Embed Size (px)
Citation preview

Pharmacology Conscious SedationDrugs ..
It is yet a matter of selection!
Wael Galal; M.D.Anesthesia Consultant
KFH Al-Baha


Whipping the patient ..Is it necessary!!

My Presentation Objectives!!Beyond reviewing drugs used for conscious sedation
• Which drugs I can choose, for which patient, procedure and under which circumstances?
• How to administer sedation?
• What I can expect to happen?
• What to do when the unexpected happen?(The Rescue Concept)





• Select your patient• Select for which procedure• Select your agent• Select method(s) of administration• Select sedational circumstances
... Then you master it all.
Pharmacologic Selection

Which one of these individuals can be given conscious
sedation? … Select for yourself!

Common Bad Selections for Conscious Sedation
• Obesity and other patients presenting with difficult airway indicators
• Full stomach including those with bleeding varices undergoing EGD maneuvers
• Neglecting the ASA classification (i.e. III or IV)
• Patients with severe cardiorespiratory illness
• Patients with impaired psychologic fitness
• Procedures taking longer than 1-2 hr

Common Conscious Sedation Procedures
• Endoscopy
• Lumbar puncture
• Wound care
• Minor surgical procedures: simple suturing, dental procedures
• Placement of implanted devices, catheters, and tubes
• Bone marrow aspiration
• Reduction and immobilization of fractures
• Removal of implanted devices and tubes
• Magnetic resonance imaging and computed tomography scan

The Ideal …Agent!!

The Ideal Sedating Agent• Predictable onset of
action
• Lack of cumulative effects
• Promote rapid recovery
• Minimal side-effects
• Residual analgesia
• Short duration of action
• Patient safety
• Reversible
• No residual depression
• Painless administration

Classification• Benzodiapezin
es:– Midazolam– Diazepam
• IV Anesthetics:– Ketamine– Propofol
Benzodiapezines:
– Midazolam(Dormicum)
– Diazepam(Valium)
Opioids:
-Fentanyl-Morphine-Meperidine
(Demerol)
Anesthetics/sedatives:
– Thiopentone(Pentohal)
– Ketamine– Propofol– Dexmedeto-
midine
ALL THESE 3-GROUPS OF DRUGS ARE APPROVED FOR
CONSCIOUS SEDATION; However!!

Drug Choice for Conscious Sedation
• This depends on the requirement of:
–Amnesia Midazolam–Analgesia Opiates / Ketamine–Relaxation IV anesthetics/Not
Ketamine–Consciousness Avoid anesthetics

ALL SEDATIVES
• Cause Upper Airway Obstruction
• Produce Respiratory Depression
• Blunt Ventilatory Response to – CO2 (main ventilatory drive) and – Oxygen.
Can Do the Following:


How This Presentation Goes?• Sedation drugs follow two lists (Adult/Pediatric).
• Each Drug has a Dosage instruction to follow, initial bolus increments STOP when a maximum recommended dose is reached.
• Care with age, excretory organ dysfunction and debilitation dosage by 1/3-1/2.
GENERAL RULES

• Specific precautions (Mostly patients with CNS dep., Resp. disorders and CVD).
• REMEMBER: our target is Moderate Sedation. Dose-to-effect titration is your tool.
• Sedating agents potentiate the effects of one another (Synergism).

The Conscious Sedation Sheets (Adults/Pediatric)
Distributed to All Wards
THIS SESSION WILL SIMPLIFY & EXPLAIN

Drugs Used for Adult Sedation

DRUG Adult Dose ONSET SPECIAL CONSIDERATION
S
REVERSAL AGENT
PRECAUTIONS CONTRAINDICATIONS
& SIDE EFFECTS
MIDAZOLAM(Dormicum)
AnxiolyticSedativeAmnesicAnti-convulsant
Initial dose:1mg. – elderly/debilitated2.5mg. – healthy adultInitial dose should not exceed 2.5mgm.Usual max:Average adult<60 years:5mg. within 30 min.Elderly adult >60 years: 3.5 mg within 30 min.IV Dose rate: 1mg. over 1 min. Wait 2 min. after each increment to fully evaluate effects. Maintain level with 25% of initial IV dose.
Onset: 1 ½-5 min.
Peak: 10-15 min.
Duration: 60-90 min.
Metabolized: liver
Excreted: kidneyRecovery is dose dependent, usually 1-2 hrs.
Reduce dose by 1/3 to 1/2 when used with other CNS depressing drugs or in the elderly or debilitated.Manufacturer recommends not more than 1.5 mgm over at least two minutes in patients with decreased pulmonary reserves.
FLUMAZENIL(Anexate)
P- Elderly/debilitated
C- Hypersensitivity, acute narrow angle glaucoma
S- CNS / Resp. depression- Hypotension- Agitation- N/V, hiccups
DIAZEPAM (Valium)
SedativeAnxiolyticAnti-convulsant
Initial dose: 2mg.Usual Maximum:10-20mg. within 30 mins.Elderly 5-15 mgm. over 30 mins.IV Dose Rate: 2mg. over 3-5 min. Wait 5-10 minutes to evaluate effects.
Onset: 1-5min.
Peak: 2 min.
Duration: 15-60 min.
Metabolized: liver
Excreted: kidney
Administer into large vein
Inject close to IV siteIf additives in IV solution, flush tubing before and after administration.
Never IM
FLUMAZENIL(Anexate)
P- Elderly/debilitated
C- Hypersensitivity-Narrow angle glaucoma- Psychosis
S- CNS / resp. depression- N/V- Hypotension-Dizziness
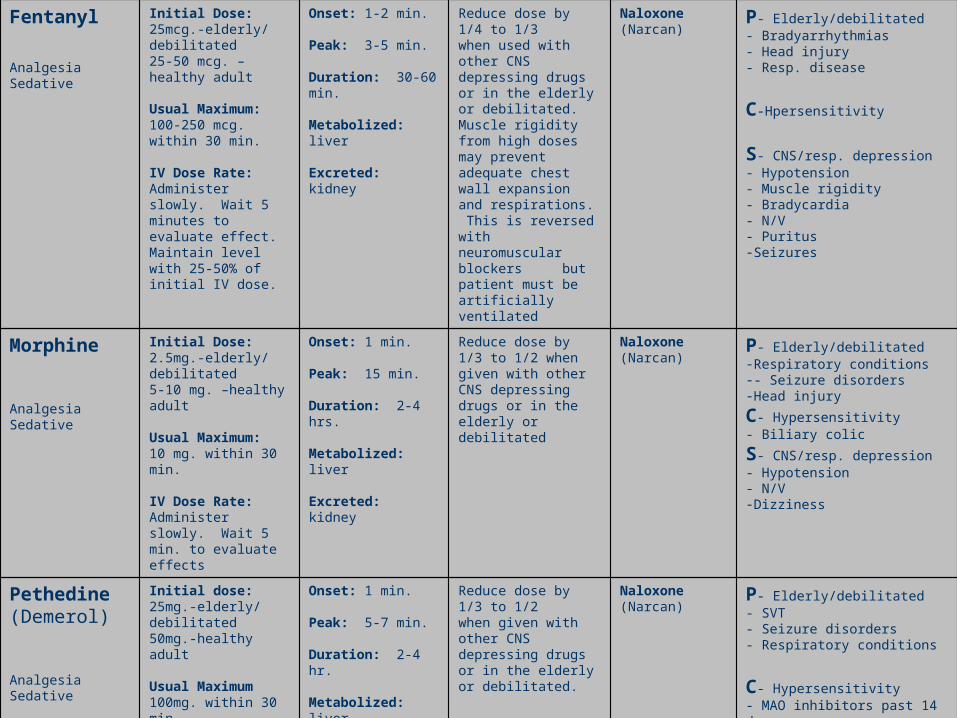
Fentanyl
AnalgesiaSedative
Initial Dose:25mcg.-elderly/debilitated25-50 mcg. –healthy adult
Usual Maximum:100-250 mcg. within 30 min.
IV Dose Rate:Administer slowly. Wait 5 minutes to evaluate effect. Maintain level with 25-50% of initial IV dose.
Onset: 1-2 min.
Peak: 3-5 min.
Duration: 30-60 min.
Metabolized: liver
Excreted: kidney
Reduce dose by 1/4 to 1/3when used with other CNS depressing drugs or in the elderly or debilitated.Muscle rigidity from high doses may prevent adequate chest wall expansion and respirations. This is reversed with neuromuscular blockers but patient must be artificially ventilated
Naloxone(Narcan)
P- Elderly/debilitated- Bradyarrhythmias- Head injury- Resp. disease
C-Hpersensitivity
S- CNS/resp. depression- Hypotension- Muscle rigidity- Bradycardia- N/V- Puritus-Seizures
Morphine
AnalgesiaSedative
Initial Dose:2.5mg.-elderly/debilitated5-10 mg. –healthy adult
Usual Maximum:10 mg. within 30 min.
IV Dose Rate:Administer slowly. Wait 5 min. to evaluate effects
Onset: 1 min.
Peak: 15 min.
Duration: 2-4 hrs.
Metabolized: liver
Excreted: kidney
Reduce dose by 1/3 to 1/2 when given with other CNS depressing drugs or in the elderly or debilitated
Naloxone(Narcan)
P- Elderly/debilitated-Respiratory conditions-- Seizure disorders-Head injuryC- Hypersensitivity- Biliary colicS- CNS/resp. depression- Hypotension- N/V-Dizziness
Pethedine(Demerol)
AnalgesiaSedative
Initial dose:25mg.-elderly/debilitated50mg.-healthy adult
Usual Maximum100mg. within 30 min.
IV Dose Rate:Administer slowly. Wait 5 minutes to evaluate effects
Onset: 1 min.
Peak: 5-7 min.
Duration: 2-4 hr.
Metabolized: liver
Excreted: kidney
Reduce dose by 1/3 to 1/2when given with other CNS depressing drugs or in the elderly or debilitated.
Naloxone(Narcan)
P- Elderly/debilitated- SVT- Seizure disorders- Respiratory conditions
C- Hypersensitivity- MAO inhibitors past 14 days
S- CNS/resp. depression- Hypotension- N/V

Thiopental (Pentothal)
General anaesthetic agent
Initial dose:50 - 100 mgUsual maximum:3mg/kgIncremental and maximum doses are reduced to 1/3- 1/2 in the elderly.
Onset: 1- 2 min Peak: 4-8 min
Duration of Action: 10 - 30 min
Metabolized: liver
Excreted: kidney
Reduce dose to 1/3 to 1/2when given with other CNS depressing drugs or in the elderly or debilitated.
- S- Hypotension, myocardial depression, CNS and respiratory depression, nausea, vomiting, diarrhea, laryngospasmC- Respiratory conditionsPorphyriasP- Inactive, debilitated, and elderly may be more susceptible to adverse effects. Increased toxicity with other CNS depressants
KETAMINE(Ketalar)
General anaesthetic agent
Initial dose:0.2 - 1.0 mg/kg
Usual maximum:2mg/kg.
Onset: 30 sec. IV 3-4 min. IM
Duration: 5-10 min. IV 12-25 min. IM
Full Recovery: 30-120 minInitial IV dose over 60 sec.(rapid administration may cause respiratory depression)
Antisecretory agent such as atropine (.01mgm/kg) or scopalamine given priorBarbituates and Ketamine should not be injected using the same syringe.Not recommended outside the OR.
- S- Nystagmus,resp. depression, hypersalivation, laryngospasm, non- purposeful movements, emesis, HR,B/P, ICP- “Emergence reaction”- Unpleasant dreams/hallucinations(most common in females>age 10)
C- Hx CV disease or hypertension- Active pulmonary infection or disease- Head injury- Glaucoma or acute globe injury- Psychosis- Conditions with intracranial hypertension- Seizure or CNS disorders- Hx of airway instability, tracheal surgery or stenosis
Propofol (Diprivan)
General anaesthetic agentAnti-emeticAnti-convulsant
Initial dose:10 - 20mg incremental doses every 5 minutes as neededUsual Maximum: 100mg. Give slow IV push to avoid hypotension.
Onset: 30 sec Duration of Action: 10 - 15 min
Reduce dose by 1/3 to 1/2when given with other CNS depressing drugs or in the elderly or debilitated.Restricted to monitored ICU/ED patients and/or use by anesthesia personnel
- S- Respiratory depression, - HR,B/PP- Hx CV disease or hypotension- Active pulmonary infection or disease- Concomitant use with narcotics- Hx of airway instability, tracheal surgery or stenosis

Drugs Used for Pediatric Sedation

DRUG Pediatric Dose ONSET SPECIAL CONSIDERATIONS
REVERSAL AGENT
PRECAUTIONS CONTRAINDICATIONS
& SIDE EFFECTS
MIDAZOLAM(Dormicum)
AnxiolyticSedativeAmnesicAnti-convulsant
No manufacturer published recommendations
Onset: 1 ½-5 min.Peak: 10-15 min.Duration: 60-90 min.Metabolized: liverExcreted: kidneyRecovery is dose dependent, usually 1-2 hrs.
Reduce dose by 1/3 to 1/2 when used with other CNS depressing drugs or in the debilitated.Manufacturer recommends not more than 1.5 mgm over at least two minutes in patients with decreased pulmonary reserves.
FLUMAZENIL(Anexate)
P- Debilitated
C- Hypersensitivity, acute narrow angle glaucoma
S- CNS / Resp. depression- Hypotension- Agitation- N/V, hiccups
DIAZEPAM (Valium)
SedativeAnxiolyticAnti-convulsant
No manufacturer published recommendationsClinician info:>30 days of age0.25mg/KG over 3 min. Can repeat in 15-30 min. until total of 0.75mg/Kg
Onset: 1-5min.Peak: 2 min.Duration: 15-60 min.Metabolized: liverExcreted: kidney
Administer into large vein
Inject close to IV site
If additives in IV solution, flush tubing before and after administration.
Never IM
FLUMAZENIL(Anexate)
P- Debilitated
C- Hypersensitivity- Narrow angle glaucoma- Psychosis
S- CNS /resp. depression- N/V- Hypotension-Dizziness

Fentanyl
AnalgesiaSedative
No manufacturer published recommendations
Onset: 1-2 min.
Peak: 3-5 min.
Duration: 30-60 min.
Metabolized: liver
Excreted: kidney
Reduce dose by 1/4 to 1/3when used with other CNS depressing drugs or in the debilitated.Muscle rigidity from high doses may prevent adequate chest wall expansion and respirations. This is reversed with neuromuscular blockers but patient must be artificially ventilated.
Naloxone(Narcan)
P- Debilitated- Bradyarrhythmias- Head injury- Resp. disease
C-Hpersensitivity
S- CNS/resp. depression- Hypotension- Muscle rigidity- Bradycardia- N/V- Puritus-Seizures
Morphine
AnalgesiaSedative
0.05-0.1mg/kg slowly Onset: 1 min.
Peak: 15 min.
Duration: 2-4 hrs.
Metabolized: liver
Excreted: kidney
Reduce dose by 1/3 to 1/2 when given with other CNS depressing drugs or in the debilitated.
Naloxone(Narcan)
P- Debilitated-Respiratory conditions-- Seizure disorders-Head injury-C- Hypersensitivity-Biliary colic-S- CNS/resp. depression- Hypotension- N/V-Dizziness
Pethedine(Demerol)
AnalgesiaSedative
1-2 mg/kg slowly Onset: 1 min.
Peak: 5-7 min.
Duration: 2-4 hr.
Metabolized: liver
Excreted: kidney
Reduce dose by 1/3 to 1/2 when given with other CNS depressing drugs or in the debilitated.
Naloxone(Narcan)
P- Debilitated- SVT- Seizure disorders- Respiratory conditionsC- Hypersensitivity- MAO inhibitors past 14 daysS- CNS/resp. depression- Hypotension- N/V

Thiopental (Pentothal)
General anaesthetic agent
Initial dose:50 - 100 mgUsual maximum:3mg/kgIncremental and maximum doses are reduced to 1/3- 1/2 in the elderly.
Onset: 1- 2 min Peak: 4-8 minDuration of Action: 10 - 30 minMetabolized: liverExcreted: kidney
Reduce dose to 1/3 to 1/2when given with other CNS depressing drugs or in the inactive or debilitated.
Not recommended outside the OR.
- S- Hypotension, myocardial depression, CNS and respiratory depression, nausea, vomiting, diarrhea, laryngospasm
C- Respiratory conditionsPorphyrias
KETAMINE(Ketalar)
General anaesthetic agent
Initial dose:0.2 - 1.0 mg/kg
Usual maximum:2mg/kg.
Onset: 30 sec. IV3-4 min. IM
Duration: 5-10 min. IV12-25 min. IM
Full Recovery: 30-120 minInitial IV dose over 60 sec.(rapid administration may cause respiratory depression)
Antisecretory agent such as atropine (.01mgm/kg) or scopalamine given priorBarbituates and Ketamine should not be injected using the same syringe.
Not recommended outside the OR.
- S- Nystagmus,resp. depression, hypersalivation, laryngospasm, non- purposeful movements, emesis, HR,B/P, ICP- “Emergence reaction”- Unpleasant dreams/hallucinations(most common in females>age 10)
C- Hx CV disease or hypertension- Active pulmonary infection or disease- Head injury- Glaucoma or acute globe injury- Psychosis- Conditions with intracranial hypertension- Seizure or CNS disorders- Hx of airway instability, tracheal surgery or stenosis
Propofol (Diprivan)
General anaesthetic agentAnti-emeticAnti-convulsant
Initial dose:10 - 20mg incremental doses every 5 minutes as needed
Usual Maximum: 100mg.
Give slow IV push to avoid hypotension.
Onset: 30 sec
Duration of Action: 10 - 15 min
Reduce dose by 1/3 to 1/2when given with other CNS depressing drugs or in the inactive or debilitated.
Restricted to monitored ICU/ED patients and/or use by anesthesia personnel
- S- Respiratory depression, - HR,B/P
P- Hx CV disease or hypotension- Active pulmonary infection or disease- Concomitant use with narcotics- Hx of airway instability, tracheal surgery or stenosis

Reversal Agents for Drugs used for Adult and Pediatric Sedation
DRUG
ACTION&
ONSET
ADMINISTRATION GUIDELINES
(In Adults)
PEDIATRIC DOSING SPECIAL CONSIDERATIONS
PRECAUTIONS CONTRAINDICATIONS
SIDE EFFECTS
NALOXONE(Narcan)
Reversal of narcotics
Onset: 1-2 min.
0.4mg. –2mg. IV
May repeat as needed in 2-3 min. intervals PRN
0.01mg/kg every 2-3 min.
May repeat as needed.
If does not produce desired outcome a subsequent dose of 0.1mg/kg may be administered.
Alternate infusion at 0.4mg/hour
Can precipitate VT/VF in patients with CV disease or receiving potentially cardiotoxic drugs.
P - Cardiovascular disease
C- Hypersensitivity- Narcotic dependency
S- N/V, sweating- Tachycardia, hypertension- Pulmonary edema
FLUMAZENIL(Anexate)
Reversal of benzodiazepine
induced sedation
Onset: 1-2 min.
Peak effect: 6-10 min.High Risk people may be necessary to increase interval between doses to over one minute.
Initial dose:0.2mgm. IV over 15 sec.Wait 45 sec, additional 0.2mg. doses at one minute intervals until maximum of 4 additional doses have been given.
Maximum cumulative dose is 1.0 mg.Repeat above in 20 min. if neededNo more than 3 mg. in one hour.
No manufacturer published recommendations
Can precipitate seizures in those with seizures controlled by benzodiazepines, with tricyclic depression overdose & with high risk for seizures.
P - Resedation, monitor for resedation, respiratory depression for up to 120 min. Resedation least likely in low dose sedation, (eg < 10mg Versed)
C- Hypersensitivity- Tricyclic antidepressant overdose- Benzodiazepine dependency
S - Visual disturbances, diaphoresis, seizures, arrhythmias

BEN
ZOD
IAZEPIN
ES


BEN
ZOD
IAZEPIN
ES• BINDING: Strongly bind to
plasma proteins• DISTRIBUTION: Highly lipid
soluble and accumulate in body fat
• t ½: MIDAZOLAM = 1.5-2.5 hrs, DIAZEPAM = 30-100 hrs
• METABOLISM: HEPATIC; hydroxylation and conjugation with glucuronic acid
• EXCRETION: Renal (urine), milk.• Freely cross placental barrier.• 1st trimester fetal abnormalities• 3rd trimester fetal dependence
and floppy-infant syndrome.

BEN
ZOD
IAZEPIN
ES

Adult SedationMidazolam (Dormicum):• A Benzodiazepine.
• Initial Dose: 1 - 2.5 mg (max. 2.5 mg).
• Maximum: 3.5 - 5 mg in 30 min.
• How to administer: Evaluate Your Patient first insert & secure IV Give The Initial Dose Slowly Wait 2 min to evaluate effects Give Incremental Dosing in order to maintain sedation level with ¼ of the initial dose DO NOT EXCEED MAX DOSE.
• Onset: 1 ½ -5 min - Peak: 10-15 min - Duration: 60-90 min.
• Recovery is dose dependent, usually 1-2 hrs.

• Pediatric Patients Less Than 6 Months of Age No manufacturer published recommendations
• Pediatric Patients 6 Months to 5 Years of Age: 0.05 to 0.1 mg/kg
• Pediatric Patients 6 to 12 Years of Age: 0.025 to 0.05 mg/kg
Pediatric Sedation Midazolam

• Elderly • Debilitated • Respiratory Disorders
• CNS / Resp. depression• Hypotension• Agitation• N/V• Hiccups
• Hypersensitivity• Acute narrow angle glaucoma

Adult Sedation
Diazepam (Valium):• A Benzodiazepine.
• Initial Dose: 2 mg (max. 2.5 mg).
• Maximum: 10-20 mg in 30 min (1/2 this dose in the elderly).
• How to administer: Evaluate Your Patient first insert & secure IV Give The Initial Dose Slowly Wait 5-10 min to evaluate effects Give Incremental Doses in order to maintain sedation level with ¼ of the initial dose DO NOT EXCEED MAX DOSE.
• Onset: 1-5 min - Peak: 20 min - Duration: 15-60 min.

• No manufacturer published recommendations
• > 1 month of age: 0.25 mg/kg over 3 min; Can repeat in 15-30 min until total of 0.75mg/kg (MAX DOSE)
Pediatric Sedation Diazepam

• Elderly • Debilitated • Respiratory Disorders
• CNS / Resp. depression• Hypotension• N/V• Dizziness
• Hypersensitivity• Acute narrow angle glaucoma• Psychosis

Potency
• Midazolam > Diazepam = 4:1
• Diazepam is a more cumulative drug, it has a long half life (≈30 hrs). Midazolam t½ =1-2hrs; less cumulative.

Adult SedationFentanyl:• A Potent Opioid.
• Initial Dose: 25-50 µg.
• Maximum: 100-250 µg in 30 min.
• How to administer: Evaluate Your Patient first insert & secure IV Give The Initial Dose Slowly Wait 5 min to evaluate effects Give Incremental Dosing in order to maintain sedation level with ¼- ½ of the initial dose DO NOT EXCEED MAX DOSE.
• Onset: 1-2 min - Peak: 3-5 min - Duration: 30-60 min.• Recovery is dose dependent, usually 1 hr.

• No manufacturer published recommendations
• We try 0.25-1 µg/kg/dose.
Pediatric Sedation Fentanyl

• Elderly • Debilitated • Respiratory Disorders• Bradyarrhythmias• Head injury
• CNS / Resp. depression• Hypotension, bradycardia• N/V, pruritus, seizures• Muscle rigidity
• Hypersensitivity

OPIO
ID A
GEN
TS• Derivatives of opium or synthetic derivatives
resembling the natural opioid agents• Morphine and codeine are naturally occurring agents
in opium• Extensively metabolized in the liver• Excreted in Urine• Meperidine is not recommended for use beyond
48hrs from build up of metabolites and risk of convulsions
• Bind to receptors in the CNS & PNS

Adult Sedation
Morphine:• An Opioid.
• Initial Dose: 2.5-10 mg.
• Maximum: 10 mg in 30 min.
• How to administer: Evaluate Your Patient first insert & secure IV Give The Initial Dose Slowly Wait 5 min to evaluate effects Give Incremental Dosing in order to maintain sedation level with ¼- ½ of the initial dose DO NOT EXCEED MAX DOSE.
• Onset: 1 min - Peak: 15 min - Duration: 2-4 hrs.

• 0.05 - 0.1 mg/kg slowly
Pediatric Sedation Morphine

• Elderly • Debilitated • Respiratory Disorders• Seizure disorders• Head injury
• CNS / Resp. depression• Hypotension• N/V, pruritus• Dizziness
• Hypersensitivity• Biliary colic

Adult Sedation
Meperidine, Pethidine (Demerol):• An Opioid.
• Initial Dose: 25-50 mg.
• Maximum: 100 mg in 30 min.
• How to administer: Evaluate Your Patient first insert & secure IV Give The Initial Dose Slowly Wait 5 min to evaluate effects Give Incremental Dosing in order to maintain sedation level with ⅓ - ½ of the initial dose DO NOT EXCEED MAX DOSE.
• Onset: 1 min - Peak: 5-7 min - Duration: 2-4 hrs.

• 1 - 2 mg/kg slowly
Pediatric Sedation Demerol

• Elderly • Debilitated • Respiratory Disorders• Seizure disorders• SVT
• CNS depression• Resp. depression
• Hypersensitivity• MAO inhibitors• Hypotension• N/V

Potency
Fentanyl > Morphine > Pethidine
Fentanyl > Morphine : 100 times
Morphine > Pethidine : 10 times
In equivalent doses ..0.1 mg/kg Morphine=
1mg/kg Pethidine=1µg/kg Fentanyl

Important Steps
Reversal of Sedation Drugs
1. Stop administering sedating/anesthetic agents
2. Open the airway / support ventilation
3. Support the circulation
4. Adminstre a reversal agent(s) in accordance to the given overdosage agent
5. Call for help !!

What’s The Most Important Part of a ….
Given “tool”?
THE CONCEPT OF RESCUE

Rescue from sedation means Rescue of a patient from a deeper level of sedation than intended is an intervention by a
practitioner proficient in airway management and life support measures
Adult sedation BLS and preferably ACLS
Pediatric Sedation BLS and preferably PALS

GOT TOO MUCH PAPERWORK??
RememberRemember, it’s a…, it’s a…

Maintain Continual Contact With Your Patient

JUST
OPEN THE AIRWAY

Reversal Agents for Drugs used for Adult and Pediatric Sedation
DRUG
ACTION&
ONSET
ADMINISTRATION GUIDELINES
(In Adults)
PEDIATRIC DOSING SPECIAL CONSIDERATIONS
PRECAUTIONS CONTRAINDICATIONS
SIDE EFFECTS
NALOXONE(Narcan)
Reversal of narcotics
Onset: 1-2 min.
0.4mg. –2mg. IV
(1-2 up to 100 micrograms/kg) May repeat as needed in 2-3 min. intervals PRN
0.01mg/kg every 2-3 min.
May repeat as needed.
If does not produce desired outcome a subsequent dose of 0.1mg/kg may be administered.
Alternate infusion at 0.4mg/hour
Can precipitate VT/VF in patients with CV disease or receiving potentially cardiotoxic drugs.
P - Cardiovascular disease
C- Hypersensitivity- Narcotic dependency
S- N/V, sweating- Tachycardia, hypertension- Pulmonary edema
FLUMAZENIL(Anexate)
Reversal of benzodiazepine
induced sedation
Onset: 1-2 min.
Peak effect: 6-10 min.High Risk people may be necessary to increase interval between doses to over one minute.
Initial dose:0.2mg IV over 15 sec.Wait 45 sec, additional 0.2mg. doses at one minute intervals until maximum of 4 additional doses have been given.
Maximum cumulative dose is 1.0 mg.Repeat above in 20 min. if neededNo more than 3 mg. in one hour.
No manufacturer published recommendations
Can precipitate seizures in those with seizures controlled by benzodiazepines, with tricyclic depression overdose & with high risk for seizures.
P - Resedation, monitor for resedation, respiratory depression for up to 120 min. Resedation least likely in low dose sedation, (eg < 10mg Versed)
C- Hypersensitivity- Seizure disorders- Tricyclic antidepressant overdose- Benzodiazepine dependency
S - Visual disturbances, diaphoresis, seizures, arrhythmias

Naloxone:
1. The reversal agent for opioid agents2. The dose may need to be repeated because the
duration of action of naloxone may be shorter than that of the narcotic being reversed
3. Acute narcotic reversal may cause pain, nausea, vomiting, hypertension and CHF
4. Desired effects are alertness and adequate ventilation without discomfort; naloxone should be titrated to effect in 0.1 mg increments to avoid serious side effects

Flumazenil:
1. Is a specific reversal agent for benzodiazepines?
2. May cause seizures in benzodiazepines dependent patients
3. Should be titrated in effect in 0.2 mg. increments over one minute

Risk Reduction Associated with Conscious Sedation

Causes of complicationsAssociated with Conscious Sedation Agents
• Inappropriate patient selection
• Unanticipated response
• Inappropriate monitoring of pharmacological effects
• Over-medication

Improve Patient Selection
• Use the ASA classification
• Assess airway
• Assess neurologic, psychological, and cardiorespiratory fitness
• Follow NPO guidelines

Prepare for Unexpected Events
• Anticipate for known abnormal reactions
• Adequate preparation of all necessary equipment
• Call for help
• Basic/Advanced life support

Adequate Monitoring of Drug Effects
• Establish standard monitoring for ALL CASES
• Maintain continual patient contact and observation


Prevention of Oversedation
• Use standard drug dosage and precautions (use distributed leaflets)
• Titrate dosage to response
• Allow enough time to a drug to appear
• Get reversal agents as well as other emergency drugs in reach of your hand
• Basic/Advanced life support


Any Questions
?

Summary
• Choose your patient carefully, learn about his/her body weight and comorbidities.
• Check and understand your monitoring and resuscitation equipment
• Use medication judiciously, remember you can’t take it out but you can always give more!
• Have reversal agents available but always remember basic resuscitation techniques.
• Be vigilant and prepare for the unexpected.