Saskatchewan Seniors Oral Health and Long Term Care Strategy
86
Saskatchewan Seniors’ Oral Health and Long Term Care Strategy Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan Saskatchewan Oral Health Coalition October 24, 2016
Saskatchewan Seniors Oral Health and Long Term Care Strategy
Saskatchewan Seniors’ Oral Health and Long Term Care Strategy
Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan
Saskatchewan Oral Health Coalition October 24, 2016
A clean, healthy, pain-free mouth contributes greatly to:
• chewing and being able to enjoy a variety of nutritious foods
• clear speech and communication • sleeping well • overall health • general comfort and a higher quality of life • a more attractive personal appearance, positive
self-esteem and satisfying social interactions
Our Goal: Health and Wellness
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Oral conditions and dysfunctions are extremely painful and can devastate the quality of life of an individual.
Status of Oral Health among older adults in Long Term Care (LTC) homes in Saskatchewan
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Quite honestly, there is a lack of care being provided – daily care and regular appointments to control gum disease and examine the teeth.
Approximately 72% of residents in long term homes reported that routine oral hygiene is their greatest single need. (findings from University of Saskatchewan - College of Dentistry pilot study)
Better Oral Health in Long Term Care
• LTC residents often suffer from some form of dementia, and most have physical and medical challenges too.
• These fragile elderly are at an especially high risk for a number of serious conditions because they: • Often forget to brush their teeth or are unable to do it
without help • May resist or refuse assistance • May have problems recognizing and reporting pain and
discomfort in the mouth
Better Oral Health in Long Term Care
Resident Challenges
So if these are the facts… • Increasing population and associated high
prevalence of chronic diseases • Population of older adults will experience
“doubling phenomena” • Population over age 65 will double by 2030
• Older adults are retaining more teeth • Retention of natural teeth puts them at risk for
dental and oral diseases such as caries and periodontal diseases
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Knowing what we know – <read bullets> What can we do?
Better Health and Wellness • If the mouth is being cared for like the rest of the body,
diseases manifesting in the mouth like diabetes and cancer can be spotted sooner.
• If there is regular daily care and prevention, there will be less oral disease and less systemic disease – heart disease, diabetes, stroke, aspiration pneumonia.
= Less health care dollars being spent, while achieving
a better quality of life for our people
Better Oral Health in Long Term Care
Presenter
Presentation Notes
We cannot continue to ignore the mouth. This is about better health and wellness for the people of our province! Less health care dollars being spent while achieving a better quality of life for our people. That is our passion and the reason we are here. I will pass things on to ______ to describe more.
Proportion of Seniors: • In 2015, 14.6% of the residents of Saskatchewan were
seniors. (Statistics Canada, 2015)
• By 2036, 23.3% of Saskatchewan residents are expected to be seniors. (Statistics Canada, 2010)
Seniors: ≥ 65years First Reference: Statistics Canada. Proportion of the population aged 0 to 14 years and 65 years and older, July 1, 2015, Canada, provinces and territories [Internet]. Ottawa: Statistics Canada; 2015 [updated 2015 Sep 29; cited 2015 Dec 31]. Available from: http://www.statcan.gc.ca/daily-quotidien/150929/cg-b004-eng.htm. Second Reference: Statistics Canada .Population Projections for Canada, Provinces and Territories 2009 to 2036 [Internet]. Ottawa:Statistics Canada; 2010 [updated 2015 Nov 27; cited 2015 Dec 31]. Available from: http://www.statcan.gc.ca/pub/91-520-x/91-520-x2010001-eng.pdf.
Aging Population and Long Term Care Homes:
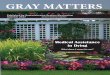
• In 2011, the percentage of Canadians seniors living in Special Care Homes increased with age. ( Census 2011)
0
5
10
15
20
25
30
35
40
65 to 69 years 70 to 74 years 75 to 79 years 80 to 84 years 85 years and over
Perc
enta
ge o
f Can
adia
ns L
ivin
g in
Sp
ecia
l Car
e Ho
mes
Age Group
Men Women Total
*Special care homes refers to nursing homes, chronic care or long-term care hospitals and residences for senior citizens
Better Oral Health in Long Term Care
Presenter
Presentation Notes
In 1981, 3% of individuals of 65-74 years of age and 17% of those ≥75 lived in special care homes. In 2006, the rates were only 1.4% and 12%, respectively. However, with the substantial rise expected in the number of seniors over the next decade (many of whom will have multiple chronic conditions), the need for long-term care beds in the near future may increase (Canadian Institute for Health Information. Health Care in Canada,2011:A Focus on Seniors and Aging [Internet].Ottawa:Canadian Institute for Health Information; 2011 [cited 2015 Dec 31]. Available from: https://secure.cihi.ca/free_products/HCIC_2011_seniors_report_en.pdf. Figure: Special care homes refers to nursing homes, chronic care or long-term care hospitals and residences for senior citizens The percentage of seniors living in special care homes in 2011 increased with age. Among the age group 65 to 69, approximately 1% lived in special care homes; among seniors aged 85 and over, the proportion was 29.6%. Reference: Statistics Canada. Percentage of the population aged 65 and over living in special care facilities by age group, Canada, 2011 [Internet]. Ottawa: Statistics Canada; 2011 [updated 2015 Nov 6; cited 2015 Dec 31]. Available from: http://www12.statcan.ca/census-recensement/2011/as-sa/98-312-x/2011003/fig/fig3_4-4-eng.cfm According to Continuing Care Reporting System 2014-2015, there were 111 residential care in Saskatchewan with 9,024 residents with the average age of 79 years; of the residents, 55.7% were 85 and above. Reference: Canadian Institute for Health Information. Continuing Care Reporting System. Quick Stats.CCRS profile of residents in continuing care facilities, 2014–2015 [Internet]. Ottawa: Canadian Institute for Health Information; 2015 [cited 2015 Dec 31]. Available from: https://www.cihi.ca/en/quick-stats. *Residential Care: this results is based on the submitting residential-based facilities in SK Given the size of the elderly in LTC homes and the extent of chronic diseases among this group, it is reasonable to conclude many of them need some level of support with their daily care including oral care. On the other hand, some diseases such as dementia pose a significant challenge for health. Residents with behavioral issues associated with dementia frequently have their oral hygiene neglected as they may be resistant and violent towards receiving oral care from LTC staff (28). The number of LTC residents suffering dementia is very high; according to Continuing Care Reporting System, in 2014-2015, 49.7% of residents of residential care in Saskatchewan had dementia (6.1% Alzheimer's disease, dementia other than Alzheimer's disease 46%) (Continuing Care Reporting System 2014-2015). ).
Aging Population and Long Term Care Homes:
• In 2014, there were 111 Residential Care Homes in
Saskatchewan with 9,024 residents. The average age was 79 years. 55.7% of the residents were ≥ 85. (Continuing Care Reporting System 2014-2015)
• In 2014, 49.7% of residents of Residential Care in Saskatchewan had dementia (6.1% Alzheimer's disease, dementia other than Alzheimer's disease 46%) (Continuing Care Reporting System 2014-2015)
Better Oral Health in Long Term Care
Presenter
Presentation Notes
In 1981, 3% of individuals of 65-74 years of age and 17% of those ≥75 lived in special care homes. In 2006, the rates were only 1.4% and 12%, respectively. However, with the substantial rise expected in the number of seniors over the next decade (many of whom will have multiple chronic conditions), the need for long-term care beds in the near future may increase (Canadian Institute for Health Information. Health Care in Canada,2011:A Focus on Seniors and Aging [Internet].Ottawa:Canadian Institute for Health Information; 2011 [cited 2015 Dec 31]. Available from: https://secure.cihi.ca/free_products/HCIC_2011_seniors_report_en.pdf. Figure: Special care homes refers to nursing homes, chronic care or long-term care hospitals and residences for senior citizens The percentage of seniors living in special care homes in 2011 increased with age. Among the age group 65 to 69, approximately 1% lived in special care homes; among seniors aged 85 and over, the proportion was 29.6%. Reference: Statistics Canada. Percentage of the population aged 65 and over living in special care facilities by age group, Canada, 2011 [Internet]. Ottawa: Statistics Canada; 2011 [updated 2015 Nov 6; cited 2015 Dec 31]. Available from: http://www12.statcan.ca/census-recensement/2011/as-sa/98-312-x/2011003/fig/fig3_4-4-eng.cfm According to Continuing Care Reporting System 2014-2015, there were 111 residential care in Saskatchewan with 9,024 residents with the average age of 79 years; of the residents, 55.7% were 85 and above. Reference: Canadian Institute for Health Information. Continuing Care Reporting System. Quick Stats.CCRS profile of residents in continuing care facilities, 2014–2015 [Internet]. Ottawa: Canadian Institute for Health Information; 2015 [cited 2015 Dec 31]. Available from: https://www.cihi.ca/en/quick-stats. *Residential Care: this results is based on the submitting residential-based facilities in SK Given the size of the elderly in LTC homes and the extent of chronic diseases among this group, it is reasonable to conclude many of them need some level of support with their daily care including oral care. On the other hand, some diseases such as dementia pose a significant challenge for health. Residents with behavioral issues associated with dementia frequently have their oral hygiene neglected as they may be resistant and violent towards receiving oral care from LTC staff (28). The number of LTC residents suffering dementia is very high; according to Continuing Care Reporting System, in 2014-2015, 49.7% of residents of residential care in Saskatchewan had dementia (6.1% Alzheimer's disease, dementia other than Alzheimer's disease 46%) (Continuing Care Reporting System 2014-2015). ).
Aging Population and Oral Health Problems: • Dental Caries • Edentulism (tooth loss) • Oral Candidiasis • Oral Pre-cancerous/cancerous Lesions • Periodontal Disease • Xerostomia (dry mouth)
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Common oral health conditions occurring in the seniors, including residents in LTC homes, are: dental caries,… Older adults are at greater risk for dental caries than younger adults because of age-related salivary changes, side effects of medications, poor diet, exposure of root surfaces through gum recession (37), changes in cognition and dexterity (34), and the presence of partial dentures (36) Dental caries has a high occurrence rate in residents in LTC homes (27, 38-40), mostly because of poor oral hygiene, excessive sugar consumption, medications that cause dry mouth and lack of dental treatment services (38)
Dental Caries Coronal Caries: • Canadians 60–79 years had the highest average DMFT
(15.7) (Canadian Health Measures Survey 2007-2009)
• In 39 Long Term Care (LTC) hospitals in Vancouver area, on average, 50.4% had coronal caries; and the average DMFT was 26.6 (Wyatt CC, 2002)
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Canadian Health Measures Survey (CHMS) exclude LTC homes In rural and urban LTC homes in Nova Scotia, among LTC dentate residents, 51% had untreated coronal caries. The average DMFT was 23.6; predictors of an increased DMFT score were years of smoking, increased age, and brushing less than once a day (Matthews DC, 2012). Root caries has become an important dental problem because people are living longer and keeping their teeth longer as opposed to earlier times where teeth were extracted due to coronal caries. As people grow older, their gums recede and root surfaces are exposed, making them more susceptible to root caries. The incidence of root caries in the elderly is associated with number of medical conditions and greater age (37). Root caries appears to be more difficult to detect and is much more difficult to treat (17). The prevalence of root caries among LTC residents is even higher. In Vancouver, the proportion of LTC hospital residents with root caries was 68.8% (39). Reference: Wyatt CC. Elderly Canadians residing in long-term care hospitals: Part II. Dental caries status. J Can Dent Assoc. 2002;68(6):359-63. Matthews DC, Clovis JB, Brillant MG, Filiaggi MJ, McNally ME, Kotzer RD, et al. Oral health status of long-term care residents-a vulnerable population. J Can Dent Assoc. 2012;78:c3 The number of Canadians with root caries is expected to grow by 50% from 2001 to 2021 and the majority of those affected by this root caries are expected to have no dental insurance (42)
Dental Caries Root Caries: • 11% of Canadians 60–79 had untreated root caries (Canadian Health
Measures Survey 2007-2009)
• In Vancouver, the proportion of LTC hospital residents with root caries was 68.8% (Wyatt CC, 2002)
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Canadian Health Measures Survey (CHMS) exclude LTC homes In rural and urban LTC homes in Nova Scotia, among LTC dentate residents, 51% had untreated coronal caries. The average DMFT was 23.6; predictors of an increased DMFT score were years of smoking, increased age, and brushing less than once a day (Matthews DC, 2012). Root caries has become an important dental problem because people are living longer and keeping their teeth longer as opposed to earlier times where teeth were extracted due to coronal caries. As people grow older, their gums recede and root surfaces are exposed, making them more susceptible to root caries. The incidence of root caries in the elderly is associated with number of medical conditions and greater age (37). Root caries appears to be more difficult to detect and is much more difficult to treat (17). The prevalence of root caries among LTC residents is even higher. In Vancouver, the proportion of LTC hospital residents with root caries was 68.8% (39). Reference: Wyatt CC. Elderly Canadians residing in long-term care hospitals: Part II. Dental caries status. J Can Dent Assoc. 2002;68(6):359-63. Matthews DC, Clovis JB, Brillant MG, Filiaggi MJ, McNally ME, Kotzer RD, et al. Oral health status of long-term care residents-a vulnerable population. J Can Dent Assoc. 2012;78:c3 The number of Canadians with root caries is expected to grow by 50% from 2001 to 2021 and the majority of those affected by this root caries are expected to have no dental insurance (42)
Edentulism and Denture Stomatitis: • Canadians 60–79 years had the highest rate of edentulism (22%) (Canadian Health Measures Survey 2007-2009)
• In Nova Scotia, among LTC residents, 41% were edentulous; 41% had some mucosal abnormality. Most of the dentures in lower jaw were non-retentive (59%) and almost half were unstable (49%) (Matthews DC, et al 2012)
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Edentulism: for some industrialized countries, including Canada, as people age, they tend to keep their teeth much longer than in the past. Where previously most elderly people could expect to replace all of their natural teeth with dentures, today most Canadians retain their natural teeth for a lifetime. In 1972, approximately 50% of Canadians above 60 years old were edentulous, whereas in 2009, almost 22% had no natural teeth (17). The highest rate of edentulism found in age group 60 to 79 years (22%) (17). The prevalence of tooth loss among LTC residents is even higher. In Nova Scotia, among LTC residents, 41% were edentulous (40) Reference: Matthews DC, Clovis JB, Brillant MG, Filiaggi MJ, McNally ME, Kotzer RD, et al. Oral health status of long-term care residents-a vulnerable population. J Can Dent Assoc. 2012;78:c3. Denture stomatitis is a common oral mucosal lesion beneath dentures in the elderly. The most common fungal infection linked to denture stomatitis is Candida Albicans. The prevalence of denture stomatitis is highly associated to denture hygiene or the amount of denture plaque Oral cancer: In Canada oral cancers are the 9th most common cancers among males and 13th among females. Oral cancer screening can detect early, localized lesions which are associated with an improved prognosis. Five-year survival rate is 2.5 times greater in patients with localized lesions than those whose oral cancer has spread to other parts of the body (49). As a result, there will be a need for continued strengthening of cancer prevention and early detection to decrease the future incidence of cancer and improving survival rate (50). Reference:Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian Cancer Statistics 2015 [Internet].Toronto: Canadian Cancer Society; 2015 [cited 2015 Dec 31]. Available from: http://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-Cancer-Statistics-2015-EN.pdf?la=en.
Oral Pre-cancerous/cancerous Lesions • In Canada, more deaths occur from oral cancer than from melanoma or cervical cancer. (Canadian Cancer Statistics 2015 ).
• The five-year survival rate for oral cancer is much lower (68% and 61% in female and male respectively) than the most common cancers, that is breast cancer and prostate cancer (Canadian Cancer Statistics 2015 ).
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Edentulism: for some industrialized countries, including Canada, as people age, they tend to keep their teeth much longer than in the past. Where previously most elderly people could expect to replace all of their natural teeth with dentures, today most Canadians retain their natural teeth for a lifetime. In 1972, approximately 50% of Canadians above 60 years old were edentulous, whereas in 2009, almost 22% had no natural teeth (17). The highest rate of edentulism found in age group 60 to 79 years (22%) (17). The prevalence of tooth loss among LTC residents is even higher. In Nova Scotia, among LTC residents, 41% were edentulous (40) Reference: Matthews DC, Clovis JB, Brillant MG, Filiaggi MJ, McNally ME, Kotzer RD, et al. Oral health status of long-term care residents-a vulnerable population. J Can Dent Assoc. 2012;78:c3. Denture stomatitis is a common oral mucosal lesion beneath dentures in the elderly. The most common fungal infection linked to denture stomatitis is Candida Albicans. The prevalence of denture stomatitis is highly associated to denture hygiene or the amount of denture plaque Oral cancer: In Canada oral cancers are the 9th most common cancers among males and 13th among females. Oral cancer screening can detect early, localized lesions which are associated with an improved prognosis. Five-year survival rate is 2.5 times greater in patients with localized lesions than those whose oral cancer has spread to other parts of the body (49). As a result, there will be a need for continued strengthening of cancer prevention and early detection to decrease the future incidence of cancer and improving survival rate (50). Reference:Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian Cancer Statistics 2015 [Internet].Toronto: Canadian Cancer Society; 2015 [cited 2015 Dec 31]. Available from: http://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-Cancer-Statistics-2015-EN.pdf?la=en.
Periodontal Disease (gingivitis and periodontitis) • In Nova Scotia, among LTC dentate residents, 67% had
Loss of Attachment (LOA) of ≥ 4 mm at one or more site (Matthews DC, et al 2012)
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Persistent presence of periodontal disease is associated with systematic conditions such as pneumonia (57), diabetes (58), cardio-vascular disease (CVD) and stroke (59). Clinically, pocket depths can be reduced by home care and professional treatment, but LOA is largely irreversible (17). Dry mouth, also known as xerostomia, is caused by reduction of saliva production. Saliva flow rate may be reduced in elderly people due to medications and various medical conditions (e.g. Sjögren’s syndrome, chemotherapy, radiotherapy) (60). Xerostomia is the most common adverse drug-related effect in the oral cavity and has been associated with over 500 medications. It is a particularly common in elderly patients. People 65 years and older are at greatest risk of developing xerostomia (60) Saliva plays a crucial role in oral health. It has natural cleansing effects, and aids in tooth remineralization, contains antibodies, helps prevent gingival ulcerations. When salivary function is diminished, there is more risk of individuals experiencing soreness, dryness of the mucosa and lips, dental caries, candidiasis, reduced sensation, difficulty eating, change in taste, impaired ability to speak, choking, difficulty in wearing dentures, and bad breath (43). Loss of the natural cleansing effect of saliva increases the oral bacterial load, which predisposes a frail person to conditions such as aspiration pneumonia (31), coronary artery disease and cerebral infarction (61). Moreover, people with xerostomia and tooth loss may have reduced masticatory ability, food avoidance from fibre, protein, vitamins, and minerals. Malnutrition may reduce immunity against infection (30)
Xerostomia (Dry Mouth)
• In a survey in LTC residents of Nova Scotia, the most common (36%) problem was xerostomia (Matthews DC, et al 2012)
Photo courtesy Peri-Products UK
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Persistent presence of periodontal disease is associated with systematic conditions such as pneumonia (57), diabetes (58), cardio-vascular disease (CVD) and stroke (59). Clinically, pocket depths can be reduced by home care and professional treatment, but LOA is largely irreversible (17). Dry mouth, also known as xerostomia, is caused by reduction of saliva production. Saliva flow rate may be reduced in elderly people due to medications and various medical conditions (e.g. Sjögren’s syndrome, chemotherapy, radiotherapy) (60). Xerostomia is the most common adverse drug-related effect in the oral cavity and has been associated with over 500 medications. It is a particularly common in elderly patients. People 65 years and older are at greatest risk of developing xerostomia (60) Saliva plays a crucial role in oral health. It has natural cleansing effects, and aids in tooth remineralization, contains antibodies, helps prevent gingival ulcerations. When salivary function is diminished, there is more risk of individuals experiencing soreness, dryness of the mucosa and lips, dental caries, candidiasis, reduced sensation, difficulty eating, change in taste, impaired ability to speak, choking, difficulty in wearing dentures, and bad breath (43). Loss of the natural cleansing effect of saliva increases the oral bacterial load, which predisposes a frail person to conditions such as aspiration pneumonia (31), coronary artery disease and cerebral infarction (61). Moreover, people with xerostomia and tooth loss may have reduced masticatory ability, food avoidance from fibre, protein, vitamins, and minerals. Malnutrition may reduce immunity against infection (30)
Importance of Prevention/Detection of Oral Problems in the Elderly
• Daily removal of plaque is an important factor for the maintenance of dental, gingival and periodontal health ( Arora V et al 2014)
• Brushing twice a day is the least expensive and most effective physical method to remove and control dental plaque (South Australian Dental Service 2009)
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Oral disease in all age groups is readily prevented by daily oral hygiene and adherence to a healthy diet. Oral diseases including caries and periodontal disease are highly preventable, considerable emphasis should be placed on prevention strategies. This should include highlighting the importance of an appropriate diet (minimal consumption of dietary carbohydrates, particularly between meals), providing patient-specific oral hygiene techniques (brushing, flossing, fluoride toothpastes), the prescription of additional fluoride to increase tooth resistance to dental caries (e.g. home fluoride rinses, fluoride varnish), and antibacterial agents (chlorhexidine, cetylpyridinium chloride) Arora V, Tangade P, T LR, Tirth A, Pal S, Tandon V. Efficacy of dental floss and chlorhexidine mouth rinse as an adjunct to toothbrushing in removing plaque and gingival inflammation - a three way cross over trial. J Clin Diagn Res. 2014;8(10):Zc01-4. Central Northern Adelaide Health Service. South Australian Dental Service. Better Oral Health in Residential Care Final Report. Adelaide: Central Northern Adelaide Health Service. South Australian Dental Service; 2009. Wyatt CC, Wang D, Aleksejuniene J. Incidence of dental caries among susceptible community-dwelling older adults using fluoride toothpaste: 2-year follow-up study. J Can Dent Assoc. 2014;80:e44. Silva MF, dos Santos NB, Stewart B, DeVizio W, Proskin HM. A clinical investigation of the efficacy of a commercial mouthrinse containing 0.05% cetylpyridinium chloride to control established dental plaque and gingivitis. J Clin Dent. 2009;20(2):55-61.
Importance of Prevention/Detection of Oral Problems in the Elderly
• A recent two year follow-up study showed, using fluoride toothpaste in elderly people slowed down the rates of progression of both coronal and root caries (Wyatt CC et al, 2014).
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Oral disease in all age groups is readily prevented by daily oral hygiene and adherence to a healthy diet. Oral diseases including caries and periodontal disease are highly preventable, considerable emphasis should be placed on prevention strategies. This should include highlighting the importance of an appropriate diet (minimal consumption of dietary carbohydrates, particularly between meals), providing patient-specific oral hygiene techniques (brushing, flossing, fluoride toothpastes), the prescription of additional fluoride to increase tooth resistance to dental caries (e.g. home fluoride rinses, fluoride varnish), and antibacterial agents (chlorhexidine, cetylpyridinium chloride) Arora V, Tangade P, T LR, Tirth A, Pal S, Tandon V. Efficacy of dental floss and chlorhexidine mouth rinse as an adjunct to toothbrushing in removing plaque and gingival inflammation - a three way cross over trial. J Clin Diagn Res. 2014;8(10):Zc01-4. Central Northern Adelaide Health Service. South Australian Dental Service. Better Oral Health in Residential Care Final Report. Adelaide: Central Northern Adelaide Health Service. South Australian Dental Service; 2009. Wyatt CC, Wang D, Aleksejuniene J. Incidence of dental caries among susceptible community-dwelling older adults using fluoride toothpaste: 2-year follow-up study. J Can Dent Assoc. 2014;80:e44. Silva MF, dos Santos NB, Stewart B, DeVizio W, Proskin HM. A clinical investigation of the efficacy of a commercial mouthrinse containing 0.05% cetylpyridinium chloride to control established dental plaque and gingivitis. J Clin Dent. 2009;20(2):55-61.
Importance of Prevention/Detection of Oral Problems in the Elderly
• Antibacterial agents such cetylpyridinium chloride (Perivex) provides protection against dental plaque and gingivitis. Perivex is non-fluoridated, alcohol free antibacterial mouth cleaning gel and is highly recommended for the residents at risk of choking. (Silva MF et al 2009)
• Brushing with mild soap and water is an effective way to clean dentures (South Australian Dental Service 2009)
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Oral disease in all age groups is readily prevented by daily oral hygiene and adherence to a healthy diet. Oral diseases including caries and periodontal disease are highly preventable, considerable emphasis should be placed on prevention strategies. This should include highlighting the importance of an appropriate diet (minimal consumption of dietary carbohydrates, particularly between meals), providing patient-specific oral hygiene techniques (brushing, flossing, fluoride toothpastes), the prescription of additional fluoride to increase tooth resistance to dental caries (e.g. home fluoride rinses, fluoride varnish), and antibacterial agents (chlorhexidine, cetylpyridinium chloride) Arora V, Tangade P, T LR, Tirth A, Pal S, Tandon V. Efficacy of dental floss and chlorhexidine mouth rinse as an adjunct to toothbrushing in removing plaque and gingival inflammation - a three way cross over trial. J Clin Diagn Res. 2014;8(10):Zc01-4. Central Northern Adelaide Health Service. South Australian Dental Service. Better Oral Health in Residential Care Final Report. Adelaide: Central Northern Adelaide Health Service. South Australian Dental Service; 2009. Wyatt CC, Wang D, Aleksejuniene J. Incidence of dental caries among susceptible community-dwelling older adults using fluoride toothpaste: 2-year follow-up study. J Can Dent Assoc. 2014;80:e44. Silva MF, dos Santos NB, Stewart B, DeVizio W, Proskin HM. A clinical investigation of the efficacy of a commercial mouthrinse containing 0.05% cetylpyridinium chloride to control established dental plaque and gingivitis. J Clin Dent. 2009;20(2):55-61.
Impacts of Poor Oral Health • Major health, social, psychological consequences
• Economic impacts • The total cost of poor oral health in older Australians
is estimated to be more than $750 million per year (Social Development Committee Parliament of South Australia, 2010)
• Employment of an “oral care specialist” such as a dental assistant, could result in net cost saving of more than $300 million annually (Stein PS, 2009)
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Social withdrawal and avoidance of social situations: Problems with speech, Avoidance of smiling.Embarrassment and shame Overall health: As Kellie discussed Economic Impacts: According to a 2002 analysis done in the United States, it was found that if 19,000 nursing homes employed an “oral care specialist” such as a dental assistant, with an average salary of $25,000 per year plus benefits, and if a 10% incidence of pneumonia among older adults was reduced due to care provided by the oral care specialist, there would be a net cost saving of more than $300 million annually (Stein PS, 2009). Stein PS, Henry RG. Poor oral hygiene in long-term care. Am J Nurs. 2009;109(6):44-50; quiz 1. Given the potential health risks of undiagnosed oral diseases, ranging from tooth decay to oral cancers, the potential cost to the health care system of untreated oral diseases could rise substantially in the next few years. In 2007, an economic analysis found the total cost of poor oral health in older Australians to be more than $750 million per year. Evidence presented to the Inquiry also suggested that thousands of hospital admissions could be avoided each year in Australia if early intervention for oral health problems had been available Reference: Social Development Committee Parliament of South Australia. Inquiry into Dental Services for Older South Australians [Internet]. [Place unknown]: Social Development Committee Parliament of South Australia;2010
Limited Access to Dental Services
• It is difficult for LTC residents to access oral care because dental services are mostly limited to emergency care within Canadian LTC homes. (Wyatt CC, 2009).
• Many LTC homes lack space for a dental unit. • Not all private dental clinics are wheelchair
accessible, or do not meet the demands of providing oral care to patients with dementia. (Yao Cs et al 2014)
Better Oral Health in Long Term Care
Presenter
Presentation Notes
A lack of interest in oral health professionals is an impediment to oral care (83). Changing and increasing caries patterns in aging dentate patients have created more challenges for clinicians. As people live longer and retain more teeth that are often already heavily restored, they will require more complex treatment (43). In a study on dentist perceptions of providing care in LTC homes, lack of financial rewards was a main barrier (38). Dentists are discouraged from providing geriatric services when insurance payments for dental services are less than the usual dental fees (84). A survey in Vancouver showed that 80% of dentists had never treated a patient in a LTC home. In addition, about two-thirds of respondents expressed no interest in offering services to elderly patients. Dentists who attended LTC homes reported they were uncomfortable about the limited options as well as the inadequate space and equipment available (85). MacEntee MI, Weiss RT, Waxler-Morrison NE, Morrison BJ. Opinions of dentists on the treatment of elderly patients in long-term care facilities. J Public Health Dent. 1992;52(4):239-44. Yao CS, MacEntee MI. Inequity in oral health care for elderly Canadians: part 2. Causes and ethical considerations. J Can Dent Assoc. 2014;80:e10. Systemic diseases: Management of frail elderly patients with multiple comorbidities usually requires collaboration with other health care professionals (e.g., dieticians, care aides nurses, physicians, social workers and speech language pathologists The 10 most common systemic diseases in the aging population that impact oral health care are: arthritis; head and neck cancer; chronic obstructive pulmonary disease; diabetes; ischemic heart disease; hypertension; mental health, cognitive impairment, Alzheimer disease; osteoporosis; Parkinson disease; and stroke (99). In some of these diseases, the person’s dexterity for oral hygiene is reduced. In some, cooperation makes it difficult for dental treatment. Many of these diseases require particular managements before, during or after dental treatments. Given the challenges of dental treatments for these patients, the dentist’s focus should always be on prevention of dental disease (99).
Daily oral care and basic professional dental services can: •Enhance the overall health and quality of life (Dyck D et al, 2012)
•Improve the success of treatment (BC Dental Association, 2011 )
•Reduce dental plaque (Dyck D et al, 2012 )
•Reduce the need for emergency care (BC Dental Association, 2011 )
•Reduce the need for invasive/complex treatment (BC Dental
Association, 2011 )
•Reduce the overall cost of care (Wyatt CC et al 1997, BC Dental Association,
2011 )
•Reduce the progression of oral disease (BC Dental Association, 2011 )
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Dyck D, Bertone M, Knutson K, Campbell A. Improving oral care practice in long-term care. Can Nurse. 2012;108(9):20-4. British Columbia Dental Association.Oral Health Care Delivery in Residential Care Facilities: A Report of the Seniors' Oral Health Secretariat [Internet]. Vancouver: British Columbia Dental Association; 2011 [cited 2015 Dec 31]. Available from: http://docplayer.net/6313298-Oral-health-care-delivery-in-residential-care-facilities.html. Wyatt CC, MacEntee MI. Dental caries in chronically disabled elders. Spec Care Dentist. 1997;17(6):196-202.
Programs/Services in Canadian Provinces
• British Columbia: The Geriatric Dentistry Program (2002): The program now offers services to the residents of several intermediate and extended care hospitals. Oral examinations and basic oral care are provided at the bedside using mobile dental equipment, while complex treatment is provided at University of British Columbia dental clinic, or at clinic within the hospital.
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The British Columbia government in 1997 passed changes to the Adult Care Regulation which governs licensed LTC homes in the province. According to this regulation, licensed LTC homes are required to provide certain oral health services to the residents. Under the regulation, the supervision clause for dental hygienists was removed which led to their enhanced role in providing care to the residents. Full time or retired dentists are encouraged to provide dental treatment in LTC homes by providing some incentive. Some health regions have oral health programs including oral health assessment, oral health promotion, preventive services and dental treatment (115). The Geriatric Dentistry Program in British Columbia started in 2002 as a joint venture between Providence Health Care and the University of British Columbia (UBC) Faculty of Dentistry. ELDERS (Elders Link with Dental Education, Research and Service) group from UBC have focused their attention on oral health in the elderly. The group was among the first in Canada to document the distribution of oral health problems in LTC homes, and to explore ways of managing the problems. The program now offers services to the residential care populations of several intermediate and extended care hospitals (117) Reference: The University of British Columbia. Geriatric Dentistry Program [Internet]. Vancouver: The University of British Columbia, Faculty of Dentistry; 2015 [cited 2015 Dec 31]. Available from: http://www.dentistry.ubc.ca/community-programs/geriatric-dentistry-program/. Halton, Ontario Oral Health Outreach Program (HOHO) is a multi-partner project and involves the coordination of dental services for people with special care needs and the elderly population. In 1999-2000 various initiatives were taken which led to the development of partnerships between Health Department and Community Care Access Centres (CCAC) of Halton Region. CCAC case managers complete oral health assessments for individuals entering a LTC home or clients living in the community who may require oral health services. At the time of the oral health assessment, financial assistance is also offered to the qualifying individuals to pay for the cost of dental treatment. It also provides referral to oral health services and dental resources in the community. Moreover, CCAC maintains a data base of those oral health professionals who are willing to provide services to the clients in their offices or other settings(120). Reference: Halton Region. Halton Oral Health Outreach Program. A Community Model for Accessing Oral Care Services that works [Internet]. Burlington: Halton Region; 2008.
Programs/Services in Canadian Provinces • Ontario: Halton, Ontario Oral Health Outreach Program Oral health assessments for individuals entering a LTC home, or clients living in the community who may require oral health services is completed. At the time of the oral health assessment, financial assistance is offered to qualifying individuals to cover the cost of dental treatment. In addition, the program maintains a data base of oral health professionals willing to provide services to clients in their offices or other settings.
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The British Columbia government in 1997 passed changes to the Adult Care Regulation which governs licensed LTC homes in the province. According to this regulation, licensed LTC homes are required to provide certain oral health services to the residents. Under the regulation, the supervision clause for dental hygienists was removed which led to their enhanced role in providing care to the residents. Full time or retired dentists are encouraged to provide dental treatment in LTC homes by providing some incentive. Some health regions have oral health programs including oral health assessment, oral health promotion, preventive services and dental treatment (115). The Geriatric Dentistry Program in British Columbia started in 2002 as a joint venture between Providence Health Care and the University of British Columbia (UBC) Faculty of Dentistry. ELDERS (Elders Link with Dental Education, Research and Service) group from UBC have focused their attention on oral health in the elderly. The group was among the first in Canada to document the distribution of oral health problems in LTC homes, and to explore ways of managing the problems. The program now offers services to the residential care populations of several intermediate and extended care hospitals (117) Reference: The University of British Columbia. Geriatric Dentistry Program [Internet]. Vancouver: The University of British Columbia, Faculty of Dentistry; 2015 [cited 2015 Dec 31]. Available from: http://www.dentistry.ubc.ca/community-programs/geriatric-dentistry-program/. Halton, Ontario Oral Health Outreach Program (HOHO) is a multi-partner project and involves the coordination of dental services for people with special care needs and the elderly population. In 1999-2000 various initiatives were taken which led to the development of partnerships between Health Department and Community Care Access Centres (CCAC) of Halton Region. CCAC case managers complete oral health assessments for individuals entering a LTC home or clients living in the community who may require oral health services. At the time of the oral health assessment, financial assistance is also offered to the qualifying individuals to pay for the cost of dental treatment. It also provides referral to oral health services and dental resources in the community. Moreover, CCAC maintains a data base of those oral health professionals who are willing to provide services to the clients in their offices or other settings(120). Reference: Halton Region. Halton Oral Health Outreach Program. A Community Model for Accessing Oral Care Services that works [Internet]. Burlington: Halton Region; 2008.
Programs/Services in Canadian Provinces • Alberta: Alberta Health Services – Calgary Zone
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The British Columbia government in 1997 passed changes to the Adult Care Regulation which governs licensed LTC homes in the province. According to this regulation, licensed LTC homes are required to provide certain oral health services to the residents. Under the regulation, the supervision clause for dental hygienists was removed which led to their enhanced role in providing care to the residents. Full time or retired dentists are encouraged to provide dental treatment in LTC homes by providing some incentive. Some health regions have oral health programs including oral health assessment, oral health promotion, preventive services and dental treatment (115). The Geriatric Dentistry Program in British Columbia started in 2002 as a joint venture between Providence Health Care and the University of British Columbia (UBC) Faculty of Dentistry. ELDERS (Elders Link with Dental Education, Research and Service) group from UBC have focused their attention on oral health in the elderly. The group was among the first in Canada to document the distribution of oral health problems in LTC homes, and to explore ways of managing the problems. The program now offers services to the residential care populations of several intermediate and extended care hospitals (117) Reference: The University of British Columbia. Geriatric Dentistry Program [Internet]. Vancouver: The University of British Columbia, Faculty of Dentistry; 2015 [cited 2015 Dec 31]. Available from: http://www.dentistry.ubc.ca/community-programs/geriatric-dentistry-program/. Halton, Ontario Oral Health Outreach Program (HOHO) is a multi-partner project and involves the coordination of dental services for people with special care needs and the elderly population. In 1999-2000 various initiatives were taken which led to the development of partnerships between Health Department and Community Care Access Centres (CCAC) of Halton Region. CCAC case managers complete oral health assessments for individuals entering a LTC home or clients living in the community who may require oral health services. At the time of the oral health assessment, financial assistance is also offered to the qualifying individuals to pay for the cost of dental treatment. It also provides referral to oral health services and dental resources in the community. Moreover, CCAC maintains a data base of those oral health professionals who are willing to provide services to the clients in their offices or other settings(120). Reference: Halton Region. Halton Oral Health Outreach Program. A Community Model for Accessing Oral Care Services that works [Internet]. Burlington: Halton Region; 2008.
Programs/Services in Canadian Provinces • Alberta: Alberta Health Services – Calgary Zone
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The British Columbia government in 1997 passed changes to the Adult Care Regulation which governs licensed LTC homes in the province. According to this regulation, licensed LTC homes are required to provide certain oral health services to the residents. Under the regulation, the supervision clause for dental hygienists was removed which led to their enhanced role in providing care to the residents. Full time or retired dentists are encouraged to provide dental treatment in LTC homes by providing some incentive. Some health regions have oral health programs including oral health assessment, oral health promotion, preventive services and dental treatment (115). The Geriatric Dentistry Program in British Columbia started in 2002 as a joint venture between Providence Health Care and the University of British Columbia (UBC) Faculty of Dentistry. ELDERS (Elders Link with Dental Education, Research and Service) group from UBC have focused their attention on oral health in the elderly. The group was among the first in Canada to document the distribution of oral health problems in LTC homes, and to explore ways of managing the problems. The program now offers services to the residential care populations of several intermediate and extended care hospitals (117) Reference: The University of British Columbia. Geriatric Dentistry Program [Internet]. Vancouver: The University of British Columbia, Faculty of Dentistry; 2015 [cited 2015 Dec 31]. Available from: http://www.dentistry.ubc.ca/community-programs/geriatric-dentistry-program/. Halton, Ontario Oral Health Outreach Program (HOHO) is a multi-partner project and involves the coordination of dental services for people with special care needs and the elderly population. In 1999-2000 various initiatives were taken which led to the development of partnerships between Health Department and Community Care Access Centres (CCAC) of Halton Region. CCAC case managers complete oral health assessments for individuals entering a LTC home or clients living in the community who may require oral health services. At the time of the oral health assessment, financial assistance is also offered to the qualifying individuals to pay for the cost of dental treatment. It also provides referral to oral health services and dental resources in the community. Moreover, CCAC maintains a data base of those oral health professionals who are willing to provide services to the clients in their offices or other settings(120). Reference: Halton Region. Halton Oral Health Outreach Program. A Community Model for Accessing Oral Care Services that works [Internet]. Burlington: Halton Region; 2008.
Programs/Services in Canadian Provinces • Alberta: Alberta Health Services – Calgary Zone
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The British Columbia government in 1997 passed changes to the Adult Care Regulation which governs licensed LTC homes in the province. According to this regulation, licensed LTC homes are required to provide certain oral health services to the residents. Under the regulation, the supervision clause for dental hygienists was removed which led to their enhanced role in providing care to the residents. Full time or retired dentists are encouraged to provide dental treatment in LTC homes by providing some incentive. Some health regions have oral health programs including oral health assessment, oral health promotion, preventive services and dental treatment (115). The Geriatric Dentistry Program in British Columbia started in 2002 as a joint venture between Providence Health Care and the University of British Columbia (UBC) Faculty of Dentistry. ELDERS (Elders Link with Dental Education, Research and Service) group from UBC have focused their attention on oral health in the elderly. The group was among the first in Canada to document the distribution of oral health problems in LTC homes, and to explore ways of managing the problems. The program now offers services to the residential care populations of several intermediate and extended care hospitals (117) Reference: The University of British Columbia. Geriatric Dentistry Program [Internet]. Vancouver: The University of British Columbia, Faculty of Dentistry; 2015 [cited 2015 Dec 31]. Available from: http://www.dentistry.ubc.ca/community-programs/geriatric-dentistry-program/. Halton, Ontario Oral Health Outreach Program (HOHO) is a multi-partner project and involves the coordination of dental services for people with special care needs and the elderly population. In 1999-2000 various initiatives were taken which led to the development of partnerships between Health Department and Community Care Access Centres (CCAC) of Halton Region. CCAC case managers complete oral health assessments for individuals entering a LTC home or clients living in the community who may require oral health services. At the time of the oral health assessment, financial assistance is also offered to the qualifying individuals to pay for the cost of dental treatment. It also provides referral to oral health services and dental resources in the community. Moreover, CCAC maintains a data base of those oral health professionals who are willing to provide services to the clients in their offices or other settings(120). Reference: Halton Region. Halton Oral Health Outreach Program. A Community Model for Accessing Oral Care Services that works [Internet]. Burlington: Halton Region; 2008.
Programs/Services in Canadian Provinces • Alberta: Alberta Health Services – Calgary Zone
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The British Columbia government in 1997 passed changes to the Adult Care Regulation which governs licensed LTC homes in the province. According to this regulation, licensed LTC homes are required to provide certain oral health services to the residents. Under the regulation, the supervision clause for dental hygienists was removed which led to their enhanced role in providing care to the residents. Full time or retired dentists are encouraged to provide dental treatment in LTC homes by providing some incentive. Some health regions have oral health programs including oral health assessment, oral health promotion, preventive services and dental treatment (115). The Geriatric Dentistry Program in British Columbia started in 2002 as a joint venture between Providence Health Care and the University of British Columbia (UBC) Faculty of Dentistry. ELDERS (Elders Link with Dental Education, Research and Service) group from UBC have focused their attention on oral health in the elderly. The group was among the first in Canada to document the distribution of oral health problems in LTC homes, and to explore ways of managing the problems. The program now offers services to the residential care populations of several intermediate and extended care hospitals (117) Reference: The University of British Columbia. Geriatric Dentistry Program [Internet]. Vancouver: The University of British Columbia, Faculty of Dentistry; 2015 [cited 2015 Dec 31]. Available from: http://www.dentistry.ubc.ca/community-programs/geriatric-dentistry-program/. Halton, Ontario Oral Health Outreach Program (HOHO) is a multi-partner project and involves the coordination of dental services for people with special care needs and the elderly population. In 1999-2000 various initiatives were taken which led to the development of partnerships between Health Department and Community Care Access Centres (CCAC) of Halton Region. CCAC case managers complete oral health assessments for individuals entering a LTC home or clients living in the community who may require oral health services. At the time of the oral health assessment, financial assistance is also offered to the qualifying individuals to pay for the cost of dental treatment. It also provides referral to oral health services and dental resources in the community. Moreover, CCAC maintains a data base of those oral health professionals who are willing to provide services to the clients in their offices or other settings(120). Reference: Halton Region. Halton Oral Health Outreach Program. A Community Model for Accessing Oral Care Services that works [Internet]. Burlington: Halton Region; 2008.
Programs/Services in Canadian Provinces • Alberta: Alberta Health Services – Calgary Zone
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The British Columbia government in 1997 passed changes to the Adult Care Regulation which governs licensed LTC homes in the province. According to this regulation, licensed LTC homes are required to provide certain oral health services to the residents. Under the regulation, the supervision clause for dental hygienists was removed which led to their enhanced role in providing care to the residents. Full time or retired dentists are encouraged to provide dental treatment in LTC homes by providing some incentive. Some health regions have oral health programs including oral health assessment, oral health promotion, preventive services and dental treatment (115). The Geriatric Dentistry Program in British Columbia started in 2002 as a joint venture between Providence Health Care and the University of British Columbia (UBC) Faculty of Dentistry. ELDERS (Elders Link with Dental Education, Research and Service) group from UBC have focused their attention on oral health in the elderly. The group was among the first in Canada to document the distribution of oral health problems in LTC homes, and to explore ways of managing the problems. The program now offers services to the residential care populations of several intermediate and extended care hospitals (117) Reference: The University of British Columbia. Geriatric Dentistry Program [Internet]. Vancouver: The University of British Columbia, Faculty of Dentistry; 2015 [cited 2015 Dec 31]. Available from: http://www.dentistry.ubc.ca/community-programs/geriatric-dentistry-program/. Halton, Ontario Oral Health Outreach Program (HOHO) is a multi-partner project and involves the coordination of dental services for people with special care needs and the elderly population. In 1999-2000 various initiatives were taken which led to the development of partnerships between Health Department and Community Care Access Centres (CCAC) of Halton Region. CCAC case managers complete oral health assessments for individuals entering a LTC home or clients living in the community who may require oral health services. At the time of the oral health assessment, financial assistance is also offered to the qualifying individuals to pay for the cost of dental treatment. It also provides referral to oral health services and dental resources in the community. Moreover, CCAC maintains a data base of those oral health professionals who are willing to provide services to the clients in their offices or other settings(120). Reference: Halton Region. Halton Oral Health Outreach Program. A Community Model for Accessing Oral Care Services that works [Internet]. Burlington: Halton Region; 2008.
Programs/Services in Canadian Provinces • Alberta: Alberta Health Services – Calgary Zone
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The British Columbia government in 1997 passed changes to the Adult Care Regulation which governs licensed LTC homes in the province. According to this regulation, licensed LTC homes are required to provide certain oral health services to the residents. Under the regulation, the supervision clause for dental hygienists was removed which led to their enhanced role in providing care to the residents. Full time or retired dentists are encouraged to provide dental treatment in LTC homes by providing some incentive. Some health regions have oral health programs including oral health assessment, oral health promotion, preventive services and dental treatment (115). The Geriatric Dentistry Program in British Columbia started in 2002 as a joint venture between Providence Health Care and the University of British Columbia (UBC) Faculty of Dentistry. ELDERS (Elders Link with Dental Education, Research and Service) group from UBC have focused their attention on oral health in the elderly. The group was among the first in Canada to document the distribution of oral health problems in LTC homes, and to explore ways of managing the problems. The program now offers services to the residential care populations of several intermediate and extended care hospitals (117) Reference: The University of British Columbia. Geriatric Dentistry Program [Internet]. Vancouver: The University of British Columbia, Faculty of Dentistry; 2015 [cited 2015 Dec 31]. Available from: http://www.dentistry.ubc.ca/community-programs/geriatric-dentistry-program/. Halton, Ontario Oral Health Outreach Program (HOHO) is a multi-partner project and involves the coordination of dental services for people with special care needs and the elderly population. In 1999-2000 various initiatives were taken which led to the development of partnerships between Health Department and Community Care Access Centres (CCAC) of Halton Region. CCAC case managers complete oral health assessments for individuals entering a LTC home or clients living in the community who may require oral health services. At the time of the oral health assessment, financial assistance is also offered to the qualifying individuals to pay for the cost of dental treatment. It also provides referral to oral health services and dental resources in the community. Moreover, CCAC maintains a data base of those oral health professionals who are willing to provide services to the clients in their offices or other settings(120). Reference: Halton Region. Halton Oral Health Outreach Program. A Community Model for Accessing Oral Care Services that works [Internet]. Burlington: Halton Region; 2008.
Programs/Services in Canadian Provinces • Alberta: Alberta Health Services – Calgary Zone
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The British Columbia government in 1997 passed changes to the Adult Care Regulation which governs licensed LTC homes in the province. According to this regulation, licensed LTC homes are required to provide certain oral health services to the residents. Under the regulation, the supervision clause for dental hygienists was removed which led to their enhanced role in providing care to the residents. Full time or retired dentists are encouraged to provide dental treatment in LTC homes by providing some incentive. Some health regions have oral health programs including oral health assessment, oral health promotion, preventive services and dental treatment (115). The Geriatric Dentistry Program in British Columbia started in 2002 as a joint venture between Providence Health Care and the University of British Columbia (UBC) Faculty of Dentistry. ELDERS (Elders Link with Dental Education, Research and Service) group from UBC have focused their attention on oral health in the elderly. The group was among the first in Canada to document the distribution of oral health problems in LTC homes, and to explore ways of managing the problems. The program now offers services to the residential care populations of several intermediate and extended care hospitals (117) Reference: The University of British Columbia. Geriatric Dentistry Program [Internet]. Vancouver: The University of British Columbia, Faculty of Dentistry; 2015 [cited 2015 Dec 31]. Available from: http://www.dentistry.ubc.ca/community-programs/geriatric-dentistry-program/. Halton, Ontario Oral Health Outreach Program (HOHO) is a multi-partner project and involves the coordination of dental services for people with special care needs and the elderly population. In 1999-2000 various initiatives were taken which led to the development of partnerships between Health Department and Community Care Access Centres (CCAC) of Halton Region. CCAC case managers complete oral health assessments for individuals entering a LTC home or clients living in the community who may require oral health services. At the time of the oral health assessment, financial assistance is also offered to the qualifying individuals to pay for the cost of dental treatment. It also provides referral to oral health services and dental resources in the community. Moreover, CCAC maintains a data base of those oral health professionals who are willing to provide services to the clients in their offices or other settings(120). Reference: Halton Region. Halton Oral Health Outreach Program. A Community Model for Accessing Oral Care Services that works [Internet]. Burlington: Halton Region; 2008.
Programs/Services in Canadian Provinces • Alberta: Alberta Health Services – Calgary Zone
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The British Columbia government in 1997 passed changes to the Adult Care Regulation which governs licensed LTC homes in the province. According to this regulation, licensed LTC homes are required to provide certain oral health services to the residents. Under the regulation, the supervision clause for dental hygienists was removed which led to their enhanced role in providing care to the residents. Full time or retired dentists are encouraged to provide dental treatment in LTC homes by providing some incentive. Some health regions have oral health programs including oral health assessment, oral health promotion, preventive services and dental treatment (115). The Geriatric Dentistry Program in British Columbia started in 2002 as a joint venture between Providence Health Care and the University of British Columbia (UBC) Faculty of Dentistry. ELDERS (Elders Link with Dental Education, Research and Service) group from UBC have focused their attention on oral health in the elderly. The group was among the first in Canada to document the distribution of oral health problems in LTC homes, and to explore ways of managing the problems. The program now offers services to the residential care populations of several intermediate and extended care hospitals (117) Reference: The University of British Columbia. Geriatric Dentistry Program [Internet]. Vancouver: The University of British Columbia, Faculty of Dentistry; 2015 [cited 2015 Dec 31]. Available from: http://www.dentistry.ubc.ca/community-programs/geriatric-dentistry-program/. Halton, Ontario Oral Health Outreach Program (HOHO) is a multi-partner project and involves the coordination of dental services for people with special care needs and the elderly population. In 1999-2000 various initiatives were taken which led to the development of partnerships between Health Department and Community Care Access Centres (CCAC) of Halton Region. CCAC case managers complete oral health assessments for individuals entering a LTC home or clients living in the community who may require oral health services. At the time of the oral health assessment, financial assistance is also offered to the qualifying individuals to pay for the cost of dental treatment. It also provides referral to oral health services and dental resources in the community. Moreover, CCAC maintains a data base of those oral health professionals who are willing to provide services to the clients in their offices or other settings(120). Reference: Halton Region. Halton Oral Health Outreach Program. A Community Model for Accessing Oral Care Services that works [Internet]. Burlington: Halton Region; 2008.
Saskatchewan Projects Background: During 2007-2008, pilot projects began in Saskatoon and Regina to provide clinical oral health services to the residents at LTC homes
• Regina: Santa Maria Senior Citizens Home • Full dental operatory • Dr. Maureen Lefebvre
• Saskatoon: St. Ann’s Home and Saskatoon Convalescent Home
• Portable dental equipment • Dr. Raj Bhargava
Better Oral Health in Long Term Care
Presenter
Presentation Notes
During 2007-2008, two pilot projects began in Saskatoon and Regina to provide clinical oral health services to the residents at LTC homes. In the Saskatoon Health Region (SHR), the University of Saskatchewan, College of Dentistry and a private practice dentist, Dr. Raju Bhargava and his team, implemented an oral health project at St. Anne’s Home and Saskatoon Convalescent Home. Within this project, the LTC residents received free oral health assessments. Portable equipment was then used to provide oral treatment for consenting residents. Treatment was paid for by the resident or their family. LTC home staff also received basic oral health education from SHR Oral Health Program staff. In Regina, in partnership with the College of Dental Surgeons of Saskatchewan (CDSS), University of Saskatchewan, College of Dentistry, and a private practice dentist, Dr. Maureen Lefebvre conducted a pilot project in the Santa Maria LTC home. Within this project, the LTC residents received free oral health assessments. Oral treatment was provided on site in dental operatory for residents who consented to treatment (paid for by the resident or their family). Over the next few years, Dr. Bhargava and his team in Saskatoon, and Dr. Lefebvre and Dr. Ed Reed with their team in Regina provided services to the LTC residents. The Santa Maria Seniors Oral Services (SOS) Program that originated in 2007 as a pilot project, continues to improve the oral health of LTC residents.
Regina Pilot: • The College of Dentistry (U of S) partnered with Santa
Maria Senior Citizens Home to provide support for: o administration o human resources (dental assistant) o oral health status/data o treatment needs
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The Regina pilot project saw the College of Dentistry at the U of S partner with Santa Maria in Regina. Dr. Maureen Lefebvre headed this pilot, conducting assessments and collecting data. I would be remiss if I did not note that Dr. Lefebvre and a team of Regina dentists continued the project working with the College of Dentistry and continue to offer oral care in Santa Maria to this day.
• College of Dentistry, (U of S) partnered with St. Ann’s Nursing Home/Saskatoon Convalescent Home
• Residents and their families were surveyed on basic oral health information.
• Saskatoon Health Region – Population and Public Health, Dental Health Educators provided education to long term care staff at two long term care homes.
Better Oral Health in Long Term Care
Saskatoon Pilot:
Presenter
Presentation Notes
The College of Dentistry also partnered with St. Ann’s and Saskatoon Convalescent Home in Saskatoon to conduct similar assessments. In addition to the assessments, Dental Health Educators employed in the health region provided training and education to staff to address the knowledge gap identified in caregivers. Dr. Bhargava initially led the pilot and at the end of the pilot continued to offer dental treatment within these facilities utilizing a private practice delivery model.
Survey Results:
A 2007 Saskatoon Health Region survey of staff, residents, and residents’ families showed that:
• 35% of residents were experiencing problems with their teeth/gums;
• 69% of residents only accessed oral care when there were problems (mobility was the main reason);
• 64% of residents perform their own daily care; and
• the main reasons LTC staff do not provide daily care to residents is uncooperative residents, and not enough time.
Better Oral Health in Long Term Care
Presenter
Presentation Notes
During 2007-2008, two pilot projects began in Saskatoon and Regina to provide clinical oral health services to the residents at LTC homes. In the Saskatoon Health Region (SHR), the University of Saskatchewan, College of Dentistry and a private practice dentist, Dr. Raju Bhargava and his team, implemented an oral health project at St. Anne’s Home and Saskatoon Convalescent Home. Within this project, the LTC residents received free oral health assessments. Portable equipment was then used to provide oral treatment for consenting residents. Treatment was paid for by the resident or their family. LTC home staff also received basic oral health education from SHR Oral Health Program staff. In Regina, in partnership with the College of Dental Surgeons of Saskatchewan (CDSS), University of Saskatchewan, College of Dentistry, and a private practice dentist, Dr. Maureen Lefebvre conducted a pilot project in the Santa Maria LTC home. Within this project, the LTC residents received free oral health assessments. Oral treatment was provided on site in dental operatory for residents who consented to treatment (paid for by the resident or their family). Over the next few years, Dr. Bhargava and his team in Saskatoon, and Dr. Lefebvre and Dr. Ed Reed with their team in Regina provided services to the LTC residents. The Santa Maria Seniors Oral Services (SOS) Program that originated in 2007 as a pilot project, continues to improve the oral health of LTC residents.
Regina and Saskatoon Data:
• Average age 86 (n = 200) • Male 29%; Female 71% • Residents requiring dental care: 67% • Residents with decay: 55% with decay • Residents with nerve involvement pain and/or infection):
15%
Presenter
Presentation Notes
What did the surveys reveal? The two surveys provided significant data related to the oral health of these residents. The results of the two pilot projects were staggering: we saw that 67% of those examined required dental care; 55% had active decay and 15% were in pain or had signs of infection.
Regina and Saskatoon Data: • Residents with own teeth: 50% • Residents with no teeth: 50% • Residents with faulty dentures: 46% • Dentures with no identification: 71.5% • Average treatment cost* per resident: $137.00
*Included oral hygiene services, treatment (fillings and extractions) and denture repair
Presenter
Presentation Notes
The oral health teams were also were able to discern statistics related to the residents with teeth, those without teeth or edentulous and those living with faulty dentures. They were also able to identify that 71% of the dentures were without any identification (which of course is a significant concern in Long Term Care). The team were also able to identify an average cost of $137.00 for treatment.
• Staff understanding of oral health issues increased significantly between pre and post surveys.
• Staff indicated most challenging aspects of providing mouth care were:
• uncooperative residents • not enough time • not enough/any appropriate supplies
Regina and Saskatoon Data:
Better Oral Health in Long Term Care
Presenter
Presentation Notes
If you ask what we accomplished? We learned a great deal about the oral needs of long term care residents. We were able to increase the awareness of all staff and specifically caregivers. We also learned significant information of the challenges faced by caregivers. This has been helpful as we moved forward seeking solutions.
Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan Since 2011, the Saskatchewan Oral Health Professions (SOHP) and Saskatchewan Oral Health Coalition have been collaborating to develop a model for oral health care in LTC:
• conducted best practice literature review • developed policies and procedures • continued data collection • informed and include other health regions and
providers.
Presenter
Presentation Notes
Our project continued on another front. While dental treatment is essential, further underlying issues needed addressing. The Saskatchewan Oral Health Professions endeavoured to deal with the causative issues and develop a model for care. We reviewed literature, we developed policies and procedures, we continued to incorporate and front line realities and we have shared our strategies with other health regions.
Background:
• In 2011, the Saskatchewan Oral Health Professions (SOHP) and Saskatchewan Oral Health Coalition (SOHC) endorsed the use and adaptation of the Australian Better Oral Health in Residential Care
• Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan program was focus tested in Saskatoon Health Region at Parkridge Centre, in two of their neighborhoods, in early 2014.
Better Oral Health in Long Term Care
Presenter
Presentation Notes
An outcome of this initial pilot was a second pilot in 2011 that supported an Oral Health Coordinator (OHC) at two LTC homes in SHR – Parkridge Centre, and Sherbrooke Community Centre. This was called the Oral Health LTC Initiative. It was supported with a $20,000 Community Wellness Grant from SHR. A registered dental assistant was hired in partnership with the University of Saskatchewan, College of Dentistry as the OHC and assisted LTC staff and residents to access oral care at each site. The College of Dentistry-General Dental Residency Program, delegated dentists from the program to provide treatment for residents who consented. All initial assessments were free of charge, to encourage residents to participate.
• Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan is a train-the-trainer model teaching the best practices to provide daily oral care.
Presenter
Presentation Notes
Better Oral Health in Long Term Care – Best Practice Standards for Saskatchewan consists of three training modules to prepare facilitators, professionals and staff.
• The Parkridge Centre pilot was used as the model for full implementation in other LTC homes in Saskatoon Health Region.
• Saskatoon Health Region Population and Public Health Dental Health Educators provided pre-assessments, facilitator training, and monitored implementation.
Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan Portfolios: Educators’, Professional, Staff)
Educators’ Portfolio Professional Portfolio Staff Portfolio
Better Oral Health in Long Term Care
Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan Posters and Pamphlets
Better Oral Health in Long Term Care
Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan Oral Health Assessment Tool (OHAT)
Better Oral Health in Long Term Care
Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan Oral Health Care Plan (OHCP)
Better Oral Health in Long Term Care
Better Oral Health in Long Term Care
The oral care costs are included in the $20.25/month charged to each resident for personal care items. (Pilot program at Parkridge Centre in Saskatoon )
Residents with Natural Dentition Not Requiring Assistance: •Fluoridated toothpaste ($0.72) •Toothbrushes GUM ($0.52) •End-Tuft toothbrushes GUM ($0.50)
Residents Needing Assistance or Having Swallowing or Expectorating Difficulties: • Perivex ($1.67) • Toothbrushes GUM ($0.52) • End-Tuft toothbrushes GUM ($0.50)
Residents that are edentulous: •Perivex ($1.67) •Toothbrushes GUM ($0.52) •Polident Tablet ($0.11)
Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan Basic Oral Hygiene Supplies
Presenter
Presentation Notes
Based on the pilot program at Parkridge Centre in Saskatoon the following products should be supplied to each resident within the monthly allowance for personal care items for LTC homes. This is approximately $20.25 per month.
Long Term Care Smiles: The Journey of Implementing
an Oral Health Program at Parkridge Centre, Saskatoon
2011 – Yearly treatments Better Oral Health in Long Term Care
Presenter
Presentation Notes
Parkridge had a dental therapist coming for dental care however later into 2011 Parkridge began a systematic dental cleaning and treatment program was implemented that co-ordinated with the U of S College of Dentistry. But this was not enough. A great start of awareness but how were we going to have the staff more aware of oral health importance and change the practice of minimal oral care (toothettes) to effective oral care (brushing with a toothbrush) between treatments.
November 2012
Why re-invent the wheel?
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Nov 2012, Canadian Nurse (explain what it is) came out with an Oral Care Protocol for LTC. The site was Deer Lodge Centre in Winnipeg. They experienced what many LTC Centres also experience. Oral Care for dependent residents in LTC consist of sponge swabs dipped in liquid mouth rinse and denture care with regular toothpaste and Polident. The study sought to answer the questions: Are sponge swabs effective in cleaning the oral cavity? The Winnipeg pilot showed improvements, specifically Reductions in: plaque Swollen and bleeding gums Ulcerations Severe halitosis Staff members were resistant to change until they saw the benefits of tooth brushing. The use of sponge swabs also declined. At Parkridge we have many residents with high medical and behavioural needs. Many of these residents do not swish and spit. There was no way of getting foaming toothpaste out of the mouth therefore a sponge swab dipped in mouth wash was the only care they were receiving. I phoned Deer Lodge Centre, talked to authors of the article which were employees of the home. I was most interested in how they delivered the oral care of the high needs residents. Apparently they purchased soft small headed toothbrushes with large soft rubber barrelled handles which could be used as mouth props. Holding the mouth open as oral care was given. They also found a oral non-foaming antibacterial mouth gel named Perivex which did not contain fluoride and was suitable for brushing those residents teeth that did not swish and spit. It also doubled as lip moisturizer. Also great for loosening the coating on the tongue. They also gave me a wealth of information about their suppliers and cost of the supplies.
• The oral health kit is based on the model used @ Deer Lodge Centre in Winnipeg.
Equipment
Better Oral Health in Long Term Care
• Meetings with Material Management to bring products into our Stores inventory.
Presenter
Presentation Notes
This information started many meetings with Leslie Topola and the staff of oral educators and SHR Material Management. We finally received the products. Toothbrushes changed every 6 months. During this time there were also many other projects with tighter timelines that our Staff Development Dept had to implement. Oral care became derailed numerous times, only prolonging the project. Containers from Superstore dedicated for oral health products only completed the kit.
MAY 2014
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Performing an OHAT Work in pairs – one examiner, and one recorder (operator/resident safety, infection control and reduced examination time for resident)
Better Oral Health in Long Term Care
Clinical Nurse Educators used a mannequin with teeth and tongue to educate the staff and champions of each
Neighborhood/Unit.
Presenter
Presentation Notes
DHEs trained Clinical Nurse Educators (CNE) and one Speech Language Pathologist (SLP) on how to perform the OHAT and daily oral care. CNE then trained the CCA’s on the units in the importance and techniques for giving oral care.
Better Oral Health in Long Term Care
Practice on each other
Presenter
Presentation Notes
As well as practice on each other
Work Standards Developed (Parkridge Centre Staff Development and Saskatoon Health Region Dental Educators)
1. Oral Care Routine Assessment: • Basic assessment process
2. Proper Oral Health in LTC: • Basic oral care for natural teeth • Basic oral care for the Edentulous resident • Oral care for a resident with dysphagia
Better Oral Health in Long Term Care
Presenter
Presentation Notes
During this time with a lot of help from Leslie and her team of oral Health educators, two new Work Standards were developed.
Presently at Parkridge Centre: • Oral care has now been implemented on all
neighborhoods (units), staff are practicing oral care techniques.
• Products have been assigned SKU numbers and can be ordered through our Saskatoon Health Region Materials Management (Stores) by the neighborhood clerks.
• A Dental Assistant visits the neighborhoods weekly to educate staff, assist with new resident assessments, conduct 6 month re-assessments and staff referrals to deal with challenges for oral care of residents. This is paid by the Saskatoon Health Region.
Better Oral Health in Long Term Care
Daily Oral Care Supply Costs: • Included are: toothbrushes, toothpaste, Perivex non-
foaming antibacterial gel, denture cups, Polident, and mouthwash.
• The costs are included in the $20.25 charged monthly to each resident for personal care items at Parkridge Centre.
Cost per resident Before implementation After implementation
Standard Toothbrush, toothpaste, denture cups, Polident, mouthwash
Before implementation: Oral care products: $5065.70 yearly cost divided by 237 residents = $21.37/ resident/yr. divided by 12 = $1.78 / resident / month After implementation of new oral care program: Oral care products: $8060.36 yearly cost divided by 237 residents = $34.00/resident/yr. divided by 12 months = $2.38 / resident / month Cost difference per month = $1.05 / resident /month (increase of $2986.20 yearly cost although start up costs were included in this year that the program has been in effect). Benefits far outweigh costs
Better Oral Health in Long Term Care
Update: 2016
• Oct 2015 saw the transition from the pilot project as the Saskatoon Health Region OHP hired a dental assistant into the LTC OH Coordinator position.
• LTC OHC has audited/refreshed staff at Parkridge and implemented Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan at Sherbrooke and Sunnyside
• More LTC homes in Saskatoon Health Region interested • Saskatoon Health Region LTC Advisory Committee has
the reviewed Better Oral Health in LTC strategy and is supportive.
Better Oral Health in Long Term Care
Presenter
Presentation Notes
In October 2015 a transition occurred. The Saskatoon Health Region NEED WORDS… [OHP] hired a dental assistant into the Long Term Care Oral Health Coordinator position. The coordinator has audited/refreshed staff at Parkridge and implemented Better Oral Health in Long Term Care at Sherbrooke and Sunnyside. The Saskatoon Health Region is regularly contacted by other Long Term Care homes who want to be included. The Saskatoon Health Region Long Term Care Advisory Committee have the reviewed Better Oral Health in Long Term Care proposal and is supportive of it – and have stated that it is long overdue As we have moved this project forward, we remain committed to developing a model that can be instituted across Saskatchewan in every health region and every long term care home.
LTC - Oral Health Coordinator Role:
• Train staff to provide daily care • Provide health education and
promotion • Communicate/liaise with family • Coordinate/liaise with LTC staff
to expedite effective care • Coordinate consent/medical
history process as required
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Some of the roles I play as the oral heal Coordinator in LTCS A full day of training is booked at the home who has asked for me to come and train their staff. ½ day of powerpoints and videos and ½ day of hands on training with their residents. Daily I provide health education to the Care aides and promote the Beetter Oral Health program Laise with family can look like a phone call to find out if a family member can join a resident at the dental appt because we think they would be more relaxed with their presence there with them Laise with staff can look like phone calls to coordinate OT staff and dental staff for the same time of appts that are made. Consent and medical history process require my time at the LTC home consulting with the residents RN’s to make sure the consents are current medications for the dentist to review before treatment I love Sheri Townsend’s Quote “In order to provide the appropriate daily oral care supports, we must accommodate the medical and behavioral needs of our residents”
LTC Oral Health Coordinator
Oral Health Assessment Tool Kit
Better Oral Health in Long Term Care
Presenter
Presentation Notes
I know my presence has made a huge difference in The Better Oral Health, Best Practice Standards program becoming successful in the LTC homes. Because I am there, in the homes, as an Oral Health Presence! It reminds them about the oral health of their residents that they care for. When they see me coming into their neighbourhoods with my oral health assessment tool kit, they greet me and ask me “who are you here to see today and could you possibly see someone else as well?” Before this program was introduced to their homes when the care aides were having trouble accessing a resident’s mouth, they would have often given up but. Now that I am there for them to ask for my assistance they are not giving up. So often a short demonstration gets them on their way to do it on their own.. Some times though they will ask me, “are you here to do foot care?” I say “no mouth care!!!!!” Only because they are not used to having someone in there home addressing oral care in the LTC setting.
Thankful Residents
This particular resident was having her partial dentures cleaned every day, but not her natural teeth! Notice the big smile after the care aide has completed her oral care! This particular care aide requested that I visit and help her become more comfortable doing oral care for this resident, who was new to her area of care.
Better Oral Health in Long Term Care
Presenter
Presentation Notes
I feel my position as the first Oral health Coordinator of LTC very pivotal in the Dental World! As the health professionals that are working in LTC such as care-aids, RN’s and LPNs become more comfortable with my position and as they are becoming more comfortable with assisting the LTC residents with their oral health, they are now asking me questions about the residents’ mouths. They are also asking me questions about their own oral health and their children’s oral health as well. It seems to be win/ win situation all around as these health professionals are learning about Oral health on so many levels because of my presence in the LTC homes.
Love this Smile This Residents’ body has stiffened up and he can no longer care for his own mouth on his own. A care aide assists him by guiding his hand with the hand over technique, but some days he can’t grip his toothbrush at all. They then provide full assistance.
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Spending time with these LTC Residents has changed my life in a very rewarding way. Getting to know them and finding out how they found their way to LTC homes is very sobering! 25 to 35 year olds that have had strokes or aneurysms or car accidents and diving accidents leaving some quadriplegics to children who are victims of Shaken Baby Syndrome to survivors of a house fire who suffered brain damage from the smoke inhalation to residents in the later stages of MS to so many elder residents with dementia!
Smiles all Around
This resident is happy he is able to see the dentist in his own home, and also that I have been able visit him to help him brush and floss his own teeth more effectively. He told me “no one had ever explained to him why he should brush his teeth”.
Better Oral Health in Long Term Care
Presenter
Presentation Notes
All of these people Residents that I have talked about have full dentitions and no-one brushing their teeth until this program was introduced to their homes. I have seen mouths of residents who while they were healthy took very good care of their oral health, paying and receiving thousands of dollars of dental work completed and then after entering LTC, developing decay all around that extensive dental work and ending up losing their teeth. Why has this happened? Because no one was assisting them basic with oral care of brushing and flossing.
Before assistance After assistance
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Often after a resident is seen by a Hygienist in the LTC setting I will do a follow-up visit a week or so after to see how the care in coming along. The build up you see around these teeth is just plaque ! This is a bio film that will buildup in anyone mouth . Simple daily brushing will remove this plaque. When a resident cannot perform their own daily oral care they are at the mercy of the staff in the LTC home to assist them with this care.
Resident that has benefited with the use of an electric tooth brush
Before brushing After brushing
Better Oral Health in Long Term Care
Presenter
Presentation Notes
The Hygienist had suggested an electric tooth brush for this resident ! I demonstrated how to use the electric toothbrush to the staff ! Look at the difference after one brushing! The care staff had only been brushing the top half of the teeth ! Once they are shown how to pull the lips down and away from their teeth? Only then will they see the build- up at the gum line and be able to remove it !
I have been asked by residents and their families:
“Why do LTC homes have spaces allotted for beauty salons
and physical therapy rooms in the planning of the building development,
but no Dental Clinics ?”
Better Oral Health in Long Term Care
Presenter
Presentation Notes
Because there are now dentists and Hygienists that visit the LTC homes to provide dental treatment, I am able to refer the residents in need or dental pain to these oral health professionals. I am able to help with the completing of the consent forms. These consent forms need to be in place for the residents before they are seen by the dentist. When the Dentists, Assistants and Hygienists come to the LTC homes often they will have to do their dental procedures in the solariums, activity rooms or even meeting rooms ! No space has been allotted for a Dentist or a Hygienist to do their treatment ! I have to tell them that oral health has not been a priority in LTC in the past. People entering LTC never used to have their own natural teeth like they do now.
The SOHP and SOHC have developed and
endorsed the following recommendations
for consideration and action by the
Saskatchewan Ministry of Health:
Better Oral Health in Long Term Care
Recommendation #1: The Saskatchewan Government, Ministry of Health, endorse the Saskatchewan Seniors’ Oral Health and Long Term Care Strategy developed by SOHP collaboratively with SOHC and Seniors Health and Continuing Care in the Saskatoon Health Region.
Better Oral Health in Long Term Care
Recommendation #2: An OHC, who is a registered and licensed oral health professional (minimum of one) , should be employed in each health region to facilitate the delivery of initial oral assessments, dental examinations and treatment, daily oral hygiene for residents and oral health education. The OHC will work collaboratively with the LTC, multi-disciplinary team to improve the oral and overall health of residents.
Better Oral Health in Long Term Care
Recommendation #3: Upon entry into a LTC home, an initial oral assessment must be completed by a registered and licensed oral health professional, through the general and medical consent provided by the LTC home.
i. Oral assessments should be routinely performed every 6 months thereafter, by an oral health professional or a health care professional trained in oral health assessments.
ii. Non-oral health professionals performing oral health assessments or care will receive appropriate training developed by the Saskatchewan Oral Health Professions.
iii. Training will be provided by oral health professionals.
Better Oral Health in Long Term Care
Recommendation #4: Initial oral assessments will include: i. Personal client record*, including consent for dental examination
ii. Review of medical and dental history
iii. Complete examination of the oral cavity, which includes:
• Assessment of hard and soft tissues
• Assessment of oral hygiene care
• Oral cancer screening
• Denture assessment *Note: Implementation of a Saskatchewan electronic health record should include an oral health record.
Better Oral Health in Long Term Care
Recommendation #5: Oral Health Care Policies and Procedures for LTC and Personal Care Homes* are standardized and implemented based on best practice for optimal oral and overall health for residents in LTC in Saskatchewan. Policies should ensure that every LTC resident has the right and access to the following oral health care services:
i. An individualized oral health care plan ii. Basic oral hygiene supplies iii. Daily oral hygiene iv. Access to professional oral health services v. Oral health record included within the health record vi. Dental recommendations/orders are followed *Note: As per Section 23 of the current Personal Care Home Regulation (1996), each resident receive a dental examination, as necessary.
Better Oral Health in Long Term Care
Recommendation #6: Treatment needs based on the dental examination, may be provided by dentists, denturists, dental hygienists, dental therapists and/or dental assistants. Residents may access dental services through their personal oral health professional or through dental services as available through the LTC home. Dental examinations require:
i. Consent for dental examination ii. Treatment plan and progress notes iii. Estimate and consent for financial responsibility iv. Consent for treatment
Better Oral Health in Long Term Care
Recommendation #7: The Saskatchewan Seniors’ Oral Health and Long Term Care Strategy is incorporated into post-secondary educational health training programs, orientation, and continuing professional development (i.e. for care aides, nurses, physicians, etc.).
Better Oral Health in Long Term Care
Recommendation #8: The standard for new LTC homes includes provision for a treatment room suitable for a variety of health professionals including access to portable dental equipment to facilitate dental treatment.
Better Oral Health in Long Term Care
Kitchen/ Dental Clinic!
Recommendation #9: Surveillance, evaluation and continuous quality improvement be performed on an ongoing basis to demonstrate improved health and oral health status outcomes.
Better Oral Health in Long Term Care
Recommendation #10: The Saskatchewan government establish a safety net program to increase access to oral health services for low income seniors (similar to Ministry of Health Supplementary Health/Family Health Benefits or Alberta’s Dental Assistance for Seniors Program through which low income seniors are eligible for up to $5000 every 5 years for those aged 65 and older).
Better Oral Health in Long Term Care
Our Provincial Vision for Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan
• Consistent integration of oral health into policy and practice of LTC homes
• A provincial framework for oral health assessment, oral health care planning and oral care treatment for residents
• A multidisciplinary team approach to improve the oral health of the residents
Better Oral Health in Long Term Care
• Improved quality of life for residents who suffer from poor oral health and nutritional deficiencies
• Regular assessments and oral health treatments
• Residents receiving oral health treatment in the LTC homes rather than having to face the challenges involved with travelling offsite for care
Better Oral Health in Long Term Care
Our Provincial Vision for Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan
• Decreased occurrence of systemic conditions in the residents
• Decreased health care spending
Better Oral Health in Long Term Care
Our Provincial Vision for Better Oral Health in Long Term Care: Best Practice Standards for Saskatchewan
How can you support and/or move Better Oral Health in Long Term Care forward in your workplace?
Better Oral Health in Long Term Care
Presenter
Presentation Notes
We know that Saskatchewan Health has no mandated requirements to provide oral health examinations, dental treatment, or even daily mouth care in the Long Term Care Act. [is this right reference?] We also know that Improved oral health in long term care can improve overall health, reduce hospitalizations, and significantly improve quality of life. We also know that daily oral care is critical to quality of life and preventing systemic disease.