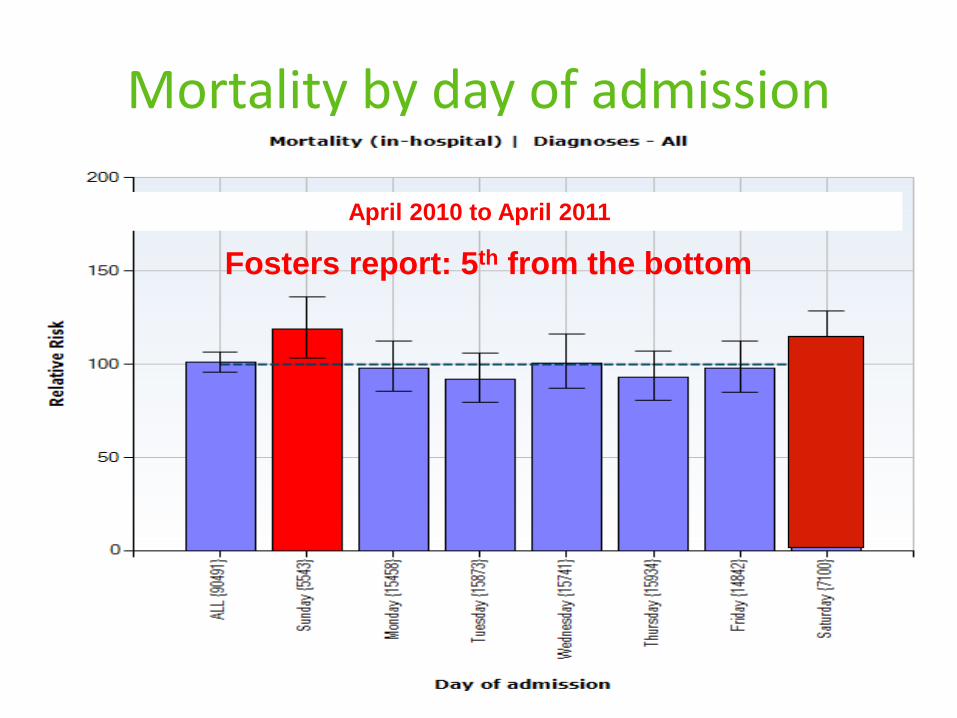
Mortality by day of admission
April 2010 to April 2011
Fosters report: 5th from the bottom
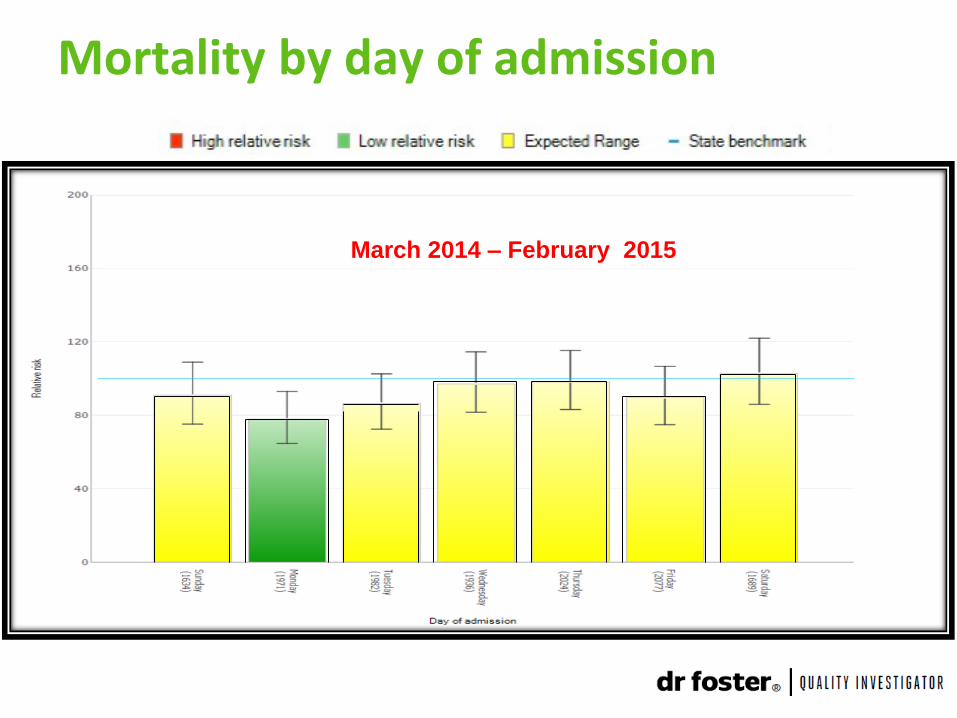
Mortality by day of admission
March 2014 – February 2015
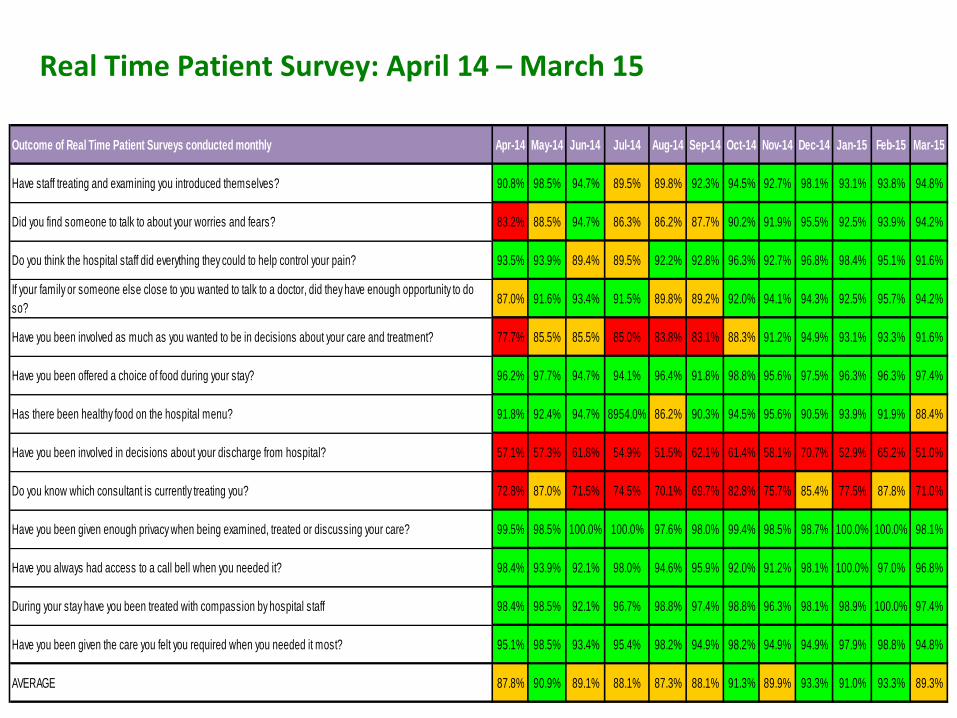
Outcome of Real Time Patient Surveys conducted monthly Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Have staff treating and examining you introduced themselves? 90.8% 98.5% 94.7% 89.5% 89.8% 92.3% 94.5% 92.7% 98.1% 93.1% 93.8% 94.8%
Did you find someone to talk to about your worries and fears? 83.2% 88.5% 94.7% 86.3% 86.2% 87.7% 90.2% 91.9% 95.5% 92.5% 93.9% 94.2%
Do you think the hospital staff did everything they could to help control your pain? 93.5% 93.9% 89.4% 89.5% 92.2% 92.8% 96.3% 92.7% 96.8% 98.4% 95.1% 91.6%
If your family or someone else close to you wanted to talk to a doctor, did they have enough opportunity to do
so?87.0% 91.6% 93.4% 91.5% 89.8% 89.2% 92.0% 94.1% 94.3% 92.5% 95.7% 94.2%
Have you been involved as much as you wanted to be in decisions about your care and treatment? 77.7% 85.5% 85.5% 85.0% 83.8% 83.1% 88.3% 91.2% 94.9% 93.1% 93.3% 91.6%
Have you been offered a choice of food during your stay? 96.2% 97.7% 94.7% 94.1% 96.4% 91.8% 98.8% 95.6% 97.5% 96.3% 96.3% 97.4%
Has there been healthy food on the hospital menu? 91.8% 92.4% 94.7% 8954.0% 86.2% 90.3% 94.5% 95.6% 90.5% 93.9% 91.9% 88.4%
Have you been involved in decisions about your discharge from hospital? 57.1% 57.3% 61.8% 54.9% 51.5% 62.1% 61.4% 58.1% 70.7% 52.9% 65.2% 51.0%
Do you know which consultant is currently treating you? 72.8% 87.0% 71.5% 74.5% 70.1% 69.7% 82.8% 75.7% 85.4% 77.5% 87.8% 71.0%
Have you been given enough privacy when being examined, treated or discussing your care? 99.5% 98.5% 100.0% 100.0% 97.6% 98.0% 99.4% 98.5% 98.7% 100.0% 100.0% 98.1%
Have you always had access to a call bell when you needed it? 98.4% 93.9% 92.1% 98.0% 94.6% 95.9% 92.0% 91.2% 98.1% 100.0% 97.0% 96.8%
During your stay have you been treated with compassion by hospital staff 98.4% 98.5% 92.1% 96.7% 98.8% 97.4% 98.8% 96.3% 98.1% 98.9% 100.0% 97.4%
Have you been given the care you felt you required when you needed it most? 95.1% 98.5% 93.4% 95.4% 98.2% 94.9% 98.2% 94.9% 94.9% 97.9% 98.8% 94.8%
AVERAGE 87.8% 90.9% 89.1% 88.1% 87.3% 88.1% 91.3% 89.9% 93.3% 91.0% 93.3% 89.3%
Real Time Patient Survey: April 14 – March 15
Friends and Family Test 2014-2015
• The CQUIN Target for the year has been achieved.
• Both A&E and Inpatients response rates were achieved:
– Inpatient Areas 40% required 40.63% achieved
– A&E 20% required 31.76 achieved
• NHS England representative commented “Congratulations on this notable achievement”
• WWL will now receive £110,000 in recognition.
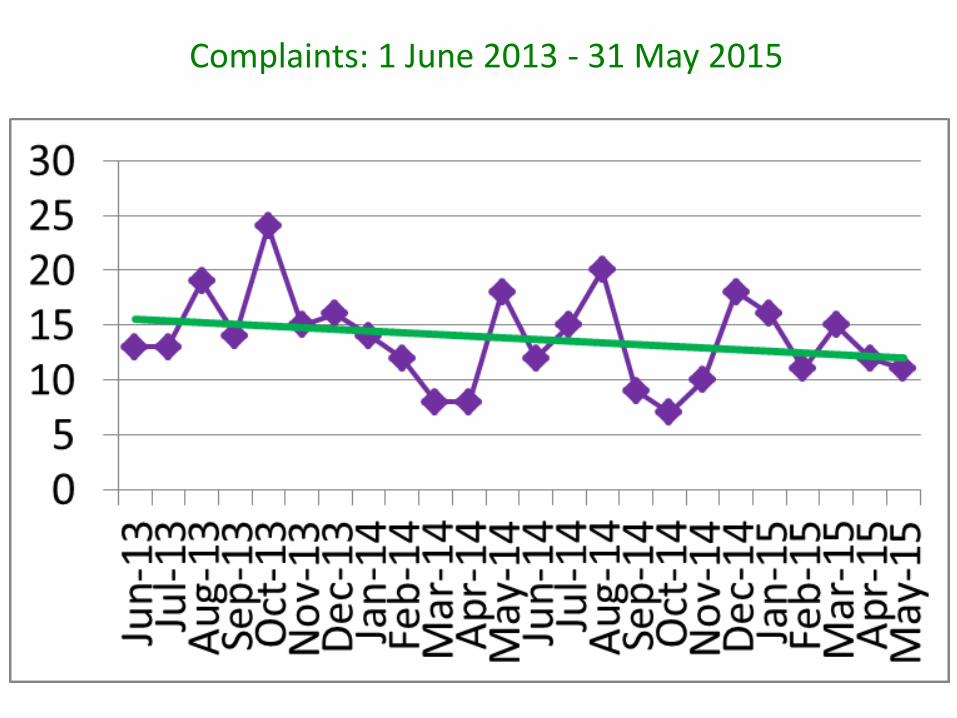
Complaints: 1 June 2013 - 31 May 2015
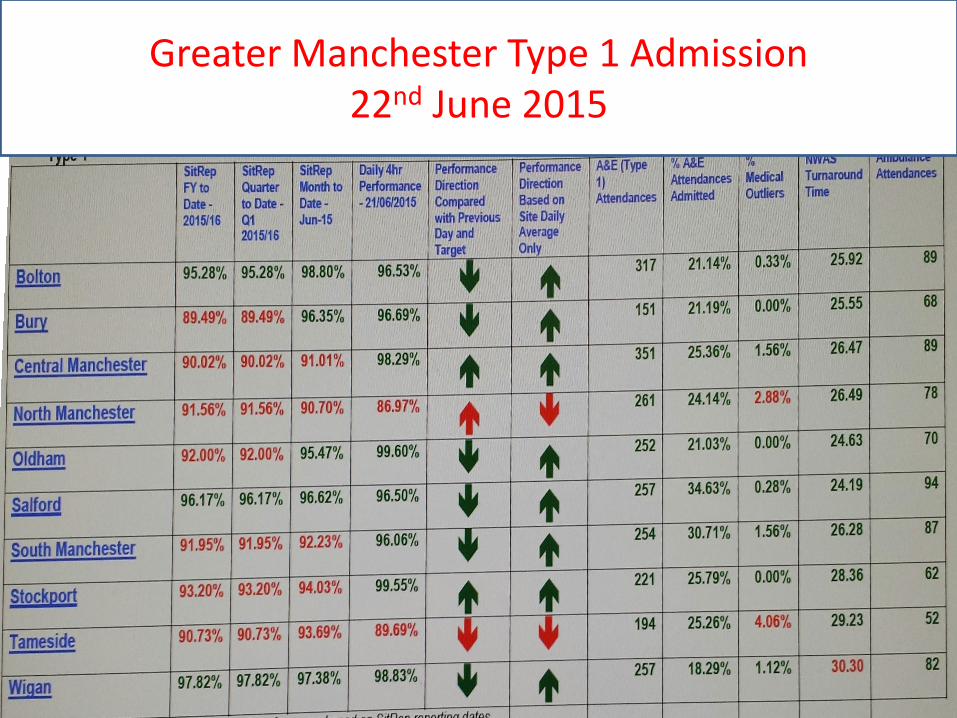
Greater Manchester Type 1 Admission 22nd June 2015
9. Transfer to community, primary and social care
Support services, both in the hospital and in primary, community and mental health settings must be available seven days a week to ensure that the next steps in the patient’s care pathway, as determined by the daily consultant-led review, can be taken.
10 Clinical Standards

Thank you
John Boyington, Chairman,
Bury GP Federation
Seven Day Access to Primary Care
NHS Improving Quality and NHS England
Bury GP Federation
Seven Day Access to Primary Care Developing and delivering the Bury model
Improving Access to Seven Day Services Event
25th June 2015
Bury – Greater Manchester
61
25/06/2015 Bury GP Practices Ltd
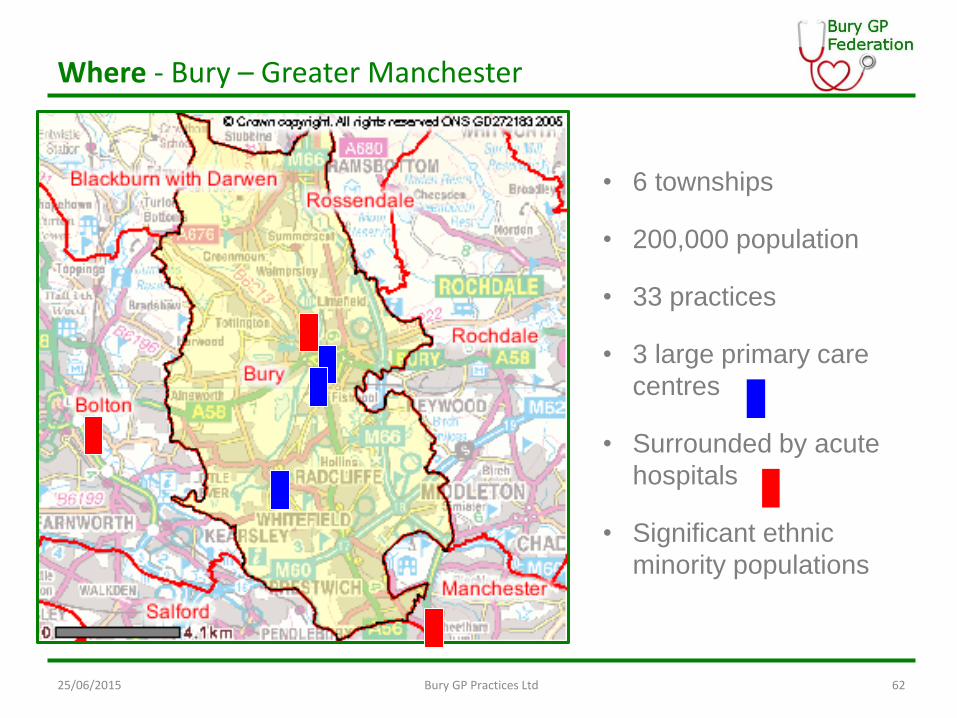
Where - Bury – Greater Manchester
62
• 6 townships
• 200,000 population
• 33 practices
• 3 large primary care
centres
• Surrounded by acute
hospitals
• Significant ethnic
minority populations
25/06/2015 Bury GP Practices Ltd
Bury GP Practices Ltd
• Preliminary development started 2011
• final structure agreed – September 2012
• Shareholders loaned Company 99p per patient as start-up fund - £175k
• Company registered at Companies House in November 2012
• Initial Board February 2013
• Board Revised 2014
• Further changes to Board structure now being approved
• 30 of the CCG’s 33 practices hold shares
25/06/2015 Bury GP Practices Ltd 63
PMCF : Easy-GP Summary
Building on the services and experience from Healthier Radcliffe Pilot (Ph1)
Easy GP Programme is founded on the following principles:
• Right care at the right time for patients at a place convenient to them
• Provide services that better value patients time
• Offer patients greater freedom to exercise control when interacting with General Practice
• Ensuring Patients have information they want to make better choices about GP services
25/06/2015 Bury GP Practices Ltd 64
200,000 registered patients 12 month programme
6 month service period £3M funding 30 of 33 GP Practices
Extended Working Hours
Longer opening hours including :
• Extended weekday opening (8am to 8pm), and
• Saturdays and Sundays (8am to 6pm)
– All services available locally but not in every GP practice
– Every patient’s notes available to GP providing cover during extended hours
– Reducing likelihood of people needing to go to hospital
– Making it easier for those who work or have school age children to avoid disrupting their working/school day
– Easier for families to attend with elderly relatives
Telephone Consultations
25/06/2015 Bury GP Practices Ltd 65
Easy GP Projects (1)
Ensure that all patients who request an appointment are offered the option of a telephone consultation:
– Currently about 35% of practices offer telephone consultation to patients
– We believe that such consultations can be a better use of GP and patient time
– Patients are often capable of knowing whether they need to see the clinician face-to-face
– A higher proportion of telephone consultations would release GP time and reduce waiting times for appointments
1 2
Increased Online Access
Increase use of online services from current 4% of patients to 60%+:
– Currently patients who register can make appointments or re-order prescriptions using online
– All practices in Bury are enabled for online access
– Registration is a difficult process which is not user friendly – we plan to change this significantly and offer help to patients to register and use online services
– More services should be available to patients over time including them having access to their own health records and the ability to ‘email’ their GP.
– Increasing registration will significantly widen access
GP Comparison Website
25/06/2015 Bury GP Practices Ltd 66
Easy GP Projects (2)
Develop a “GP-Comparison” website to enable patients to make better choices about GP services:
– Current websites offer limited information to patients
– This website would offer information in a detailed and searchable form, modelled on successful comparison-style sites used elsewhere
– The website would enable patients to search for staff availability, service availability, staff expertise etc and would show information for all relevant practices in Bury
3 4
• The service model was developed collaboratively with input from member practices.
• Defined a number of ‘design principles’ which influenced the nature of the service:
– Service operates from 6:30pm – 8pm weekdays and 8am – 6pm on weekends & Bank Hols
– Designed to provide up to 1,425 GP appointments per week outside of core GP hours
– The service is delivered from 5 local GP practice locations
– All patients registered with a Bury GP are able to access appointments at any of the five sites.
– All clinicians working in the service have read and write access to the patient’s GP record.
– Delivered collaboratively by over 30 local GPs and up to 20 local admin/support staff.
Designing the Bury EWH service
25/06/2015 Bury GP Practices Ltd 67
– Designed to be sustainable, both in terms of sharing the demand placed on the GP workforce (no obligation on individual GPs) and meet the future access needs of local patients.
– The main focus is currently to provide additional GP appointments to all patients (focus of PMCF pilot)
– Appointments are accessed through the patients’ own practices as ‘an extension’ of the primary care service offered by their GP practice
– Aims to use a consistent core staff base (preferably from within member practices) to provide continuity and consistency in the service and to make it a familiar experience for patients.
– Where possible, the service will be delivered through a member practice. Where this is not possible, then the GP Federation will build its own in-house capacity to deliver the service.
Designing the Bury EWH service
25/06/2015 Bury GP Practices Ltd 68
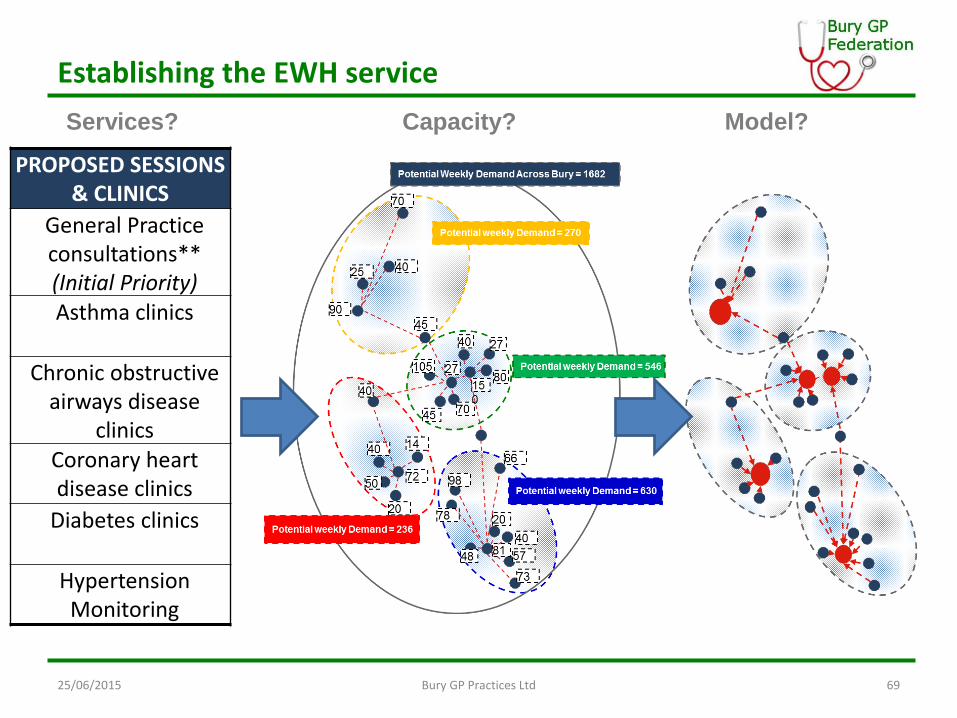
Establishing the EWH service
PROPOSED SESSIONS & CLINICS
General Practice consultations** (Initial Priority) Asthma clinics
Chronic obstructive airways disease
clinics Coronary heart disease clinics
Diabetes clinics
Hypertension Monitoring
Services? Capacity? Model?
25/06/2015 Bury GP Practices Ltd 69
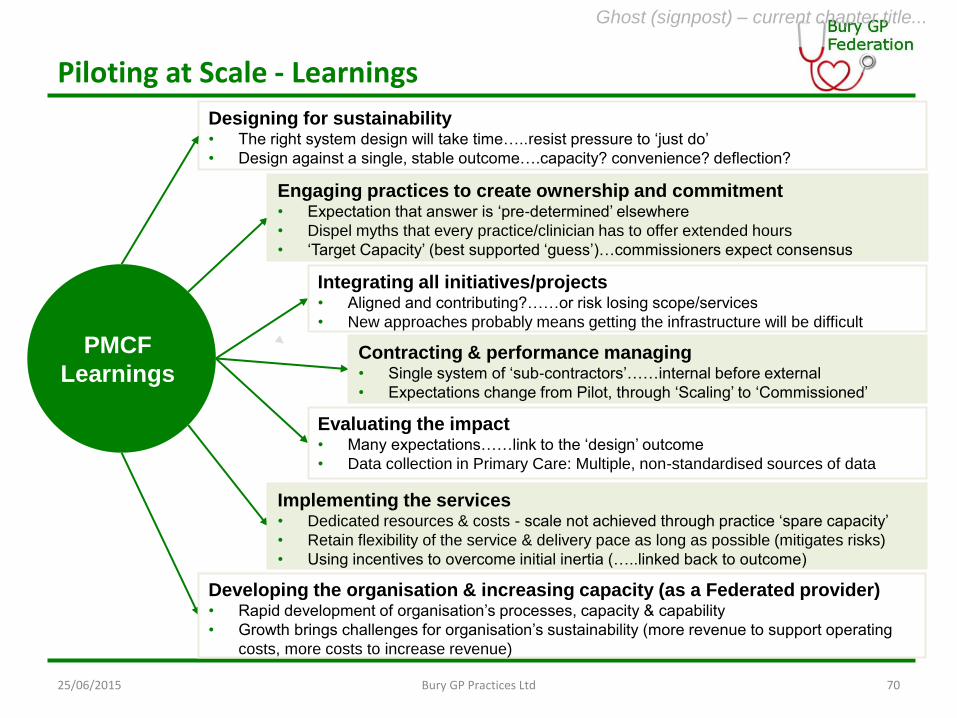
Piloting at Scale - Learnings
PMCF
Learnings
Designing for sustainability • The right system design will take time…..resist pressure to ‘just do’
• Design against a single, stable outcome….capacity? convenience? deflection?
Engaging practices to create ownership and commitment • Expectation that answer is ‘pre-determined’ elsewhere
• Dispel myths that every practice/clinician has to offer extended hours
• ‘Target Capacity’ (best supported ‘guess’)…commissioners expect consensus
Integrating all initiatives/projects • Aligned and contributing?……or risk losing scope/services
• New approaches probably means getting the infrastructure will be difficult
Contracting & performance managing • Single system of ‘sub-contractors’……internal before external
• Expectations change from Pilot, through ‘Scaling’ to ‘Commissioned’
Evaluating the impact • Many expectations……link to the ‘design’ outcome
• Data collection in Primary Care: Multiple, non-standardised sources of data
Implementing the services • Dedicated resources & costs - scale not achieved through practice ‘spare capacity’
• Retain flexibility of the service & delivery pace as long as possible (mitigates risks)
• Using incentives to overcome initial inertia (…..linked back to outcome)
Developing the organisation & increasing capacity (as a Federated provider) • Rapid development of organisation’s processes, capacity & capability
• Growth brings challenges for organisation’s sustainability (more revenue to support operating
costs, more costs to increase revenue)
Ghost (signpost) – current chapter title...
Bury GP Practices Ltd 25/06/2015 70
25/06/2015 Bury GP Practices Ltd 71
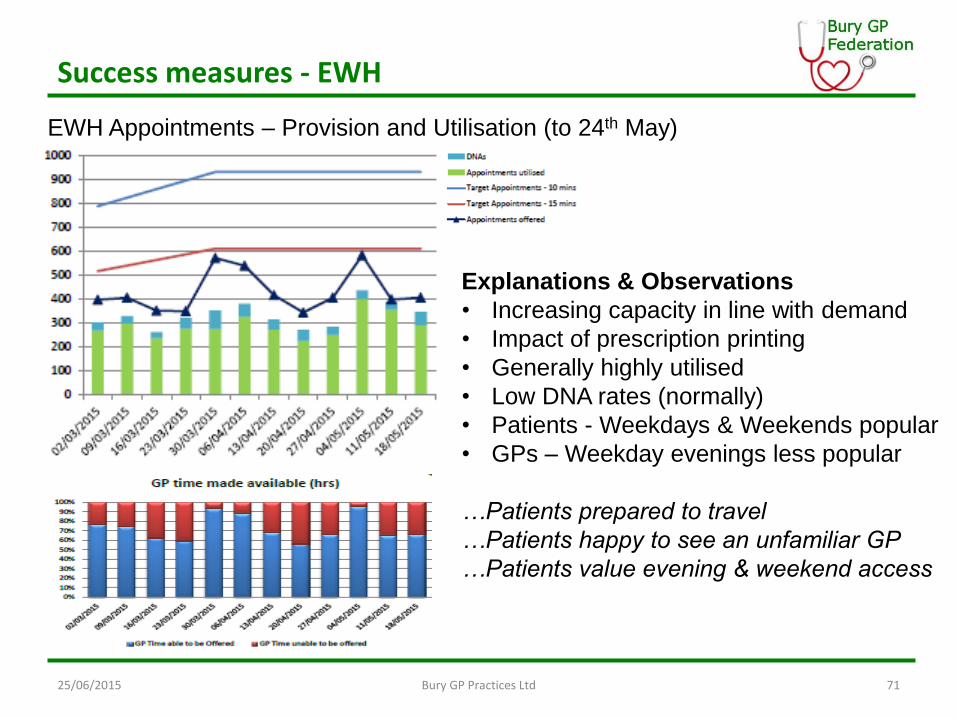
Success measures - EWH
EWH Appointments – Provision and Utilisation (to 24th May)
Explanations & Observations
• Increasing capacity in line with demand
• Impact of prescription printing
• Generally highly utilised
• Low DNA rates (normally)
• Patients - Weekdays & Weekends popular
• GPs – Weekday evenings less popular
…Patients prepared to travel
…Patients happy to see an unfamiliar GP
…Patients value evening & weekend access
25/06/2015 Bury GP Practices Ltd 72
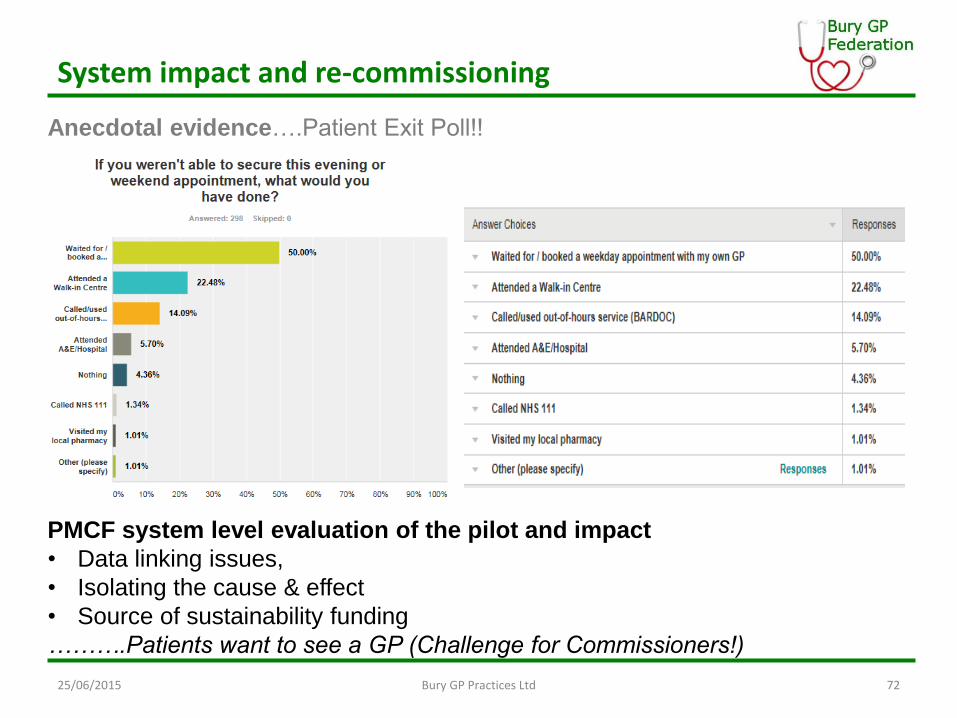
System impact and re-commissioning
Anecdotal evidence….Patient Exit Poll!!
PMCF system level evaluation of the pilot and impact
• Data linking issues,
• Isolating the cause & effect
• Source of sustainability funding
……….Patients want to see a GP (Challenge for Commissioners!)
25/06/2015 Bury GP Practices Ltd 73
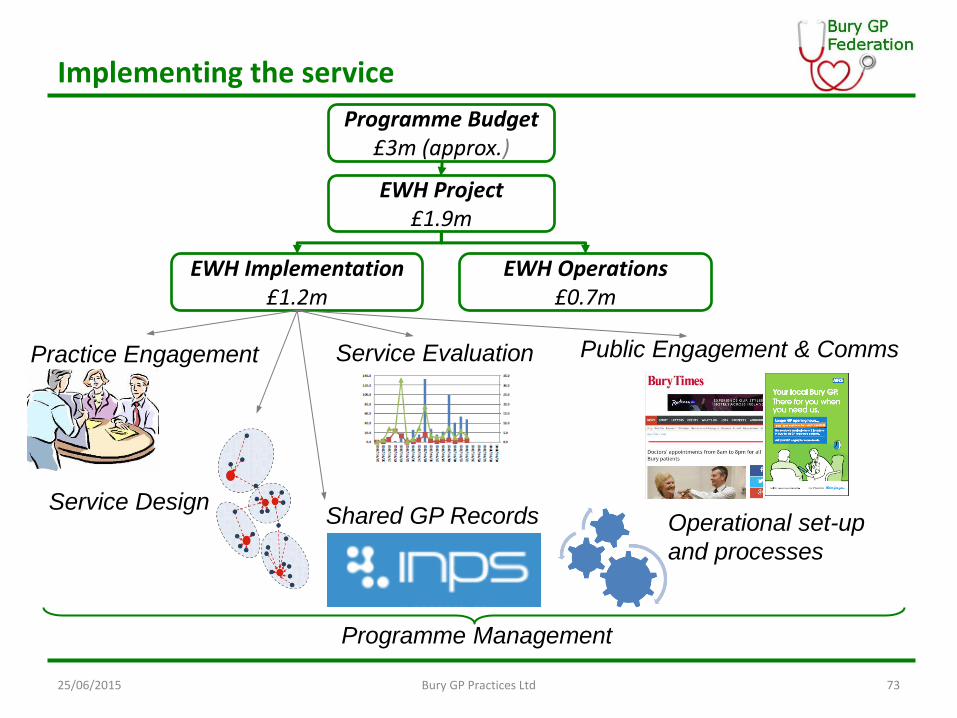
Implementing the service
Programme Budget £3m (approx.)
EWH Project £1.9m
EWH Implementation £1.2m
EWH Operations £0.7m
Programme Management
Public Engagement & Comms
Shared GP Records
Service Evaluation
Service Design Operational set-up
and processes
Practice Engagement
Lessons Learned
This is hard work and takes time!
• Collaboration needs to be encouraged – can’t be demanded
• It takes time and effort to get things lined-up
• GP’s need to be free to engage as providers but commissioners need to commission whole population service
• Patients want and value this service
25/06/2015 Bury GP Practices Ltd 74
Lessons Learned
NO PLAN SURVIVES FIRST CONTACT WITH THE ENEMY
75
or your allies!
25/06/2015 Bury GP Practices Ltd
Dr Gilbert Wieringa, Consultant & Clinical Lead for Laboratory
Medicine,
Bolton NHS FT
Point of Care Testing NHS Improving Quality and NHS England
NHS services, 7 days a week
The contribution of near patient
diagnostic testing
Gilbert Wieringa, 25th June 2015
Diagnostics technology
Applications
• Emergency care
• Long term condition management
• Self management
• Screening/diagnosis
Abingdon Emergency Care Unit
• Opening times: 0800-2000, Mon-Fri; 0800-1600 w/e
• Exclusions: stroke, ?MI
• Referrals: From GPs, community nurses, ambulance
paramedics
• Facilities: 5 beds, max 72 hour stay
• Staff: GPs, nurses, HCAS, therapists, social workers
Abingdon Emergency Care Unit
Ongoing outcomes:
• 5000 patients seen in 2014, average age 89
• Typical diagnoses: heart failure, chest/bladder infections
• 65% discharged same day, 18% EMU admission, 17%
acute admission referral
• “Small decrease” in A/E admissions at John Radcliffe
Hospital
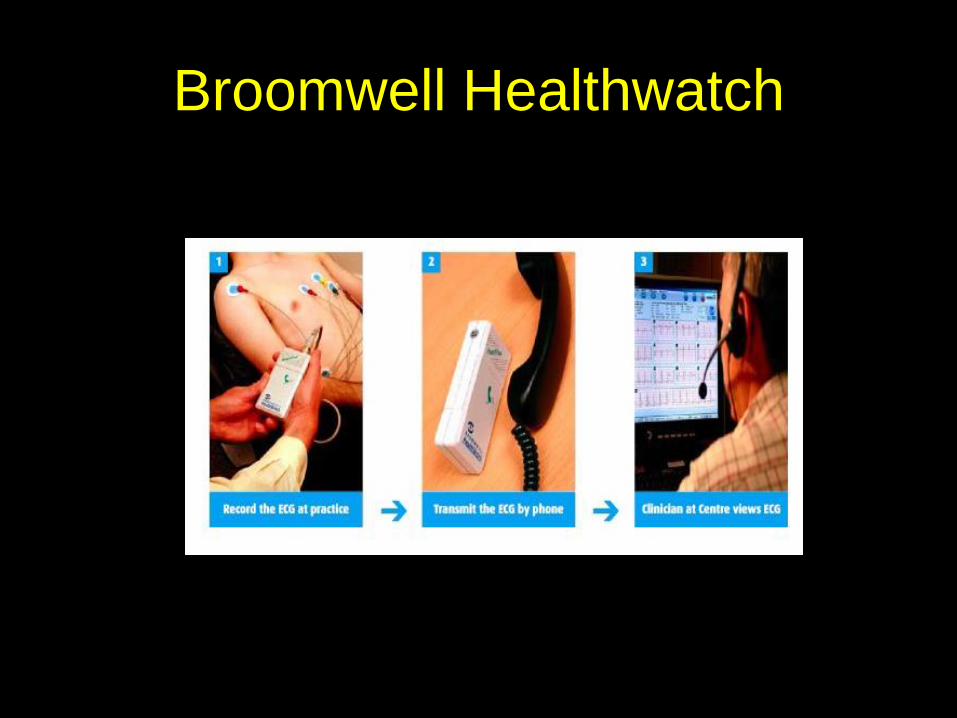
Broomwell Healthwatch
Examples of IS providers
New roles for community pharmacy
Health promotion,
disease prevention
Managing long term
conditions
Medicines use reviews
Prescribing
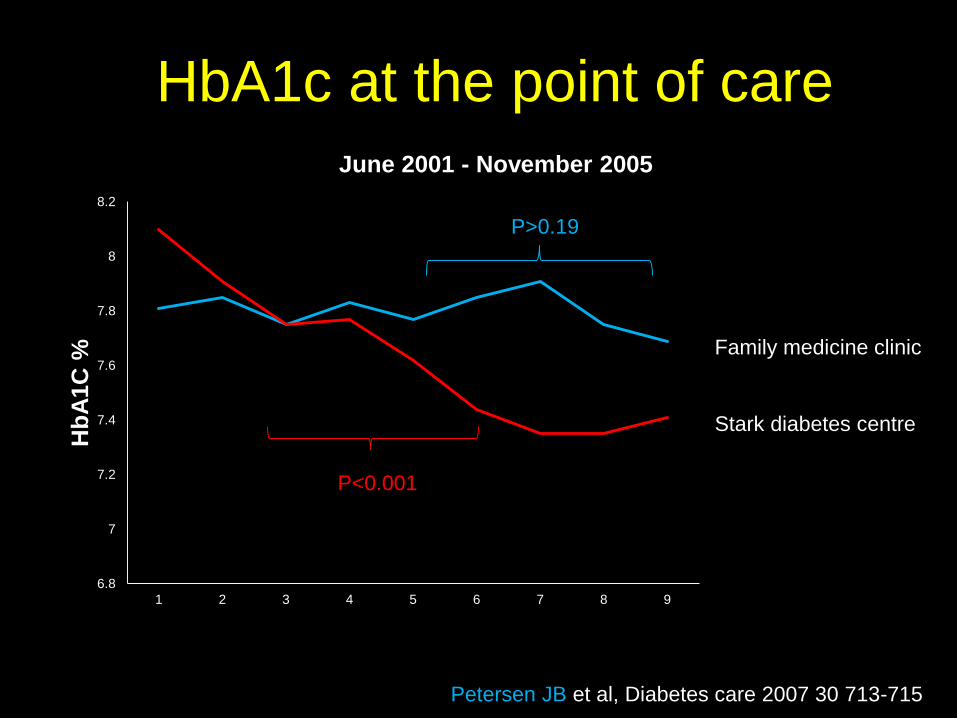
HbA1c at the point of care
6.8
7
7.2
7.4
7.6
7.8
8
8.2
1 2 3 4 5 6 7 8 9
Hb
A1C
%
June 2001 - November 2005
Family medicine clinic
Stark diabetes centre
P<0.001
P>0.19
Petersen JB et al, Diabetes care 2007 30 713-715
Self-monitoring of oral anticoagulation: a
systematic review and meta-analysis.
Significant reductions in:
Thromboembolic events
All cause mortality
Major haemorrhage
11/14 RCTs reported improved INR results
Heneghan C et al, Lancet 2006 367(9508); 404-411
Accessing POCT: Patients’ perspectives
Sounded like a very good idea and just right for people like me who don’t want to be bothering the doctor or nurse.
“You know the outcome immediately instead of waiting for 7-10 days for the result.”
“Seemed a lot quicker than at the doctor’s surgery, with less hanging around and less people queued up. I would recommend it to anyone.”
Accessing POCT: Patients’ perspectives
“It doesn’t matter who I see. I have plenty of
confidence in my doctor and the pharmacist.”
“I was seen as soon as I arrived, given a seat and
attended to in private. What a good idea and a
super service.”
“Nice and warm, friendly staff.”
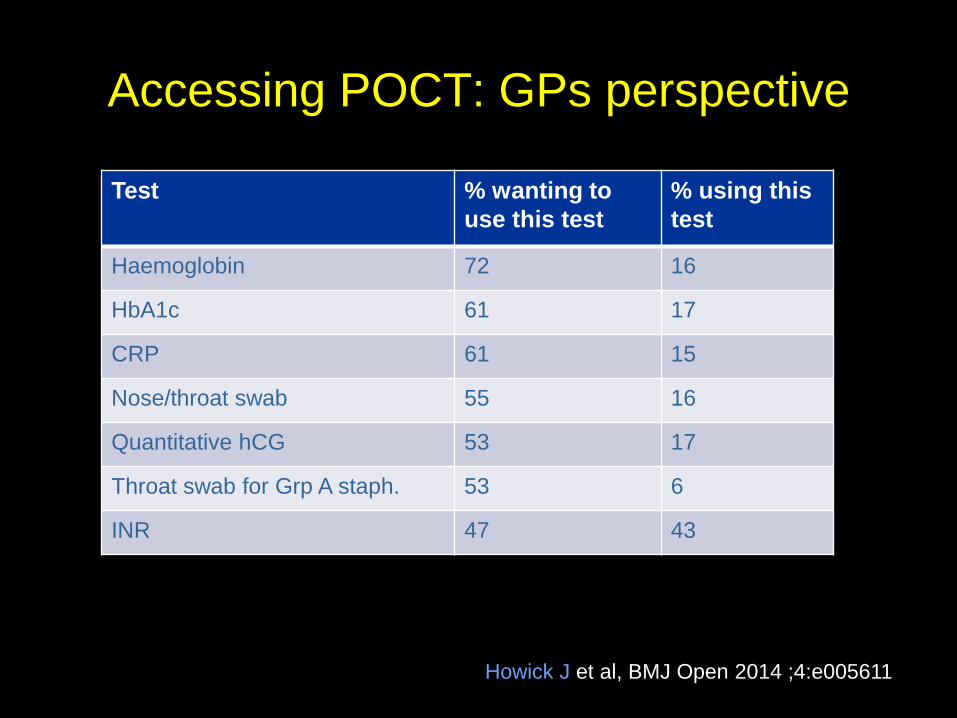
Accessing POCT: GPs perspective
Test % wanting to
use this test
% using this
test
Haemoglobin 72 16
HbA1c 61 17
CRP 61 15
Nose/throat swab 55 16
Quantitative hCG 53 17
Throat swab for Grp A staph. 53 6
INR 47 43
Howick J et al, BMJ Open 2014 ;4:e005611
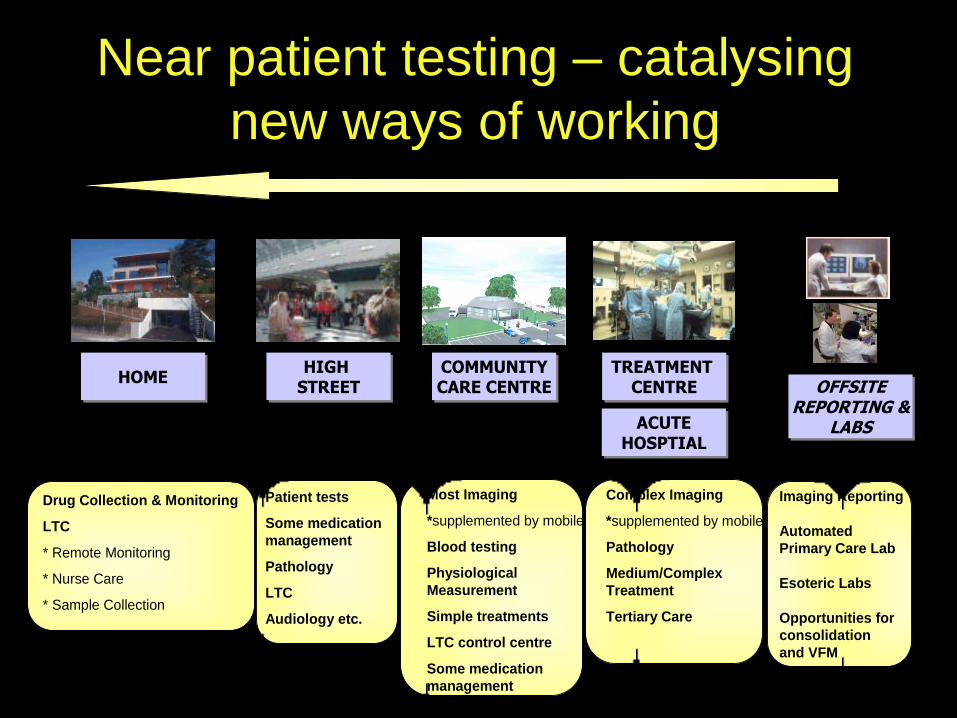
Near patient testing – catalysing
new ways of working
HOMEHOME HIGH STREET
HIGH STREET
COMMUNITYCARE CENTRE
COMMUNITYCARE CENTRE
TREATMENT CENTRE
TREATMENT CENTRE
ACUTEHOSPTIAL
ACUTEHOSPTIAL
Drug Collection & Monitoring
LTC
* Remote Monitoring
* Nurse Care
* Sample Collection
Patient tests
Some medication
management
Pathology
LTC
Audiology etc.
Most Imaging
*supplemented by mobile
Blood testing
Physiological
Measurement
Simple treatments
LTC control centre
Some medication
management
Complex Imaging
*supplemented by mobile
Pathology
Medium/Complex
Treatment
Tertiary Care
OFFSITEREPORTING &
LABS
OFFSITEREPORTING &
LABS
Imaging Reporting
Automated
Primary Care Lab
Esoteric Labs
Opportunities for
consolidation
and VFM
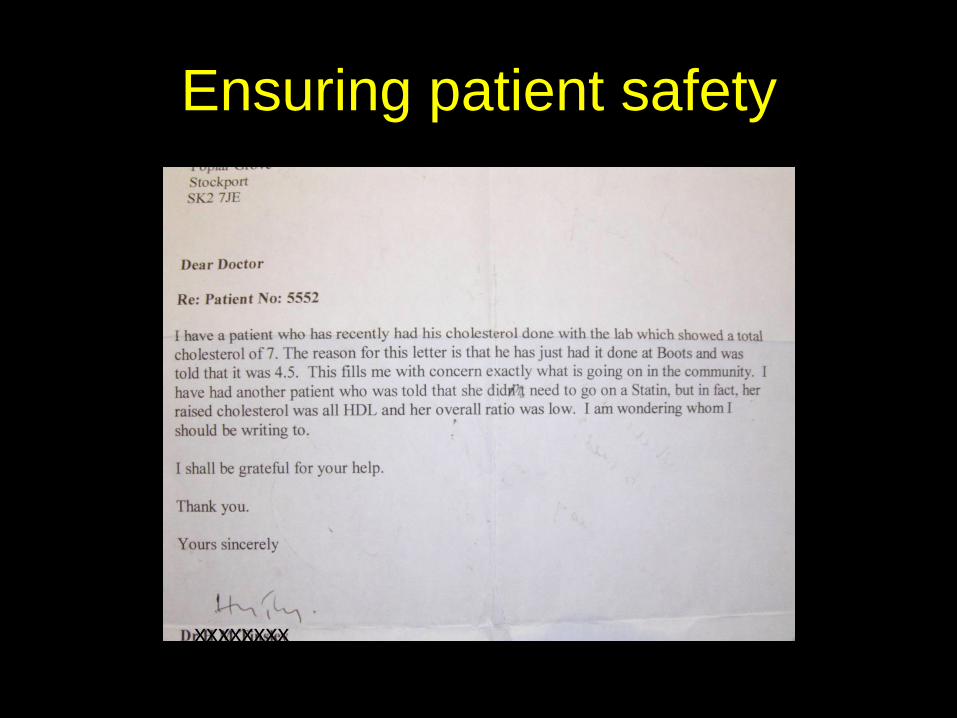
Ensuring patient safety
xxxxxxxx
NHS services, 7 days a week forum
• Less than 50% organisations provide diagnostic/
scientific services 7 days a week
• A better understanding is needed of how to
commission diagnostic and scientific services
• Providers should be required to demonstrate
how their diagnostic services support 7 day
working
December 2013
Panel of Presenters
Q & A
NHS Improving Quality and NHS England
Refreshment Break
NHS Improving Quality and NHS England
Paul Fleming, Associate Director, IM&T, NHS Stockport CCG
Technology to Integrate and Empower
NHS Improving Quality and NHS England

Connect, Integrate,
Empower, Collaboratele
headline
NHS Stockport Clinical Commissioning Group
7th Floor
Regent House
Heaton Lane
Stockport SK4 1BS
Tel: 0161 426 9900 Fax: 0161 426 5999
Text Relay: 18001 + 0161 426 9900
Website: www.stockportccg.org
Paul Fleming
Associate Director IM&T
Expectation
Reality

Connect: 21st Century Health & Social Care Informatics
Integrate: Integrated Digital Care Record linkage
Empower: Consistent, multi-channel public experience
Collaborate: Collective Health & Social Care Informatics
(HSCI) governance and delivery
Areas of work

Where did we start?
Not the most exciting place
GOVERNANCE
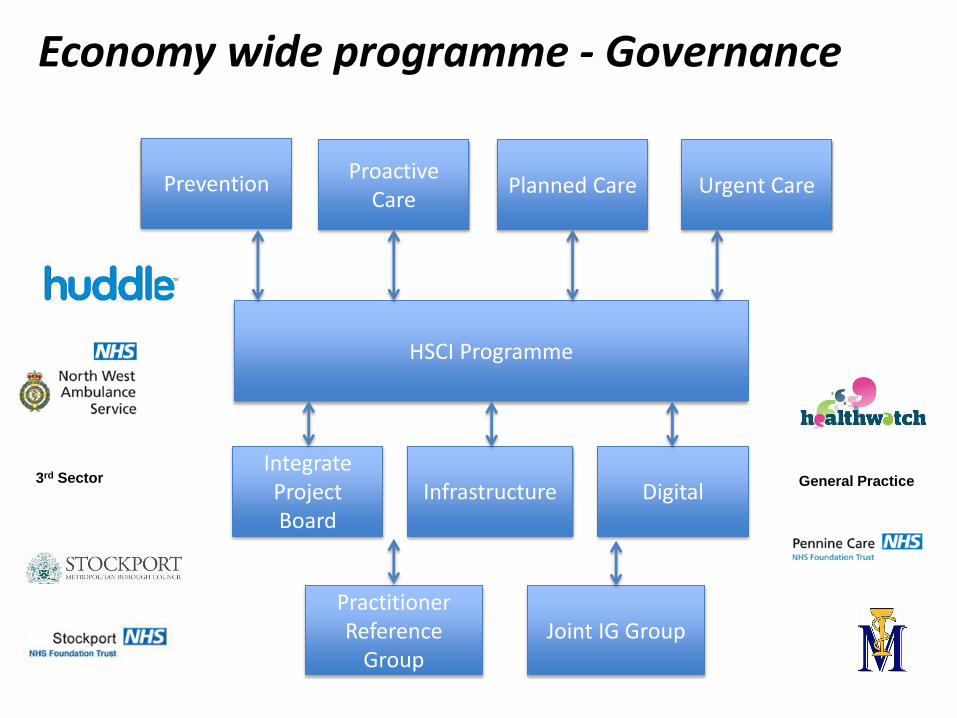
HSCI Programme
Proactive Care
Planned Care Urgent Care Prevention
Integrate Project Board
Digital
Joint IG Group
Economy wide programme - Governance
Infrastructure
Practitioner Reference
Group
3rd Sector General Practice
Connect
Physiological – Shelter warmth, food etc
Safety & security
Social needs
Esteem
Self - actualisation
WIFI
Connect

Connect
• Build on the Stockport network ‘logon anywhere’
• Standardise communications
systems – NHS Mail, Telephony etc • Provide infrastructure to enable
mobile working • Collaborate on intelligence
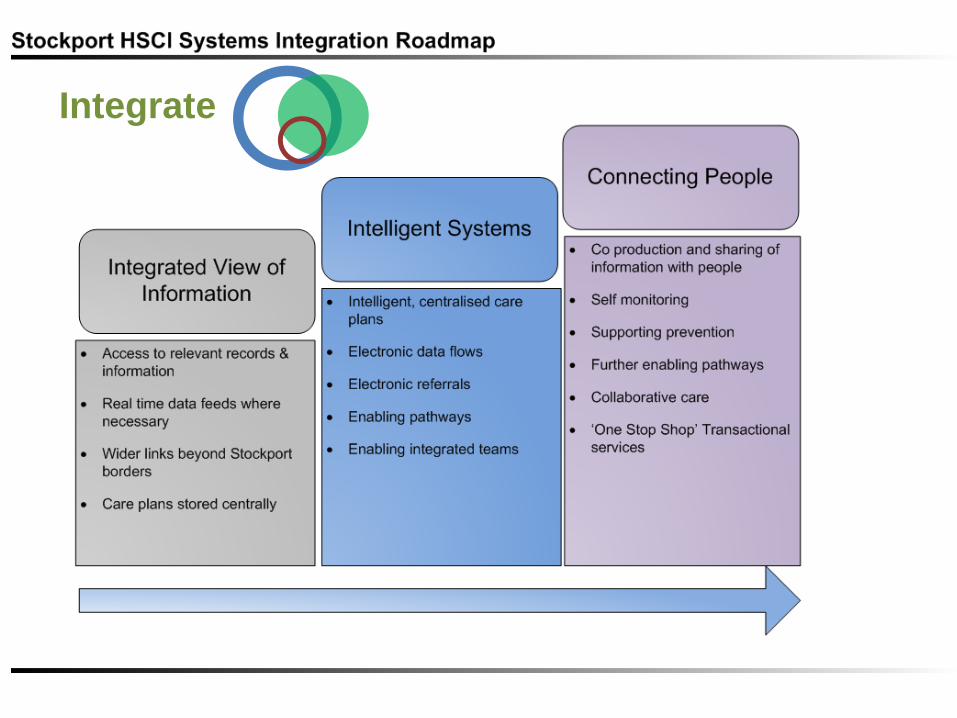
Integrate
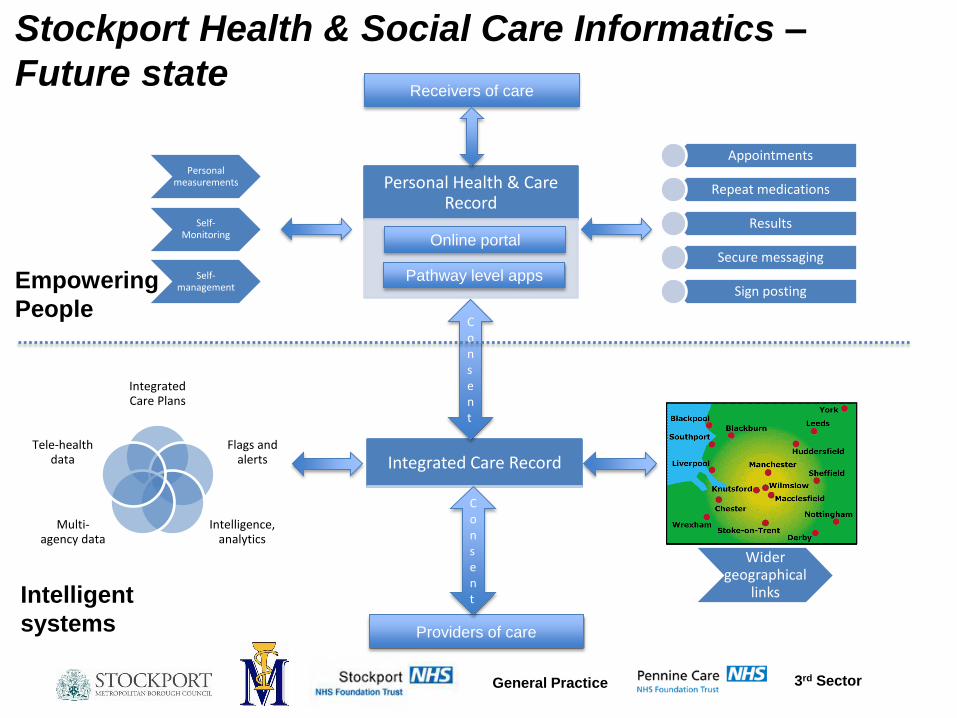
Personal Health & Care Record
Integrated Care Record
Consent
Appointments
Repeat medications
Results
Secure messaging
Sign posting
Personal measurements
Self- Monitoring
Self-management
Integrated Care Plans
Flags and alerts
Intelligence, analytics
Multi-agency data
Tele-health data
Wider geographical
links
Pathway level apps
General Practice 3rd Sector
Providers of care
Receivers of care
Stockport Health & Social Care Informatics –
Future state
Online portal
Intelligent
systems
Empowering
People
Consent
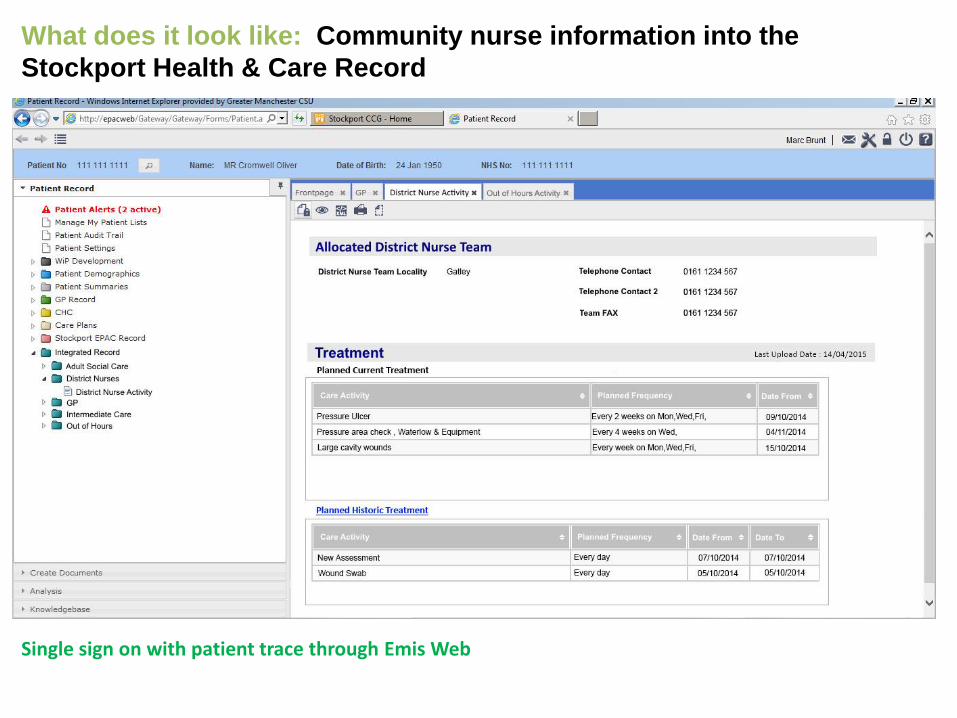
What does it look like: Community nurse information into the
Stockport Health & Care Record
Single sign on with patient trace through Emis Web
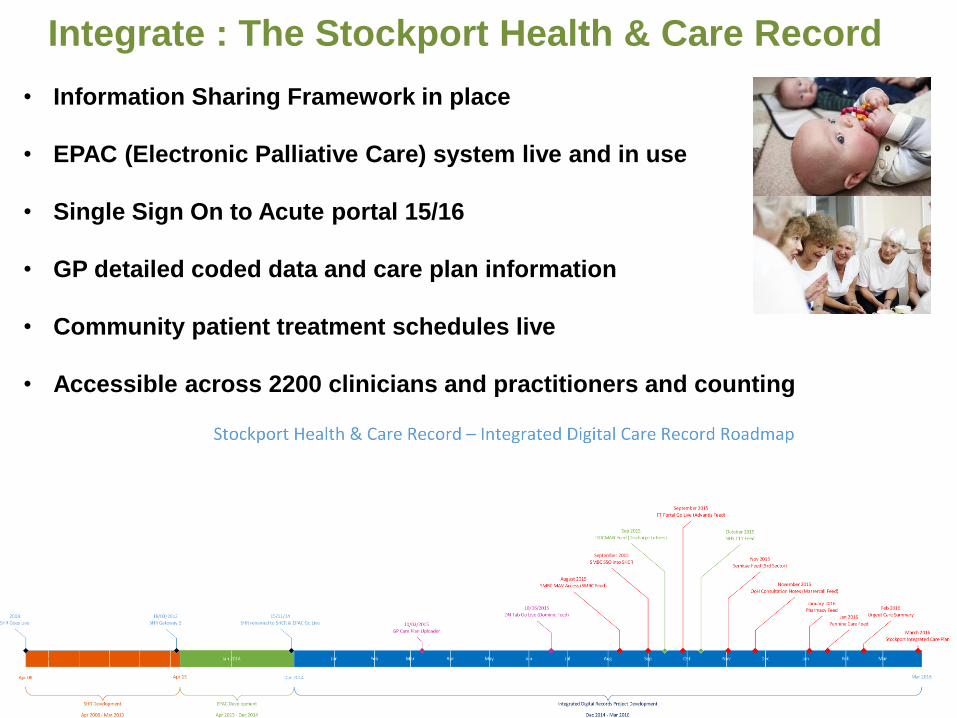
• Information Sharing Framework in place
• EPAC (Electronic Palliative Care) system live and in use
• Single Sign On to Acute portal 15/16
• GP detailed coded data and care plan information
• Community patient treatment schedules live
• Accessible across 2200 clinicians and practitioners and counting
Integrate : The Stockport Health & Care Record
Clinical Systems Single, Multiple, Consolidated?
• Direct Interoperability
• Integration products
• Single system
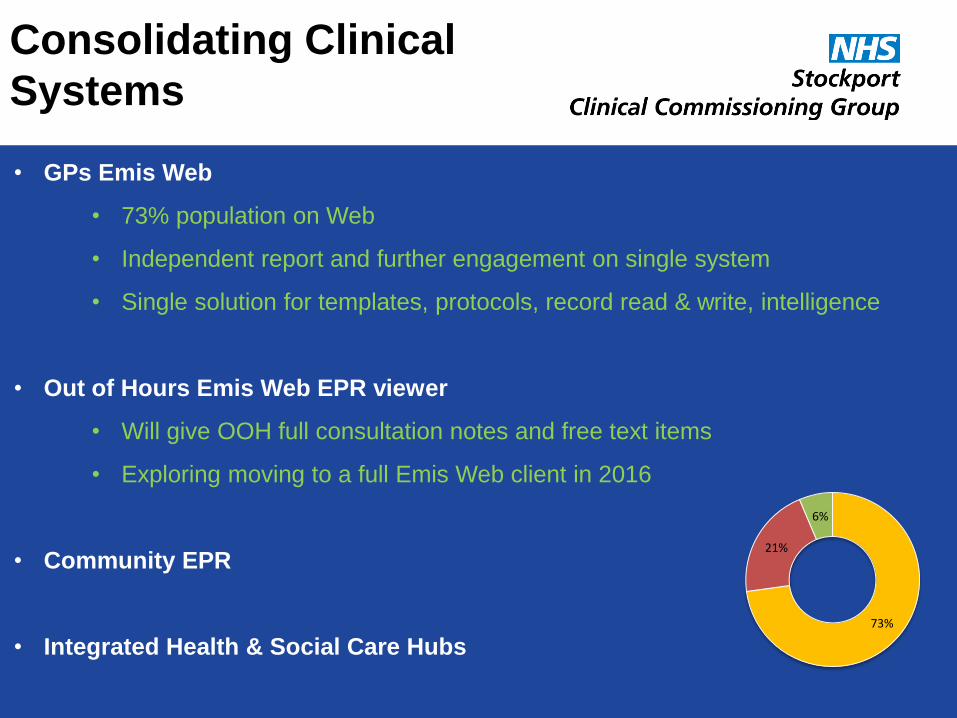
• GPs Emis Web
• 73% population on Web
• Independent report and further engagement on single system
• Single solution for templates, protocols, record read & write, intelligence
• Out of Hours Emis Web EPR viewer
• Will give OOH full consultation notes and free text items
• Exploring moving to a full Emis Web client in 2016
• Community EPR
• Integrated Health & Social Care Hubs
Consolidating Clinical
Systems
73%
21%
6%
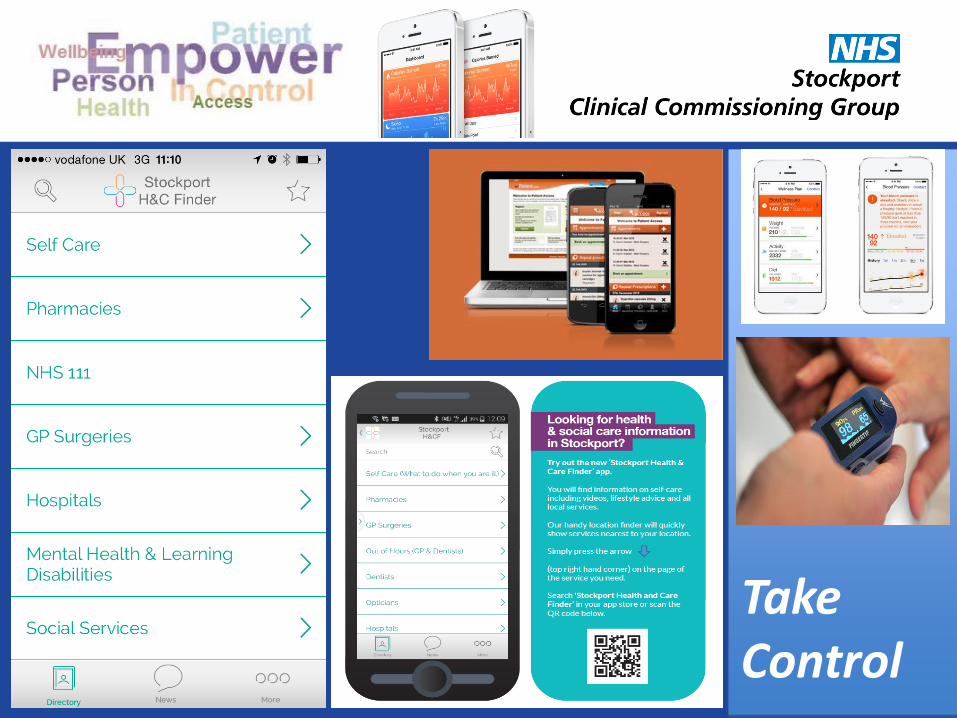
Take Control
What will it mean for People • Reduce duplication, people
not repeating information • Practitioners can access all
relevant information about a person
• Find the at risk people using
combined data • Empowered people accessing
and adding to their online records to take control
• Transactions with services are
online • Teams can work together
• Use apps and online content
to find local health & care services and information
(Central Lancashire Health Economy)
Jane Kitchen – Transformation Manager, CCGs
Kate Burgess - Locality Commissioning Manager,
Lancashire County Council
Jo Blofeld - Patient & Public Involvement Lead,
Lancashire Care NHS FT
Step up Step Down – Discharge to
Assess and Trusted Assessor
NHS Improving Quality and NHS England

Central Lancashire Health and Social Care –
Whole System Transformation Programme
Step Up Step Down
Patient story
Jo Blofeld – Patient and Carer Experience Lead
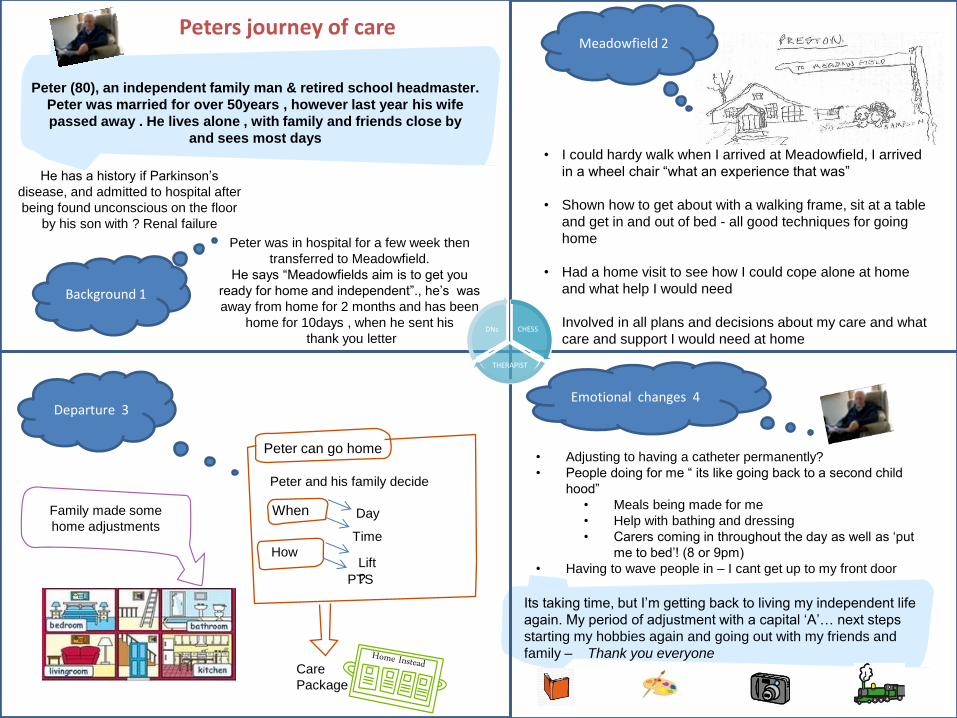
Peter was in hospital for a few week then
transferred to Meadowfield.
He says “Meadowfields aim is to get you
ready for home and independent”., he’s was
away from home for 2 months and has been
home for 10days , when he sent his
thank you letter
Peter (80), an independent family man & retired school headmaster.
Peter was married for over 50years , however last year his wife
passed away . He lives alone , with family and friends close by
and sees most days
He has a history if Parkinson’s
disease, and admitted to hospital after
being found unconscious on the floor
by his son with ? Renal failure
Peters journey of care
Background 1
Meadowfield 2
• I could hardy walk when I arrived at Meadowfield, I arrived
in a wheel chair “what an experience that was”
• Shown how to get about with a walking frame, sit at a table
and get in and out of bed - all good techniques for going
home
• Had a home visit to see how I could cope alone at home
and what help I would need
• Involved in all plans and decisions about my care and what
care and support I would need at home
Departure 3
Peter can go home
When
Peter and his family decide
How
Day
Time
Lift
? PTS
Care
Package
Family made some
home adjustments
Emotional changes 4
• Adjusting to having a catheter permanently?
• People doing for me “ its like going back to a second child
hood”
• Meals being made for me
• Help with bathing and dressing
• Carers coming in throughout the day as well as ‘put
me to bed’! (8 or 9pm)
• Having to wave people in – I cant get up to my front door
Its taking time, but I’m getting back to living my independent life
again. My period of adjustment with a capital ‘A’… next steps
starting my hobbies again and going out with my friends and
family – Thank you everyone
CHESS
THERAPIST
DNs
To the staff at Meadowfield, I wish to thank the staff at rehab Meadowfield for the care and attention given over the last few weeks. The patience and attention to detail have to be seen as well as experienced, when I arrived after kidney failure. I could hardly stand up – now I feel confident and able to readily lead a life suited to my age It has been a pleasure to be part of a constantly changing atmosphere at Meadowfield and the staff have shown great insight and practicality in helping to cultivate a cheerful and pleasant life whilst helping me pick up the threads of life again Thank you Peter Fox
https://www.youtube.com/watch?v=QOR1oUbnJLM
Panel of Presenters
Q & A
NHS Improving Quality and NHS England
Facilitated Workshop Session to discuss
NHS Improving Quality and NHS England
1. Local Challenges and Barriers
2. What enablers or support is needed to deliver 7 Day Services
Remember to complete your forms about the type of support you would find useful
Jo James
Programme Lead, NHSIQ
Summary, Next Steps and Close
NHS Improving Quality and NHS England

Lunch
& Market Place Networking
www.nhsiq.nhs.uk
http://www.7daysat.nhs.uk/
NHS Improving Quality and NHS England




























