Embed Size (px)
Citation preview

Real-Effectiveness Medicine
Antti Malmivaara, MD, PhD, Chief Physician
Centre for Health and Social Economics

Real-effectiveness medicine - background
All activities within medicine (education, clinical work, leadership, research) have an ultimate aim to advance the health and wellbeing of everyday patients in ordinary health care settings.
15.12.2014 Malmivaara A; CHESS/THL 2
Malmivaara A. Real-Effectiveness Medicine – pursuing the best effectiveness in the ordinary
care of patients. Annals of Medicine 2013;45:103-106.

Real-effectiveness medicine is a systematic undertaking which utilises information and skills on four levels for the pursuit of best effectiveness of patient care in the real-world setting. The four levels are:
1. Clinical know-how
2. Up-to-date scientific evidence
3. Documentation of performance
4. Benchmarking between providers
Real-effectiveness medicine - definition
15.12.2014 Malmivaara A; CHESS/THL 3
Malmivaara A. Real-Effectiveness Medicine – pursuing the best effectiveness in the ordinary
care of patients. Annals of Medicine 2013;45:103-106.

Real-Effectiveness Medicine
15.12.2014 Malmivaara A; CHESS/THL 4
Malmivaara A. Real-Effectiveness Medicine – pursuing the best effectiveness in the ordinary
care of patients. Annals of Medicine 2013;45:103-106.

The performance information in REM should be disease specific:
what is the demographic and clinical profile of patients having a particular disease, how are they treated, and what are the outcomes of the treatment at one’s own health care unit.
The question posed is similar to the PICO in RCTs: patients, intervention, comparison intervention, and outcome.
The PICO data from ordinary care should be compared with results of systematic reviews and recommendations from clinical practice guidelines, as well as with peers (benchmarking) to assess the appropriateness of the treatments and treatment processes.
When baseline confounding can be adequately controlled, even differences in treatment outcomes between different units treating similar patients or providing similar interventions (e.g. particular surgical procedures) can be compared.
The PICO based information
15.12.2014 Malmivaara A; CHESS/THL 5
Malmivaara A. Real-Effectiveness Medicine – pursuing the best effectiveness in the ordinary care of
patients. Annals of Medicine 2013;45:103-106.

Real-Effectiveness Medicine
15.12.2014 Malmivaara A; CHESS/THL 6
Malmivaara A. Real-Effectiveness Medicine – pursuing the best effectiveness in the ordinary
care of patients. Annals of Medicine 2013;45:103-106.

Randomised controlled trials (RCTs) provide the least biased information of the efficacy of medical interventions and creates the basis for systematic reviews on effectiveness of interventions.
However, RCTs have two major limitations. They mostly assess effectiveness of interventions in ideal settings (ideal patients and most competent practitioners) and they focus on specific interventions rather than considering how effective is the optimal clinical pathway (crucial for overall effectiveness).
For these reasons there is also a need for valid data on actual performance in the routine settings, particularly as all educational, research and leadership activities in medicine are intended to advance care of ordinary patients.
Real-effectiveness medicine – why?
15.12.2014 Malmivaara A; CHESS/THL 7
Malmivaara A. Real-Effectiveness Medicine – pursuing the best effectiveness in the ordinary care of patients.
Annals of Medicine 2013;45:103-106.

15.12.2014 Malmivaara A; CHESS/THL 8
Bench-marking
Quality
Scientific evidence
Clinical expertise
Real-Effectiveness Medicine

REM – Competence (level 1)
• Effective, efficient (cost-effective) and equal services are unimaginable without staff competence
• Nearly all available evidence on effectiveness and efficiency is based on randomized trials in circumstances where medical competency has been very good
• There is evidence that effectiveness in ordinary care is less than that found in trials undertaken for ideal groups of patients and treated by the very best experts
15.12.2014 Malmivaara A; CHESS/THL 9

The Royal Collage of Physicians and Surgeons of Canada framework for competence
15.12.2014 Malmivaara A; CHESS/THL 10

REM – Competence – cont’d
• For increasing staff competency, scientific evidence provided by the BEME Collaboration can be utilized. The BEME Collaboration, established in 1999, strives towards evidence-based education. It has published over 20 systematic reviews, along with guidance books based on these reviews (http://www.bemecollaboration.org/).
15.12.2014 Malmivaara A; CHESS/THL 11

15.12.2014 Malmivaara A; CHESS/THL 12
Bench-marking
Quality
Scientific evidence
Clinical expertise
Real-Effectiveness Medicine

REM – Evidence (level 2)
• The second level of REM consists of the utilization up-to-date of high quality scientific evidence, particularly from RCTs and systematic reviews, health technology assessment (HTA) reports, and clinical guidelines.
• Also other scientific and patient-based information (e.g. on diagnostic tests and patients’ values and preferences) according to the EBM (Evidence Based Medicine) framework should be used
15.12.2014 Malmivaara A; CHESS/THL 13

Hierarchy of Evidence (Guyatt G.
2005)
• Meta-analysis of RCTs
• systematic review of RCTs
Individual RCT
Observational studies
patient-important outcomes
Basic research test tube, animal, human physiology
Clinical experience

REM – Evidence – cont’d
• When summarizing the available evidence in systematic reviews, the quality of evidence in the original studies should be based on
– the degree of internal validity of each study
– the reproducibility (consistency) of the findings across clinically homogenous studies
-> inferences on methodologically high quality studies.
15.12.2014 Malmivaara A; CHESS/THL 15

REM – Evidence – cont’d
• Systematic reviews provide very little data applicable to the disadvantaged patient groups.
• However, a recent recommendation on how to include these patient groups in systematic reviews has been launched (Welch V et al. PLos Med 2012).
15.12.2014 Malmivaara A; CHESS/THL 16
Malmivaara A. On decreasing inequality in a cost-effective way. BMC Health
Serv Res. 2014;14:79.

15.12.2014 Malmivaara A; CHESS/THL 17
Bench-marking
Quality
Scientific evidence
Clinical expertise
Real-Effectiveness Medicine

REM – Quality/Performance (level 3) • One of the largest challenges in modern
medicine is how to solve the problem of nearly lack of knowledge on what happens for the ordinary patient in ordinary health care
• Validly documented data on patient characteristics, interventions and outcomes for each specific diagnosis are needed for assessment and improvement of quality of services.
• Assessment and improvement of performance throughout the clinical pathway are needed.
15.12.2014 Malmivaara A; CHESS/THL 18

The clinical pathway (Peltola et al 2011*)
Admission to ward A
Treatments in ward A
Admission to ward B
Discharge to another hospital
Outpatient care
Medication purchase
The treatment chain
First hospital episode
time
Discharge home
15.12.2014 Malmivaara A; CHESS/THL 19
*Peltola, M., Juntunen, M., Häkkinen, U., Rosenqvist, G., Seppälä, T. T., & Sund, R. (2011). A methodological
approach for register-based evaluation of cost and outcomes in health care. Annals of Medicine, 43, S4-S13

REM – Quality/Performance – cont’d
• The performance indicators should be those (i) for which there is scientific evidence that a particular change in the care process leads to improved outcomes, (ii) they capture whether the process is indeed provided, (iii) the process indicator lies sufficiently near the important outcomes, and (iv) there is low or no risk of inducing adverse consequences.
15.12.2014 Malmivaara A; CHESS/THL 20
Chassin, M. R., Loeb, J. M., Schmaltz, S. P., & Wachter, R. M. Accountability measures - using
measurement to promote quality improvement. New England Journal of Medicine 2010; 363:
683-688

REM – Quality/Performance – cont’d
• Standardized use of performance indicators among different health care organisations makes benchmarking between peers possible.
• For performance assessment both national registries based usually on administrative data and clinical registries are needed.
15.12.2014 Malmivaara A; CHESS/THL 21

REM – Quality/Performance – cont’d
• Administrative registries may provide follow-up of patients on an individual level throughout the treatment chain.
• Nationwide administrative registries can also be very powerful in bringing evidence that has high generalizability.
– For example two studies have showed that up-taking of new hip and knee endoprothesis models lead to 50% and 30% of heightened risk of reoperation for the first 15 patients in the hospital, respectively (Peltola et al. 2013)
15.12.2014 Malmivaara A; CHESS/THL 22

REM – Quality/Performance – cont’d
• Electronic patient record systems will bring new opportunities for quality improvement. But: development of patient record systems needs definitions and classifications, which should be done as teamwork between researchers and clinicians.
• Standardized documentation of health care units’ performance for each patient group ensuring the quality of the registers is a huge task, which needs sufficient resources.
15.12.2014 Malmivaara A; CHESS/THL 23

15.12.2014 Malmivaara A; CHESS/THL 24
Bench-marking
Quality
Scientific evidence
Clinical expertise
Real-Effectiveness Medicine

REM – Benchmarking (Level 4)
• The fourth level includes benchmarking between treatment providers = learning from the best practices of peers. Again, information of patient characteristics, diagnostic procedures and treatments, and of the outcomes is needed for the comparisons between providers and also for comparisons over time.
• The primary focus in benchmarking is between the treatment processes – how well these concord with current scientific evidence.
• If baseline imbalances between patients treated by different providers can be satisfactorily adjusted for, also comparisons based on treatment outcomes can be made
15.12.2014 Malmivaara A; CHESS/THL 25

REM – Benchmarking – cont’d
• Benchmarking should assess quality of treatment processes, effectiveness, safety and costs of services for well defined patient groups taking.
• Also the disadvantaged persons must be taken into consideration. The lost opportunities for providing effective and safe services for the disadvantaged patient groups also lessen cost-effectiveness of the health care systems.
• The ACS-NSQIP program produces periodic assessments of high and low outlier institutions, self-assessment tools for the centers, structured visits for the assessment of data quality and performance, and dissemination of best practices.
15.12.2014 Malmivaara A; CHESS/THL 26

15.12.2014 Antti Malmivaara/CHESS/THL
Häkkinen U, Malmivaara A. [Guest editors]. The PERFECT project: measuring performance of
health care episodes. Ann Med 2011;43(Suppl1)

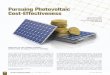
PERFECT = PERFormance, Effectiveness and Cost of Treatment episodes
To develop research methods for register-
based measurement of cost-effectiveness of
treatment episodes.
to create a comparative database that allows
the treatments and their costs and outcomes to be
compared between hospitals, hospital districts,
regions and population groups
15.12.2014 Malmivaara A; CHESS/THL 28

Description of the PERFECT-Project
BASIC REPORTS
THL Hospital discharge register,
Hospital productivity
(Benchmarking)
database
SOCIAL INSURANCE
INSTITUTION Register on Health and
Social Benefits
STATISTICS OF FINLAND Cause-of-Death Register
OTHER
REGISTERS Implant Register on
Orthopaedic Endoprostheses,
Hospitals patient registers
RESEARCH
PERFECT DATA BASE
F
E
E
D
B
A
C
K
15.12.2014 Malmivaara A; CHESS/THL 29

Results – hip fracture indicators in PERFECT
Hip fracture Proportion of patients who have waited for
surgery more than 48 hours
Proportion of patients who have (returned home and have) bisphosphonate treatment within 90 days
Space-diagrams showing the proportions of the deceased, and of those who are in hospitals or in residences for the elderly or of those who have returned home and during 0-365 days
15.12.2014 Malmivaara A; CHESS/THL 30

Proportion of hip fracture patients (%) who have waited for surgery more than 48 hours in Finnish hospitals.
Sund et al Finnish Medical
Journal 2011;66:1655-1662.
15.12.2014 Malmivaara A; CHESS/THL 31

State diagram describing hip fracture treatment at
one Finnish hospital (A) in 2005. Red denotes to
being dead, yellow being at home.
Sund et al. Ann Med
2011;43 (Suppl 1):S39-S46
15.12.2014 Malmivaara A; CHESS/THL 32

State diagram describing hip fracture treatment
at one Finnish hospital (B) in 2005. Red denotes
to being dead, yellow being at home.
Sund et al. Ann Med
2011;43 (Suppl 1):S39-S46
15.12.2014 Malmivaara A; CHESS/THL 33

50
60
70
80
90
100
Risk adjusted figures (95 % CI’s) for the Finnish hospitals showing percentages of hip fracture patients living at home within 120 days after hospitalization.
15.12.2014 Malmivaara A; CHESS/THL 34

15.12.2014 Malmivaara A; CHESS/THL 35
Comparing ischaemic stroke in six European countries. The EuroHOPE register study.
Malmivaara A1, Meretoja A2,3, Peltola M1,
Numerato D4, Heijink R5, Engelfriet P5, Wild
SH6, Belicza É7, Bereczki D7, Medin E8, Goude
F8, Boncoraglio G9, Tatlisumak T2, Seppälä T1,
Häkkinen U1.
European Journal of Neurology, in press

15.12.2014 Malmivaara A; CHESS/THL 36
Background We assessed the incidence of
hospitalisations, treatment, and case-fatality of ischaemic
stroke utilizing a comprehensive multi-national database
to attempt to compare the health care systems in six
European countries; aiming also to identify the limitations
and make suggestions for future improvements in the
between-country comparisons.
Methods National registers of hospital discharges for
ischaemic stroke identified by codes 433-434 (ICD-9) and
code I63 (ICD-10), medication purchases, and mortality
were linked at the patient level in each of the participating
countries and regions: Finland, Hungary, Italy, the
Netherlands, Scotland, and Sweden. Patients with an
index admission in 2007 were followed for one year.
Comparing ischaemic stroke in six European countries.

15.12.2014 Malmivaara A; CHESS/THL 37
Results We identified 64,170 patients with a disease
code for ischaemic stroke. The number of patients
registered per 100 000 European standard population
ranged from 77 in Scotland to 407 in Hungary. Large
differences were observed in medication use. The age-
and sex-adjusted all-cause case-fatality among
hospitalised patients at one year from stroke was highest
in Hungary 31.0% (95% CI 30.5– 31.5). Regional
differences in age and sex adjusted one-year case-fatality
within countries were largest in Hungary (range: 23.6% to
37.6%), and smallest in the Netherlands (20.5% to
27.3%).
Comparing ischaemic stroke in six European countries.

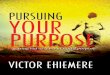
Regional variation in mortality, stroke
• Age- and sex-adjusted one-year mortality by regions, ischaemic stroke in 2008
EuroHOPE final seminar, 8th of April, Stockholm. Contact: [email protected] 38
Comparing ischaemic stroke in six European countries.

• Conclusions It is feasible to link population-wide register data among European countries to describe incidence of hospitalisations, treatment patterns, and case-fatality of ischaemic stroke on a national level. However, the coverage and validity of administrative register data for ischaemic stroke should be developed further, and population-based and clinical stroke registers created to allow better control of case-mix.
15.12.2014 Malmivaara A; CHESS/THL 39
Comparing ischaemic stroke in six European countries.

Conclusions
1. Good competency of health care staff is the basis for effective patient care
– without competency, effectiveness and efficiency (cost-effectiveness) are not possible.
– ability to provide equal high quality services also to the vulnerable patient groups depends also on the competency of professionals.
– Efforts to increase staff competency (at individual, team and organizational levels) should be the foremost priority of all health care organizations.
15.12.2014 Malmivaara A; CHESS/THL 40

Conclusions – cont’d
2. The Evidence Based Medicine (EBM) framework should be utilized in all activities.
• Scientific evidence, especially from high quality randomized trials and systematic reviews should be considered, and whenever appropriate lead to changes in clinical practice – also abandoning existing treatments when new compelling evidence shows that they are not beneficial to the patients.
• The main burden of proving effectiveness of interventions should lie on those practitioners and scholars who use or mandate the treatments.
15.12.2014 Malmivaara A; CHESS/THL 41

Conclusions – cont’d
3. Quality of the treatment throughout the clinical pathways should be documented, and this information used for continuous improvement of treatment processes to advance effectiveness and efficiency of care, also among the disadvantaged patient groups.
• The main categories of quality indicators are structural (denoting to the quality of the infrastructure where the work is undertaken), process (denoting to the quality of the diagnostic, treatment and rehabilitation activities) and outcome (denoting to effectiveness compared to peers treating similar patients).
15.12.2014 Malmivaara A; CHESS/THL 42

Conclusions – cont’d
4. Benchmarking with peer units treating similar patients should be exercised regularly to learn from the best practices.
15.12.2014 Malmivaara A; CHESS/THL 43

Conclusions – to sum up
Promotion of staff competency and evidence based medicine approach is the backbone of effectiveness, efficiency and equality in ordinary care.
Scientifically sound assessment of health care units´ performance and benchmarking with peer units produces crucial data for decision-making, given standardized data on patient characteristics, interventions, outcomes and costs.
Validation work needs to be carried out in order to ascertain the quality of data.
The Real-Effectiveness Medicine framework can be utilised by clinicians, researchers organizations, and policy makers.
15.12.2014 Malmivaara A; CHESS/THL 44

Defining the current ability for providing effective treatment in ordinary health care
Bench-marking
Quality
Scientific evidence
Clinical competence
How well do we perform in
comparison to our peers?
What is the quality of
care we provide?
How well do we apply the
latest evidence?
How good is our
competence?
15.12.2014 Malmivaara A; CHESS/THL 45

Pursuing the best effectiveness in ordinary care
15.12.2014 Malmivaara A; CHESS/THL 46

15.12.2014 Malmivaara A; CHESS/THL 47
In Gatchel RJ, Schultz IZ (Eds). V.Malmivaara A. Chapter 26. RealEffectiveness. Medicinein.
Musculoskeletal. Disorders. Springer 2014

Thank you !
15.12.2014 Malmivaara A; CHESS/THL 48