Embed Size (px)
Citation preview
| 1
Eyes for the invisible: microfluidic paper-based analytics (µPads) and
3rd - generation sequencing in clinical microbiology
John WA Rossen, PhD, MMM
Principle Investigator - Genomics for Infection Prevention
Head Molecular Unit
Department of Medical Microbiology, University of Groningen, University Medical
Center Groningen, Groningen, The Netherlands
Disclosure of speaker’s interests
(Potential) conflict of interest None
Potentially relevant company relationships in
connection with eventNone
Sponsorship or research funding
Fee or other (financial) payment
Shareholder
Other relationship
· Interreg IVa-funded projects EurSafety
Heath-net (III-1-02=73) and SafeGuard
(III-2-03=025)
· None
· None
· None
Disclosure slide for speaker at further training events

Eyes for the invisible
A Dutch tradition?
Antoni van Leeuwenhoek (1632-1723)
Martinus Beijerinck (1851 - 1931)
Filtration experiments Virus
Questions the patients have regarding infections/infectious diseases
1. Did you prevent colonization and infection today?
2. Do I have an infection/ID and which one?
3. What is the optimal therapy?
Molecular Diagnostics – a powerful tool
• Detection (Real-time PCR/NASBA/LAMP)
– Unculturable micro-organisms
– Viral/bacterial load
– Therapeutic monitoring
• Typing (PCR, DNA arrays, Sequencing, AFLP)
– Surveillance of infectious diseases
– Outbreak investigation (epi-typing)
– Pathogenesis and course of infection (patho-typing) • drug resistance (genes) and virulence genes
Does NGS fits it all?

Wet-lab technicians – practical work
Analysis performed by
• E-lab Technicians (Sigrid/Erwin)
• Master Kai Zhou teaches
Post-docs and PhDs
Amplicon-based approach
• Use of the Hospital Acquired Infections (HAI) BioDetection approach for:
– rapid identification of negative clinical samples
– detection of microbes and resistance/virulence genes
10
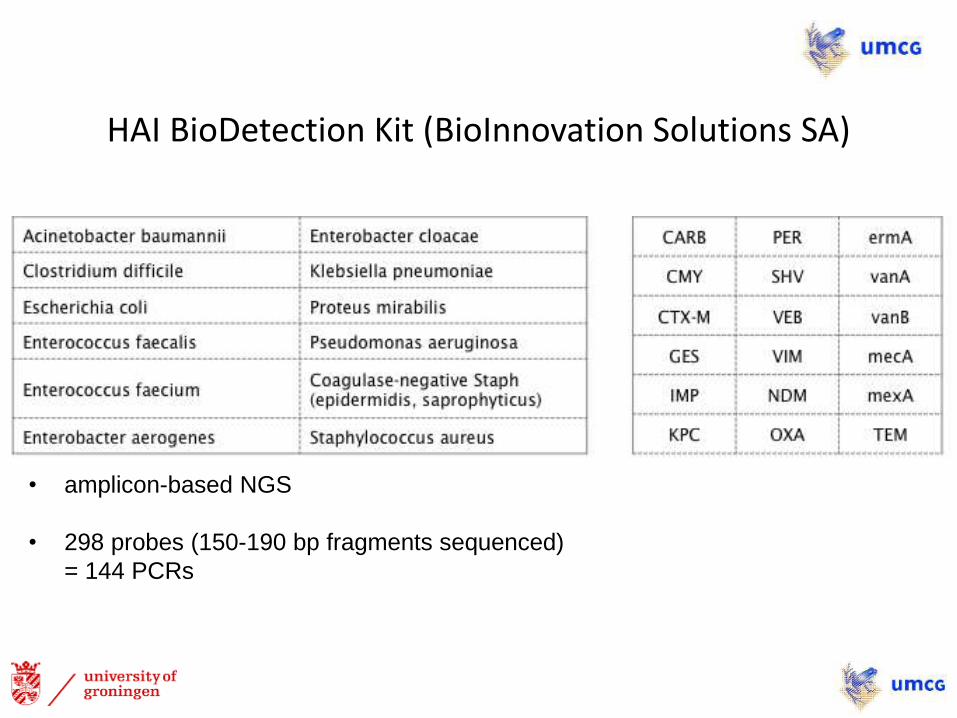
HAI BioDetection Kit (BioInnovation Solutions SA)
• amplicon-based NGS
• 298 probes (150-190 bp fragments sequenced)
= 144 PCRs
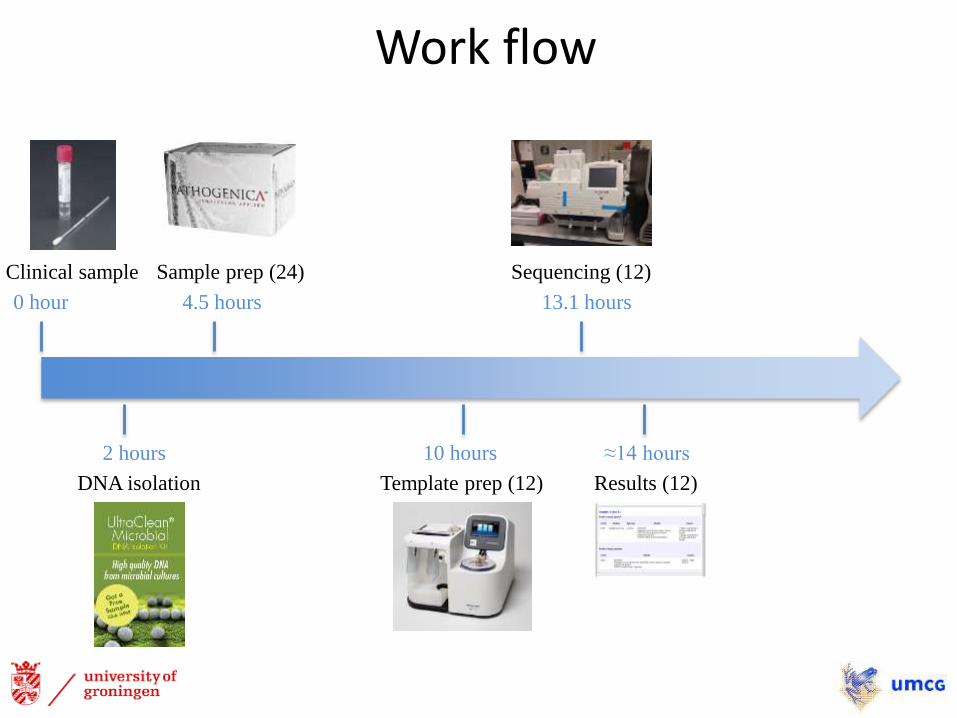
0 hour
Clinical sample
2 hours
DNA isolation
4.5 hours
Work flow
Sample prep (24)
10 hours
Template prep (12)
13.1 hours
Sequencing (12)
≈14 hours
Results (12)
Whole (full) genome sequencing
• Resolve resistance mechanisms
• Find virulence genes
• Outbreak investigation
Klebsiella pneumoniae KPC-outbreak
• KPC-KP ST258
• Hospital and nursing home (July – Dec 2013)
• 6 positive patients
• Extensive environmental contamination
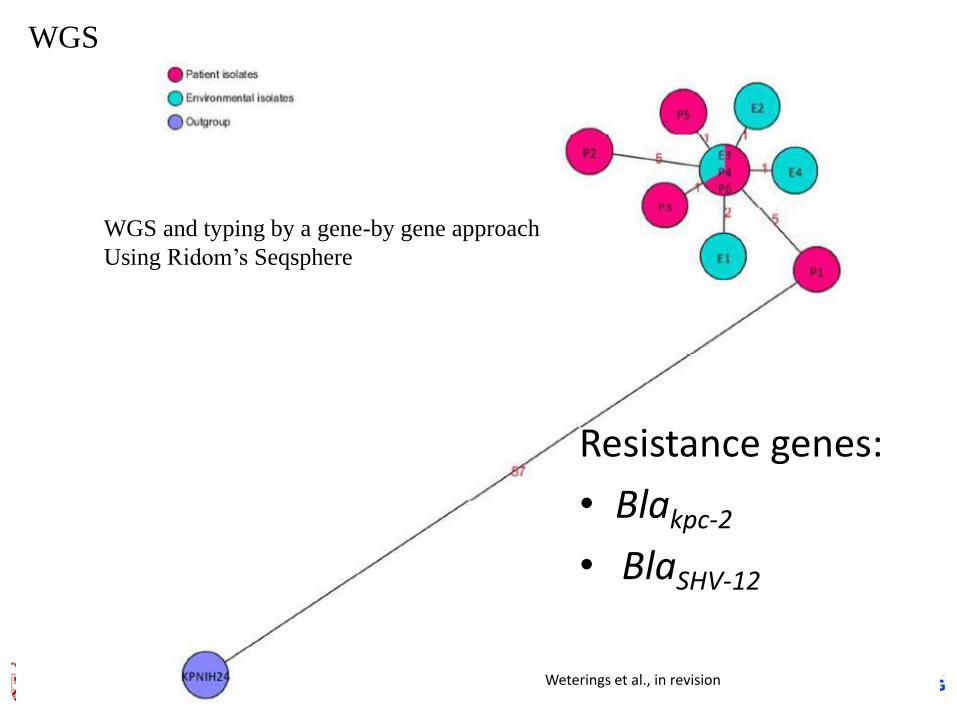
Weterings et al., in revision
WGS and typing by a gene-by gene approach
Using Ridom’s Seqsphere
WGS
Resistance genes:
• Blakpc-2
• BlaSHV-12
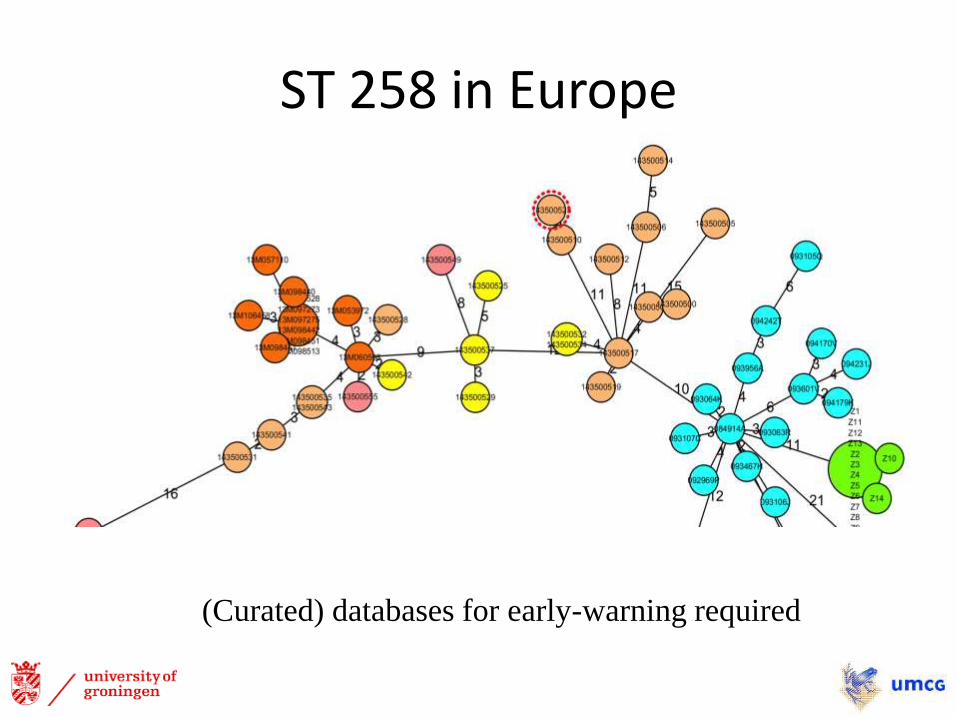
ST 258 in Europe
(Curated) databases for early-warning required
Outbreak in a reha-center
• Between May and September 2012
• CTX-M-15 producing K. pneumoniae
• first occurred in a university hospital and later spread to a nearby rehabilitation center
• sequence type (ST) known to be an epidemic clone
• May 2013 - similar CTX-M-15 producing ST15 K. pneumoniae isolated from a patient admitted to the university hospital
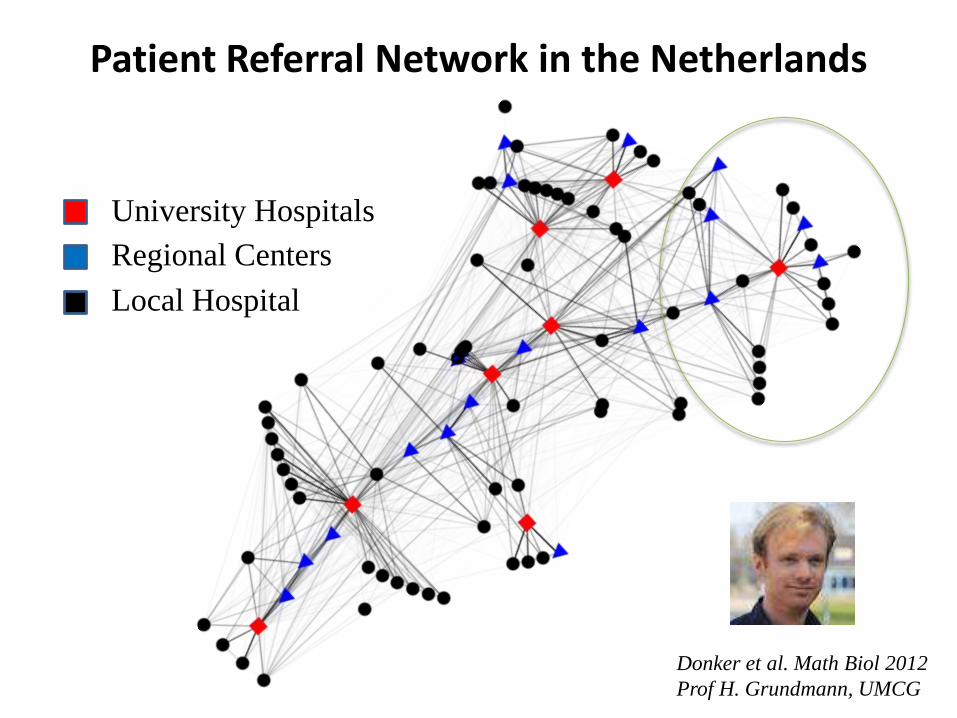
Patient Referral Network in the Netherlands
Donker et al. Math Biol 2012
Prof H. Grundmann, UMCG
University Hospitals
Regional Centers
Local Hospital
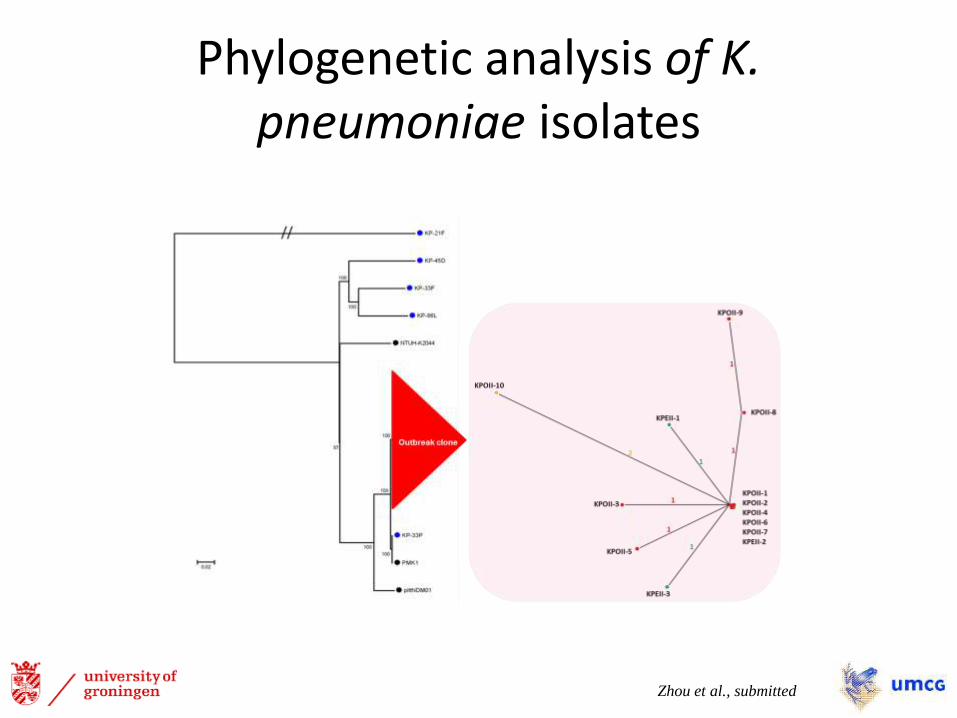
Phylogenetic analysis of K. pneumoniae isolates
Zhou et al., submitted
Combining data
• An epidemiological link was found between the 2012 and 2013 isolates
• Supported by whole-genome sequencing (WGS) only a few single-nucleotide polymorphisms (SNPs) were detected
• WGS analysis of environmental isolates indicates a possible role for the environment in dissemination of outbreak clones.
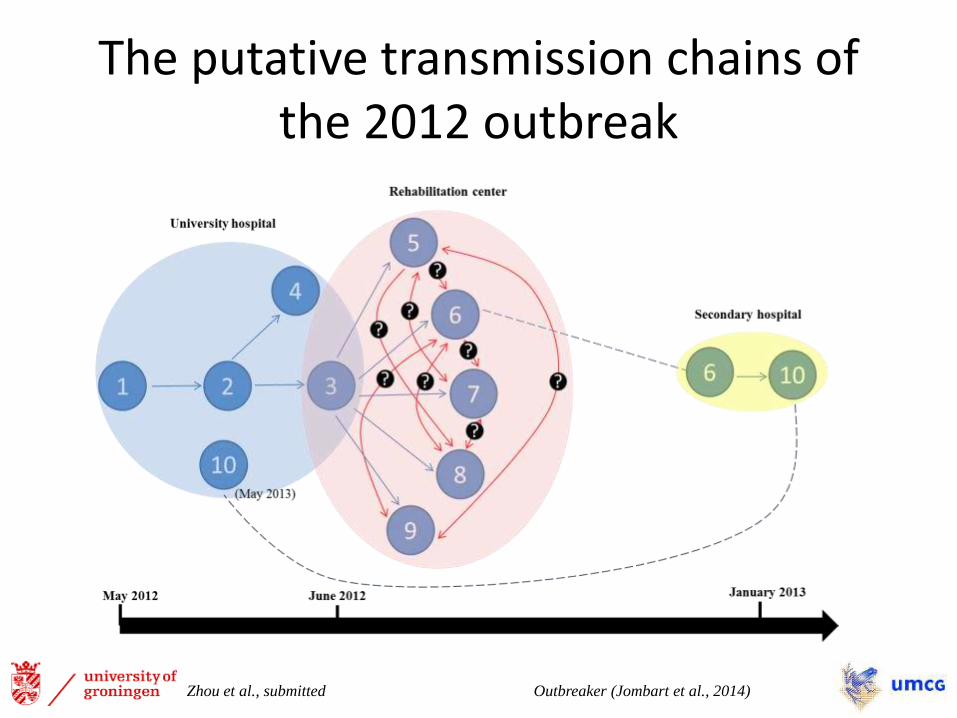
The putative transmission chains of the 2012 outbreak
Outbreaker (Jombart et al., 2014) Zhou et al., submitted
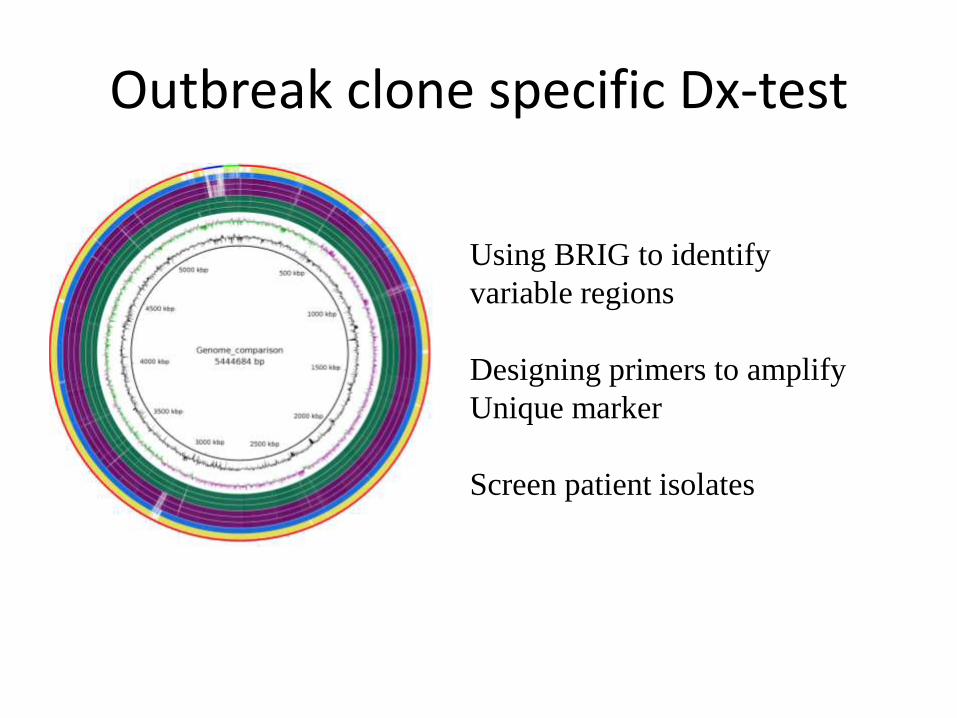
Outbreak clone specific Dx-test
Using BRIG to identify
variable regions
Designing primers to amplify
Unique marker
Screen patient isolates
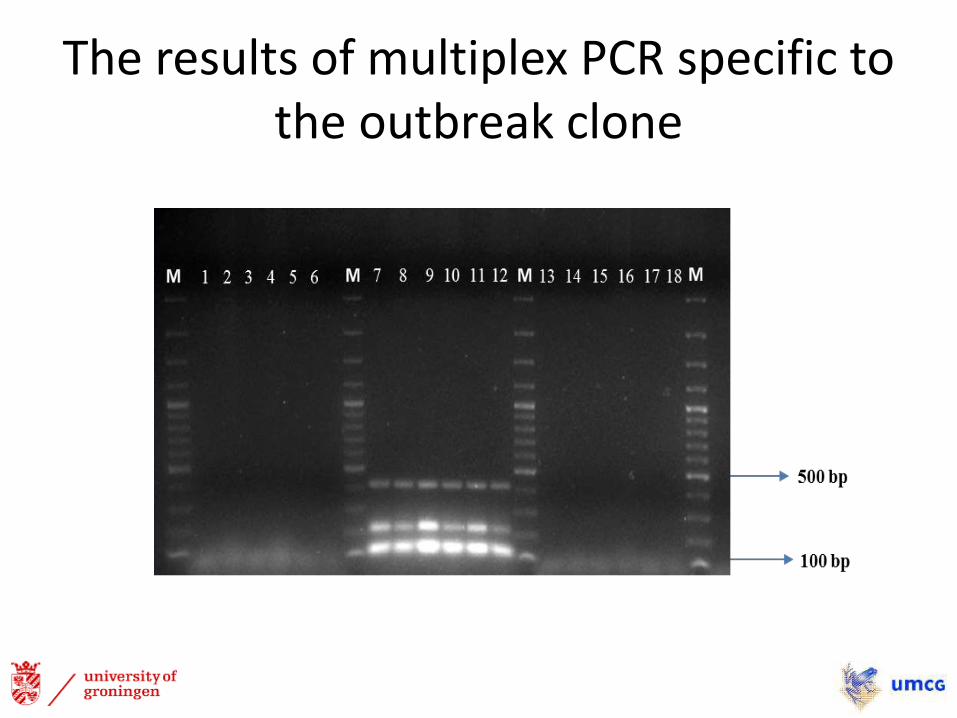
The results of multiplex PCR specific to the outbreak clone
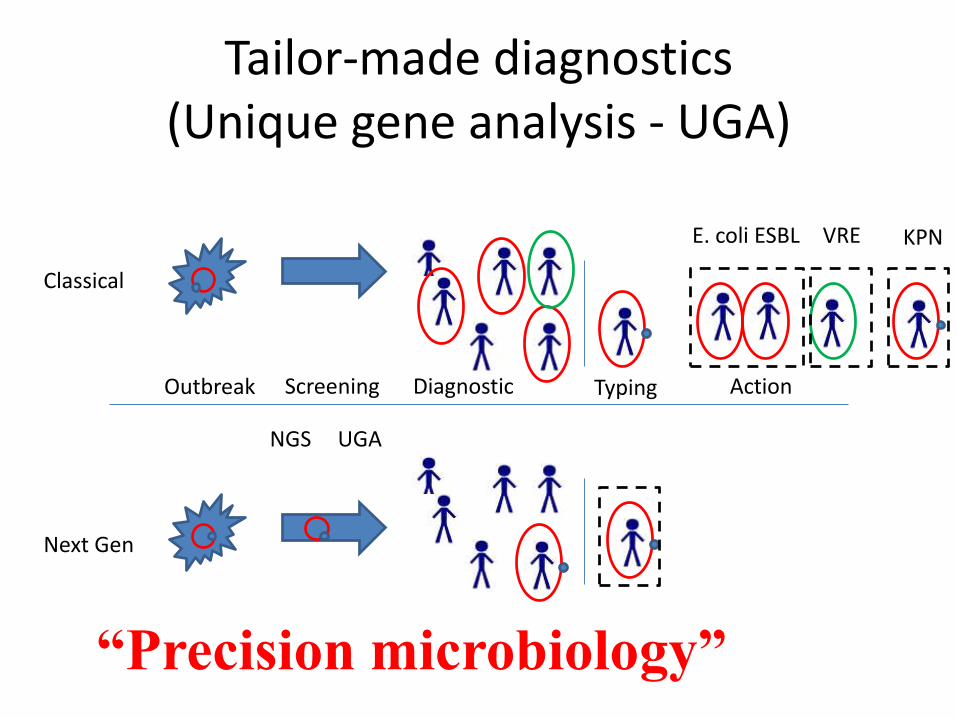
Tailor-made diagnostics(Unique gene analysis - UGA)
Classical
Screening DiagnosticOutbreak Typing Action
E. coli ESBL VRE KPN
Next Gen
NGS UGA
“Precision microbiology”
Conclusions
• WGS allows typing and molecular characterization of the outbreak clone (AMR, virulence)
• The outbreak-specific multiplex PCR facilitated rapid patient screening procedures
• The study emphasizes the necessity of regional collaborations for efficient infection control measures and indicates the potential of WGS for optimized outbreak management in hospital settings
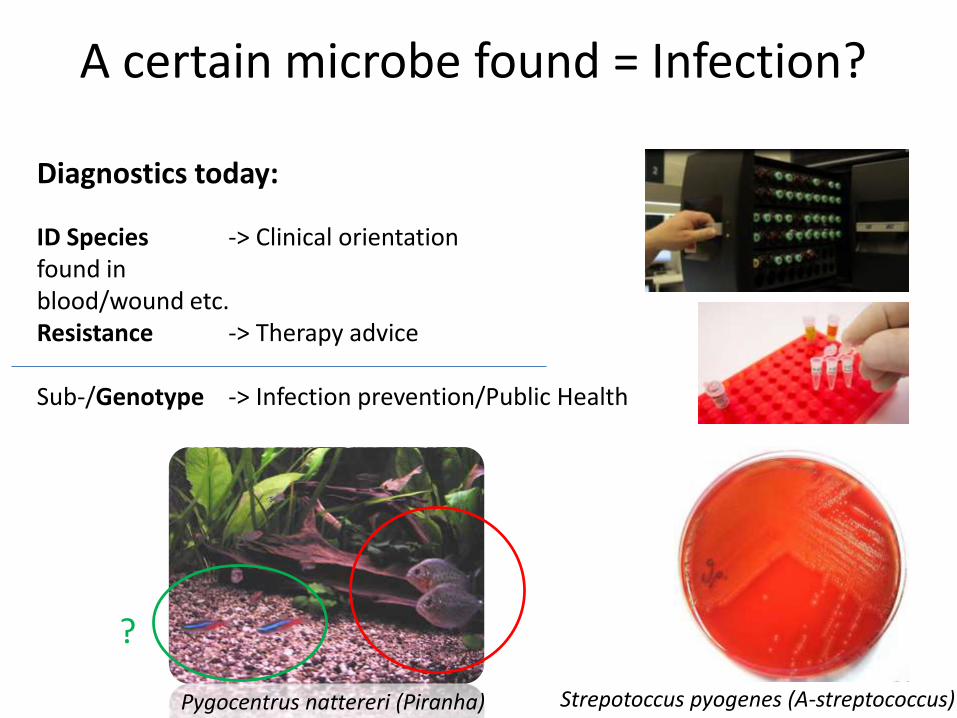
A certain microbe found = Infection?
Diagnostics today:
ID Species -> Clinical orientationfound in blood/wound etc.Resistance -> Therapy advice
Sub-/Genotype -> Infection prevention/Public Health
Pygocentrus nattereri (Piranha) Strepotoccus pyogenes (A-streptococcus)
?
Infectious Disease Staging/Therapy follow-upby diagnostic gene expression profiling
Whole transcriptome sequencing
R
N
AMetagenome sequencing
-> Collaborate with Pathology, Oncology, Genetics
Pharmacomicrobiomics
High-throughput sequencing for everyone ?
Phase 1: more is better
Phase 2: smaller is better
Phase 3: single-molecule
Phase 4: nanopores
“democratization” of next-generation sequencing
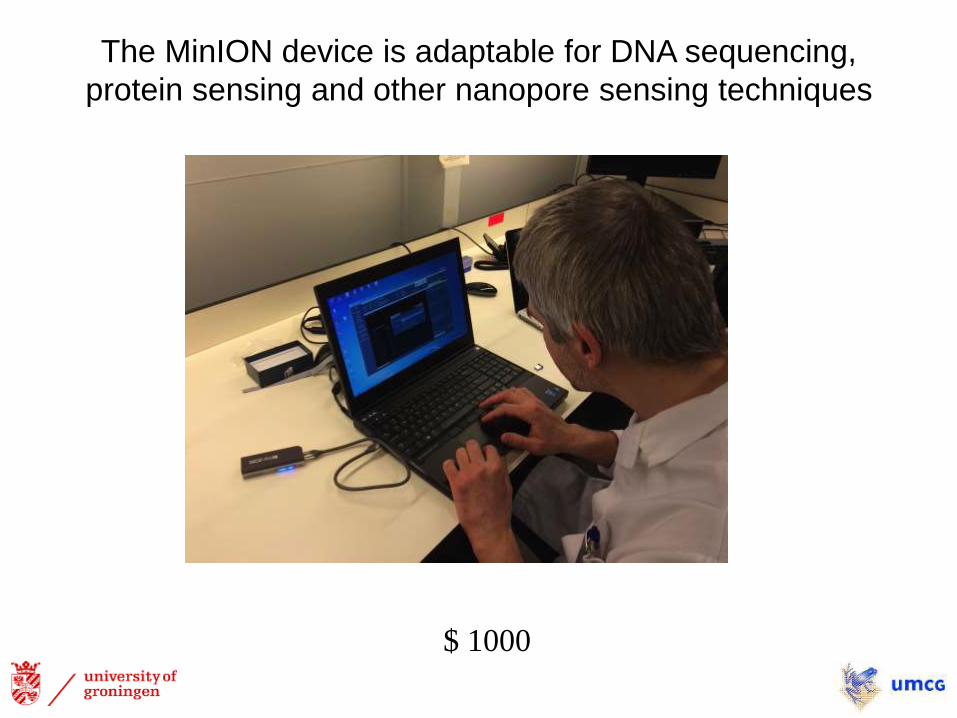
The MinION device is adaptable for DNA sequencing,
protein sensing and other nanopore sensing techniques
$ 1000
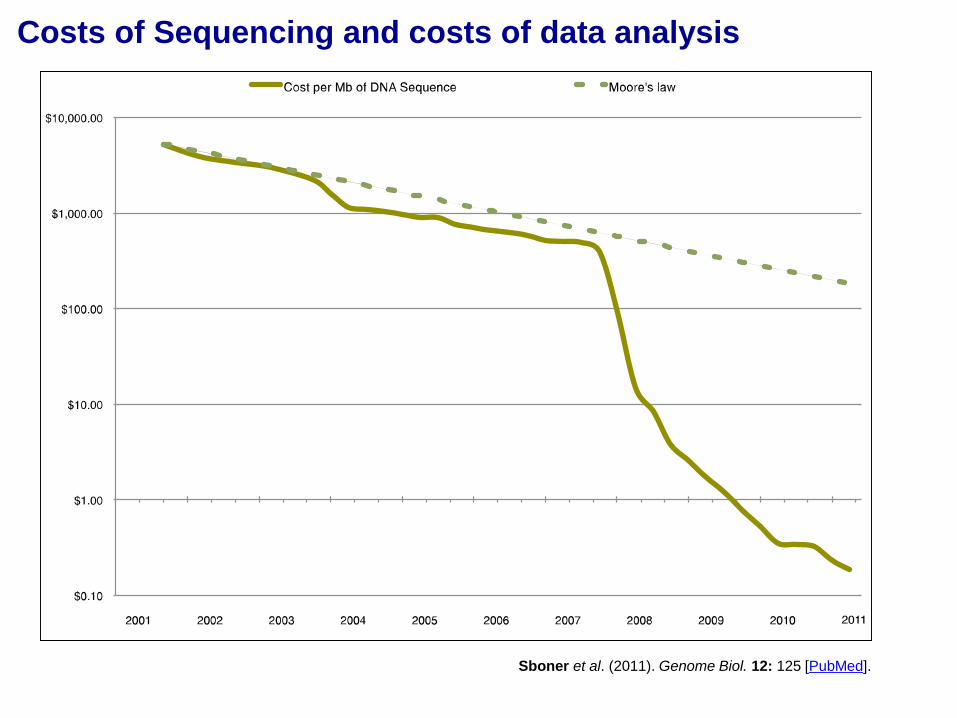
Costs of Sequencing and costs of data analysis
Sboner et al. (2011). Genome Biol. 12: 125 [PubMed].
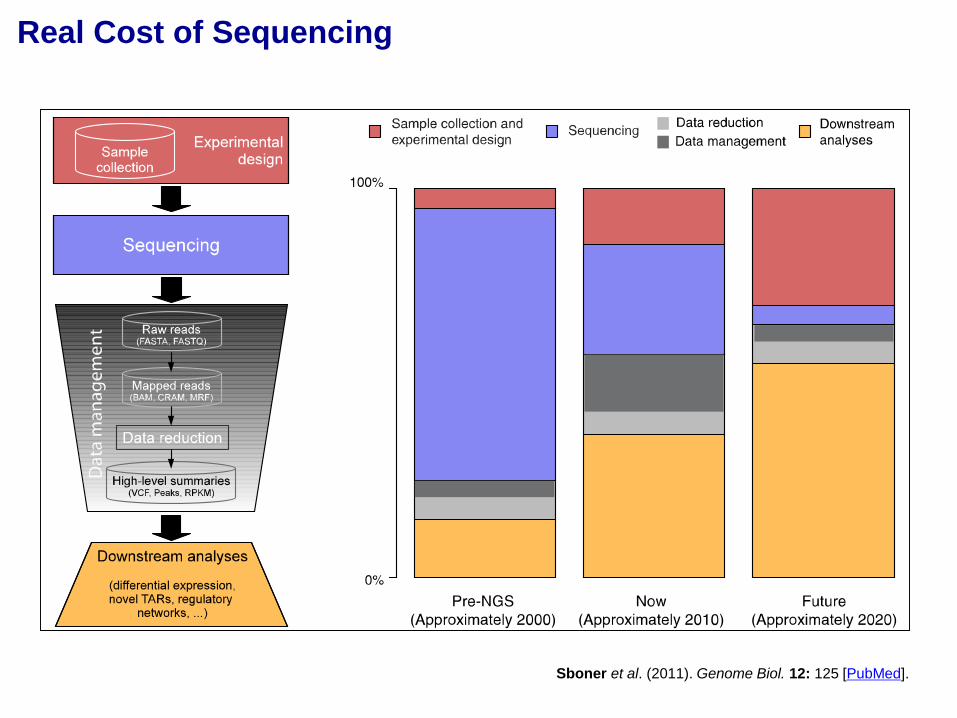
Real Cost of Sequencing
Sboner et al. (2011). Genome Biol. 12: 125 [PubMed].
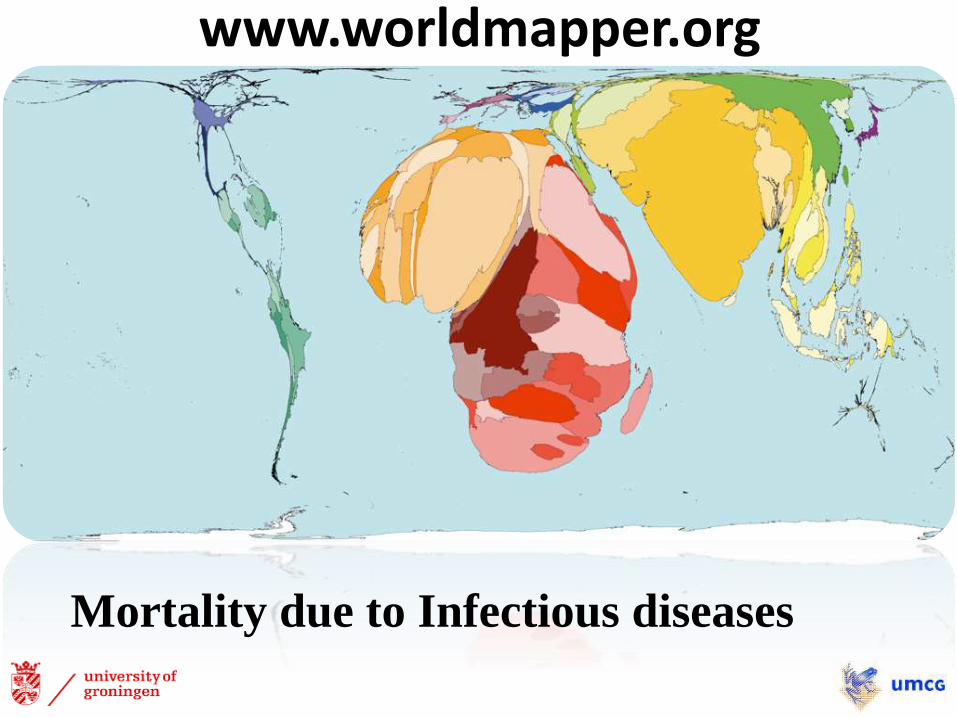
www.worldmapper.org
Mortality due to Infectious diseases
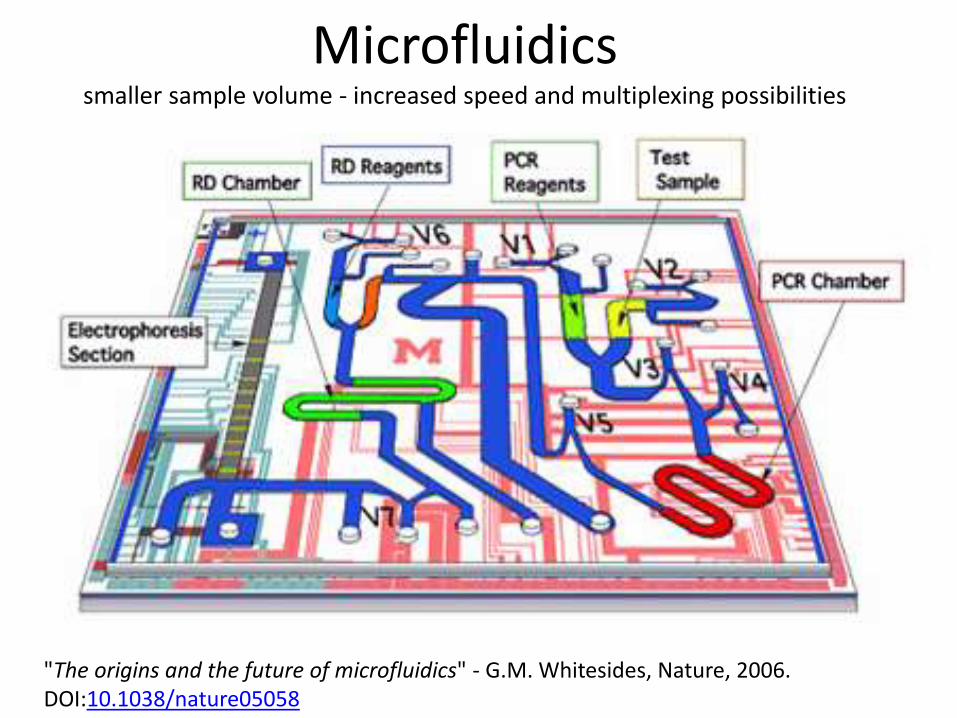
Microfluidics smaller sample volume - increased speed and multiplexing possibilities
"The origins and the future of microfluidics" - G.M. Whitesides, Nature, 2006. DOI:10.1038/nature05058

Microfluid-based point-of-care testing
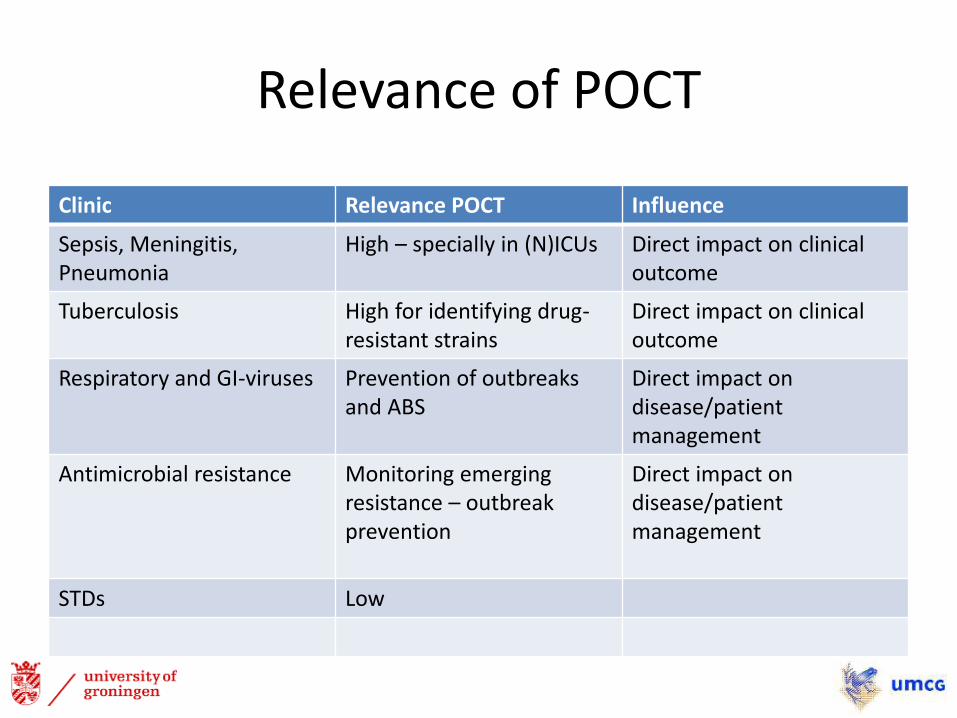
Relevance of POCT
Clinic Relevance POCT Influence
Sepsis, Meningitis, Pneumonia
High – specially in (N)ICUs Direct impact on clinical outcome
Tuberculosis High for identifying drug-resistant strains
Direct impact on clinical outcome
Respiratory and GI-viruses Prevention of outbreaks and ABS
Direct impact on disease/patient management
Antimicrobial resistance Monitoring emerging resistance – outbreak prevention
Direct impact on disease/patient management
STDs Low
POCT in resource-limited settings
• No costly laboratory based systems
• No need for well-trained technicians
• No need for good sample transport networks
• Self-contained quality control
• Fast – same day result
• Linked to a site where clinical decision making is available at the same patient visit

New technological trends• Smart Phone Diagnostics
• μPADs (micro-paper based analytical devices)
Partially from Martinez et al., Anal. Chem. (2010)
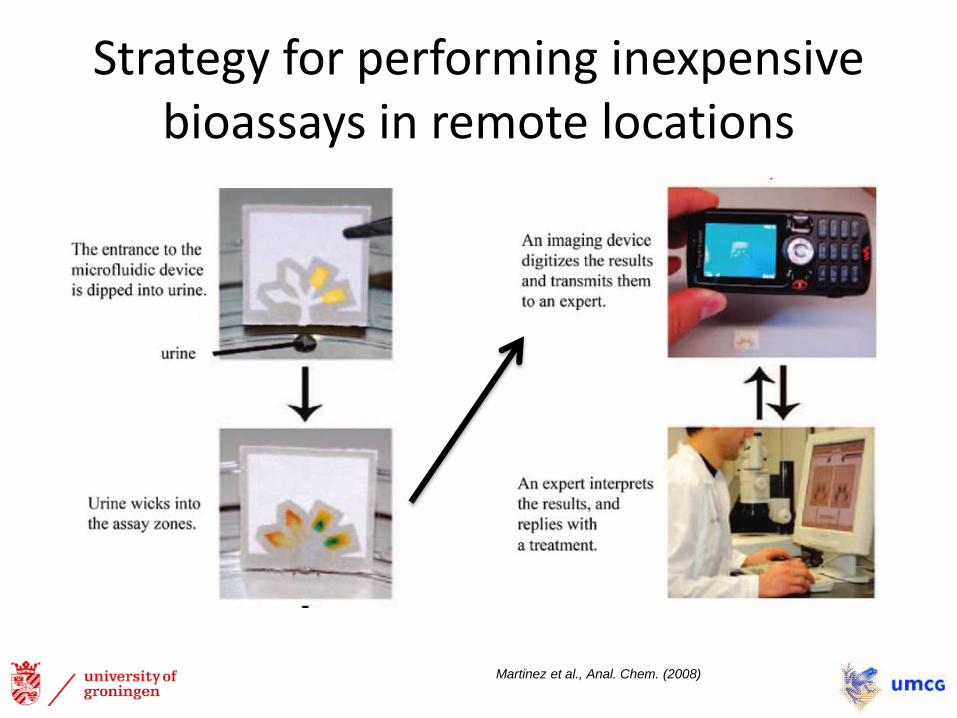
Strategy for performing inexpensive bioassays in remote locations
Martinez et al., Anal. Chem. (2008)
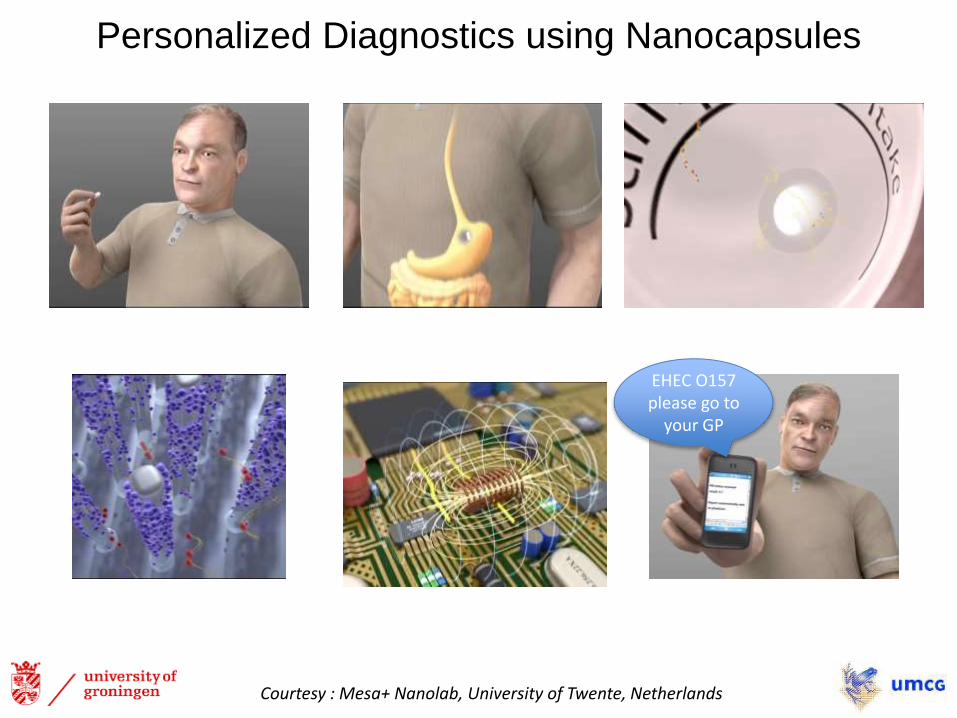
Personalized Diagnostics using Nanocapsules
Courtesy : Mesa+ Nanolab, University of Twente, Netherlands
EHEC O157 please go to
your GP
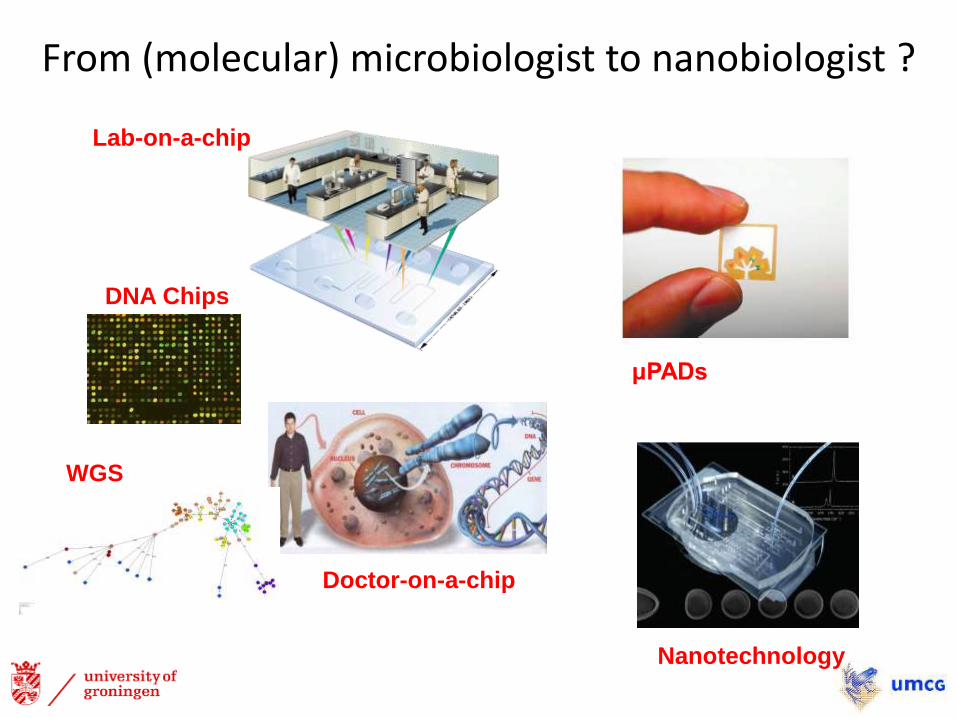
From (molecular) microbiologist to nanobiologist ?
WGS
DNA Chips
Lab-on-a-chip
Doctor-on-a-chip
Nanotechnology
μPADs
Method centered diagnostics
CostTime
Quality
€-hour-systematic100 h * 3€ = 1h * 300€
Cost
Prevention
Quality
Time
Therapy
Diagnostic
Patient-centered diagnostics
MMB mission
Protect patients against infections by
• Fast and precise Dx
• Advising in optimal treatment
• Obtain and share knowledge
in the patient’s interest
Application of on-demand in-house developed and validated
diagnostics: personalized theragnostics
“Voici mon secret. Il est très simple: on ne voit bien qu'avec le cœur.
L'essentiel est invisible pour les yeux.”
Le Petit Prince (1943) by Antoine de Saint Exupéry
Translation: “Here is my secret. It is very simple: It is only with the heart
that one can see rightly; what is essential is invisible to the eye.”

ESCMID Postgraduate Technical Workshop
Capacity-building Workshop: rapid NGS for characterization and typing of resistant gram negative bacilli
October 7th – 9th, 2015, UMCG Groningen, The Netherlands





























