Embed Size (px)
Citation preview

HIV - Diagnosis and Management
Guide: Dr.S.L. Mathur sirPresented by Dr.Sohanlal Sharma
Introduction• HIV, the etiological agent of AIDS, belongs to lentivirus subgroup of
the retroviridae family
• The first indication of this new syndrome came in 1981 in homosexual drug addict males in USA
• they had two things in common- Pneumocystis pneumonia and Kaposi’s sarcoma.
. Recently its origin has been traced to Kinishasa in CONGO.
• AIDS Pandemic is primarily caused by HIV-1M.

Routes of transmission
Diagnosis of AIDSWHO case definition for AIDS surveillance
Major signs:• Wt loss more than 10%
• Chronic diarrhea for more than one month.
• Fever more than one month.
Minor Signs:• .Persistent cough more than a month
• .Gen. pruritic dermatitis
• .History of herpes Zoster
• .Oropharyngeal Candidiasis
• . Gen lymphadenopathy
Laboratory Diagnosis of HIV infection
1) Non Specific Tests-
a) Total Leukocyte and lymphocyte
b) T cell subset.
c) Platelet count-
d) Lymph node biopsy

Laboratory Diagnosis of HIV infection
2.Specific Tests for HIV infection- These include demonstration of -
• HIV antigen,
• Antibodies,
• Viral nucleic acids or other components and
• Isolation of virus
2/7/2015 6Biochemistry for medics

Laboratory Diagnosis of HIV infection
i) Detection of antigen
o Following a contact, as by blood transfusion, the viral antigen may be detectable in blood after about 2 weeks.
o If the infecting dose is small, as following a needle stick injury, the process may be considerably delayed.
o The major core antigen p24 is the earliest virus marker to appear in blood.
2/7/2015 7Biochemistry for medics
Laboratory Diagnosis of HIV infection
• i) Detection of antigen (contd.)• Free p24 antigen disappears from circulation and
remains absent during the long asymptomatic phase to reappear only when severe clinical disease sets in.
• The p24 Capture ELISA assay, which uses anti p24 antibody as the solid phase can be used for this.
• This test is positive in about 30% of the infected persons.
• In the first few weeks after infection and in the terminal phase, the test is uniformly positive.
2/7/2015 8Biochemistry for medics

Laboratory Diagnosis of HIV infection
• Detection of antibodieso It takes 2-8 weeks to months for the antibodies to appear in
circulation
o IgM antibodies appear first, to be followed by IgG antibodies
o Once antibodies appear they increase in titer for the next several months
o IgM antibodies disappear in 8-10weeks while IgG antibodies remain through out.
2/7/2015 9Biochemistry for medics
Laboratory Diagnosis of HIV infection
• Detection of antibodies (contd.)• Screening tests and supplemental tests.
Screening tests include-
o ELISA- ELISA
o p24 Capture ELISA assay
2/7/2015 10Biochemistry for medics
Laboratory Diagnosis of HIV infection
ELISA
1) First generation - whole viral lysates
2) Second generation - recombinant antigen
3) Third generation - synthetic peptide
4) Fourth generation - antigen + antibody (Simultaneous detection of HIV antigen and antibody) - HIV duo
2/7/2015 11Biochemistry for medics
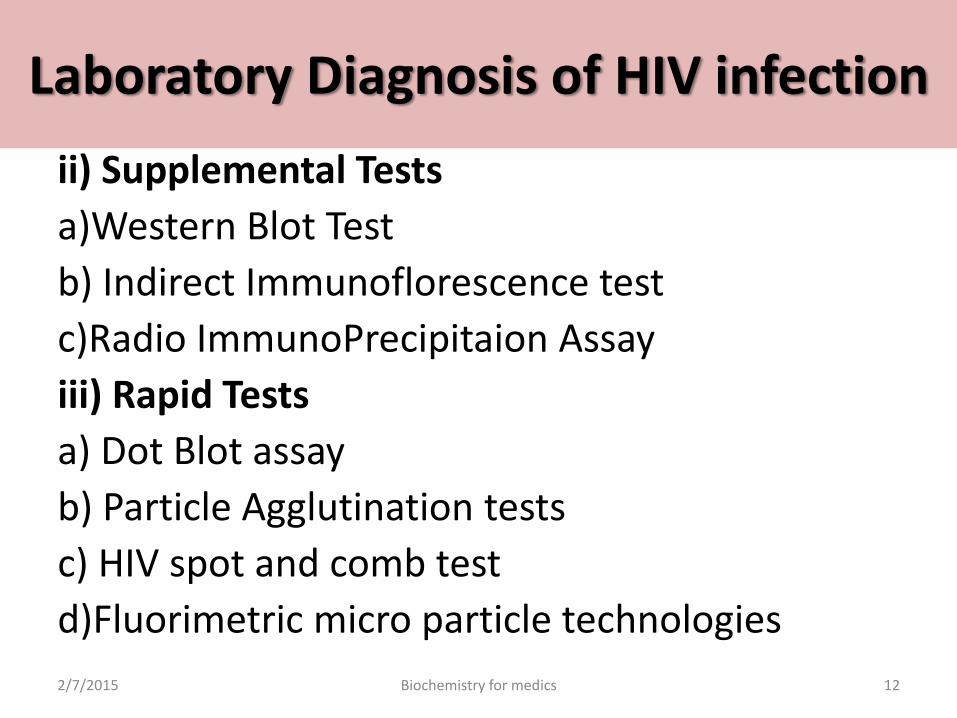
Laboratory Diagnosis of HIV infection
ii) Supplemental Tests
a)Western Blot Test
b) Indirect Immunoflorescence test
c)Radio ImmunoPrecipitaion Assay
iii) Rapid Tests
a) Dot Blot assay
b) Particle Agglutination tests
c) HIV spot and comb test
d)Fluorimetric micro particle technologies
2/7/2015 12Biochemistry for medics

Laboratory Diagnosis of HIV infection
• Three different techniques namely RT-PCR, nucleic acid sequence based amplification (NASBA) and branched-DNA (b-DNA) assay have been employed to develop commercial kits.
2/7/2015 Biochemistry for medics 13

Who to test When to test
Pregnant women andmale partners
At first antenatal care visitRe-test in third trimester or peripartumOffer partner testing
Infants and children <18 months old
At 4–6 weeks for all whose mothers are HIV Positive or status uncertain; Final status after 18 months and/or when breastfeeding ends
ChildrenEstablish HIV status for all health contacts Tell their HIV status & parents or caregiver’s status
AdolescentsIntegrate into all health care encounters.Annually if sexually active; with new sexual partners
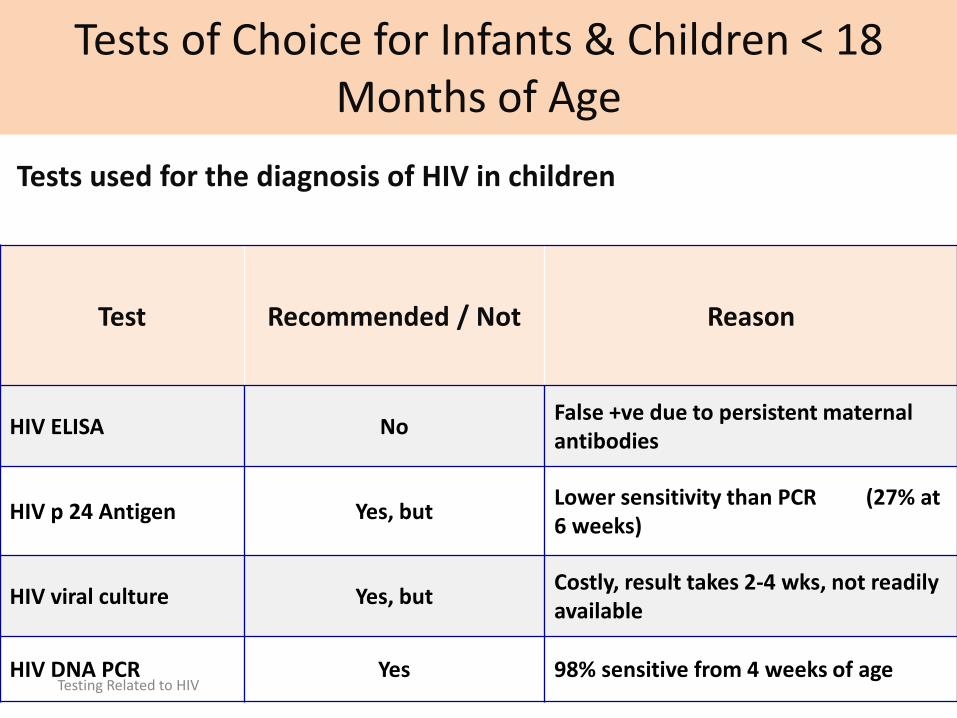
Tests of Choice for Infants & Children < 18 Months of Age
Tests used for the diagnosis of HIV in children
Test Recommended / Not Reason
HIV ELISA NoFalse +ve due to persistent maternal antibodies
HIV p 24 Antigen Yes, butLower sensitivity than PCR (27% at 6 weeks)
HIV viral culture Yes, butCostly, result takes 2-4 wks, not readily available
HIV DNA PCR Yes 98% sensitive from 4 weeks of ageTesting Related to HIV
Clinical Manifestations
• AIDS is only the last stage in the wide spectrum of clinical features in HIV infection.
• The center for disease control (USA) has classified the clinical course of HIV infection under various groups.
• Acute HIV infection• Asymptomatic or Latent infection• Persistent generalized lymphadenopathy (PGL)• AIDS related complex• Full blown AIDS (Last stage)
2/7/2015 16Biochemistry for medics
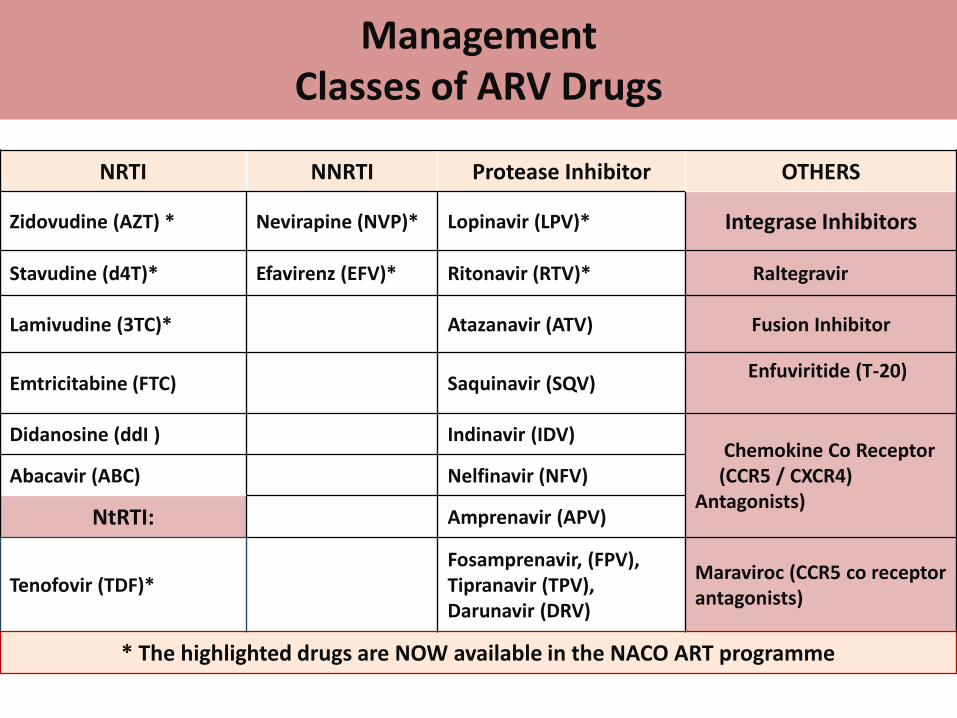
NRTI NNRTI Protease Inhibitor OTHERS
Zidovudine (AZT) * Nevirapine (NVP)* Lopinavir (LPV)* Integrase Inhibitors
Stavudine (d4T)* Efavirenz (EFV)* Ritonavir (RTV)* Raltegravir
Lamivudine (3TC)* Atazanavir (ATV) Fusion Inhibitor
Emtricitabine (FTC) Saquinavir (SQV) Enfuviritide (T-20)
Didanosine (ddI ) Indinavir (IDV) Chemokine Co Receptor(CCR5 / CXCR4)
Antagonists)Abacavir (ABC) Nelfinavir (NFV)
NtRTI: Amprenavir (APV)
Tenofovir (TDF)*Fosamprenavir, (FPV), Tipranavir (TPV), Darunavir (DRV)
Maraviroc (CCR5 co receptor antagonists)
* The highlighted drugs are NOW available in the NACO ART programme
ManagementClasses of ARV Drugs

RT
Provirus
ProteinsRNA
DNA
RNA
DNA
DNA
RT
RNA
RNA
DNA
DNA
DNA
Viral regulatoryproteins
Viral protease
Reversetranscriptase
Viral integraseIntegrase Inhibitor
Mechanism of Drug Action
ProteaseInhibitorsLopinavirRitonavir
Reversetranscriptase
Zidovudine
Stavudine
Lamivudine
Nevirapine
Efavirenz
FusionInhibitor
ARV Clinical Pharmacology

Indication of ART
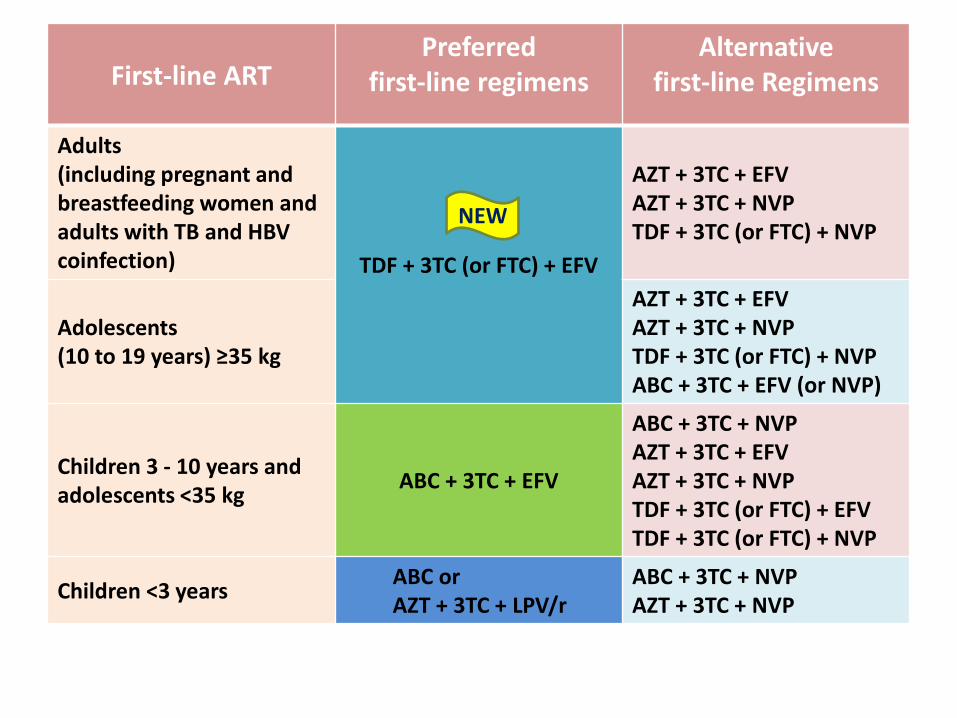
First-line ARTPreferred
first-line regimensAlternative
first-line Regimens
Adults(including pregnant andbreastfeeding women and adults with TB and HBV coinfection) TDF + 3TC (or FTC) + EFV
AZT + 3TC + EFVAZT + 3TC + NVPTDF + 3TC (or FTC) + NVP
Adolescents (10 to 19 years) ≥35 kg
AZT + 3TC + EFVAZT + 3TC + NVPTDF + 3TC (or FTC) + NVPABC + 3TC + EFV (or NVP)
Children 3 - 10 years and adolescents <35 kg
ABC + 3TC + EFV
ABC + 3TC + NVPAZT + 3TC + EFVAZT + 3TC + NVPTDF + 3TC (or FTC) + EFVTDF + 3TC (or FTC) + NVP
Children <3 yearsABC orAZT + 3TC + LPV/r
ABC + 3TC + NVPAZT + 3TC + NVP
NEW

Association between OIs & CD4 Count
Approach to OIs
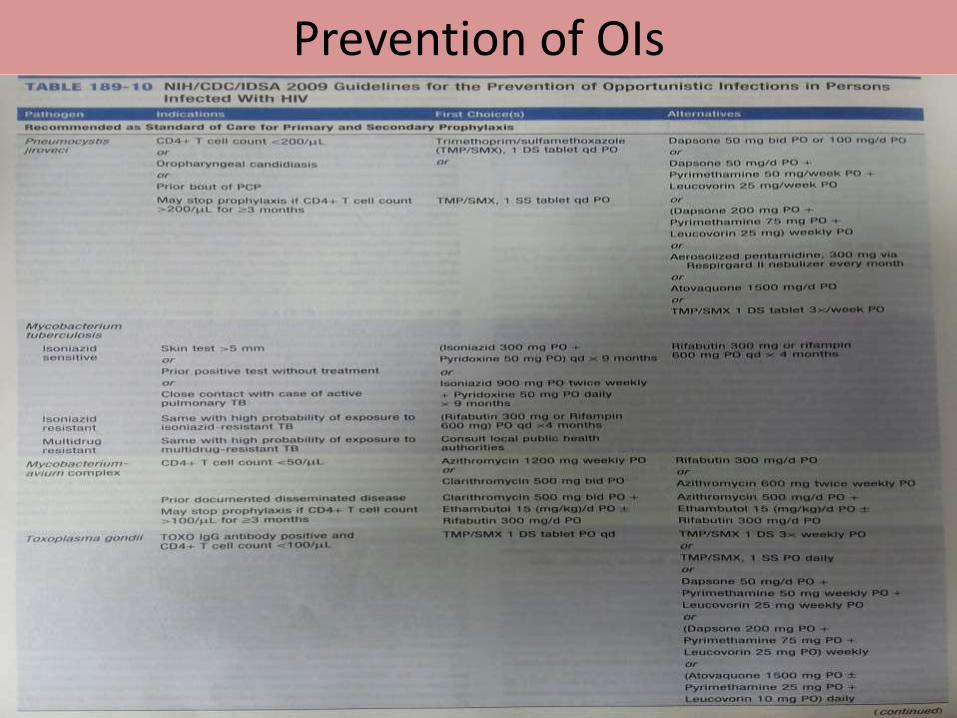
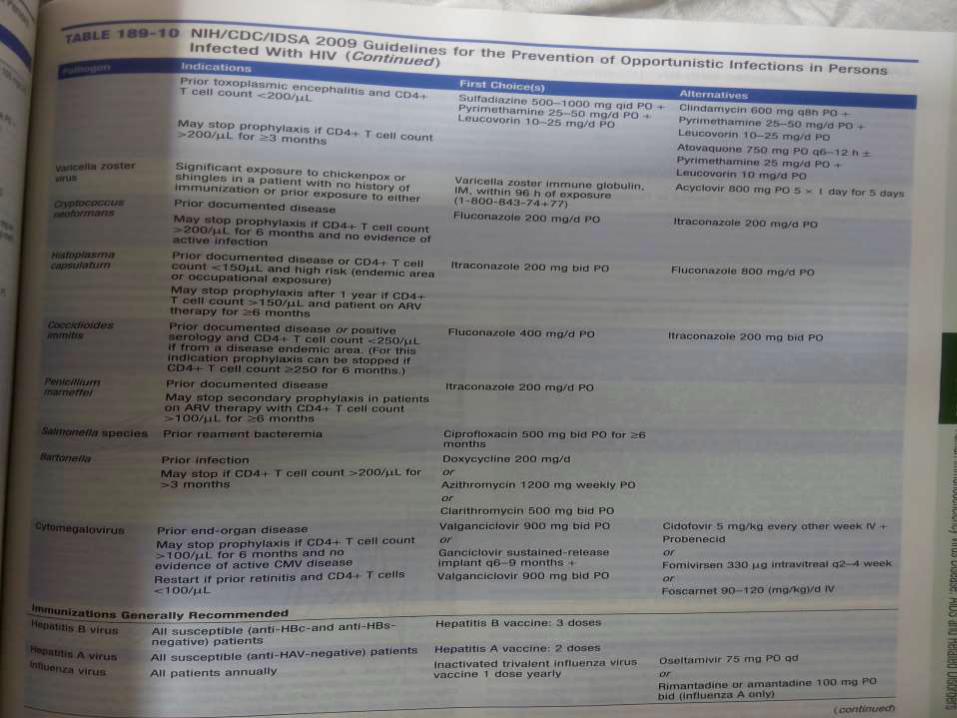
Prevention of OIs
Timing of ART with TB
• ART should be started in all TB patients, including drug-resistant TB,irrespective of the CD4 count
• AKT should be initiated first, followed by ART as soon as possiblewithin the first 8 weeks of treatment.
• HIV-positive TB patients with profound immunosuppression (CD4<50) should receive ART immediately within the first 2 weeks of AKT .
• ART should be started in any child with active TB disease as soon aspossible and within 8 weeks After the initiation of AKT irrespective ofthe CD4 and clinical stage.
• Preferred NNRTI is EFV in patients starting ART while on AKT .

Timing of ART with Cryptococcal meningitis
• Immediate ART not recommended in cryptococcal meningitis due to the high risk of IRIS with CNS disease, which may be life-threatening .
• Among PLHIV with a recent cryptococcal meningitis,
– ART initiation should be deferred until there is evidence of a sustained clinical response to antifungal therapy and
– after two to four weeks of induction and consolidation treatment with amphotericin containing regimens combined with flucytosine or fluconazole; or