Embed Size (px)
Citation preview
Remote monitoring:
Future Directions for
Research
Marc Lange, Secretary General
Competence Centre
Health Care Authorities
Industry
Health Care Delivery
Citizens/Patient Representative
InnovationAgency
Insurers
Social Care
Dissemination Organisation
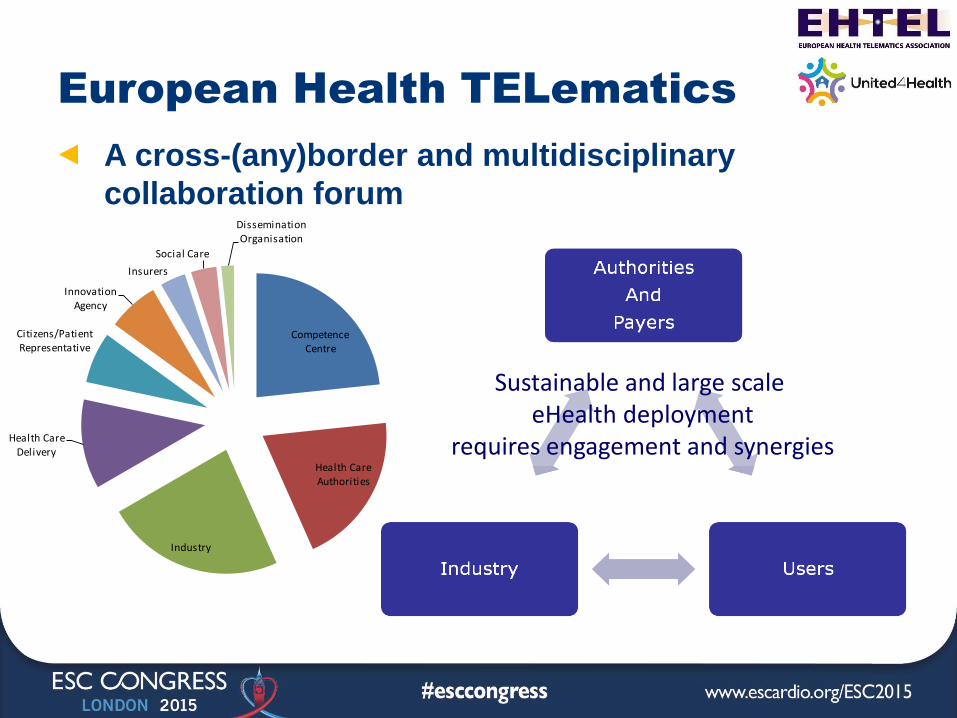
European Health TELematics
A cross-(any)border and multidisciplinary
collaboration forum
Sustainable and large scale eHealth deployment
requires engagement and synergies
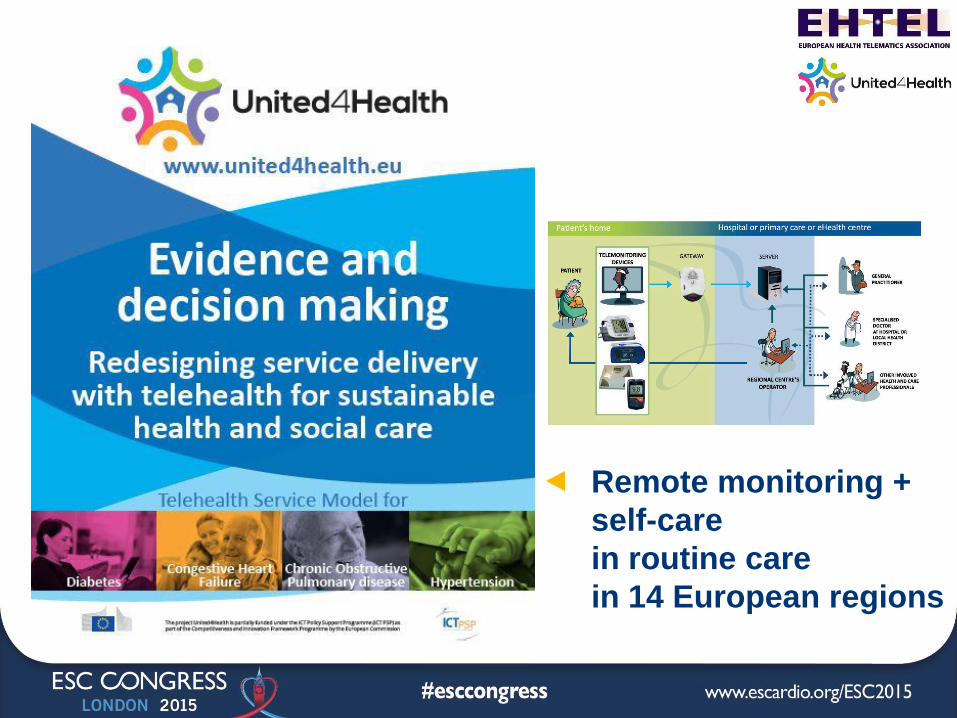
United4Health
Remote monitoring +
self-care
in routine care
in 14 European regions
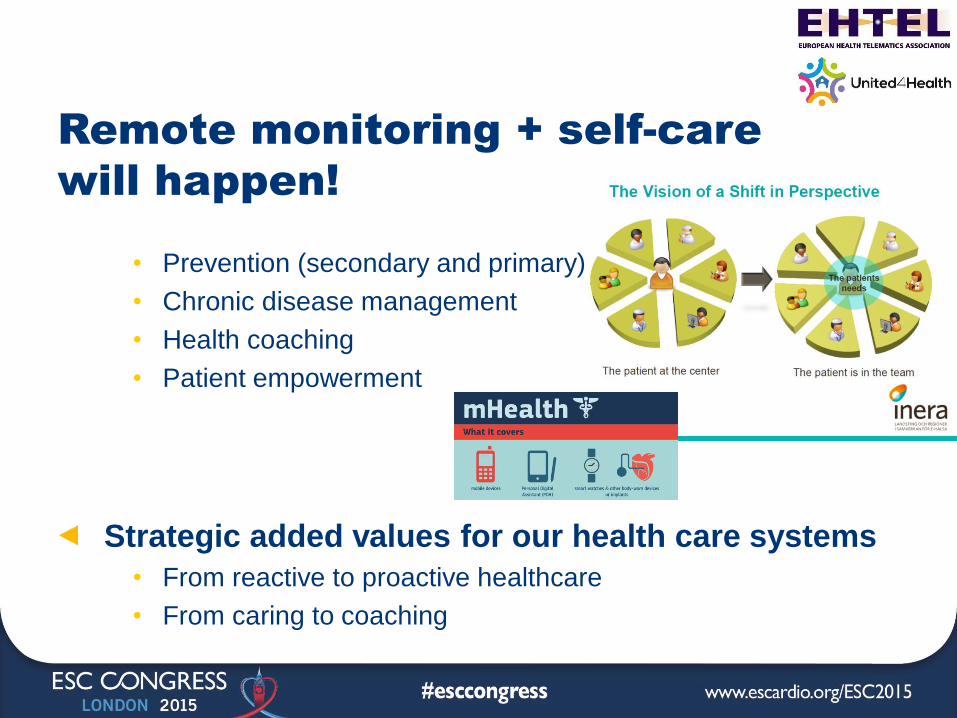
Remote monitoring + self-care
will happen!
• Prevention (secondary and primary)
• Chronic disease management
• Health coaching
• Patient empowerment
Strategic added values for our health care systems
• From reactive to proactive healthcare
• From caring to coaching
The missing evidence
The decision-making dashboard
The deployment in routine care roadmap
Today’s evidence
From an RCT with 21 remote services in 9 Regions Safety and clinical effectiveness
• At least as safe and efficient as regular services
Patient satisfaction and health-related quality of life
• Tendency to improve health-related Quality of Life (SF36)
• Very positive Patients (SUTAQ) in almost all pilots
▲ Costs per patient or in efficiency gains, no reduction, possibly because
• Technology market still to expensive
• Sub-optimisation of the organisation of care
• Inadequate scaling of the service
Lessons learned: the impact of
non-clinical parameters (1)
Why the service is considered for roll-out
• The values of the health care system
• Its objectives with the service
What technology is being used
• Connectivity, device ownership, sophistication
Who will benefit from it
• Enrolment process, eligibility criteria
Where the service is running
• The organisations and the workforce profile in charge
Model for Assessment of Telemedicine (MAST)
Lessons learned: the impact of
non-clinical parameters (2)
How the service is designed
• With a focus on primary or secondary care setting
• Limited to health care setting or with the implication of the
social care sector
When the service is being studied,
• The cost of the technology will decrease because of the
market and the opportunities to mutualise the cost of the
supportive infrastructure
+
Summative or formative assessment
Model for Assessment of Telemedicine (MAST)
Directions for Research?
Evidence on the relationship between outcome and environment
• What is the profile of the patients that can benefit the most?
• What are the best technological options, for what type of
patients, having in mind the “moving target” aspects of
technology?
• How to organise the responsibility/liability chain?
• How best to obtain efficiency gains?
• How to address the fact that nurses will often be the first line of
response?
• …
(Evidence-based health care)
Clinical evidence
• Based on RTC
(the gold standard)
• Summative assessment
“Clinicians [may be] ready
to believe that there is an
objective determinable
“right answer” to research
questions.”1
Management evidence
• Based on use cases,
lessons learned …
• Formative assessment
“Managers may, quite
rightly, view the results of
research are more
subjective, and contingent
on the context and on the
characteristics of the
researchers themselves” 2
1&2. Walshe K. and Rundall TG. – 2001 – Evidence-based Management: from Theory to Practice in Health
Care (Milbank Q. 2001; 79(3): 429-57, IV-V.)
The missing evidence
The decision-making dashboard
The deployment in routine careroadmap
(Decision making)
Clinical decisions
• Decision-support systems
• Many decisions, individual
cases, in a short time frame
• Often made individually
• In a relatively unconstrained
context
• Often with immediate
feedback
Management decisions
• Heterogeneous processes,
including intuition
• Fewer but larger decisions
in a longer time frame
• Made in concert with others
• Constrained by resources,
policies and procedures,
stakeholders’ views …
• With results more difficult to
discern
Walshe K. and Rundall TG. – 2001 – Evidence-based Management: from Theory to Practice in Health Care
(Milbank Q. 2001; 79(3): 429-57, IV-V.)
Lessons learned:
the need for action research1
For evidence-based tools for decision-making in healthcare
• The results of the research need to be action-oriented and
accessible to managers
• The question for the research need to be strategic
• A match is required between the timing of the research and
the decision-making
1; Walshe K. and Rundall TG. – 2001 – Evidence-based Management: from Theory to Practice in Health Care
(Milbank Q. 2001; 79(3): 429-57, IV-V.)
Directions for Research?
Strategic management and entrepreneurial tools adapted to healthcare and remote monitoring + self-care
• Maturity modelling
for assessing the readiness of an environment to host an
innovative services and identify strategic actions to undertake
• Service Innovation Governance modelling,
for guiding the creation of innovative services
• Business modelling,
for assessing the conditions for sustainable remote monitoring
• Socio-economic evaluation, Cost & Benefit Analysis
for measuring the potential for impact of an innovative service
• …
The missing evidence
The decision-making dashboard
The deployment in routine careroadmap
(Deploying)
In Pilot environment
• Minimal organisational
changes
• Temporary setting
• Selected patients
• Project staffing
• Project funding
In Routine care
• Service redesign
with necessary
organisational changes
• There to stay
• Patient inclusive
• Regular staffing
• Healthcare system funding
U4H
Initial lessons learned (1)
Organisation
• The whole spectrum of healthcare stakeholders need to be
involved and engaged, from patients through to politicians …
Culture
• Local benefits by local ownership of local problems
• Telehealth is to be seen as a journey, not as a destination
Conclusions
• In routine care = Service redesign = Change management
U4H
Initial lessons learned (2)
Technology @ scale
• Lack of connectivity @ scale creates access inequalities
Procurement and interoperability
• Procurers need solutions that are proven to work now
• Local challenges with interoperability and integration in
primary care
Conclusions
• KISS - Keep It (the technology) Simple and Stable
• Do not underestimate the tension between
standardisation and legacy
Directions for Research?
Evidence-based guidelines and tools for helping the demand-side on
• Leadership for ICT-based innovation in healthcare
• Public Procurement of Innovative solutions in healthcare
• Managing change in a healthcare service re-design context
• Implementing legal, security, safety rules (including compliance
check lists)
• Accreditation tools for remote monitoring + self-care
(e.g. health apps for clinical practice) and
• …
Summary
Evidence on how to design remote monitoring + self-care in a given environment
Action research for evidence-based
decision-making
Guidelines and tools for helping the demand-side
Happy to answer any
questions
Marc Lange
Secretary general
EHTEL Associationrue de Trèves 49-51,
B-1040 Brussels Belgium
Tel: +32 (0)2 230 15 34
Fax: +32 (0)2 230 84 40
Mobile: +32 (0)475 27 71 45
www.ehtel.eu
www.united4health.eu
www.renewinghealth.eu
www.telemedicine-momentum.eu