Embed Size (px)
Citation preview

SEIZURE
DISORDERSBY- SAMPURNA DAS
WHAT IS SEIZURES
Seizures are discrete, time-limited alterations in brain function - including changes in motor activity, autonomic function, consciousness, or sensation -that result from an abnormal and excessive electrical discharge of a group of neurons within the brain.

CAUSES• Genetic influence• Head trauma• Brain conditions• Infectious diseases• Prenatal injury• Developmental disorders
RISK FACTORS• Age• Family history• Stroke• Other vascular diseases• Dementia• Seizures in childhood.
PATHOPHYSIOLOGY Seizure producing stimuli(trauma,high
fever,brain injury)
a small group of abnormal neurons undergo prolonged depolarizations associated with the rapid firing of repeated action potentials.
These abnormally discharging epileptic neurons recruit adjacent neurons or neurons with which they are connected into the process
PATHOPHYSIOLOGY (CONT.)
the electrical discharges of a large number of cells become abnormally linked together
creating a storm of electrical activity in the brain
Seizures may spread to involve adjacent areas of the brain or through established anatomic pathways to other distant areas
GENERALIZED SEIZURES
• 1. Generalized Tonic-Clonic
(Grand Mal)• 2. Absence (Petit Mal)• 3 Atypical Absence• 4. Atonic seizures• 5. Myoclonic Seizure• 6. Tonic seizures
PARTIAL SEIZURES
SIMPLE PARTIAL
• a. Motor seizures • d. Sensory seizures • e. Autonomic seizures • f. Psychic seizures
COMPLEX PARTIAL
• . Impairment of consciousness
• b. Associated with initial aura
• c. Simple to complex automatisms
OTHERS• Partial Seizures Secondarily Generalized • Selected Epileptic Syndromes
A. Infantile Spasms
B. Febrile Seizure
C. Lennox-Gastaut Syndrome
D. Benign Rolandic epilepsy
E. Juvenile myoclonic epilepsy
PHASES OF CONVULSION (1)PRODROMAL PHASE WITH SIGNS OR ACTIVITY WHICH PRECEDE A SEIZURE;
(2)AURAL PHASE, WITH A SENSORY WARNING;
(3)ICTAL PHASE WITH FULL SEIZURE;
(4) POSTICTAL PHASE WHICH IS THE PERIOD OF RECOVERY AFTER THE SEIZURE.
GENERALIZED TONIC-CLONIC SEIZURE• Loss of consciousness is quickly followed by a
sudden fall to ground. • In the tonic phase, muscles become rigid and
the simultaneous contractions of diaphragm and chest muscles may produce the characteristic "epileptic cry".
• The patient's eyes roll up or turn to the side and the tongue may be bitten.
• The rigidity is replaced shortly by series of synchronous clonic movements of head, face, legs and arms.
GENERALIZED TONIC-CLONIC SEIZURE
• Autonomic changes also observed included: increased blood pressure,increased heart rate, and bladder pressure; pupillary mydriasis; hypersecretion of skin and salivary glands; cyanosis of skin.
• Average duration 2 to 5 minutes.• Postictally, patients lethargic/sleepy lasting
several minutes to hours.• Incontinence seen in early postictal phase

ABSENCE SEIZURE• Onset between 4 and 14 years and
often resolve by age 18.• Brief episodes of staring with
impairment of awareness and responsive that begin without warning and end suddenly, leaving patient alert and attentive.
• In simple absence seizures, patient only stares.
Atypical Absence:• Onset between 1 to 7 years of age• similar to typical absence except that loss of
responsiveness during seizure is often less complete and more gradual in onset and cessation; Also clonic, tonic and atonic components (i.e., increase or decreases in muscle tone) are more pronounced than in typical absence
• EEG findings: slow spike and wave (< 2.5 Hz) discharge and/or incompletely generalized spike-waves
ATONIC SEIZURE
• In the more common complex absence seizures, staring is accompanied by simple automatic movements such as blinking of eyes, drooping of head, or chewing.
• Duration - short (10-45 secs), patients usually unaware of occurrence.
• Abrupt recovery without after effects
Myoclonic Seizure• Sudden, brief shock-like jerk of a
muscle or group of muscles, often occurs in healthy people as they fall asleep.
• Epileptic myoclonus usually causes synchronous and bilateral jerks of the neck, shoulders, upper arms, body, and upper legs.
Tonic seizures• Characterized by sudden bilateral
stiffening of the body, arms, or legs. Tonic seizures usually last less than 20 seconds and are more common during sleep.
• Primarily seen in younger children; commonly associated with metabolic disorder or underlying neurological deficit
• Duration 10-60 seconds; brief, if any, postictal symptoms
SIMPLE PARTIAL SEIZURES
• a. No loss of consciousness;• b. Motor seizures :• c. Sensory seizures:• d. Autonomic seizures:• e. Psychic seizures:
Complex partial seizures (temporal lobe, psychomotor epilepsy)
• A. IMPAIRMENT OF CONSCIOUSNESS OBSERVED:
• Patients may appear to be conscious, closer examination shows that they are unaware of their environment
• fail to respond or respond inappropriately to questions
• are unable to remember the seizure episode.
• B. ASSOCIATED WITH INITIAL AURA (I.E., SIMPLE PARTIAL SEIZURE) IN >50% OF PATIENTS
• The aura is a simple partial seizure which may then progress to a complex partial (and/or generalized tonic-clonic) seizure. Most common forms of aura: fear, rising epigastric sensation, unilateral "funny feeling" or "numbness", or visual disturbances; focal twitching of face or fingers.
C. SIMPLE TO COMPLEX AUTOMATISMS (REPETITIVE MOTOR ACTIVITY THAT IS PURPOSELESS, UNDIRECTED, AND INAPPROPRIATE)
• They are frequently observed during complex partial seizures. Examples include repetitive chewing or swallowing, lip smacking, fumbling movements of fingers or hands, picking at clothing, mumbling, moving about aimlessly, purposeless behavior, and clumsy perseverance of a preceding motor act.
• Average duration 1 to 3 minutes• Postictal phase - confusion, lethargy,
altered behaviour, amnesic for event
3. PARTIAL SEIZURES SECONDARILY GENERALIZED –
• partial seizure may progress through several stages reflecting spread of discharge to different brain areas. For example, seizure may begin as simple partial (i.e., aura), progress to complex partial and subsequently become secondarily generalized (tonic-clonic).
4. Selected Epileptic Syndromes-
A. Infantile Spasms• Consist of sudden flexion of the head
with abduction and extension of arms, accompanied by flexion of knees and often a little grunt or cry. Spasms may also be extension rather than flexion..
• Onset -between 4 to 7 months of age
• Characterized by spasms, developmental retardation.
• Spasms may be flexor (jackknife), extensor or mixed flexor-extensor.
• spasms usually disappear by age 3 or 4, but child left profoundly handicapped, retarded, and often with Lennox-Gaustaut syndrome
• B. Febrile Seizures
• Convulsions that occur with fever (> 38oC) in children between 6 months and 6 years of age, not secondary to an infection of brain or meninges.
• Prevalence: 2 to 5% of all children will have a febrile seizure before 6 y/o; Peak incidence at 2 years of age.
• Intellectual dysfunction and neurologic sequelae may occur following febrile status epilepticus.
• C. Lennox-Gastaut Syndrome: • This syndrome is characterized by the triad
of intractable seizures, mental and developmental retardation, and slow spike and wave pattern on the EEG.
• begin between ages 1 and 6 years • respond poorly to antiepileptic drugs. • Behavioral problems are common • Probably result from the underlying
neurologic injury, effects of frequent seizures and head injuries, and high-dose combinations of antiepileptic drugs.
• D. Benign Rolandic epilepsy:
• This syndrome frequently begins in children with a family history of epilepsy.
• Characteristic sign is a partial motor or somatosensory seizure involving the face.
• Tonic-clonic seizures may also occur, especially during sleep.
• The seizures are infrequent (some patients require no medications), are easily controlled with antiepileptic drug therapy, and stop spontaneously by age 15.
• E. Juvenile myoclonic epilepsy:
• These myoclonic seizures, with or without tonic-clonic or absence seizures, usually begin shortly before or after puberty but may first occur in early adulthood.
• Mental developemnt is normal.
COMPLICATION:
• Physical Injuries from Epilepsy• Status Epilepticus• Sudden Unexplained Death in Epilepsy• Eclampsia• Social Challenges• Anxiety
WHAT IS STATUS EPILEPTICUS?
Status epilepticus (acute prolonged seizure activity) is a series of generalised that occur without full recovery of consciousness between attack.The term has been broadened to include clinical or electrical seizure lasting at least 30 minutes,even without impairment of consciousness.
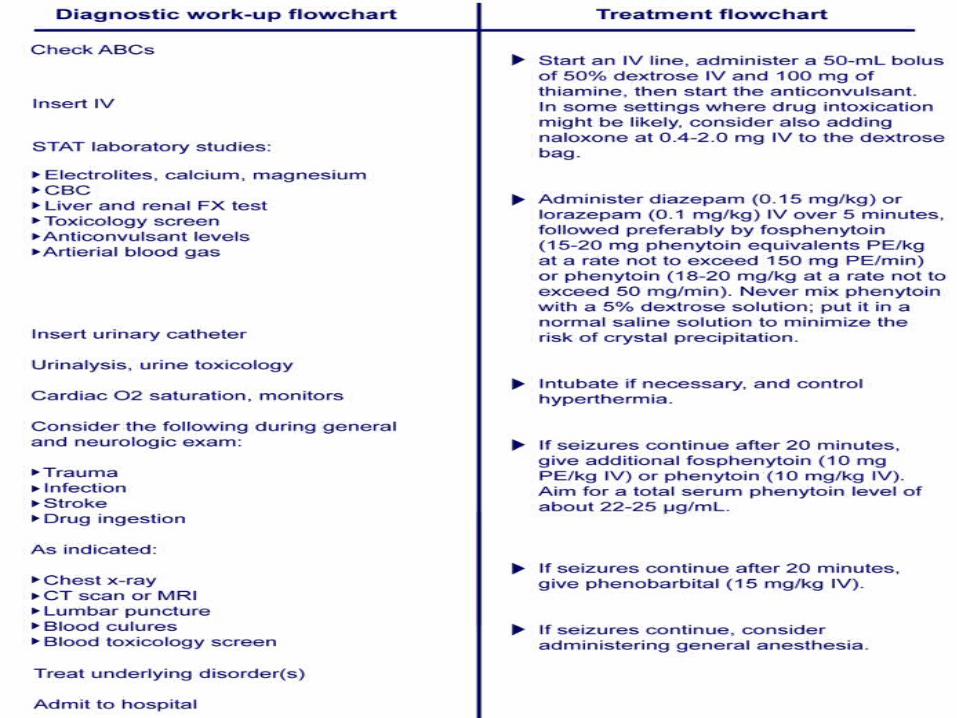
TREATMENT
• DIAZEPAM
• PHENYTOIN
• PHENOBARBITOL
• GENERAL ANAESTHESIA

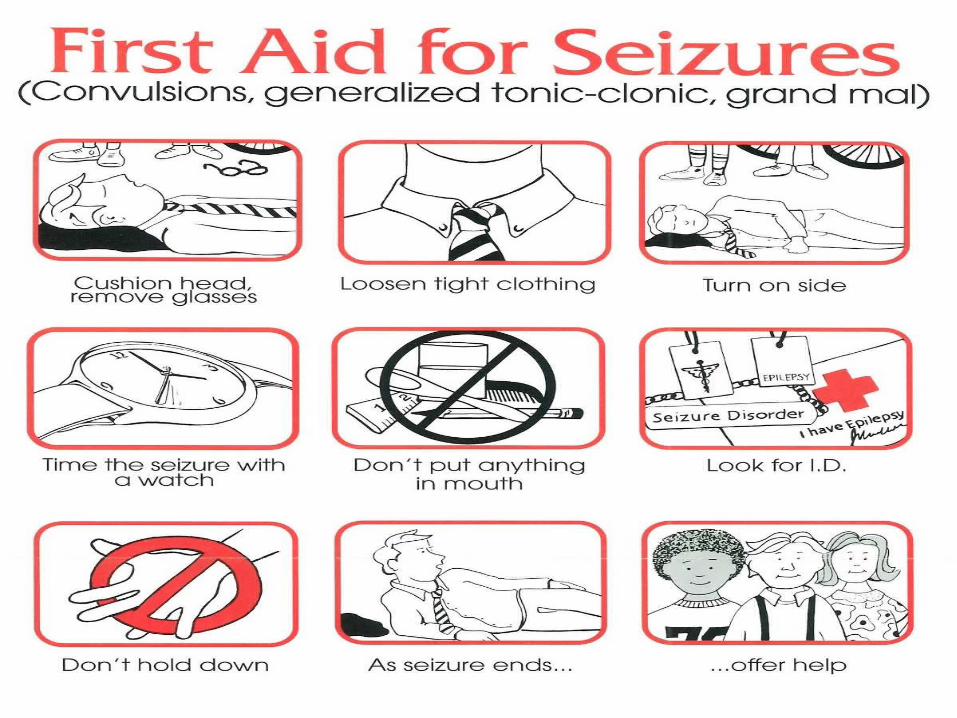
FIRST AID
DIAGNOSTIC STUDIES
• 1. HISTORY
• 2. PHYSICAL EXAMINATION
• 3. NEUROLOGICAL EXAMINATION• 4.BLOOD TESTS
• 5.ELECTROENCEPHALOGRAM

6.CT SCAN
7.MAGNETIC RESONANCE IMAGING
8.FUNCTIONAL MRI (FMRI)
9.POSITRON EMISSION TOMOGRAPHY
10.SINGLE-PHOTON EMISSION COMPUTERIZED TOMOGRAPHY
11.NEUROPSYCHOLOGICAL TESTS
MEDICAL MANAGEMENT
ANTI-EPILEPTIC DRUG (AED)• A drug which decreases the frequency
and/or severity of seizures in people with epilepsy
• Treats the symptom of seizures, not the underlying epileptic condition
• Goal: maximize quality of life by minimizing seizures and adverse drug effects
• Currently no “anti-epileptogenic” drugs available
Choosing the right AED
Seizure type
Epilepsy syndrome
Pharmacokinetic profile
Interactions/other medical conditions
Efficacy
Expected adverse effects
Cost
Classification of AEDsClassical
• Phenytoin• Phenobarbital• Primidone• Carbamazepine• Ethosuximide• Valproate
(valproic acid)• Trimethadione
(not currently in use)
Newer• Lamotrigine• Felbamate• Topiramate• Gabapentin/
Pregabalin• Tiagabine• Vigabatrin• Oxycarbazepine• Levetiracetam• Fosphenytoin
Targets for AEDs
• Increase inhibitory neurotransmitter system—GABA
• Decrease excitatory neurotransmitter system—glutamate
• Block voltage-gated inward positive currents—Na+ or Ca++
• Increase outward positive current—K+
• Many AEDs pleiotropic—act via multiple mechanisms
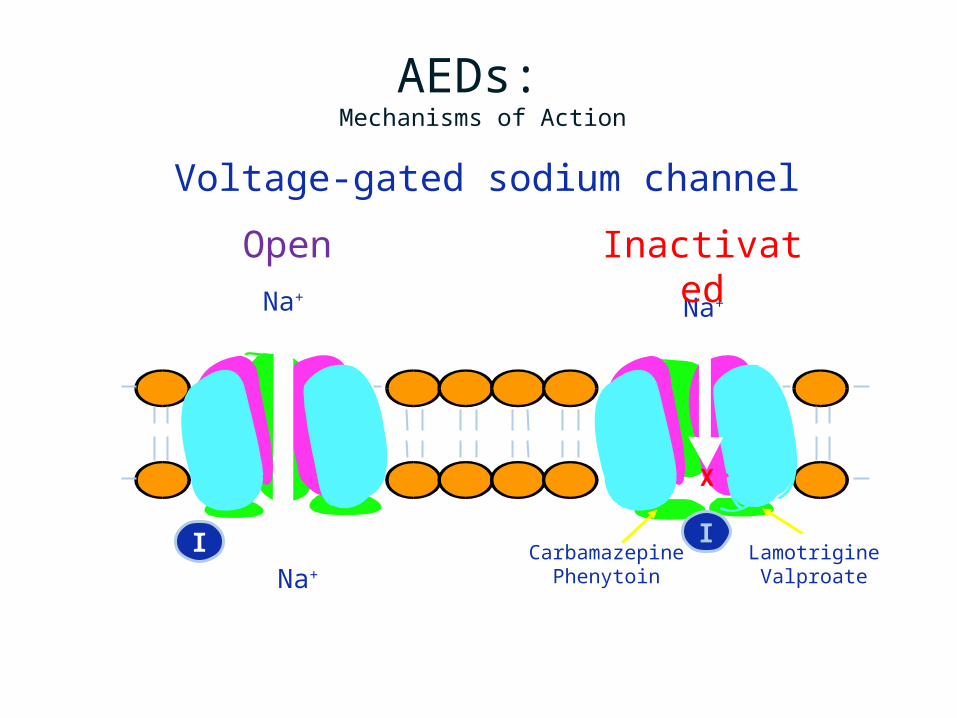
A = activation gateI = inactivation gate
McNamara JO. Goodman & Gilman’s. 9th ed. 1996:461-486.
AEDs: Mechanisms of Action
Na+ Na+
CarbamazepinePhenytoin
LamotrigineValproateNa+ Na+
I I
Voltage-gated sodium channel
Open Inactivated
X
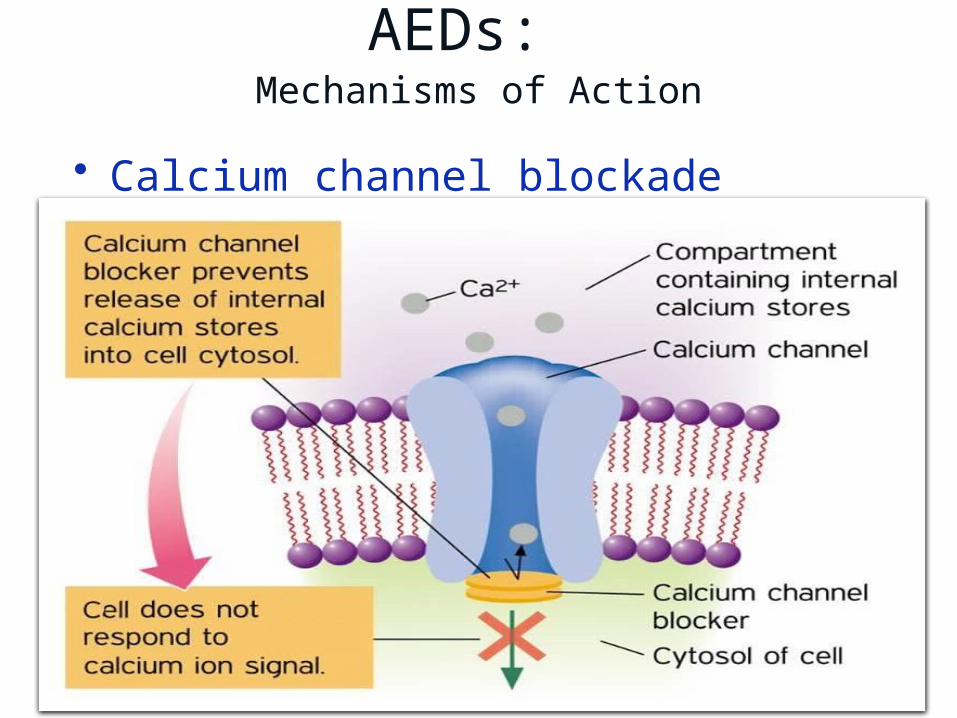
AEDs: Mechanisms of Action
• Calcium channel blockade
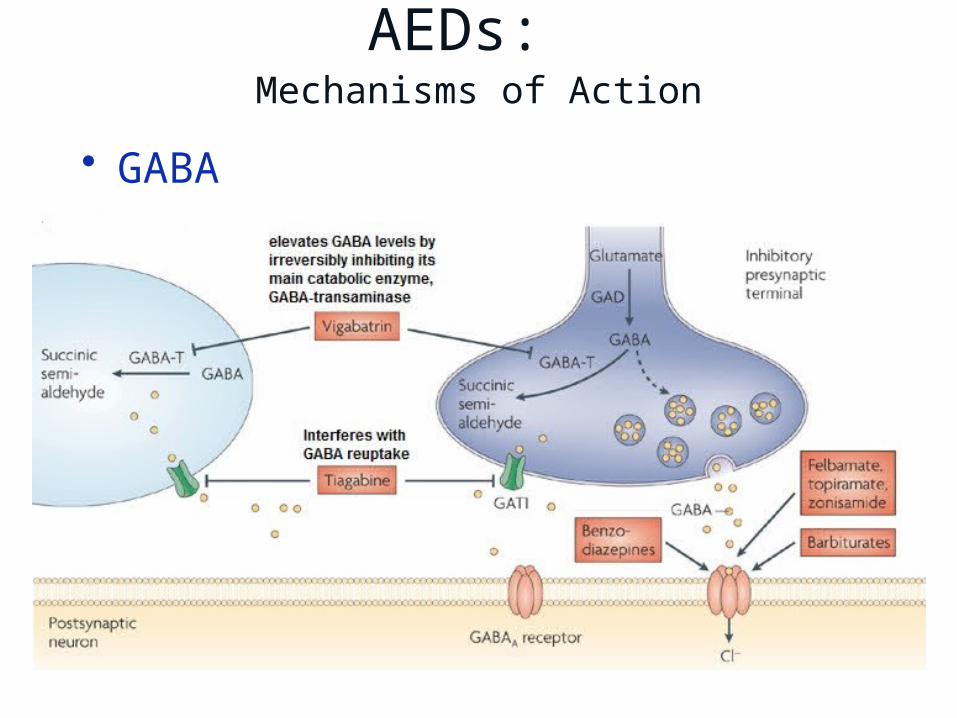
AEDs: Mechanisms of Action
• GABA

Side effect issues
• Sedation - especially with barbiturates• Cosmetic - phenytoin• Weight gain – valproic acid, gabapentin• Weight loss - topiramate• Reproductive function – valproic acid• Cognitive - topiramate• Behavioral – felbamate, leviteracetam• Allergic - many
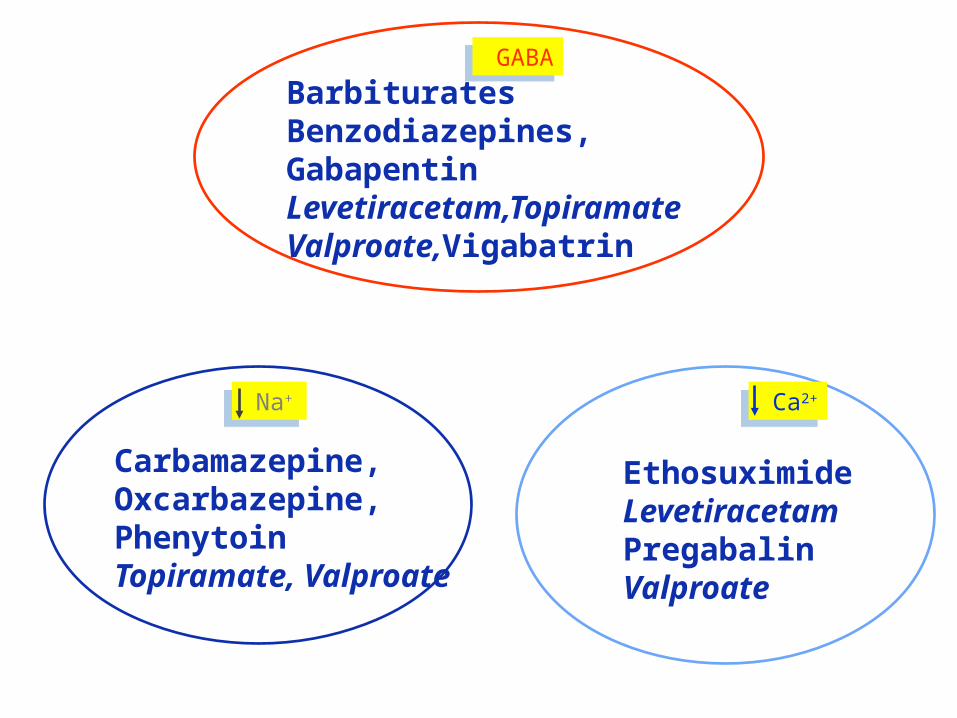
Carbamazepine,Oxcarbazepine, PhenytoinTopiramate, Valproate
EthosuximideLevetiracetamPregabalinValproate
BarbituratesBenzodiazepines, GabapentinLevetiracetam,TopiramateValproate,Vigabatrin
Na+ Na+ Ca2+ Ca2+
GABA GABA
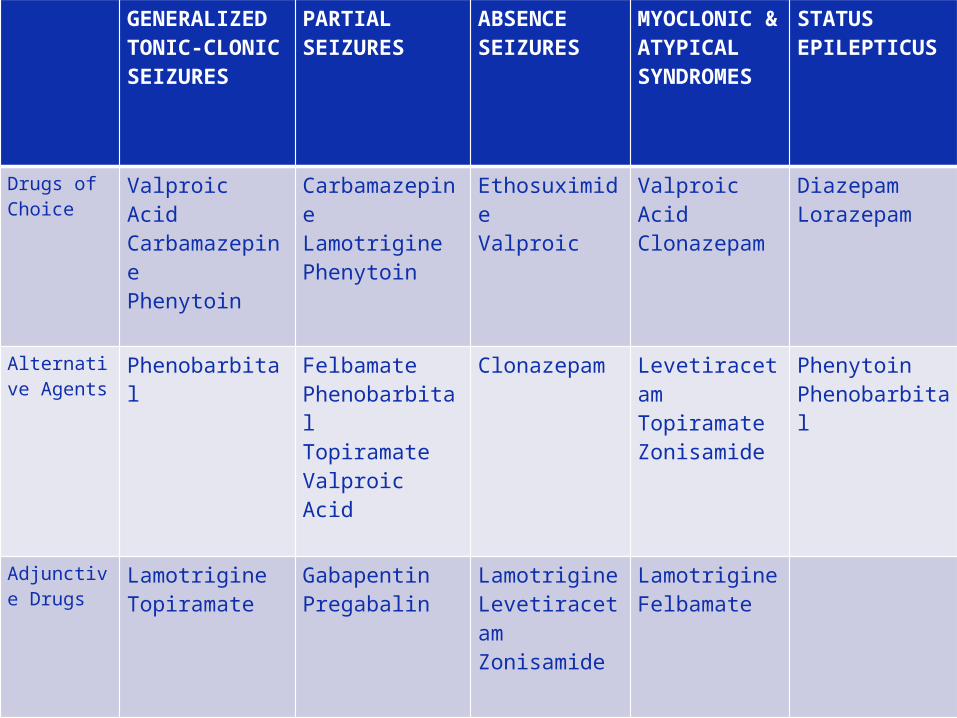
GENERALIZED TONIC-CLONIC SEIZURES
PARTIAL SEIZURES
ABSENCE SEIZURES
MYOCLONIC & ATYPICAL SYNDROMES
STATUS EPILEPTICUS
Drugs of Choice
Valproic AcidCarbamazepinePhenytoin
CarbamazepineLamotriginePhenytoin
EthosuximideValproic
Valproic AcidClonazepam
DiazepamLorazepam
Alternative Agents
Phenobarbital FelbamatePhenobarbitalTopiramateValproic Acid
Clonazepam LevetiracetamTopiramateZonisamide
PhenytoinPhenobarbital
Adjunctive Drugs
LamotrigineTopiramate
GabapentinPregabalin
LamotrigineLevetiracetamZonisamide
LamotrigineFelbamate
Other Clinical Uses
Valproic acid –maniaCarbamazepine, Lamotrigine –
bipolar disorderCarbamazepine –trigeminal
neuralgiaGabapentin –pain of neuropathic
originTopiramate –migrainePregabalin –neuropathic pain
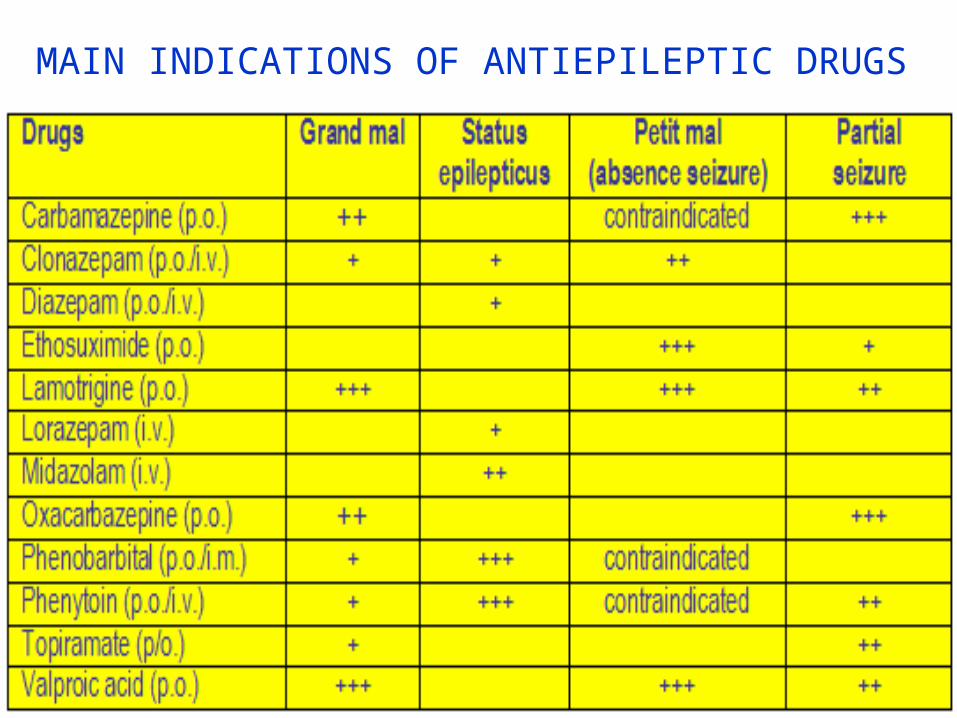
MAIN INDICATIONS OF ANTIEPILEPTIC DRUGS
TOXICITY
• Teratogenicity• Overdosage Toxicity• Life-Threatening Toxicity
Teratogenicity
Valproic acid –neural tube defectsCarbamazepine –craniofacial
anomalies, spina bifidaPhenytoin –fetal hydantoin syndrome

Overdosage Toxicity
• Respiratory depression
Management: supportive Airway management Mechanical ventilation
Life-Threatening Toxicity
Valproic acid –fatal hepatoxicityLamotrigine –Stevens-Johnson
syndromeZonisamide –severe skin reactionsFelbamate –aplastic anemia, acute
hepatic failure

NON PHARMACOLOGICALMANAGEMENT
KETOGENIC / LOW CARBOHYDATE DIET
VAGAL NERVE STIMULATION (VNS)

SURGICAL MANAGEMENT

• Temporal lobe resection• Lesionectomy• Functional Hemispherectomy• Corpus Callosotomy• Extratemporal Cortical Resection
ACTIVITY MODIFICATION AND
RESTRICTIONS
DO WITH PRECAUTION------
•DRIVING
•ASCENDING HEIGHTS
•WORKING WITH FIRE OR COOKING
•USING POWER TOOLS
•DANGEROUS ITEMS
•TAKING UNSUPERVISED BATHS
•SWIMMING

NURSING MANAGEMENT
ASSESSMENT:
• HISTORY, INCLUDING PRENATAL, BIRTH, AND DEVELOPMENTALHISTORY, FAMILY HISTORY, AGE AT SEIZURE ONSET, HISTORY OF ALL ILLNESS AND TRAUMAS.
•DETERMINE WHETHER THE PATIENT HAS AN AURA BEFORE AN EPILEPTIC SEIZURE, WHICH MAY INDICATE THE ORIGIN OF SEIZURE.
•OBSERVE AND ASSESS NEUROLOGICAL CONDITION.
•ASSESS VITALS AND NEUROLOGICAL SIGNS CONTINUOUSLY.
•ASSESS EFFECT OF EPILEPSY ON LIFESTYLE.
NURSING DIAGNOSIS1. Risk for trauma2. Risk for suffocation3. Risk for Ineffective Airway
Clearance4. Risk for Ineffective Breathing
Pattern5. Low Self-Esteem related to Stigmaassociated with condition perception
of beingout of control6. Knowledge Deficit related to lack
of exposure, unfamiliaritywith resources Information
misinterpretation lack of recall;cognitive limitation

NURSING MANAGEMENT































