Embed Size (px)
Citation preview
What’s so sweet about glycemic control?
June 3, 2016

• Provide an overview of why glucose control is important in surgical patient outcomes.
• Demonstrate an understanding of how anesthetics and surgery can
impact the body’s ability to remain within glycemic boundaries • Outline the optimal surgical patient glycemic goal range.
• Identify the effectiveness of glycemic control on mortality and
morbidity of adult patients during the intra and post-operative period.
• Discuss possible change ideas to implement glucose control.
Objectives
2016 CANADIAN SURGICAL
SITE INFECTION
PREVENTION AUDIT Dr. Claude Laflamme
March 24, 2016

Audit Participation
Sites 52
Patients 2082
Clean I & II 1998
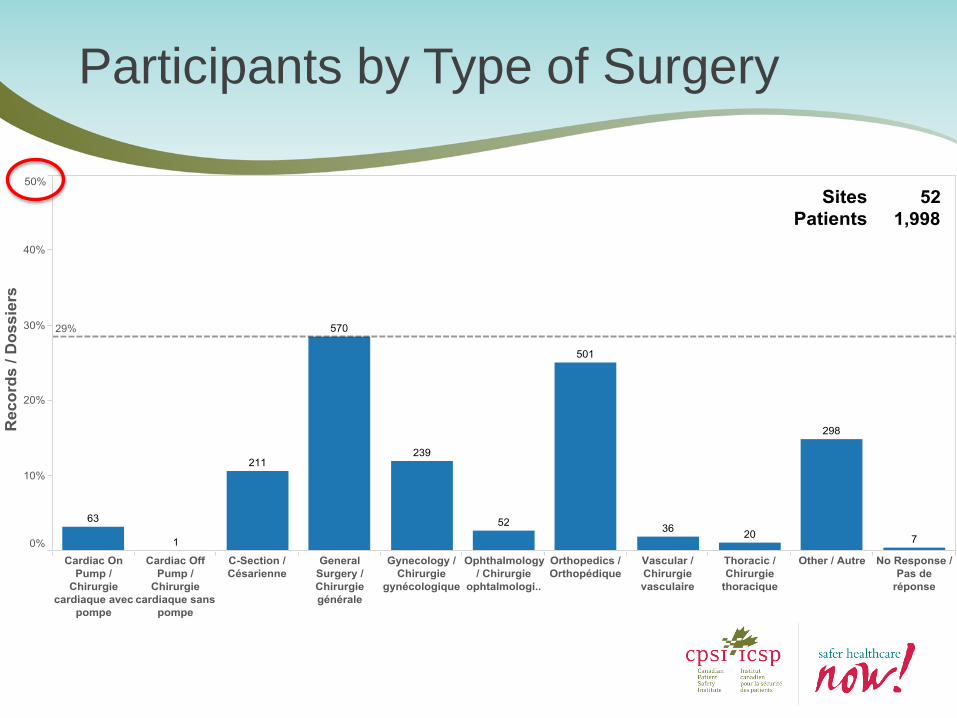
Participants by Type of Surgery
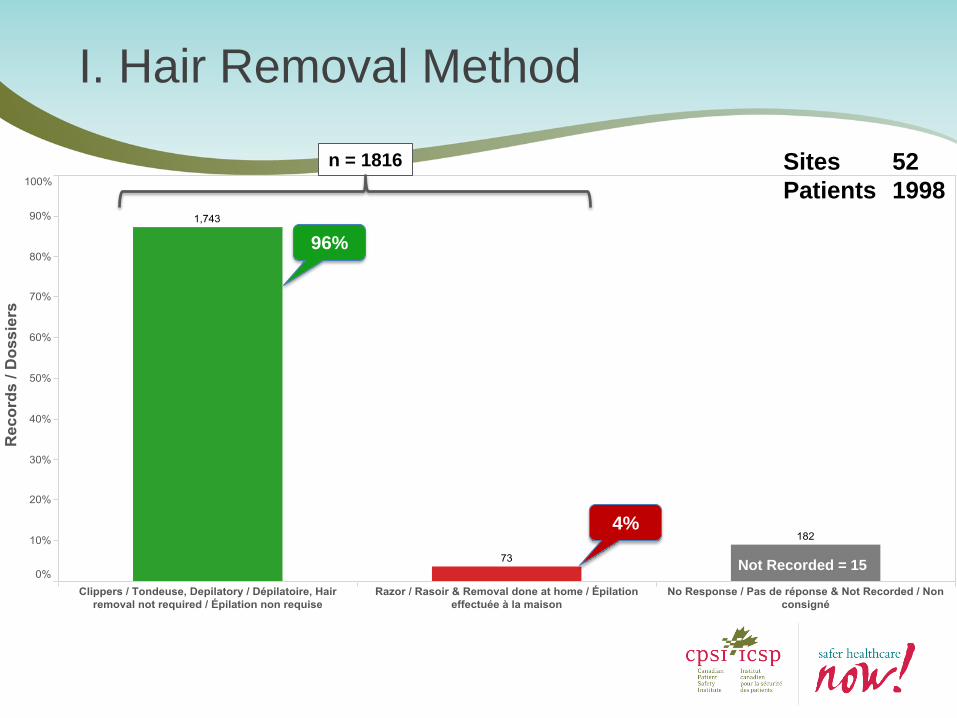
I. Hair Removal Method
Sites 52
Patients 1998
96%
4%
n = 1816
Not Recorded = 15
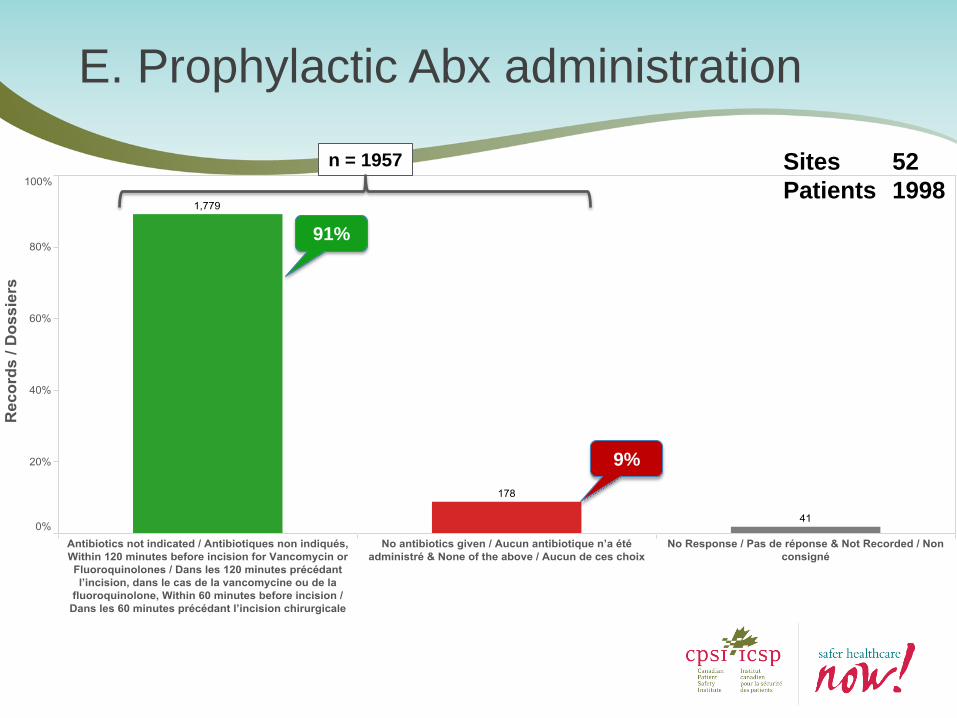
E. Prophylactic Abx administration
Sites 52
Patients 1998
n = 1957
91%
9%
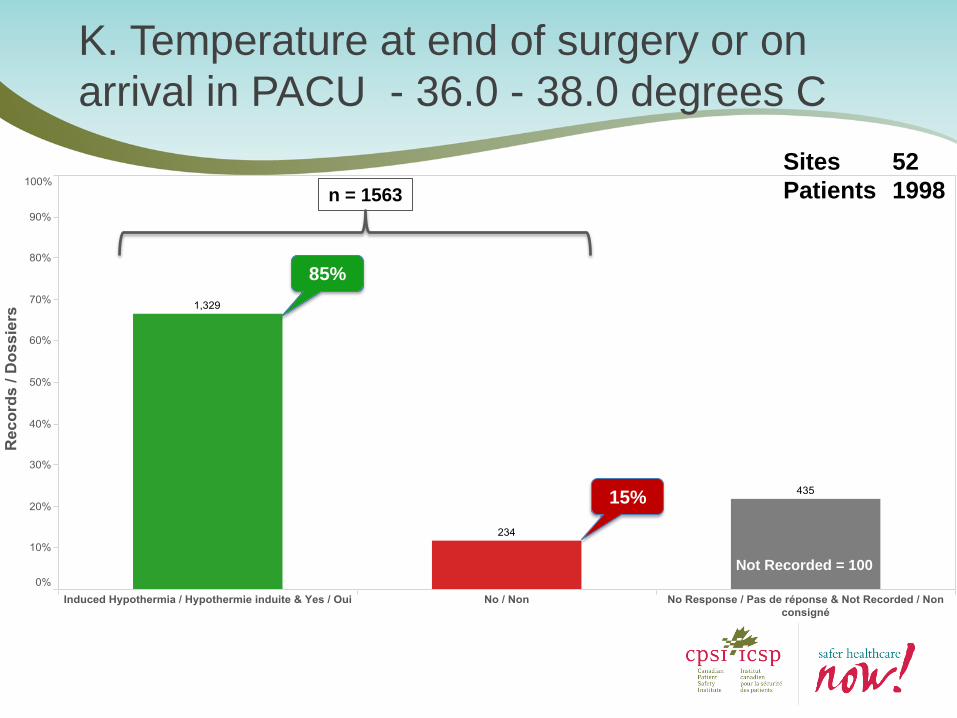
K. Temperature at end of surgery or on
arrival in PACU - 36.0 - 38.0 degrees C
Sites 52
Patients 1998 n = 1563
85%
15%
Not Recorded = 100
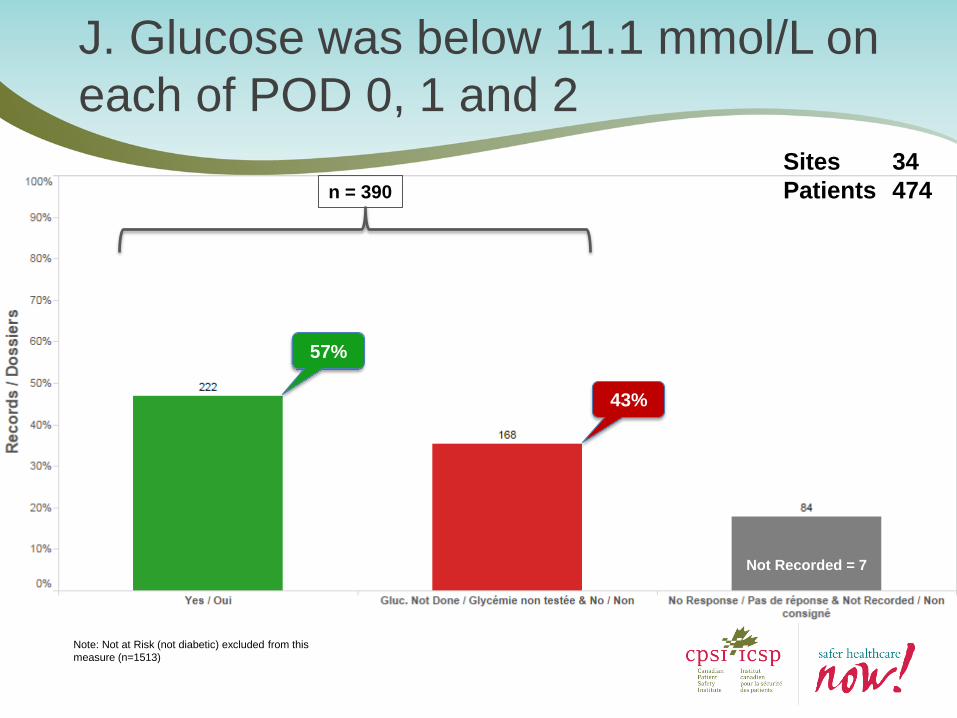
J. Glucose was below 11.1 mmol/L on
each of POD 0, 1 and 2
Sites 34
Patients 474
Note: Not at Risk (not diabetic) excluded from this
measure (n=1513)
n = 390
57%
43%
Not Recorded = 7
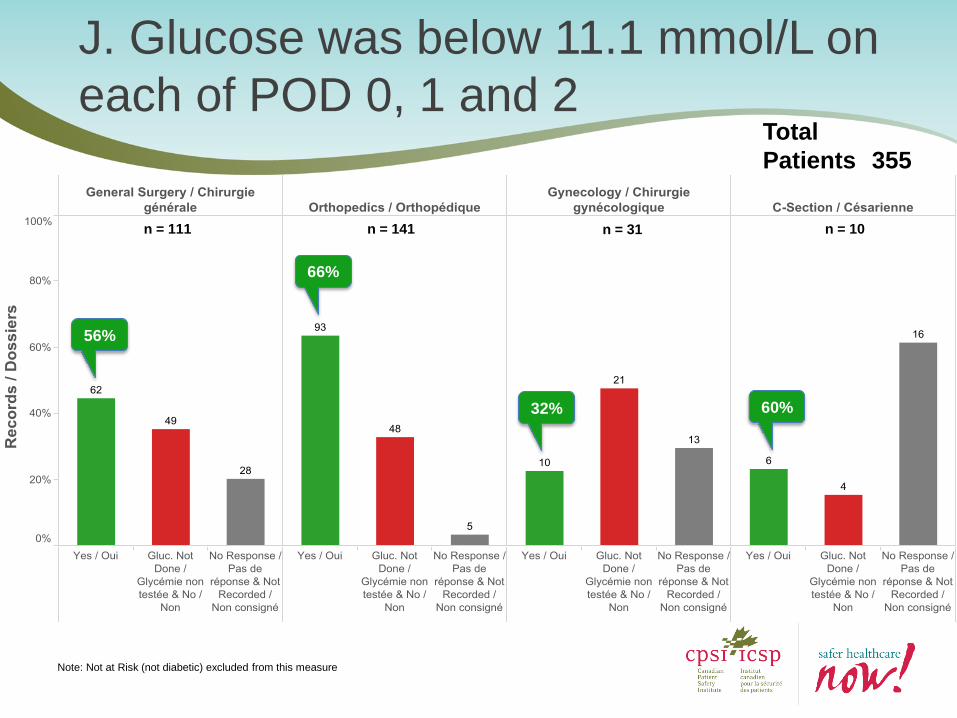
J. Glucose was below 11.1 mmol/L on
each of POD 0, 1 and 2 Total
Patients 355
56%
66%
32% 60%
Note: Not at Risk (not diabetic) excluded from this measure
n = 111 n = 141 n = 31 n = 10
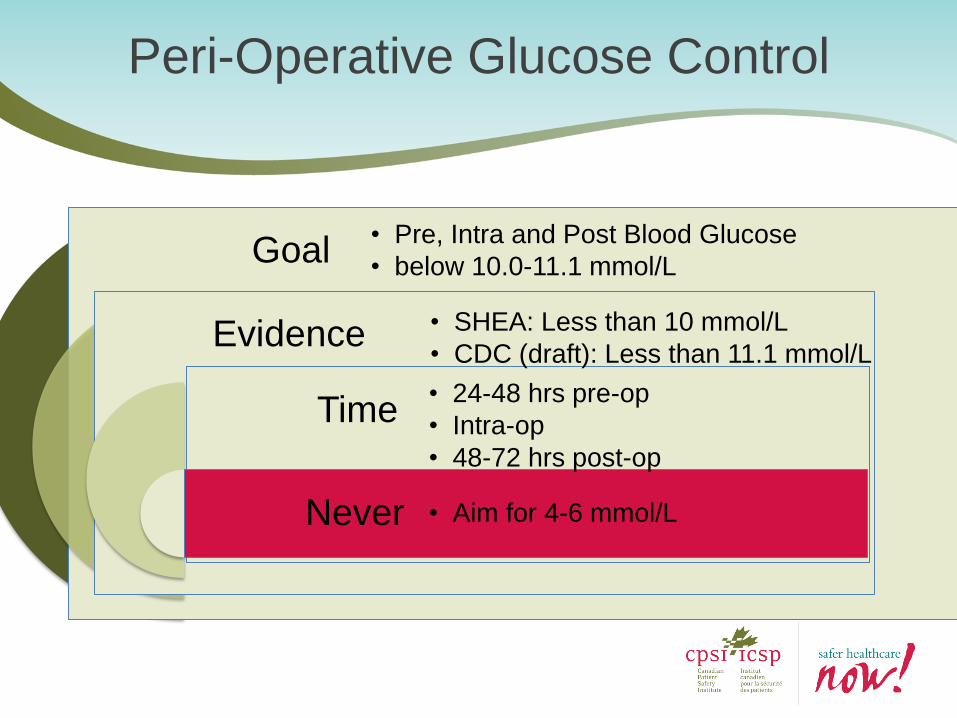
Goal
Evidence
Time
Never
• Pre, Intra and Post Blood Glucose
• below 10.0-11.1 mmol/L
• SHEA: Less than 10 mmol/L
• CDC (draft): Less than 11.1 mmol/L
• 24-48 hrs pre-op
• Intra-op
• 48-72 hrs post-op
• Aim for 4-6 mmol/L
Peri-Operative Glucose Control
The BC Perspective Curt Smecher
Anesthesiologist Abbotsford Regional Hospital
Surgical Site Infections and Diabetes
Marshall Dahl MD PhD FRCPC cert Endo
Clinical Professor, Endocrinology, University of British Columbia
Jordanna Kapeluto MD FRCPC
Endocrinology Fellow, University of British Columbia
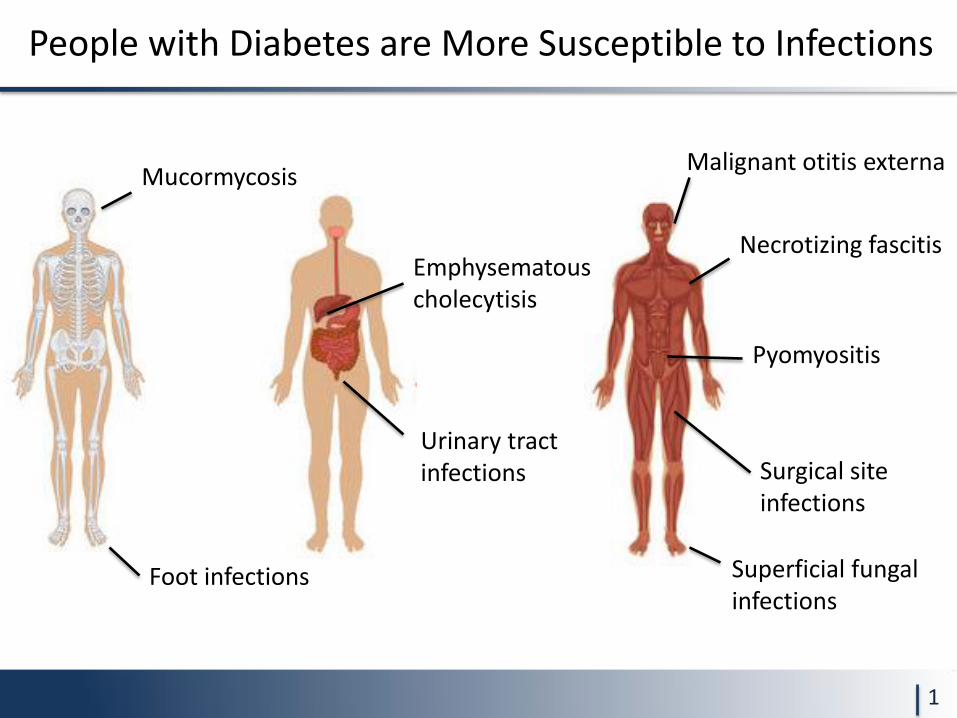
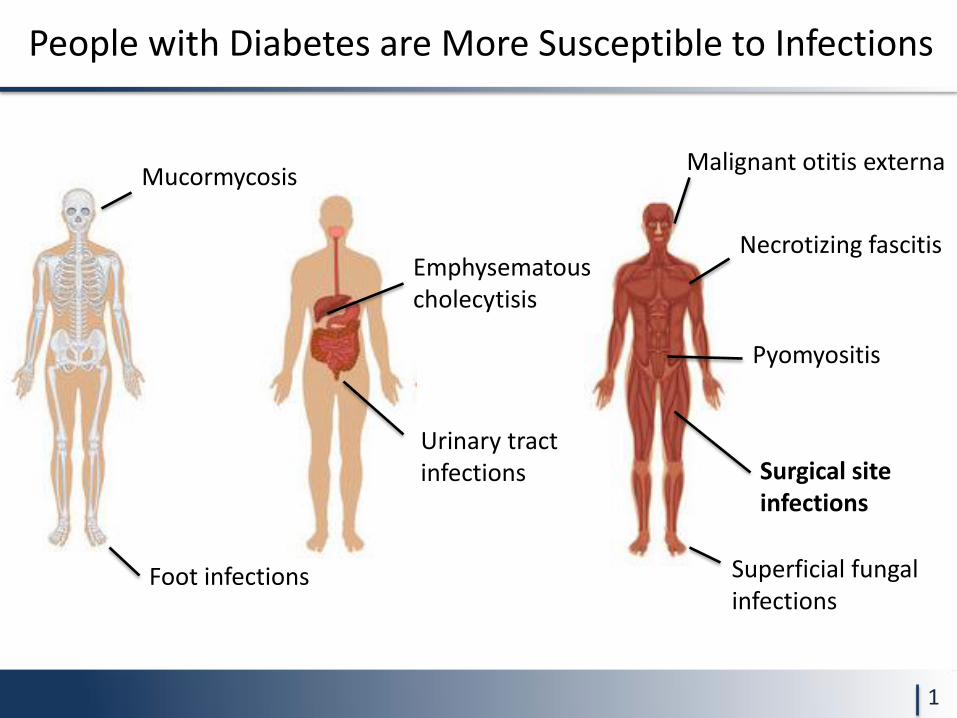
People with Diabetes are More Susceptible to Infections
1
Foot infections
Urinary tract infections
Superficial fungal infections
Mucormycosis Malignant otitis externa
Emphysematous cholecytisis
Pyomyositis
Necrotizing fascitis
Surgical site infections
People with Diabetes are More Susceptible to Infections
1
Foot infections
Urinary tract infections
Superficial fungal infections
Mucormycosis Malignant otitis externa
Emphysematous cholecytisis
Pyomyositis
Necrotizing fascitis
Surgical site infections
Hyperglycemia Impairs Immune Response
• Neutrophil function is impaired during hyperglycemia
– Chemotaxis, phagocytosis
• Cell-mediated immunity and Complement system are also impaired
• Occurs in laboratory setting by increasing glucose concentration in normal blood (glucose >11.1)
• Occurs in diabetes serum vs non-diabetes serum
2
Surgical Site Infection (SSI)
• CDC definition:
• SSIs are often localized to the incision site but can also extend into deeper adjacent structures
Horan TC et al: Infect Control Hosp Epidemiol. 1992;13(10):606 3
infection related to an operative procedure occurs at or near the surgical incision
• within 30 days of the procedure • within one year if prosthetic material is
implanted at surgery
Perioperative Hyperglycemia and SSI Risk
• N = 2090 general and vascular surgery patients
• Retrospective review
• Multivariate analysis: – age, emergency status, ASA classes P3-P5, operative time, diabetes,
plus postoperative glucose level.
• Colorectal patients: only postoperative glucose control a significant predictor of SSI (OR 3.2)
• Vascular surgery patients: operative time and diabetes were independent predictors of SSI
• “Postoperative hyperglycemia may be the most important risk factor for SSI. Aggressive early postoperative glycemic control should reduce the incidence of SSI.”
Ata el al; Arch Surg 2010; 145 (9): 858 4
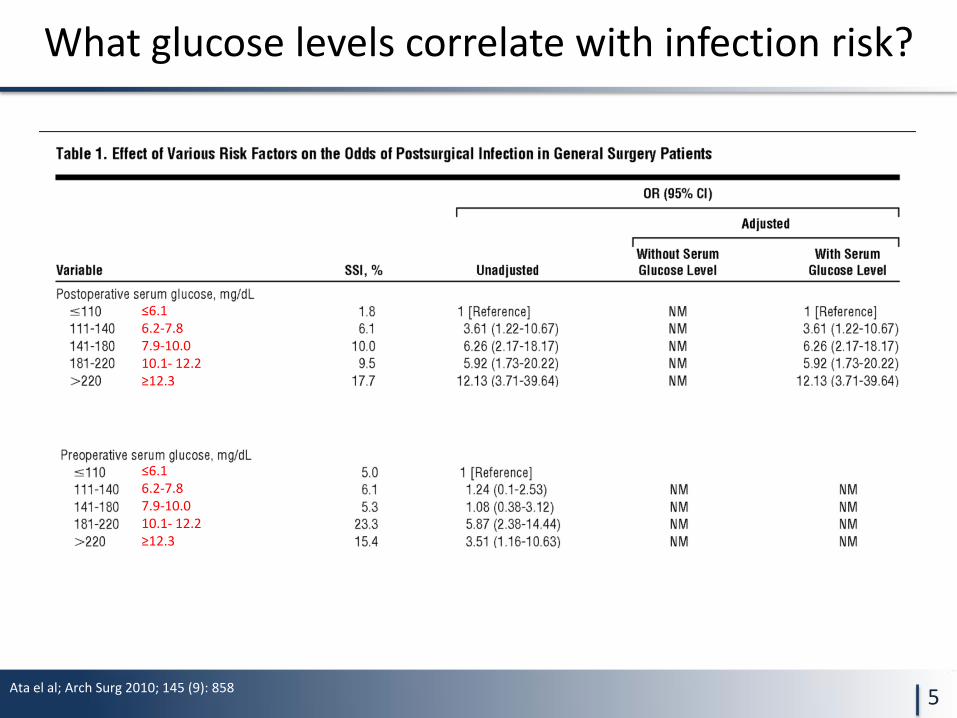
Ata el al; Arch Surg 2010; 145 (9): 858
What glucose levels correlate with infection risk?
5
≤6.1 6.2-7.8 7.9-10.0 10.1- 12.2 ≥12.3
≤6.1 6.2-7.8 7.9-10.0 10.1- 12.2 ≥12.3
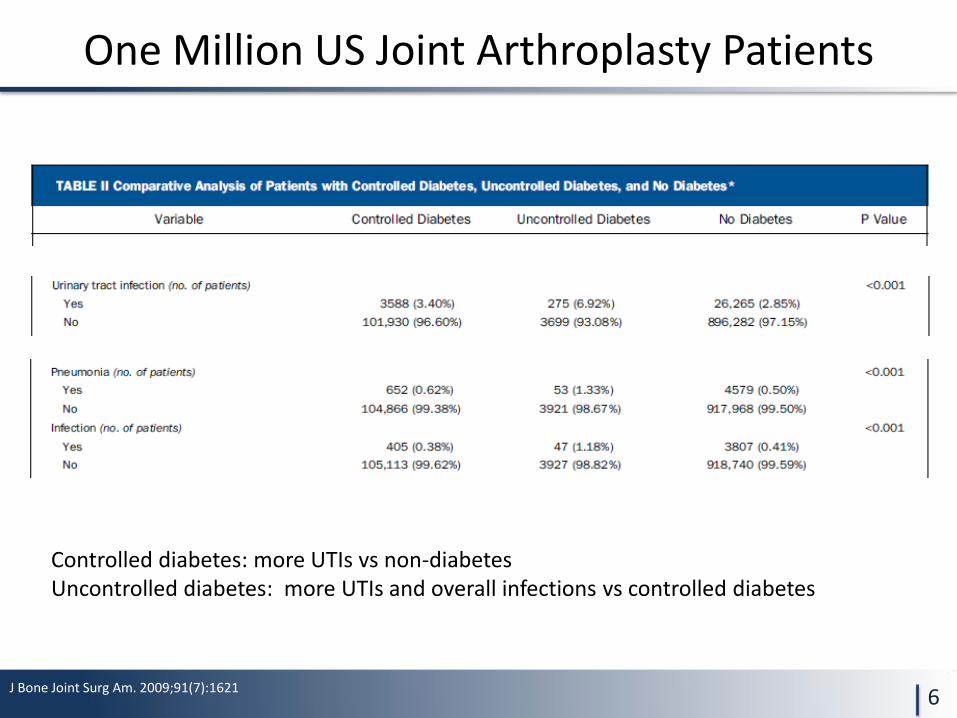
Controlled diabetes: more UTIs vs non-diabetes Uncontrolled diabetes: more UTIs and overall infections vs controlled diabetes
J Bone Joint Surg Am. 2009;91(7):1621
One Million US Joint Arthroplasty Patients
6
Is it pre-existing diabetes control or perioperative control?
• Prospective, 1000 patients, cardiothoracic surgery
• Predictors of SSI: independent risk factors – Diabetes (OR 2.76)
– Postoperative hyperglycemia [>11.1] (OR 2.02)
• Among patients with known diabetes, elevated A1c not associated with risk of SSI
• Perioperative management and acute control of glucose more important than diabetes status before surgery
Infect Control Hosp Epidemiol. 2001;22(10):607 7
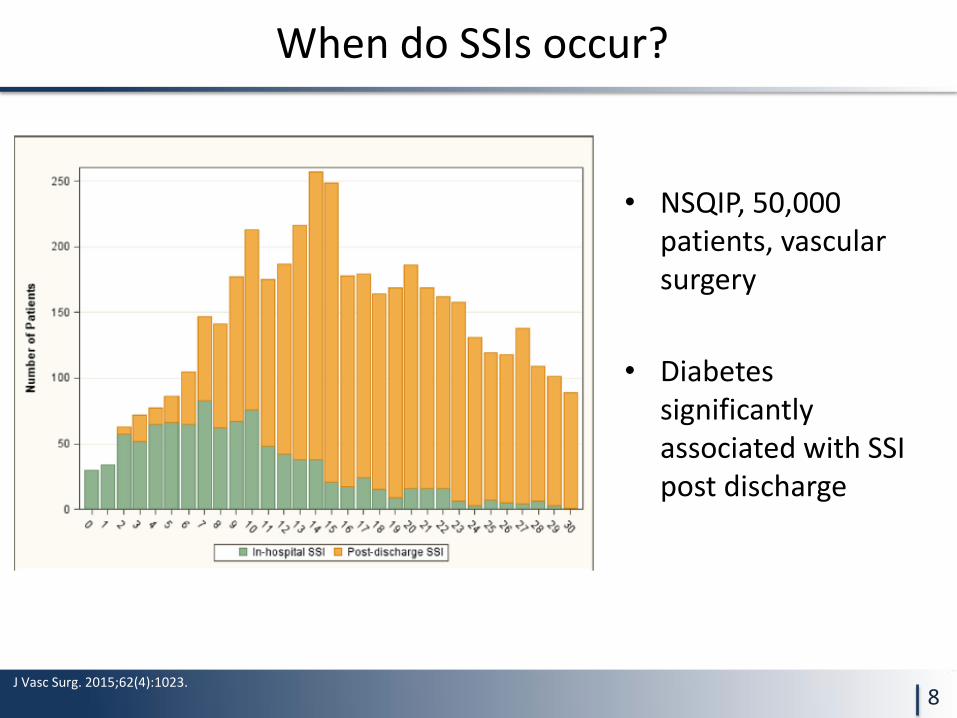
When do SSIs occur?
• NSQIP, 50,000 patients, vascular surgery
• Diabetes significantly associated with SSI post discharge
J Vasc Surg. 2015;62(4):1023. 8
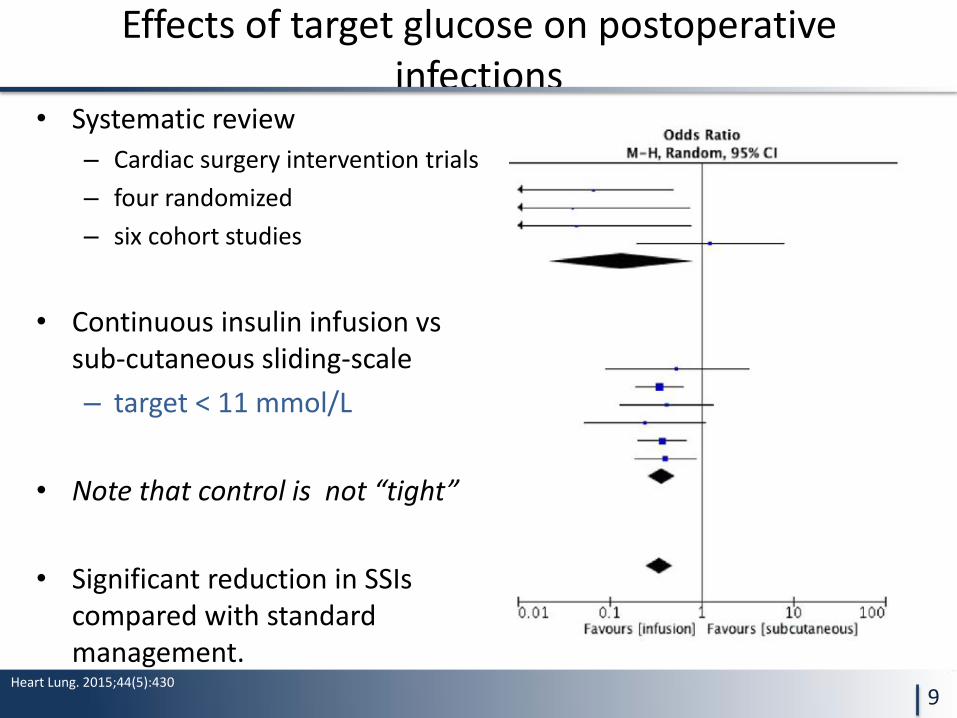
Effects of target glucose on postoperative infections
• Systematic review
– Cardiac surgery intervention trials
– four randomized
– six cohort studies
• Continuous insulin infusion vs sub-cutaneous sliding-scale
– target < 11 mmol/L
• Note that control is not “tight”
• Significant reduction in SSIs compared with standard management.
Heart Lung. 2015;44(5):430
9
Other Factors in Diabetes that Predispose to SSIs
• Vascular Insufficiency
– Tissue ischemia, anaerobic bacteria
• Sensory peripheral neuropathy
– Local trauma and ulceration
• Autonomic neuropathy
– Urinary retention and stasis
• Increased skin and nasal colonization
– More frequent S. Aureus and methicillin-resistance
• Increased E. Coli binding to bladder epithelium
10
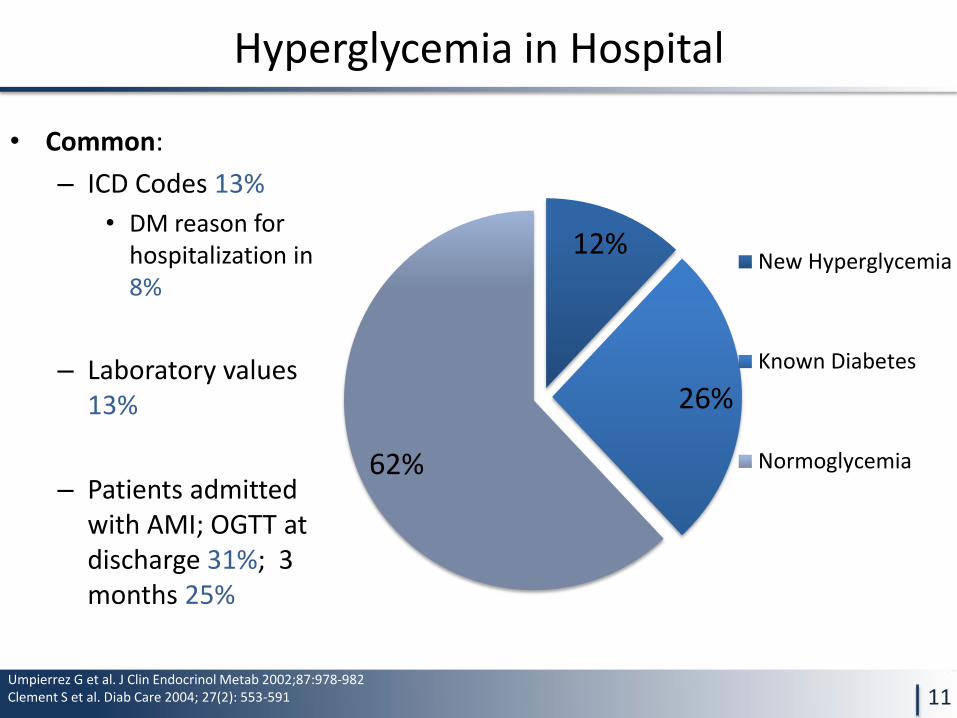
Hyperglycemia in Hospital
11
12%
26%
62%
New Hyperglycemia
Known Diabetes
Normoglycemia
• Common:
– ICD Codes 13%
• DM reason for hospitalization in 8%
– Laboratory values 13%
– Patients admitted with AMI; OGTT at discharge 31%; 3 months 25%
Umpierrez G et al. J Clin Endocrinol Metab 2002;87:978-982 Clement S et al. Diab Care 2004; 27(2): 553-591
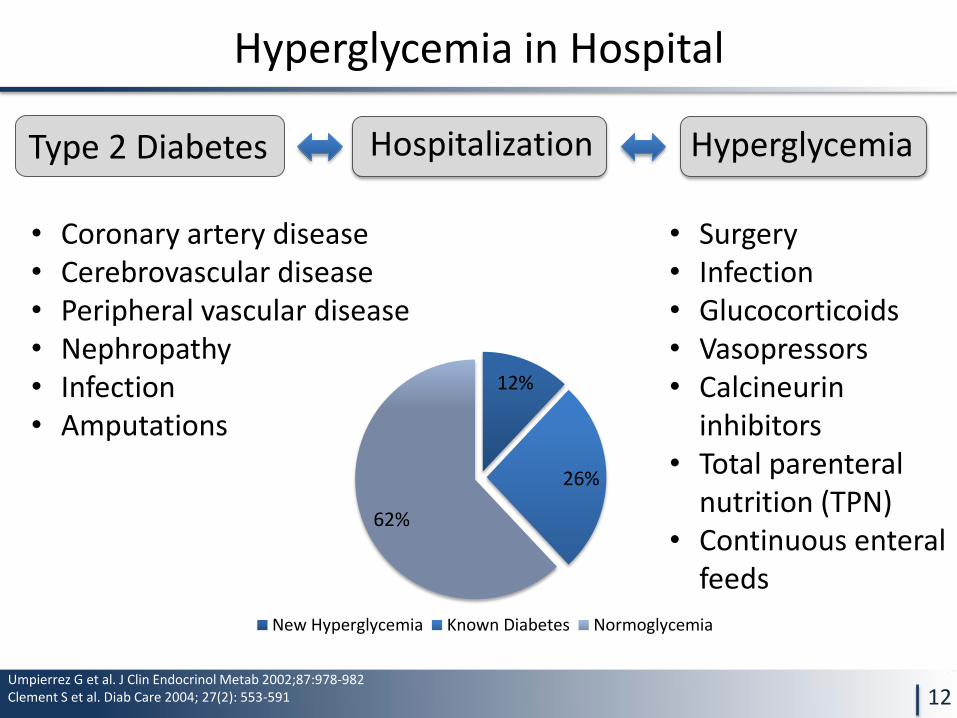
Hyperglycemia in Hospital
12
12%
26%
62%
New Hyperglycemia Known Diabetes Normoglycemia
Hospitalization Type 2 Diabetes Hyperglycemia
• Coronary artery disease • Cerebrovascular disease • Peripheral vascular disease • Nephropathy • Infection • Amputations
• Surgery • Infection • Glucocorticoids • Vasopressors • Calcineurin
inhibitors • Total parenteral
nutrition (TPN) • Continuous enteral
feeds
Umpierrez G et al. J Clin Endocrinol Metab 2002;87:978-982 Clement S et al. Diab Care 2004; 27(2): 553-591
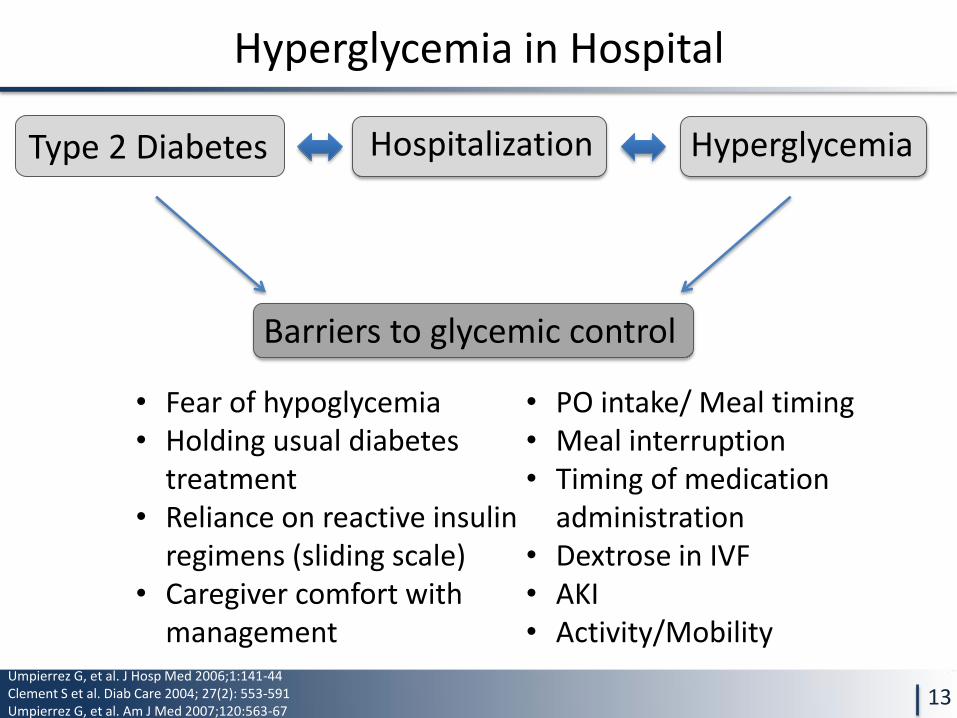
Hyperglycemia in Hospital
13
Hospitalization Type 2 Diabetes Hyperglycemia
Umpierrez G, et al. J Hosp Med 2006;1:141-44 Clement S et al. Diab Care 2004; 27(2): 553-591 Umpierrez G, et al. Am J Med 2007;120:563-67
Barriers to glycemic control
• Fear of hypoglycemia • Holding usual diabetes
treatment • Reliance on reactive insulin
regimens (sliding scale) • Caregiver comfort with
management
• PO intake/ Meal timing • Meal interruption • Timing of medication
administration • Dextrose in IVF • AKI • Activity/Mobility
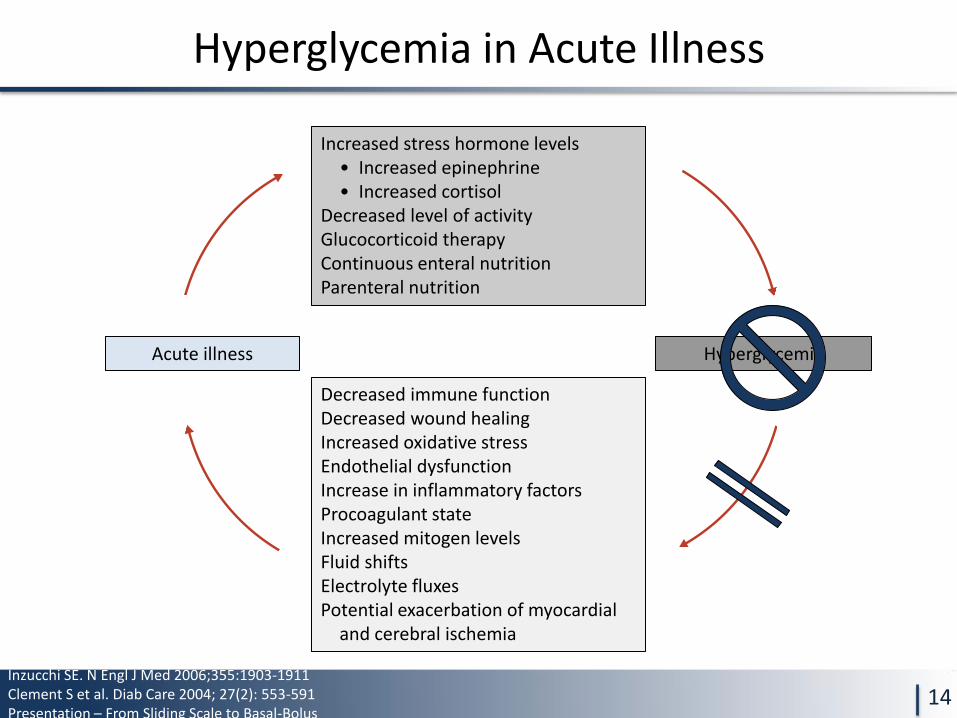
Hyperglycemia in Acute Illness
14
Increased stress hormone levels • Increased epinephrine • Increased cortisol
Decreased level of activity Glucocorticoid therapy Continuous enteral nutrition Parenteral nutrition
Acute illness Hyperglycemia
Decreased immune function Decreased wound healing Increased oxidative stress Endothelial dysfunction Increase in inflammatory factors Procoagulant state Increased mitogen levels Fluid shifts Electrolyte fluxes Potential exacerbation of myocardial
and cerebral ischemia
Inzucchi SE. N Engl J Med 2006;355:1903-1911 Clement S et al. Diab Care 2004; 27(2): 553-591 Presentation – From Sliding Scale to Basal-Bolus
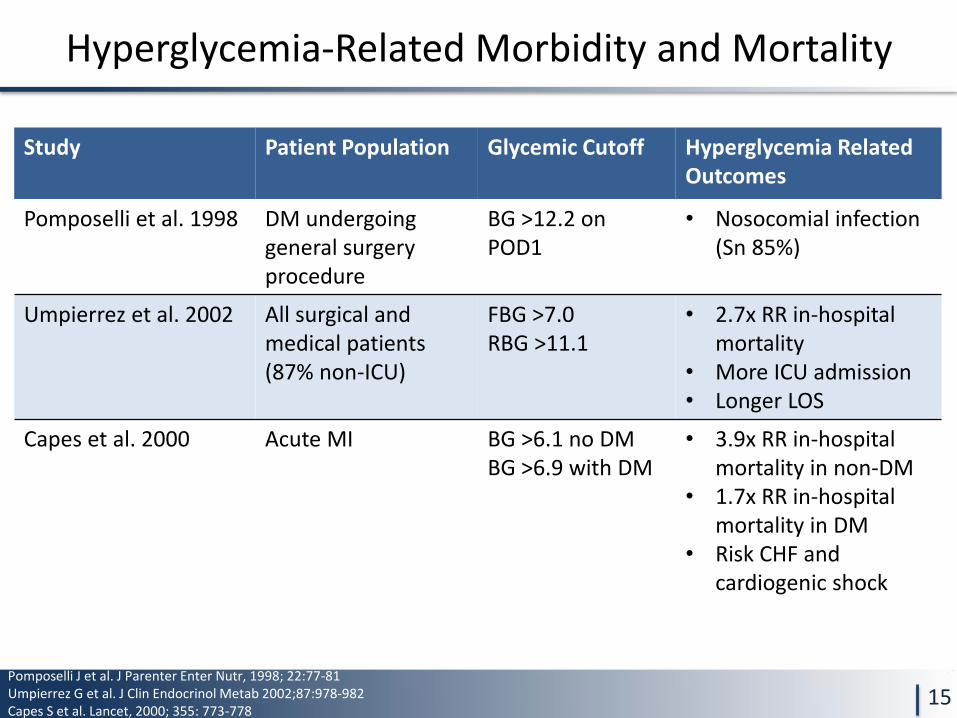
Hyperglycemia-Related Morbidity and Mortality
15
Study Patient Population Glycemic Cutoff Hyperglycemia Related Outcomes
Pomposelli et al. 1998 DM undergoing general surgery procedure
BG >12.2 on POD1
• Nosocomial infection (Sn 85%)
Umpierrez et al. 2002 All surgical and medical patients (87% non-ICU)
FBG >7.0 RBG >11.1
• 2.7x RR in-hospital mortality
• More ICU admission • Longer LOS
Capes et al. 2000 Acute MI BG >6.1 no DM BG >6.9 with DM
• 3.9x RR in-hospital mortality in non-DM
• 1.7x RR in-hospital mortality in DM
• Risk CHF and cardiogenic shock
Pomposelli J et al. J Parenter Enter Nutr, 1998; 22:77-81 Umpierrez G et al. J Clin Endocrinol Metab 2002;87:978-982 Capes S et al. Lancet, 2000; 355: 773-778
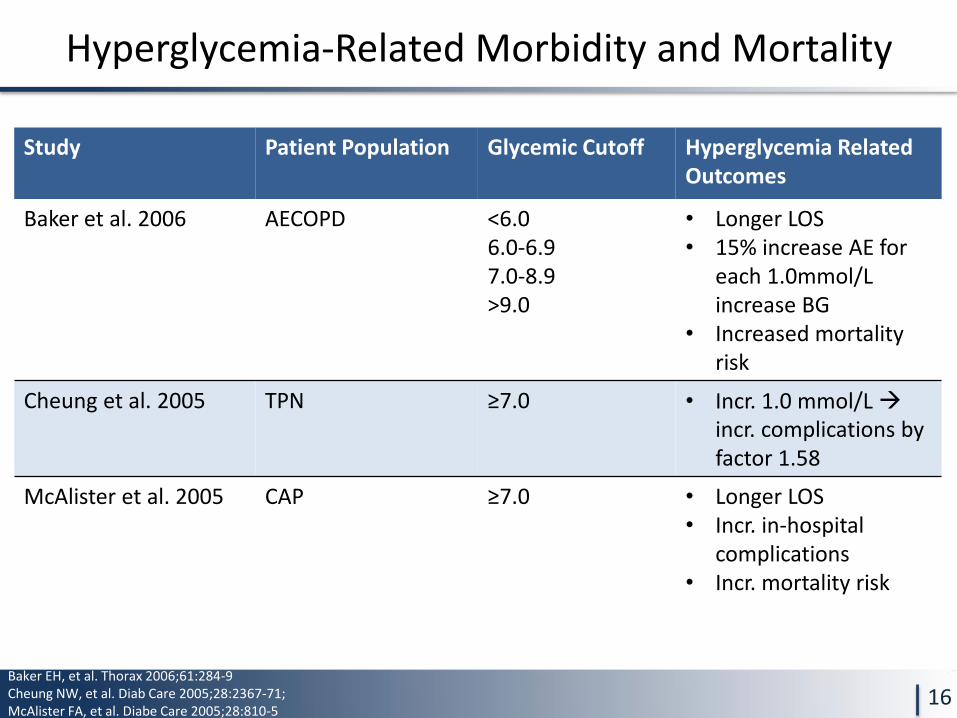
Hyperglycemia-Related Morbidity and Mortality
16
Study Patient Population Glycemic Cutoff Hyperglycemia Related Outcomes
Baker et al. 2006 AECOPD <6.0 6.0-6.9 7.0-8.9 >9.0
• Longer LOS • 15% increase AE for
each 1.0mmol/L increase BG
• Increased mortality risk
Cheung et al. 2005 TPN ≥7.0 • Incr. 1.0 mmol/L incr. complications by factor 1.58
McAlister et al. 2005 CAP ≥7.0 • Longer LOS • Incr. in-hospital
complications • Incr. mortality risk
Baker EH, et al. Thorax 2006;61:284-9 Cheung NW, et al. Diab Care 2005;28:2367-71; McAlister FA, et al. Diabe Care 2005;28:810-5
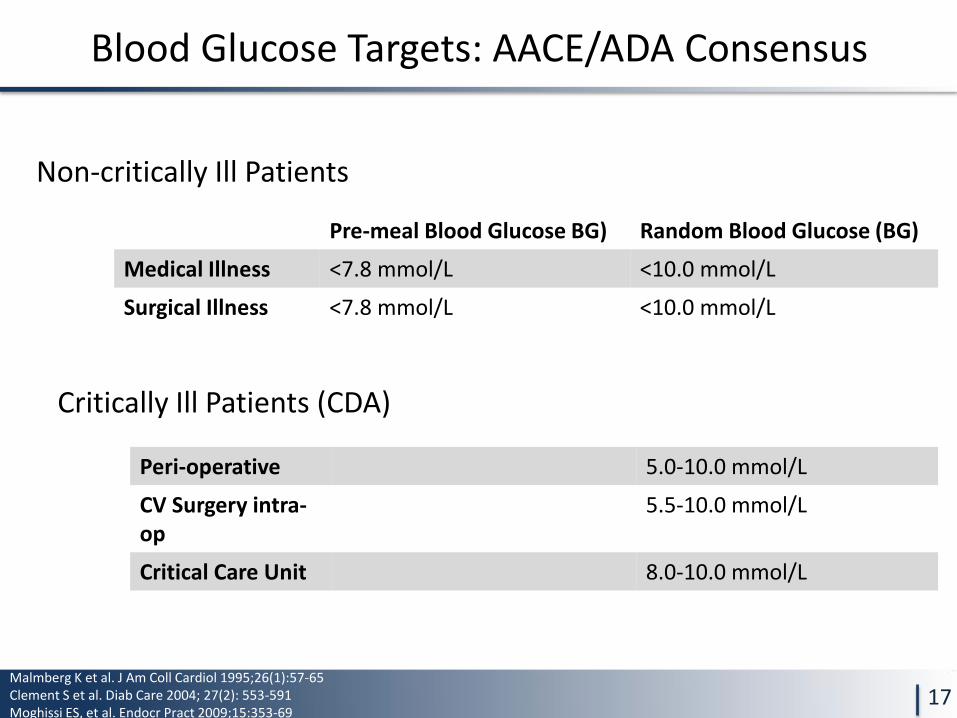
Blood Glucose Targets: AACE/ADA Consensus
17
Non-critically Ill Patients
Critically Ill Patients (CDA)
Pre-meal Blood Glucose BG) Random Blood Glucose (BG)
Medical Illness <7.8 mmol/L <10.0 mmol/L
Surgical Illness <7.8 mmol/L <10.0 mmol/L
Peri-operative 5.0-10.0 mmol/L
CV Surgery intra-op
5.5-10.0 mmol/L
Critical Care Unit 8.0-10.0 mmol/L
Malmberg K et al. J Am Coll Cardiol 1995;26(1):57-65 Clement S et al. Diab Care 2004; 27(2): 553-591 Moghissi ES, et al. Endocr Pract 2009;15:353-69
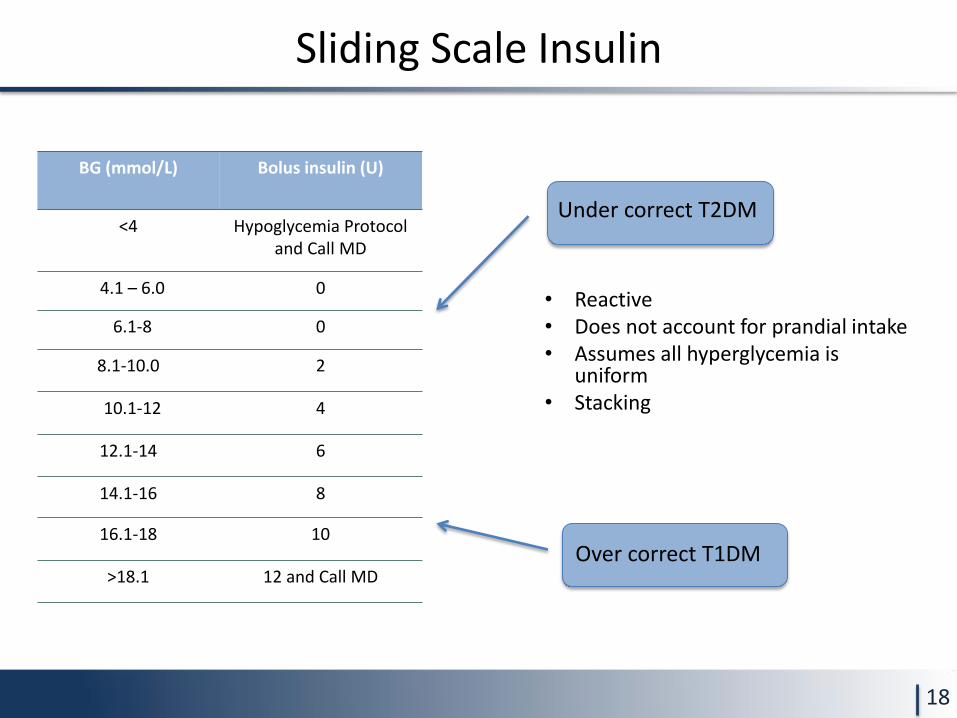
• Reactive • Does not account for prandial intake • Assumes all hyperglycemia is
uniform • Stacking
Sliding Scale Insulin
18
BG (mmol/L) Bolus insulin (U)
<4 Hypoglycemia Protocol and Call MD
4.1 – 6.0 0
6.1-8 0
8.1-10.0 2
10.1-12 4
12.1-14 6
14.1-16 8
16.1-18 10
>18.1 12 and Call MD
Under correct T2DM
Over correct T1DM
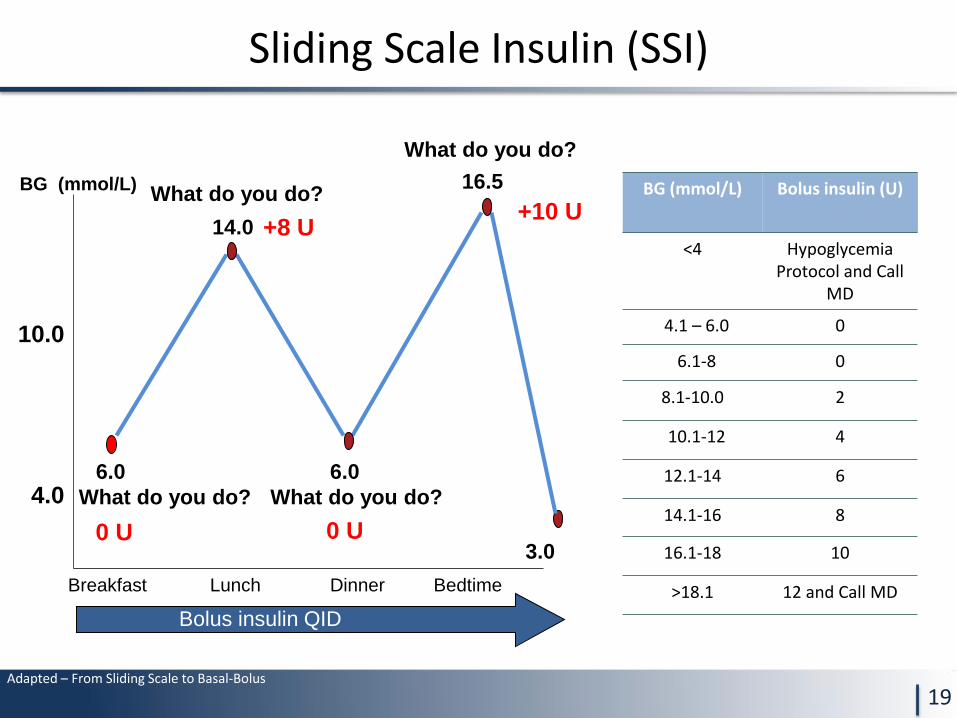
Sliding Scale Insulin (SSI)
19
4.0
10.0
Breakfast Lunch Dinner Bedtime
6.0
Bolus insulin QID
14.0
6.0
16.5
3.0
What do you do?
What do you do?
What do you do?
What do you do?
+8 U
0 U 0 U
+10 U
BG (mmol/L) BG (mmol/L) Bolus insulin (U)
<4 Hypoglycemia Protocol and Call
MD
4.1 – 6.0 0
6.1-8 0
8.1-10.0 2
10.1-12 4
12.1-14 6
14.1-16 8
16.1-18 10
>18.1 12 and Call MD
Adapted – From Sliding Scale to Basal-Bolus
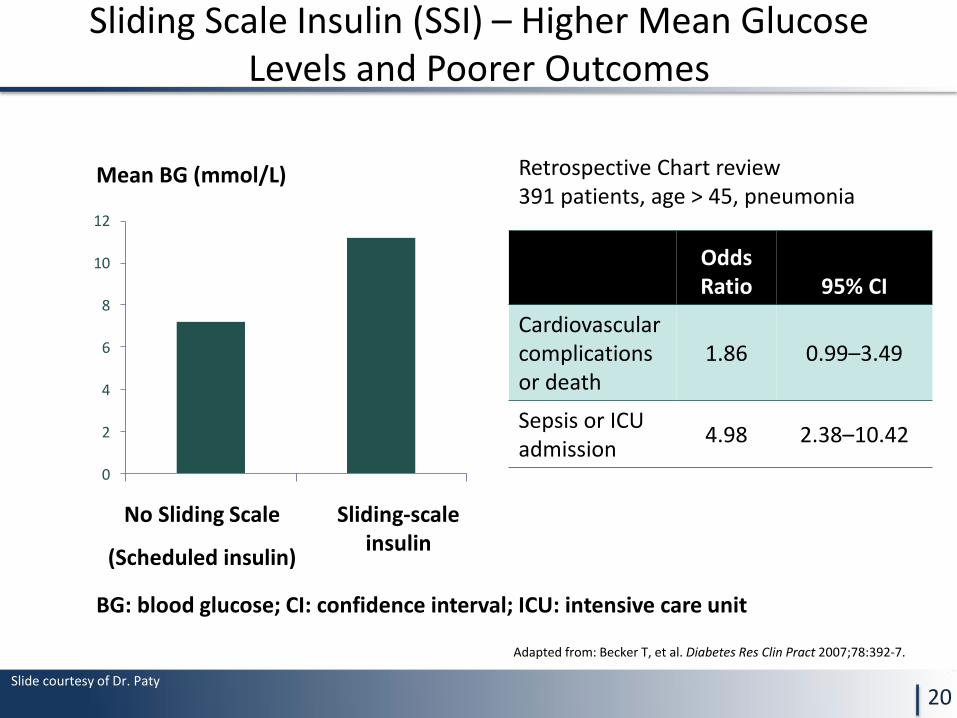
Sliding Scale Insulin (SSI) – Higher Mean Glucose Levels and Poorer Outcomes
20
Adapted from: Becker T, et al. Diabetes Res Clin Pract 2007;78:392-7.
0
2
4
6
8
10
12
Mean BG (mmol/L)
No Sliding Scale
(Scheduled insulin)
Sliding-scale insulin
BG: blood glucose; CI: confidence interval; ICU: intensive care unit
Odds Ratio 95% CI
Cardiovascular complications or death
1.86 0.99–3.49
Sepsis or ICU admission
4.98 2.38–10.42
Retrospective Chart review 391 patients, age > 45, pneumonia
Slide courtesy of Dr. Paty
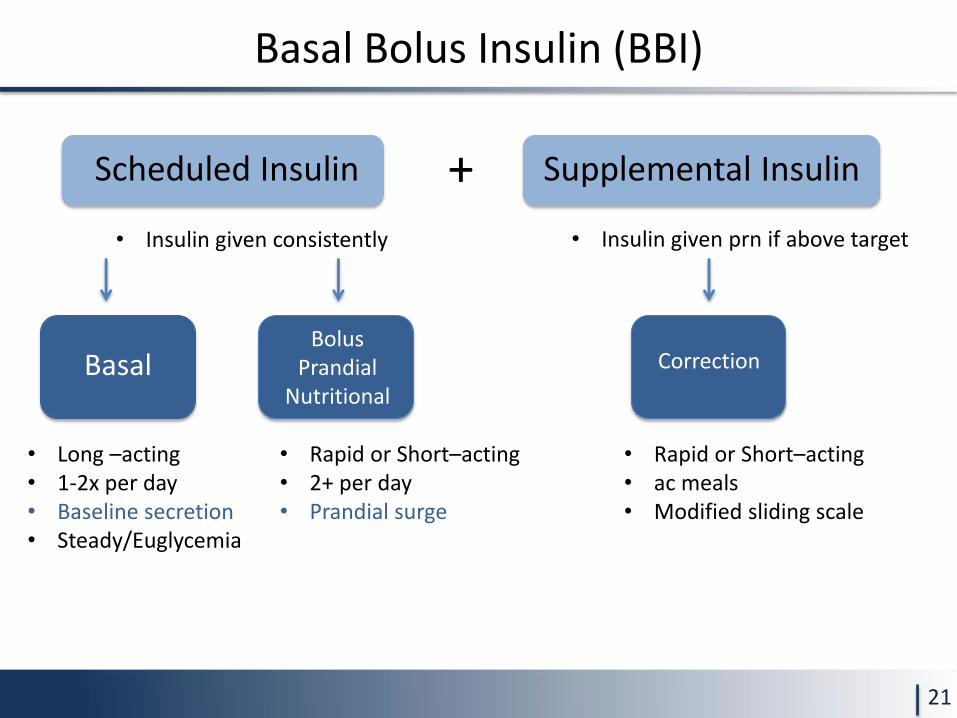
Basal Bolus Insulin (BBI)
21
• Insulin given consistently
• Long –acting • 1-2x per day • Baseline secretion • Steady/Euglycemia
• Rapid or Short–acting • 2+ per day • Prandial surge
• Insulin given prn if above target
Scheduled Insulin Supplemental Insulin +
Basal Bolus
Prandial Nutritional
Correction
• Rapid or Short–acting • ac meals • Modified sliding scale
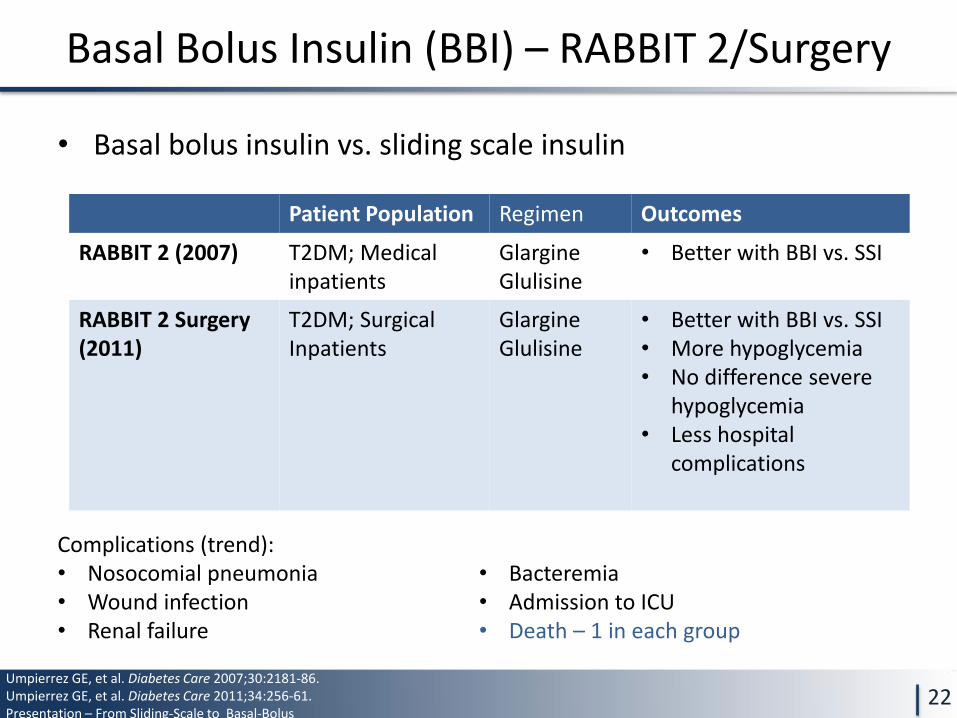
• Basal bolus insulin vs. sliding scale insulin
Basal Bolus Insulin (BBI) – RABBIT 2/Surgery
22
Patient Population Regimen Outcomes
RABBIT 2 (2007) T2DM; Medical inpatients
Glargine Glulisine
• Better with BBI vs. SSI
RABBIT 2 Surgery (2011)
T2DM; Surgical Inpatients
Glargine Glulisine
• Better with BBI vs. SSI • More hypoglycemia • No difference severe
hypoglycemia • Less hospital
complications
Umpierrez GE, et al. Diabetes Care 2007;30:2181-86. Umpierrez GE, et al. Diabetes Care 2011;34:256-61. Presentation – From Sliding-Scale to Basal-Bolus
Complications (trend): • Nosocomial pneumonia • Wound infection • Renal failure
• Bacteremia • Admission to ICU • Death – 1 in each group
CDA 2013 - Recommendations
23
1. Provided that their medical conditions, dietary
intake, and glycemic control are acceptable,
people with diabetes should be maintained on
their pre-hospitalization oral anti-hyperglycemic
agents or insulin regimens [Grade D, Consensus]
Recommendation 1
CDA 2013 - Recommendations
24
2. For hospitalized patients with diabetes treated with insulin,
a proactive approach that includes basal, bolus, and
correction (supplemental) insulin, along with pattern
management, should be used to reduce adverse events and
improve glycemic control, instead of the reactive sliding-
scale insulin approach that uses only short- or rapid-acting
insulin [Grade B, Level 2]
Recommendation 2
CDA 2013 - Recommendations
25
3. For the majority of non critically ill patients treated with
insulin, pre-meal BG targets should be 5.0 to 8.0 mmol/L in
conjunction with random BG values <10.0 mmol/L, as long
as these targets can be safely achieved [Grade D, consensus]
4. For most medical/surgical critically ill patients with
hyperglycemia, a continuous IV insulin infusion should be
used to maintain glucose levels between 8.0-10.0 mmol/L
[Grade D, consensus]
Recommendation 3 and 4
CDA 2013 - Recommendations
26
5. To maintain intraoperative glycemic levels between 5.5-10.0
mmol/L for patients with diabetes undergoing CABG, a
continuous IV insulin infusion protocol administered by
trained staff, [Grade C, Level 3] should be used
6. Perioperative glycemic levels should be maintained
between 5.0-10.0 mmol/L for most other surgical situations,
with appropriate protocol and trained staff to ensure safe
and effective implementation of therapy and to minimize
the likelihood of hypoglycemia [Grade D, Consensus]
Recommendation 5 and 6
CDA 2013 - Recommendations
27
7. In hospitalized patients, hypoglycemia should be
avoided: – Protocols for hypoglycemia avoidance, recognition and
management should be implemented with nurse –initiated
treatment, including glucagon for severe hypoglycemia when
IV access is not readily available [Grade D, consensus]
– Patients at risk of hypoglycemia should have ready access to
an appropriate source of glucose (oral or IV) at all times,
particularly when NPO or during diagnostic procedures [Grade D,
Consensus]
Recommendation 7
CDA 2013 - Recommendations
28
8. Healthcare professional education, insulin protocols and order sets may be used to improve adherence to optimal insulin use and glycemic control [Grade C, Level 3]
9. Measures to assess, monitor, and improve glycemic control within the inpatient setting should be implemented, as well as diabetes-specific discharge planning [Grade D, Consensus]
Recommendation 8 and 9
Questions?


The10K