Embed Size (px)
Citation preview

Payment Models that Support Medical Home and ACO Principles:
Maryland’s Experience
Web Seminar
April 25, 2013
Follow this event on Twitter Hashtag: #AHRQIX

Using the Webcast Console and Submitting Questions
2
Click the Q&A widget to get the Q&A box to appear
To submit a question, type question here and hit submit.

Accessing Presentations
Download slides from console
Click on the “Download Slides” widget for a PDF version
3

What is the Health CareInnovations Exchange?
Publicly accessible, searchable database of health policy and service delivery innovations
Searchable QualityTools Successes and attempts Innovators’ stories and lessons learned Expert commentaries Learning and networking opportunities New content posted to the Web site every two weeks
Sign up at http://www.innovations.ahrq.gov under “Stay Connected”
4

Innovations Exchange Web Event Series
Archived Event MaterialsAvailable within two weeks under Events & Podcasts http://www.innovations.ahrq.gov
Next EventsThursday May 9, 2013 1-2pm ET
A Close Look at Care Coordination within Patient-Centered Medical Homes: West Virginia’s Experience
Wednesday June 5, 2013 1-2pm ET
Building Health Information Exchanges to Support Accountable Care Organizations and Medical Homes: Delaware’s Experience
5

Today’s Event Moderator
Meredith B. Rosenthal, PhD
Professor of Health Economics and Policy
Harvard School of Public Health
6

Motivation: Goals of New Accountability Contracts
When we seek root causes of quality gaps and When we seek root causes of quality gaps and cost problems, fragmentation rears its headcost problems, fragmentation rears its head
Payment reform can reduce fragmentation by Payment reform can reduce fragmentation by making a single entity accountable for all caremaking a single entity accountable for all care
Incentives and performance measurement are the Incentives and performance measurement are the key leverskey levers
Patient-centered medical homes are one such Patient-centered medical homes are one such concept and a building block for others including concept and a building block for others including accountable care organizationsaccountable care organizations
7

Patient-Centered Medical Home Basics
Joint Principles: physician-directed care; whole person Joint Principles: physician-directed care; whole person orientation; coordinated and integrated care; quality orientation; coordinated and integrated care; quality and safety; enhanced access; payment system that and safety; enhanced access; payment system that rewards value (i.e., not resource-based relative value rewards value (i.e., not resource-based relative value scale)scale)
National Committee for Quality Assurance has a National Committee for Quality Assurance has a measurement tool that has de facto become another measurement tool that has de facto become another definitiondefinition
Broadly, a set of structures, processes that improve Broadly, a set of structures, processes that improve access and reliability of care with a focus on individual access and reliability of care with a focus on individual patient needs and payment to support all of the abovepatient needs and payment to support all of the above
8

9
Initiatives Are Proliferating Private/public Patient-Centered Medical Home pilots Private/public Patient-Centered Medical Home pilots
have proliferated across the country have proliferated across the country All major national carriers are sponsoring some kind All major national carriers are sponsoring some kind
of pilot or initiativeof pilot or initiative Two Medicare demonstrationsTwo Medicare demonstrations Numerous existing and emerging Medicaid and other Numerous existing and emerging Medicaid and other
State –sponsored initiativesState –sponsored initiatives Hoped for effects: improved access and quality of Hoped for effects: improved access and quality of
care (population health); improved care coordination care (population health); improved care coordination and aggressive management of high-risk patients will and aggressive management of high-risk patients will equate to cost savingsequate to cost savings

Payment Incentives to Support Medical Homes
Fee for service is incompatible with medical home Fee for service is incompatible with medical home concepts: huddles, between visit monitoring, care concepts: huddles, between visit monitoring, care coordination, and support for self management are coordination, and support for self management are not reimbursablenot reimbursable
Payers may add a care management fee – per Payers may add a care management fee – per member per month – to cover these costsmember per month – to cover these costs
Such mixed payment may also soften productivity Such mixed payment may also soften productivity incentivesincentives
Pay for performance or shared savings used to get Pay for performance or shared savings used to get practices focused on quality, downstream costs practices focused on quality, downstream costs
10

Contracting Challenges with Medical Homes
Multi-payer environment may make it hard for Multi-payer environment may make it hard for practices to fully step off hamster wheelpractices to fully step off hamster wheel
Small primary care practices (arguably the place we Small primary care practices (arguably the place we want transformation the most) not good candidates want transformation the most) not good candidates for high-powered incentivesfor high-powered incentives
Shared savings subject to enormous random Shared savings subject to enormous random variation with small numbers of patientsvariation with small numbers of patients
Need to guard against possible unintended Need to guard against possible unintended consequences of patient access problems, provider consequences of patient access problems, provider financial lossesfinancial losses
11

Zoom Out to Accountable Care Organizations
Regardless of how successful medical homes are, Regardless of how successful medical homes are, primary care cannot fix fragmented care aloneprimary care cannot fix fragmented care alone
Building medical neighborhoods and entities large Building medical neighborhoods and entities large enough to manage total costs (i.e., Accountable Care enough to manage total costs (i.e., Accountable Care Organizations) is requiredOrganizations) is required
At a minimum payers should provide incentives for At a minimum payers should provide incentives for hospitals and specialists to work with medical homes hospitals and specialists to work with medical homes (e.g., BlueCross BlueShield Michigan)(e.g., BlueCross BlueShield Michigan)
12

Target Spending
Maximum shared savings = 7.5%*
Year1 max shared loss=5%* Year2 max shared loss=7.5%*
Year 3 max shared loss=10%*
Total sp ending
for AC
O patien ts
87.5%*
108.
3%*
112.
5% *
116.
7%*
Risk Corridor
$0
Slope = -0.6
2% minimum savings
Risk Sharing Arrangementsto/from ACO
*Percent of target 13

Key Takeaway Points
Integrated health care delivery requires payment Integrated health care delivery requires payment approaches with greater accountability for total costs approaches with greater accountability for total costs and outcomesand outcomes
Policy initiatives are simultaneously working to Policy initiatives are simultaneously working to encourage implementation of specific clinic models to encourage implementation of specific clinic models to manage populations and complementary payment manage populations and complementary payment mechanismsmechanisms
A spectrum of mixed payment and risk sharing A spectrum of mixed payment and risk sharing approaches are availableapproaches are available
Key issues of balancing appropriate risk, incentives Key issues of balancing appropriate risk, incentives against potential unintended consequencesagainst potential unintended consequences
14

Presenter
Ben Steffen, MA
15
Executive DirectorMaryland Health Care Commission

Maryland Program History
16
Studies in 2009 showedStudies in 2009 showedTools to enhance primary care are limited in Maryland lawTools to enhance primary care are limited in Maryland lawHigher payment for primary care alone would be inadequateHigher payment for primary care alone would be inadequate
Legislation in 2010 establishedLegislation in 2010 establishedAuthority of the state to launch a multi-payer PCMH pilotAuthority of the state to launch a multi-payer PCMH pilotExemption for a cost-based incentive payment tied to PCMH Exemption for a cost-based incentive payment tied to PCMH Authority for carriers to establish single carrier PCMH Authority for carriers to establish single carrier PCMH programs with incentive-based reward structure (shared programs with incentive-based reward structure (shared savings) and data sharingsavings) and data sharing

Maryland Health Care Commission
Convene stakeholders to form multi-payer Convene stakeholders to form multi-payer Patient-Centered Medical Home (PCMH) program: Patient-Centered Medical Home (PCMH) program: state action exemption to Federal anti-trust state action exemption to Federal anti-trust
Develop standards and approval process for Develop standards and approval process for single payer PCMH programs (2 programs single payer PCMH programs (2 programs recognized as of March 2013)recognized as of March 2013)
Participation in multi-payer: 5 commercial and 6 Participation in multi-payer: 5 commercial and 6 Medicaid managed care organizationsMedicaid managed care organizations
17

Overview: Multi-Payer Pilot
Pilots sites included 52 participating practices: Pilots sites included 52 participating practices: includingincluding 7 solo physician; 1 nurse practitioner-led; 18 small (2-5 7 solo physician; 1 nurse practitioner-led; 18 small (2-5 practitioners); 18 medium (6-10 practitioners); 8 large (11+ practitioners); 18 medium (6-10 practitioners); 8 large (11+ practitioners); 2 federally qualified health centerspractitioners); 2 federally qualified health centers
Practices are broadly dispersed across Maryland Practices are broadly dispersed across Maryland 330 providers including physicians and nurse 330 providers including physicians and nurse
practitionerspractitioners Participation agreement binds providers and Participation agreement binds providers and
payerspayers
18

19
Multi-Payer PCMH Program

20
What We Have Accomplished
Reached 250,000 privately insured and Medicaid patients Reached 250,000 privately insured and Medicaid patients National Committee for Quality Assurance (NCQA) National Committee for Quality Assurance (NCQA)
Patient-Centered Medical Home Recognition achieved by Patient-Centered Medical Home Recognition achieved by 52 practices with two-thirds achieving Level II or III at first 52 practices with two-thirds achieving Level II or III at first milestone by March 2012 and all Level I practices milestone by March 2012 and all Level I practices submitted for Level II or III by January 2013submitted for Level II or III by January 2013
All practices participated in quality reporting by submitting All practices participated in quality reporting by submitting 2011 and 2012 data: 7 of the Maryland measures are core 2011 and 2012 data: 7 of the Maryland measures are core or alternate under the Office of the National Coordinator or alternate under the Office of the National Coordinator (ONC) meaningful use; 8 of the 33 are ACO measures (ONC) meaningful use; 8 of the 33 are ACO measures

21
Key Features: Payment Model
Fee-For-ServicePrimary care practices continue to be reimbursed under their existing fee-for-service payment arrangements with health plans
Fixed “Transformation” PaymentPrimary care practices receive a per patient per month fee (paid semi-annually) between $3.50 and $6.00
Incentive Payment (Shared Savings)Primary care practices receive a share of actual savings generated by reducing total cost of care through improved patient outcomes
+Practices must achieve NCQA recognition; invest a portion of fixed payment in care coordination
Practices must report on a set of clinical quality and utilization measures with requirements increasing over 3 years

Multi-Payer Shared Savings
““Total cost of care” includes all health services Total cost of care” includes all health services regardless of whether the services are provided by regardless of whether the services are provided by the Patient-Centered Medical Home practicethe Patient-Centered Medical Home practice
Budget is set by practice’s baseline period costs Budget is set by practice’s baseline period costs inflated by state-wide trend (7.4% in 2010-2011)inflated by state-wide trend (7.4% in 2010-2011)
Practices whose total cost of care is below budget are Practices whose total cost of care is below budget are eligible to receive shared savings paymentseligible to receive shared savings payments
Practices receive from 30-50% of shared savings Practices receive from 30-50% of shared savings depending on the number of quality metrics reported depending on the number of quality metrics reported
22

Multi-Payer Shared Savings
Only patients attributed to the practice in both years Only patients attributed to the practice in both years are included in the calculationsare included in the calculations
Patient-level cost adjustments address outliers: Patient-level cost adjustments address outliers: patients that died; trauma cases excluded; costs for patients that died; trauma cases excluded; costs for patient are capped $75,000patient are capped $75,000
Savings calculations generated from All Payer Savings calculations generated from All Payer Claim Data Base: savings trend is established by Claim Data Base: savings trend is established by 2010-2011 cost analysis with non-participating 2010-2011 cost analysis with non-participating practicespractices
23
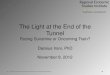
Shared Savings Results
Submitted Quality
Measures? # of Practices Pediatric
Adult/Adult Pediatric Hybrid
Yes 49 6 43
No 1 0 1
Generated Savings?
Yes 23 1 22
No 27 4 23
Eligible for Savings?
Yes 23 1 22
24

Did Practices Generate Savings?
25
All but 1 practice reported some quality metrics from All but 1 practice reported some quality metrics from electronic health records; 23 practices generated electronic health records; 23 practices generated savingssavings
Moderate relationship between reduced hospital days Moderate relationship between reduced hospital days and lower average costand lower average cost
Weaker relationship between reduced emergency room Weaker relationship between reduced emergency room visits and lower costsvisits and lower costs
Sample too small to access relationship between Sample too small to access relationship between reduced readmissions and lower costsreduced readmissions and lower costs
Random variation drove some savings; trimmed savings Random variation drove some savings; trimmed savings for practices that produced savings less than 10%for practices that produced savings less than 10%

Impact of Cap for Private Carriers
26
Shared Savings Payment Reduced under 10% Cap
11 Practices

27
Applying the Payer Agnostic Model Consistent shared savings model; multi-payer model similar to one-sided Consistent shared savings model; multi-payer model similar to one-sided accountable care organization modelaccountable care organization modelAlignment of quality metrics across initiativesAlignment of quality metrics across initiativesLink reward structure with state improvement goalsLink reward structure with state improvement goalsBroaden participation to carriers with small market shareBroaden participation to carriers with small market shareBuild trust in All-Payer Claims Database (attribution and shared savings)Build trust in All-Payer Claims Database (attribution and shared savings)
Sustaining Practice Transformation External practice transformation support is criticalExternal practice transformation support is criticalTransformation team embedded in the state Transformation team embedded in the state Ongoing funding is key Ongoing funding is key
Key Considerations

28
Care Coordination and ManagementProviders have opportunity to define the mix and should be held Providers have opportunity to define the mix and should be held accountable for resultsaccountable for resultsCombination of provider-based, payer-based, and community-Combination of provider-based, payer-based, and community-based support may work bestbased support may work best
Electronic Health Technology is Essential to Success National Committee for Quality Assurance PCMH Level 2 National Committee for Quality Assurance PCMH Level 2 recognition requires electronic health recordsrecognition requires electronic health recordsStandardized carrier data feeds needed Standardized carrier data feeds needed Link PCMH practices to Health Information Exchange (HIE) Link PCMH practices to Health Information Exchange (HIE) initiatives and encourage HIEs to develop tools to support new care initiatives and encourage HIEs to develop tools to support new care modelsmodels
Key Considerations

29
Enhance primary care functionsEnhance primary care functions Enhance coordination by engaging and link providersEnhance coordination by engaging and link providers Develop community health workforceDevelop community health workforce Align and link data systems including Health Align and link data systems including Health
Information Exchanges (HIE) capabilities for clinical Information Exchanges (HIE) capabilities for clinical management and All-Payer Claims Database for management and All-Payer Claims Database for provider efficiency and quality measurementprovider efficiency and quality measurement
Evolving Existing Efforts

30
Community Integrated MedicalHome
Planning Testing
1.Increase # of transformed practices
2.Increase payer participation
3.Engage communities
4.Standardize quality and efficiency measures
5.Link to broader population health goals
Evolving Advanced Primary Care Programs
6 months 3 years

Respondent
Craig Jones, MD
Executive Director
Vermont Blueprint for Health
31

Vermont Experience
Blueprint ModelAdvanced Primary Care PracticesAdvanced Primary Care PracticesCommunity Health Teams (core, extended)Community Health Teams (core, extended)Multi-Insurer Payment ReformsMulti-Insurer Payment ReformsHealth Information InfrastructureHealth Information InfrastructureEvaluation and ReportingEvaluation and ReportingCommunity Self-Management ProgramsCommunity Self-Management ProgramsLearning Health System (support, activities)Learning Health System (support, activities)
32

Vermont Experience
PCMH TransformationPayment Reform # 1
$PPPM - NCQA scoreAll Insurers
Community Health TeamsPayment Reform # 2
Shared CostsAll Insurers
Project ManagementGrantsBlueprint
Practice FacilitatorsGrantsBlueprint
Self Management WorkshopsGrantsBlueprint
Clinical Registry & Data QualityContractBlueprint
Financial Support Mechanism Product
Evaluation, Analytics, Modeling & Reporting
ContractBlueprint

Comments and ConsiderationsComments and Considerations
Is higher payment enough? What supports and Is higher payment enough? What supports and infrastructure are important for durable infrastructure are important for durable transformation? transformation?
To what degree can primary care organize more To what degree can primary care organize more holistic team based services?holistic team based services?
To what degree can primary care impact total To what degree can primary care impact total healthcare expenditures and costs?healthcare expenditures and costs?
Importance and complexity of establishing Importance and complexity of establishing common attribution and payment methods common attribution and payment methods across all insurers across all insurers
34

Comments and ConsiderationsComments and Considerations
What payment or blend of payments lead to effective What payment or blend of payments lead to effective and sustainable change?and sustainable change?
Capacity payment/investmentCapacity payment/investment
Quality based paymentQuality based payment
Outcomes based paymentOutcomes based payment
Shared savingsShared savings
What will prevail? … savings, savings, savings, or an What will prevail? … savings, savings, savings, or an effective blend of payments and infrastructure effective blend of payments and infrastructure investmentsinvestments
35

Vermont Experience: What’s in the Works
Continued expansion: PCMHs, community health Continued expansion: PCMHs, community health
teams, Support and Services at Home (SASH)teams, Support and Services at Home (SASH)
Front load community health teamsFront load community health teams
Data systems and data qualityData systems and data quality
Comparative assessments and practice profilesComparative assessments and practice profiles
Hub and spoke (addiction, mental health disorders)Hub and spoke (addiction, mental health disorders)
Foundation for next phases of reforms (ACOs, etc.)Foundation for next phases of reforms (ACOs, etc.)
36

Questions?
Click me to get Q&A box to appear
37

The Innovations Exchange
Visit our Web site:Visit our Web site:
http://www.innovations.ahrq.gov/
Learn more about Learn more about Maryland’s ProgramMaryland’s Program, , Vermont’s ProgramVermont’s Program, and , and Blueprint VideosBlueprint Videos
Follow us on Twitter:Follow us on Twitter:
#AHRQIX#AHRQIX
Send us emailSend us email:
38







![The Richard Merkin Initiative on Payment Reform and ... · PART 2: INNOVATIONS IN CARE . RGV ACO Diabetes Care Plan . The mission of the RGV ACO is to “[improve] the quality of](https://img.pdfslide.us/doc/110x75/5ed15a04fc37b04d07005cb8/the-richard-merkin-initiative-on-payment-reform-and-part-2-innovations-in-care.jpg)