Embed Size (px)
Citation preview

Confidential 2/17/2016Slide 1
Patient Centered Medical Home,A Pathway to Value-Based Reimbursement?
Industry Webcast
February 3, 2016
11:00 PT / 2:00 ET

Confidential 2/17/2016Slide 2
Today’s discussion
○ Introduction and overview
○ PCMH clinical and financial
performance
○ The alternative payment landscape,
and its link to PCMH
○ Core competencies,
today and tomorrow
○ The Christ Hospital: PCMH’s role in
practice transformation
○ Q&A
Confidential 2/17/2016Slide 3
Speaker introductions
David RoweSVP, Marketing & Business Development
Joe Siemienczuk, MD
Chief Medical Officer
Jacquelyn Hunt, PharmD, MS
Chief Population Health Officer
Amy Mechley, MD
Medical Director – Wellness Division,
The Christ Hospital Health Network

Confidential 2/17/2016Slide 4
Enli Health Intelligence
Top-Performing Population Health Management Solution
- KLAS Research. December 2015. Population Health Management 2015: How Far Can Your Vendor Take You?
Enli

Confidential 2/17/2016Slide 5
Patient Centered Medical Home
Gauging performance & progress

Confidential 2/17/2016Slide 6
What is PCMH, practically?
The medical home is best described as a model or
philosophy of primary care that is patient-centered,
comprehensive, team-based, coordinated,
accessible, and focused on quality and safety [ … ]
Above all, the medical home is not a final destination
instead, it is a model for achieving primary care
excellence…Source: Patient-Centered Primary Care Collaborative

Confidential 2/17/2016Slide 7
PCMH provides roadmap to advanced primary care practice
○ 7K+ practices recognized by NCQA1
○ 500%+ growth in PCMH incentive
programs—from 26 (2009) to 160 (2016)2
○ Fastest growing NCQA service PCMH certification also offered by URAC, The Joint Commission, AAAHC
1. Journal of the American Board of Family Medicine. Jan – Feb, 2016. Rosenthal. Are We Learning More
About Patient-Centered Medical Homes (PCMHs), or Learning About Primary Care?
2. Health Leaders Media. January 2016. Letourneau. PCMH Model Soaring, Despite Funding Challenges

Confidential 2/17/2016Slide 8
Enli customers are pursuing PCMH more aggressively than industry at-
large
33%
50%
9%
0%
10%
20%
30%
40%
50%
60%
70%
US PCP's Enli Customers
PCMH Program Participation
Live Planning
1. Enli Health Intelligence and PYA Consultants. National CCM Provider Survey 2015
2. Enli Health Intelligence. Alternative Payment Model Participation, December 2015
○ Enli customer
participation in
PCMH networks is
>50% greater than
the national average
○ Providers
participating in
PCMH are early
adopters of
government and
commercial APMs

Confidential 2/17/2016Slide 9
Evidence supports the efficacy of the PCMH model
14 peer-reviewed studies
› 10 reported on cost, 6 found
improvements
› 13 reported on utilization, 12
found improvements
› 3 reported on quality, 2 found
improvements
› 4 reported on access, 4 found
improvements
› 4 reported on satisfaction, 4
found improvements
Source: Patient-Centered Primary Care Collaborative.
January 2015. The Patient-Centered Medical Home’s
Impact on Cost and Quality
Confidential 2/17/2016Slide 10
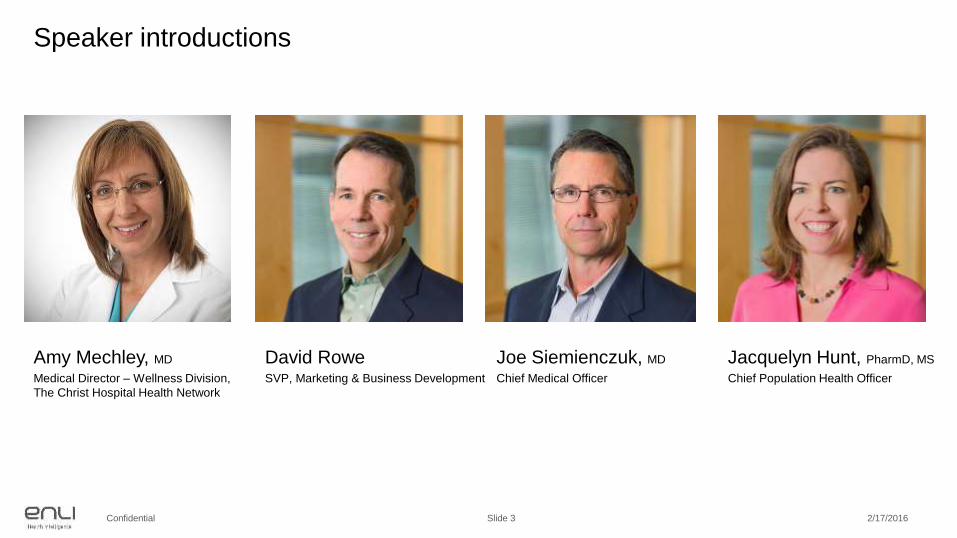
PCMH requires investment, but economics scale
○ $147,573, median annual cost1
○ $64,768 per clinician, $30 per patient1
○ 30% more, incremental short-term
impact to primary care costs2
1. Health IT Analytics. January 2016. RAND: Patient-Centered Medical Home May Cost $147K Per Year
2. JABFM. Jan – Feb, 2016. Rosenthal. Are We Learning More About Patient-Centered Medical Homes (PCMHs), or Learning About Primary Care?
3. Health IT Analytics. July 2014. CMSA Study: Patient Navigators Pay for Themselves in Two Months
○ 4%, reduction in the 30-day
readmission rate3
○ $156,000, combined savings per
navigator over six month period3
○ 2 months, average pay back period
for navigator (based upon $35K annual
salary)3

Confidential 2/17/2016Slide 11
○ HHS publishes clear objectives and goals to guide payment reform. The
proliferation of commercial and government reimbursement programs to
complement team-based delivery creates sustainable models
○ PCMH certification criteria developed and updated, providing discrete
measures and offering an onramp to other programs or models
(e.g. ACO certification)
○ The Health Care Payment Learning and Action Network launches, bringing
together public and private stakeholders to accelerate the transition to
alternative payment models
Catalyzing the transition from volume to value

Confidential 2/17/2016Slide 12
Alternative Payment Model Framework
Source: Health Care Payment Learning & Action Network, https://hcp-lan.org/workproducts/apm-whitepaper-onepager.pdf

Confidential 2/17/2016Slide 13
Medical homes well-positioned to pursue more aggressive payment
models
Payments in Category 3 are structured to
encourage providers to deliver effective and efficient
care
○ Primary care PCMHs are recognized within
Category 3 of HCP-LAN’s framework
○ PCMH practices have the flexibility to participate
in FFS reimbursement programs linked to quality
and value
○ PCMH practices accepting downside risk are
building competencies for population-based
payment programs

Confidential 2/17/2016Slide 14
…PCMH figures prominently in the Merit-Based
Incentive Payment System (MIPS), which aims to
accelerate the nation’s shift to pay-for-performance
reimbursement and financial bonuses based on quality
achievements using the PCMH as one of the most
promising foundations for systemic improvements.
Source: Health IT Analytics. January 2016. RAND: Patient-Centered Medical Home May Cost $147K Per Year

Confidential 2/17/2016Slide 15
Core Competencies, Today & Tomorrow
Teams, process, & technology

Confidential 2/17/2016Slide 16
PCMH standards & requirements
Standard Summary of Requirements
PCMH 1: Patient-Centered AccessThe practice provides 24/7 access to team-based care for both routine and urgent needs of patients/families/caregivers.
PCMH 2: Team-Based CareThe practice provides continuity of care using culturally and linguistically appropriate, team-based approaches.
PCMH 3: Population Health Management
The practice provides evidence-based decision support and proactive care reminders based on complete patient information, health assessment and clinical data.
PCMH 4: Care Management and Support
The practice systematically identifies individual patients and plans, manages and coordinates care, based on need.
PCMH 5: Care Coordination and Care Transitions
The practice systematically tracks tests and coordinates care across specialty care, facility-based care and community organizations.
PCMH 6: Performance Measurement and Quality Improvement
The practice uses performance data to identify opportunities for improvement and acts to improve clinical quality, efficiency and patient experience.

Confidential 2/17/2016Slide 17
Team-based approach to clinical care delivery
○ Clinic culture consistent with the medical home
○ Team-based training program
○ Central care team that provides support across
provider panels
○ Case management support for high-risk patients
○ Patient recognized as part of the care team

Confidential 2/17/2016Slide 18
Process to proactively engage & cost-efficiently operate
Continuous loop, grounded in ongoing
operational improvement
○ Mechanisms to identify high-risk patients
○ Communication forums and information sharing
○ Escalation procedures and triggers
○ Community connections
○ Integration of behavioral health
○ Patient access

Confidential 2/17/2016Slide 19
Technology platform to scale delivery model
○ Risk Stratification
● Tap clinical, claims, socioeconomic, health behavior data
● Build a population risk profile
● Define population goals consistent with contract requirements
○ Care Coordination
● Assign cohorts to programs
● Standardize workflows to minimize variation
● Assign tasks to team members according to licensure
● Forecast workload to align demand and capacity
○ Care Delivery
● Monitor, curate, and codify medical guidelines in the software
● Individualize care plans for patients
● Display opportunities complementary views across the enterprise
● Monitor and enhance patient health and engagement

Confidential 2/17/2016Slide 20
Challenge: Top of license teamwork

Confidential 2/17/2016Slide 21
Step 1: Filter by patients with an
appointment today

Confidential 2/17/2016Slide 22
Step 2: Rapid review of the Care Plan to
support pre-visit chart prep and
morning huddle. Use Memo for
communication and tasking

Confidential 2/17/2016Slide 23
Step 3: Easy-to-use tablet for collecting
patient information prior to the
visit

Confidential 2/17/2016Slide 24
Step 4: Hardwire evidence-based,
patient-specific standing orders
to support the rooming process

Confidential 2/17/2016Slide 25
Challenge: Test tracking & follow-up

Confidential 2/17/2016Slide 26
Step 1: Providers are able to easily
adjust cancer screening intervals

Confidential 2/17/2016Slide 27
Step 2: Filter by patients overdue for
cancer screening

Confidential 2/17/2016Slide 28
Step 3: Automated recall letter by mail,
or via the patient portal

Confidential 2/17/2016Slide 29
Step 4: Abnormal cancer work-up tracks
patients in a closed loop

Confidential 2/17/2016Slide 30
Challenge: ED follow-up

Confidential 2/17/2016Slide 31
Step 1: Population monitoring of
Emergency Department (ED)
visits

Confidential 2/17/2016Slide 32
ED Follow Up
Step 2: ED Follow-up Module enables
efficient, standard care
coordination

Confidential 2/17/2016Slide 33
Step 3: Patient goal setting includes
assessment of confidence and
barriers
Confidential 2/17/2016Slide 34
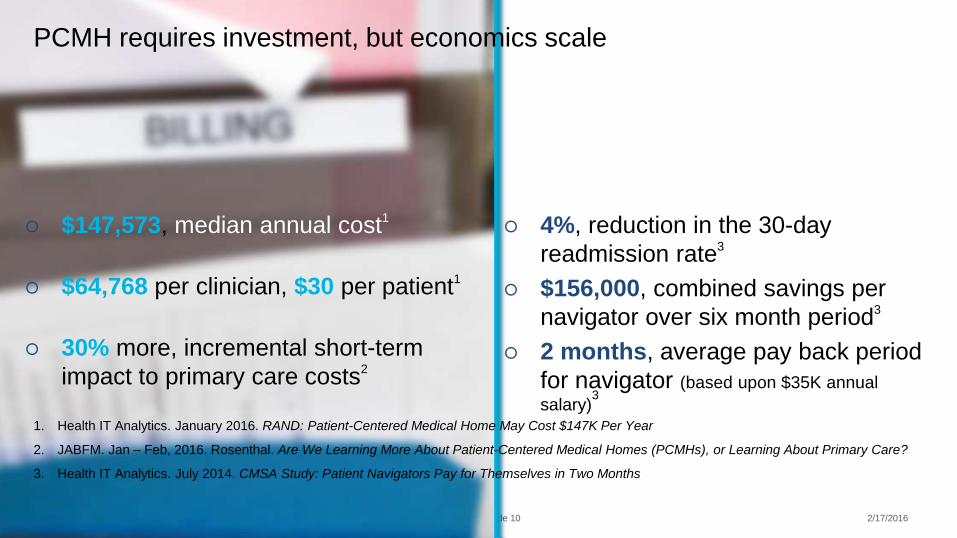
Step 4: Send patient an
Asthma Action Plan by mail,
or via the EHR portal

Confidential 2/17/2016Slide 35
CareManager addresses key PCMH certification standards
Standard FactorsDegree of Coverage
Product 360° Program EHR
PCMH 1: Patient-Centered Access
A. Patient-Centered Appointment Access X
B. 24/7 Access to Clinical Advise X
C. Electronic Access X
PCMH 2: Team-Based Care
A. Continuity X
B. Medical Home Responsibilities X X
C. Culturally & Linguistically Appropriate Services X
D. The Practice Team X X
PCMH 3: Population Health Management
A. Patient Information X
B. Clinical Data X
C. Comprehensive Health Assessment X X
D. Use Data for Population Management X X
E. Implement Evidence-Based Decision Support X X
Confidential 2/17/2016Slide 36
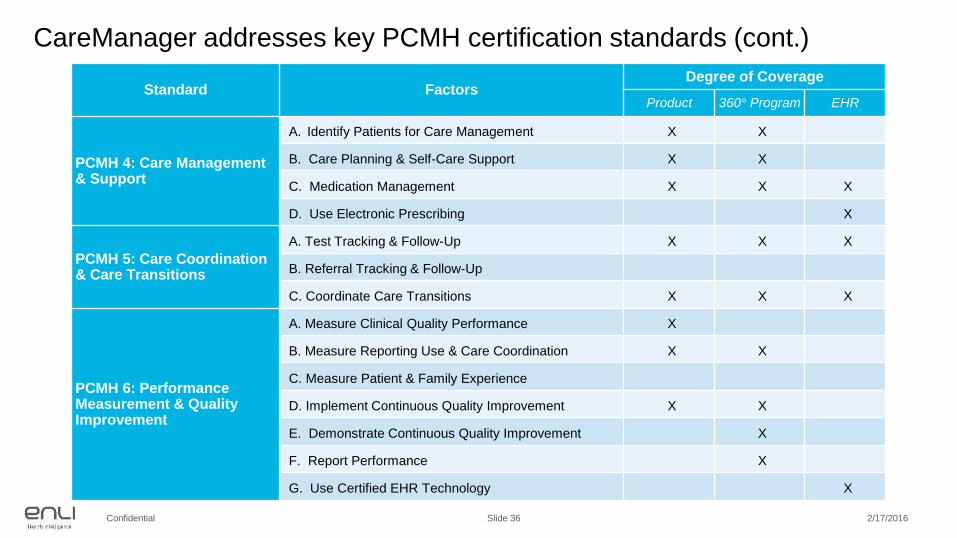
CareManager addresses key PCMH certification standards (cont.)
Standard FactorsDegree of Coverage
Product 360° Program EHR
PCMH 4: Care Management& Support
A. Identify Patients for Care Management X X
B. Care Planning & Self-Care Support X X
C. Medication Management X X X
D. Use Electronic Prescribing X
PCMH 5: Care Coordination & Care Transitions
A. Test Tracking & Follow-Up X X X
B. Referral Tracking & Follow-Up
C. Coordinate Care Transitions X X X
PCMH 6: Performance Measurement & Quality Improvement
A. Measure Clinical Quality Performance X
B. Measure Reporting Use & Care Coordination X X
C. Measure Patient & Family Experience
D. Implement Continuous Quality Improvement X X
E. Demonstrate Continuous Quality Improvement X
F. Report Performance X
G. Use Certified EHR Technology X

Confidential 2/17/2016Slide 37

Confidential 2/17/2016Slide 38
The Christ Hospital
PCMH & practice transformation
Confidential 2/17/2016Slide 39
The Christ Hospital Health Network
○ Integrated delivery system based in
Cincinnati, OH with a 555 bed acute care
hospital, 41 primary care locations, and
100+ ambulatory sites
○ Recognized national leader in clinical
excellence and patient experience
○ Focused on improving the health of the
TCH community and creating patient value
by providing exceptional outcomes,
affordable care, and the finest experiences

Confidential 2/17/2016Slide 40
The evolution of primary care…
Confidential 2/17/2016Slide 41
…The patient-doctor visit is no
longer the primary commodity.

Confidential 2/17/2016Slide 42
○ PCMH provides a framework to
evaluate clinical effectiveness and
supports our drive for better outcomes
○ PCMH standardizes best practices
across a broad network
○ PCMH aligns delivery with emerging
reimbursement models
● Commercial payers consider PCMH network
adoption in contracts
● State of Ohio has published 5-year roadmap
for payment reform on PCMH principles
● CMS is funding payment innovation
• MDs: 200+
• Staff: 1,000+
• Clinical specialties: 25
• Locations: 100+
• EHR platform: Epic
PCMH certification vs. PCMH methodology

Confidential 2/17/2016Slide 43
Value-based programs offer new revenue streams
○ Comprehensive Primary Care Initiative (CPCI)
● Multi-payer program providing primary care practices with monthly care
management payments to support practice transformation
● 4-year project: Yr. 1-2, limited risk; Yr. 3-4, base payment reduced 25% with gain
share
● Represents $10M over 4 years
● 16 of 34+ practices chosen for CPCI
○ Chronic Care Management (CCM)
● CMS-sponsored program that allows providers to bill ~$42 PMPM for non-face-to-
face care management services delivered to eligible Medicare beneficiaries
● Non-CPCI practices eligible to bill for service
● Represents $2M - $3M annually

Confidential 2/17/2016Slide 44
Team-based care was not designed into the EHR
○ The EHR user experience is
transactional, not actionable
○ EHRs are designed for data
capture, not visualization or
knowledge transfer
○ Epic ill-equipped to address more
rigorous 2014 NCQA PCMH
certification requirements, or
value-based programs like
CPCI and CCM

Confidential 2/17/2016Slide 45
Fewer resources
Quicker deployment
Higher functioning

Confidential 2/17/2016Slide 46
Financial impact > Commercial Medicare Results
Intentional investment on focused resources leads to significant improvements
Actual Earned Potential Available Actual Earned Potential Available
3%, of
$153,160
55%, of
$236,877
Q4 2014, MA Products
Q1 2015, MA Products

Confidential 2/17/2016Slide 47
Work effort > Commercial Medicare Advantage
CPCi and Non-CPCi Offices
366
118
53
93
33
417
17 12 4 7 12 12
0
50
100
150
200
250
300
350
400
450
Calls Made LMTCB Referral Placed Refused Called forReport/Waiting
Gap Closed
CPCi Offices Non-CPCi Offices

Confidential 2/17/2016Slide 48
YTD Performance > Clinical Quality Measures
Clinical Quality Measure
TCHHN
Performance
All CPC Region
Performance
Influenza Immunization 24% 37%
Tobacco Use Assessment and Cessation Intervention 94.04% 70%
Colorectal Screening 59.71% 42%
Breast Cancer Screening 63.53% 41%
Diabetes Hemoglobin A1c Poor Control (low % desirable) 11.47% 12%
Diabetes LDL Control (Patients screened for LDL test) 80.07% 62%
Diabetes LDL Control (Patients LDL < 100) 45.69% 42%
Blood Pressure Control 72.93% 68%
Ischemic Vascular Disease (Patients Screened for LDL test) 74.83% 58%
Ischemic Vascular Disease (LDL controlled) 49.74% 42%

Confidential 2/17/2016Slide 49

Confidential 2/17/2016Slide 50

Confidential 2/17/2016Slide 51
Confidential 2/17/2016Slide 52
Looking forward, what’s next?
○ TCHHN has committed to invest further in CareManager,
upgrading to incorporate additional clinical evidence to address
at-risk populations
Deployment within 6 weeks
○ TCHHN is installing CareManager Central Worklist to help with
the efficiency and effectiveness of our care teams engaged in
PCMH outreach
○ TCHHN is augmenting its technology platform and delivery
model with creative strategies focused on patient engagement!

Confidential 2/17/2016Slide 53
CareManager supports PCMH & can help put you on the path to VBR
“Enli stand outs due to its 'Knowledge to Action,' which
introduces real-time clinical decision support at the
point of care by synthesizing the latest evidence-based
guidelines and codifying them in the software”
Matt Guldin,
Chilmark Research
Clinical
decisions
informed by
evidence

Confidential 2/17/2016Slide 54
Questions & Answers
Confidential 2/17/2016Slide 55
Schedule a meeting, or stop by!
○ February 29th – March
4th
○ Upper Floor, Hall C
○ Booth #4461
Find us at HIMSS’16

Confidential 2/17/2016Slide 56
Thank you.