Embed Size (px)
Citation preview
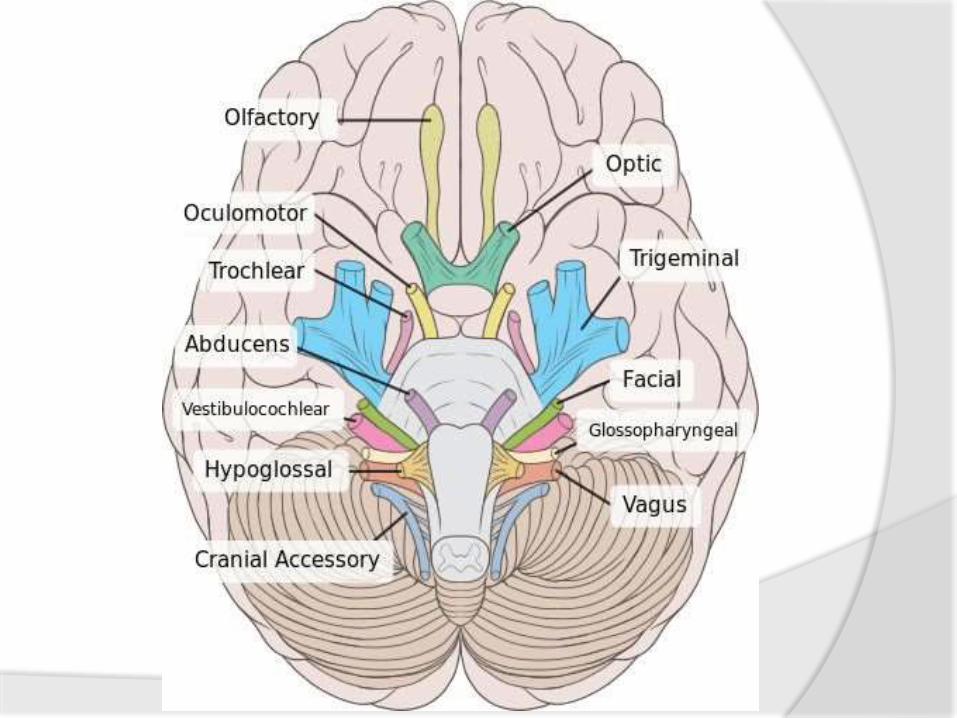
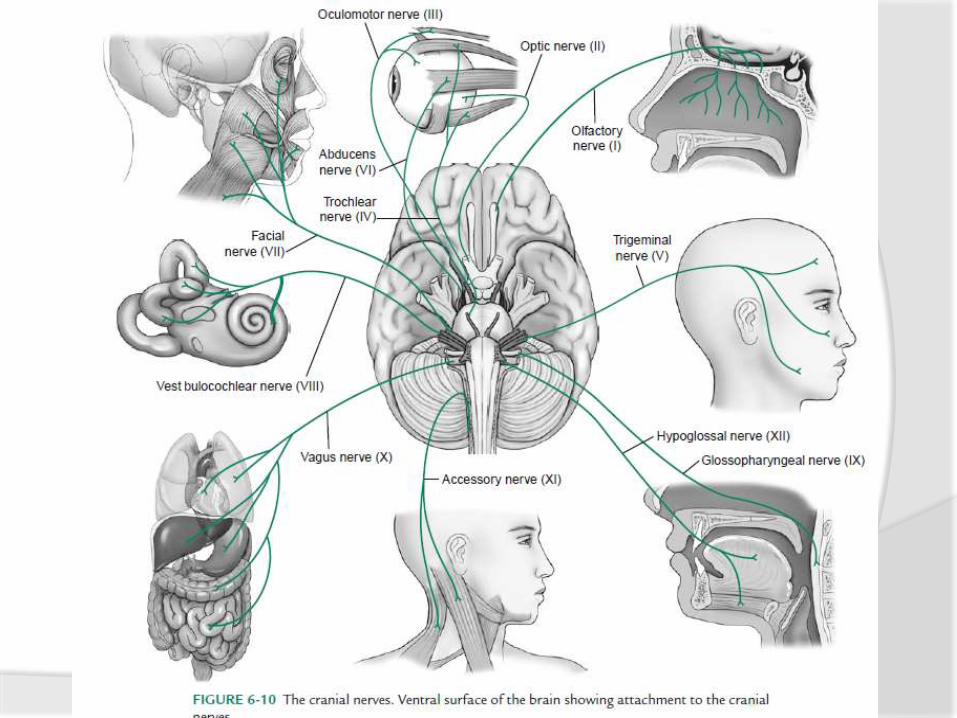
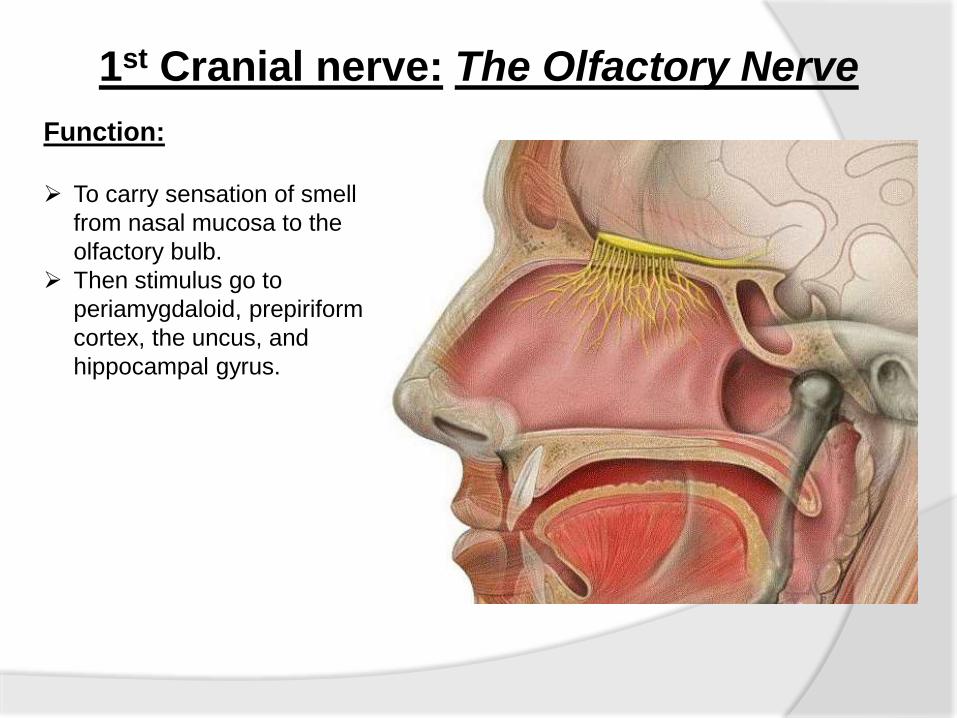
1st Cranial nerve: The Olfactory Nerve
Function:
To carry sensation of smell
from nasal mucosa to the
olfactory bulb.
Then stimulus go to
periamygdaloid, prepiriform
cortex, the uncus, and
hippocampal gyrus.
Test- Small bottles of familiar orders are required. Coffee
chocolate, lemon are mainly taken.
Patient first sniffing through each nostril to show
the airway is clear.
The test odour is placed on one nostril while other
is compressed.
Then he asked if he can smell anything and
identifying the odour.
Then test is repeated using other nostril and asked
whether the odour is same in each nostril.
After some time the test is repeated with other
odour and asked if he can distinguish the different
odour.
Result-o Those for whom each odour smells the same but
unpleasant- Parosmia
o Those who smell nothing in one or both nostrils or
whose sense much reduced on one sided
compaired to other- Ansomia
2nd cranial nerve:- The Optic NerveTest for-1. Visual acuity
2. Visual Field
3. Colour vision
4. Pupillary reaction
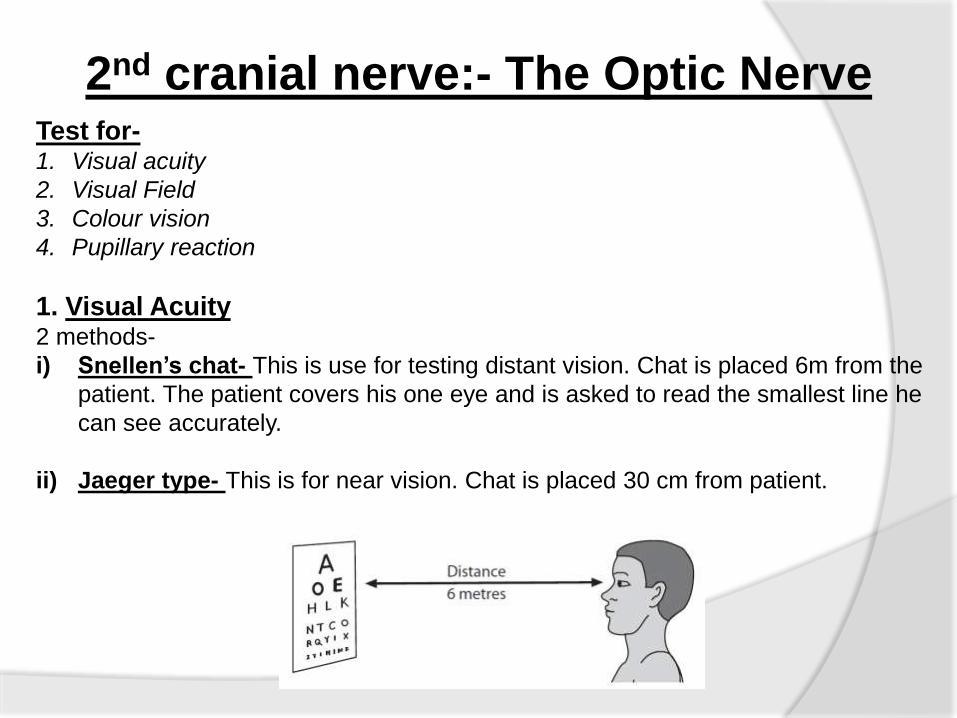
1. Visual Acuity2 methods-
i) Snellen’s chat- This is use for testing distant vision. Chat is placed 6m from the
patient. The patient covers his one eye and is asked to read the smallest line he
can see accurately.
ii) Jaeger type- This is for near vision. Chat is placed 30 cm from patient.
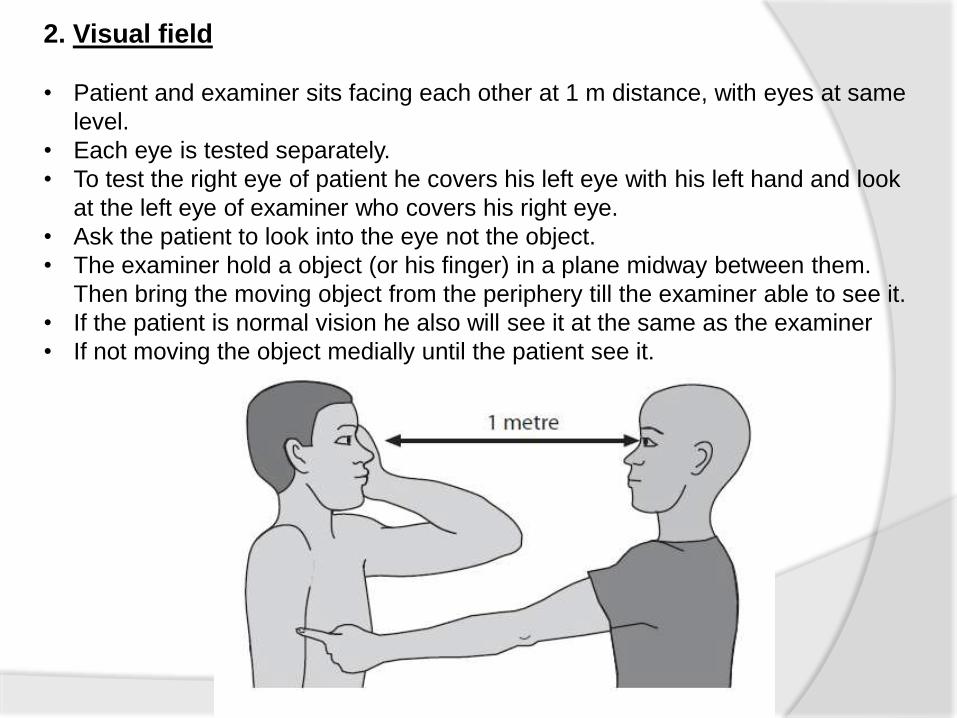
2. Visual field
• Patient and examiner sits facing each other at 1 m distance, with eyes at same
level.
• Each eye is tested separately.
• To test the right eye of patient he covers his left eye with his left hand and look
at the left eye of examiner who covers his right eye.
• Ask the patient to look into the eye not the object.
• The examiner hold a object (or his finger) in a plane midway between them.
Then bring the moving object from the periphery till the examiner able to see it.
• If the patient is normal vision he also will see it at the same as the examiner
• If not moving the object medially until the patient see it.
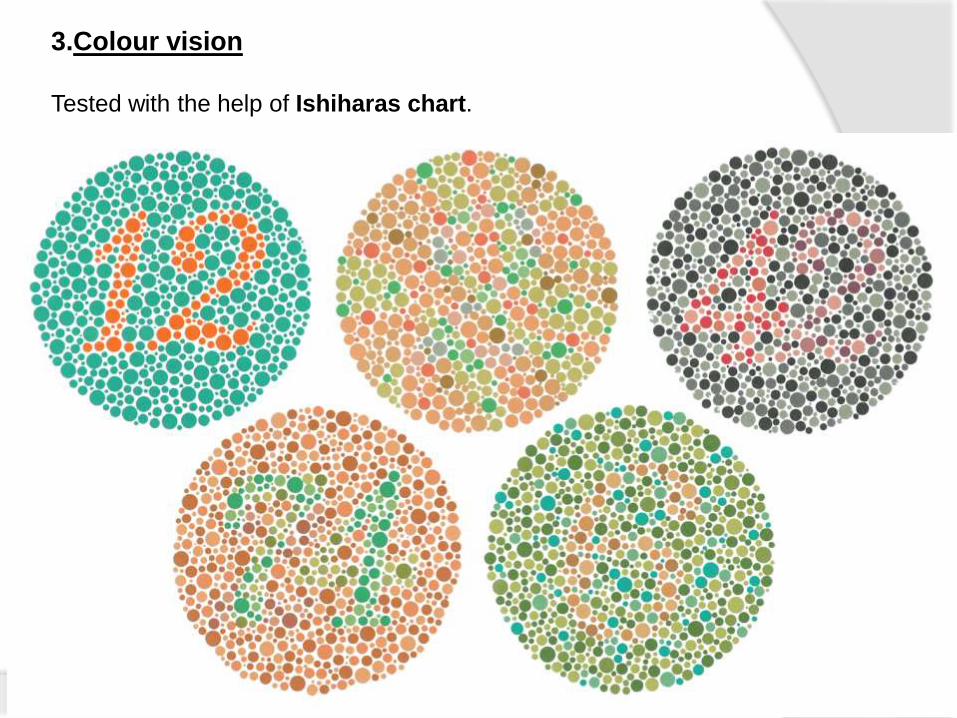
3.Colour vision
Tested with the help of Ishiharas chart.
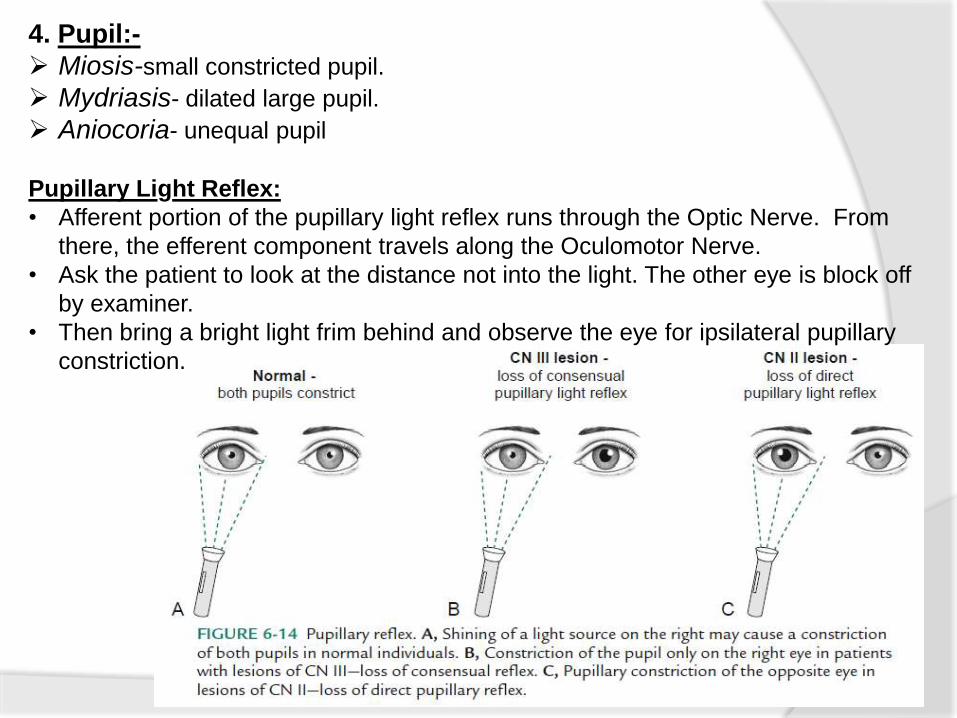
4. Pupil:-
Miosis-small constricted pupil.
Mydriasis- dilated large pupil.
Aniocoria- unequal pupil
Pupillary Light Reflex:
• Afferent portion of the pupillary light reflex runs through the Optic Nerve. From
there, the efferent component travels along the Oculomotor Nerve.
• Ask the patient to look at the distance not into the light. The other eye is block off
by examiner.
• Then bring a bright light frim behind and observe the eye for ipsilateral pupillary
constriction.
3rd , 4th, 6th cranial nerves:- The Oculomotor,
Trochlear, Abducent Nerves.
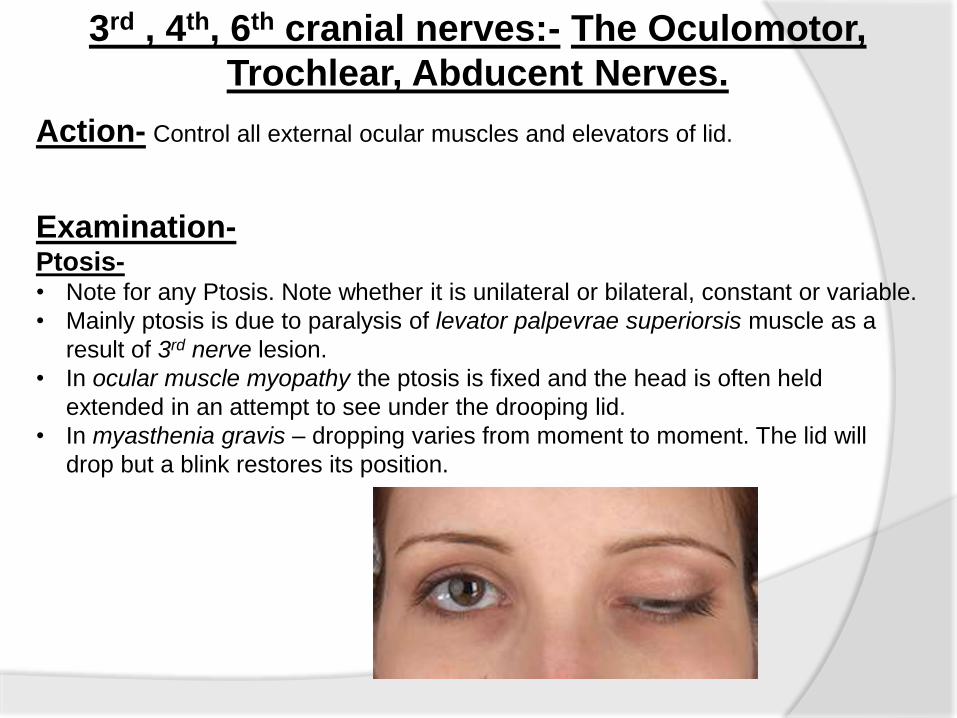
Action- Control all external ocular muscles and elevators of lid.
Examination-Ptosis-• Note for any Ptosis. Note whether it is unilateral or bilateral, constant or variable.
• Mainly ptosis is due to paralysis of levator palpevrae superiorsis muscle as a
result of 3rd nerve lesion.
• In ocular muscle myopathy the ptosis is fixed and the head is often held
extended in an attempt to see under the drooping lid.
• In myasthenia gravis – dropping varies from moment to moment. The lid will
drop but a blink restores its position.
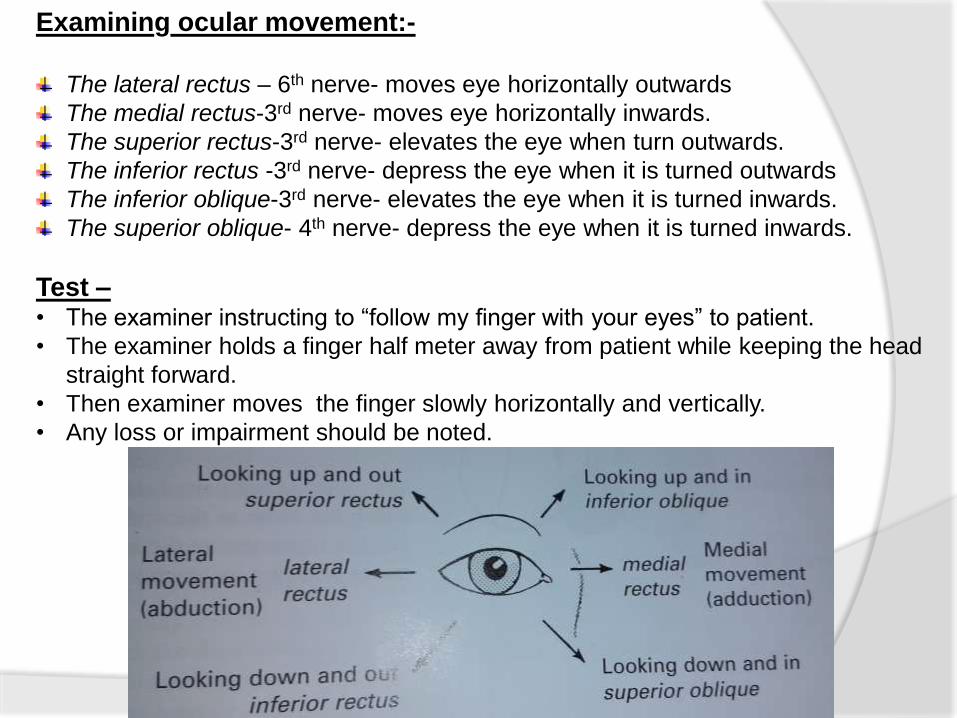
Examining ocular movement:-
The lateral rectus – 6th nerve- moves eye horizontally outwards
The medial rectus-3rd nerve- moves eye horizontally inwards.
The superior rectus-3rd nerve- elevates the eye when turn outwards.
The inferior rectus -3rd nerve- depress the eye when it is turned outwards
The inferior oblique-3rd nerve- elevates the eye when it is turned inwards.
The superior oblique- 4th nerve- depress the eye when it is turned inwards.
Test –• The examiner instructing to “follow my finger with your eyes” to patient.
• The examiner holds a finger half meter away from patient while keeping the head
straight forward.
• Then examiner moves the finger slowly horizontally and vertically.
• Any loss or impairment should be noted.
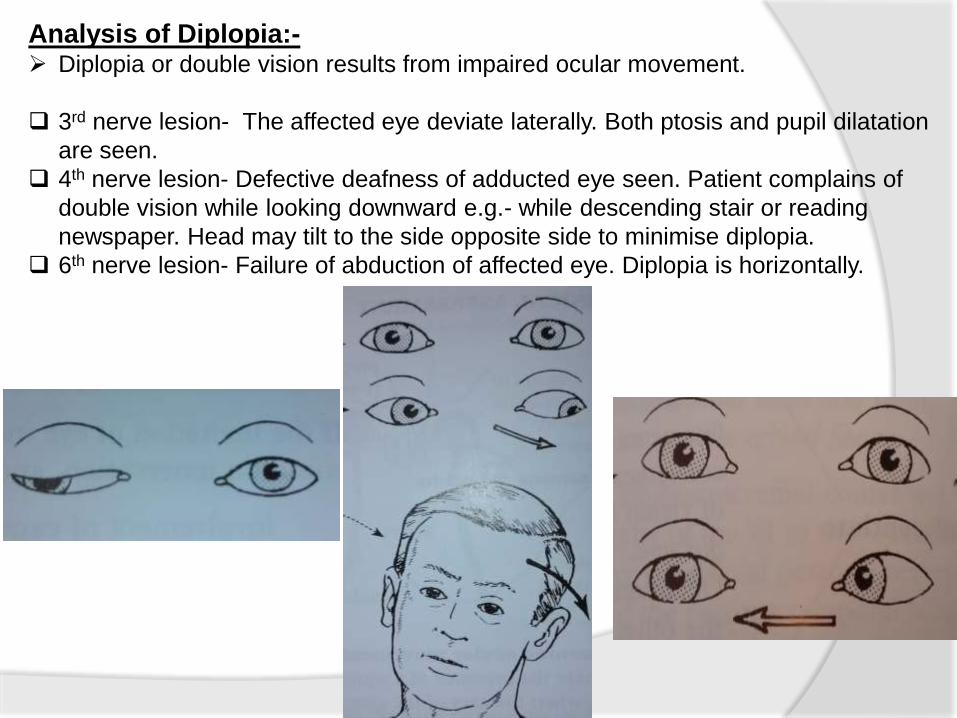
Analysis of Diplopia:- Diplopia or double vision results from impaired ocular movement.
3rd nerve lesion- The affected eye deviate laterally. Both ptosis and pupil dilatation
are seen.
4th nerve lesion- Defective deafness of adducted eye seen. Patient complains of
double vision while looking downward e.g.- while descending stair or reading
newspaper. Head may tilt to the side opposite side to minimise diplopia.
6th nerve lesion- Failure of abduction of affected eye. Diplopia is horizontally.
Analysing Nystagmus-
• Notice the nystagmus and note whether it is constant or variable.
• Patient is asked to look to a definite point or the finger (about 60 cm distance)
and then move it to left and right, upward and downward.
• Avoid long time (more than 30 sec) holding because muscle will fatigue and may
cause nystagmus in normal eye.
• So do the test for 5-10 sec.
*Note-A complete Oculomotor palsy will manifest as ptosis, dilated and fixed
pupil, and outward and slightly downward deviation of the eye.
5th cranial nerve:- The Trigeminal Nerve
Function:- It carry all form of sensation from the face, anterior part of scalp, the eye, the
anterior 2/3 of tongue.
To give motor power to muscles of mastication.
To carry all sensation from the teeth, gums, mucosa membrane of cheeks, nasal
passage, palate and nasophrynx.
Test-Sensory-
• Ask the patient if he feels any numbness or altered sensation on the face.
• Then test for light touch temperature sensation in each of 3 division of trigeminal
nerve by comparing one side with other side.
o The forehead and upper part of side of nose for opthalmic division.
o The malar region and upper lip for maxillary division.
o The chin and anterior par of tongue for mandibular division.
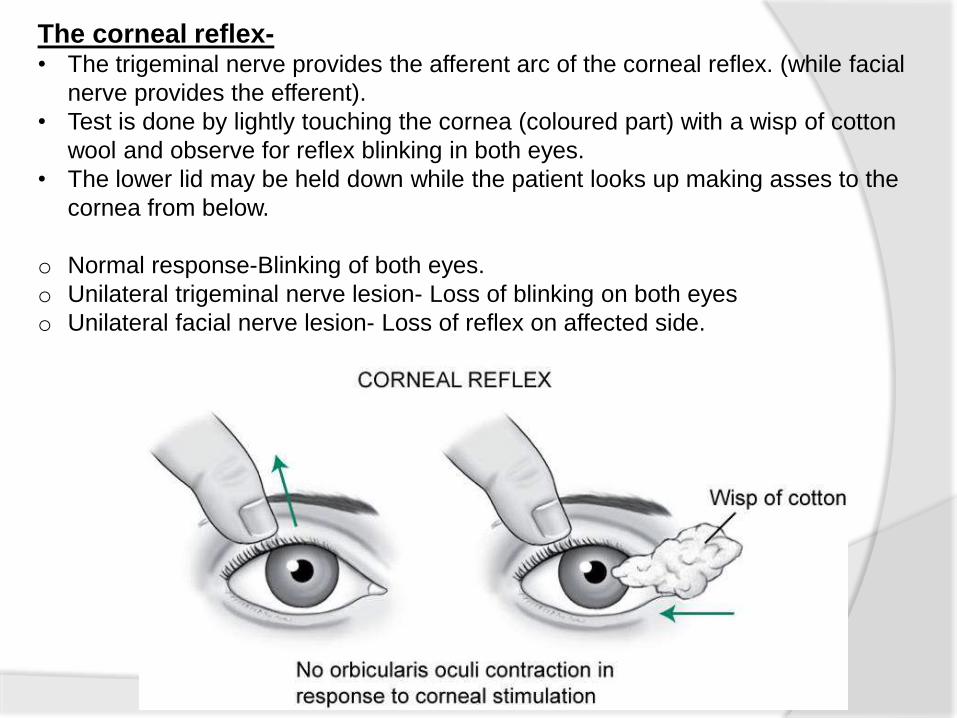
The corneal reflex-• The trigeminal nerve provides the afferent arc of the corneal reflex. (while facial
nerve provides the efferent).
• Test is done by lightly touching the cornea (coloured part) with a wisp of cotton
wool and observe for reflex blinking in both eyes.
• The lower lid may be held down while the patient looks up making asses to the
cornea from below.
o Normal response-Blinking of both eyes.
o Unilateral trigeminal nerve lesion- Loss of blinking on both eyes
o Unilateral facial nerve lesion- Loss of reflex on affected side.
Motor examination:-
Masseter and temporalis- ask the patient to clench his teeth and palpate
the contraction.
Lateral pterygoid- Ask the patient to open his mouth widely but slowly.
Note the movement of chin and look for any deviation. Jaw deviates to
paralysed side.
Both lateral pterygoid and medial pterygoid- Ask the patient to move his
lower jaw from side to side. If the muscles of one side are paralysed, the
movement of jaw to opposite side is weak or absent.
Jaw jerk –Test-
• Patient is told to open the mouth slightly.
• Examiner places a finger below the lower lip and taps it in a downward
direction with the percussion hammer.
Normal people- upward jerk seen
Abnormalities- in UMN lesion it is exaggerated and jaw clonous maybe
found.
* When patient has pathological exaggeration of all tendon reflexes in arm, and
legs, an exaggerated jaw jerk shows the lesion must be higher than the
cervical level.
7th cranial nerve:- The facial nerve
Function- Motor- facial expression and facial movement
Sensory – carry taste sensation from anterior 2/3 of tongue, sensory to outer ear.
Test-
Inspection-
• Note for wrinkle in forehead, nasolabial fold, movement of mouth while talking,
smiling.
• Also note for any twitching, tremour, or other involuntary movement in facial
muscle.
Examination of taste – This can be done by putting each drop from sugar, salt,
vinegar on tongue.in between each taste ,tongue should be clear with water.
Secretory function- saliva taste- The flow of saliva by placing a highly spicy
substance on the tongue and asked him to rise the tip of tongue ,so that examiner
see the submaxilary saliva flow.
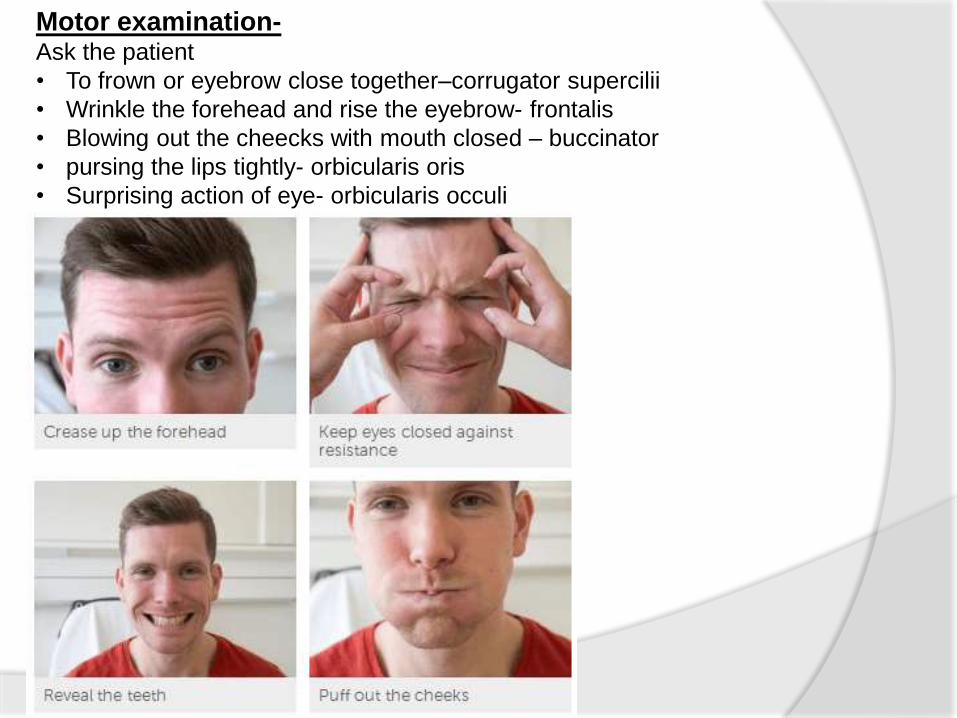
Motor examination-Ask the patient
• To frown or eyebrow close together–corrugator supercilii
• Wrinkle the forehead and rise the eyebrow- frontalis
• Blowing out the cheecks with mouth closed – buccinator
• pursing the lips tightly- orbicularis oris
• Surprising action of eye- orbicularis occuli
8th cranial nerve- The auditory nerve
Function- The cochlear nerve- it carry impulse of sound from organ of corti to the pons.
The vestibulocochlear nerve- it carries impulses from labyrinth to cerebellum.
Test-
Rinne’s test- (test compares air and bone conduction)
• Strike a tuning fork softly.
• Place the base of vibrating tuning fork on the mastoid bone.-bone conduction
• Ask the patient to tell you when the sound is no longer heard.
• Then move the fork in front of the ear – air conduction
• Ask if sound still heard.
• Normally air conduction is better then bone conduction that is the patient will
still hear the sound when place near the external meatus.
In conductive deafness the bone conduction is better than air conduction.
In nerve deafness both air and bone conduction are reduced. But in air
conduction sound still heard.
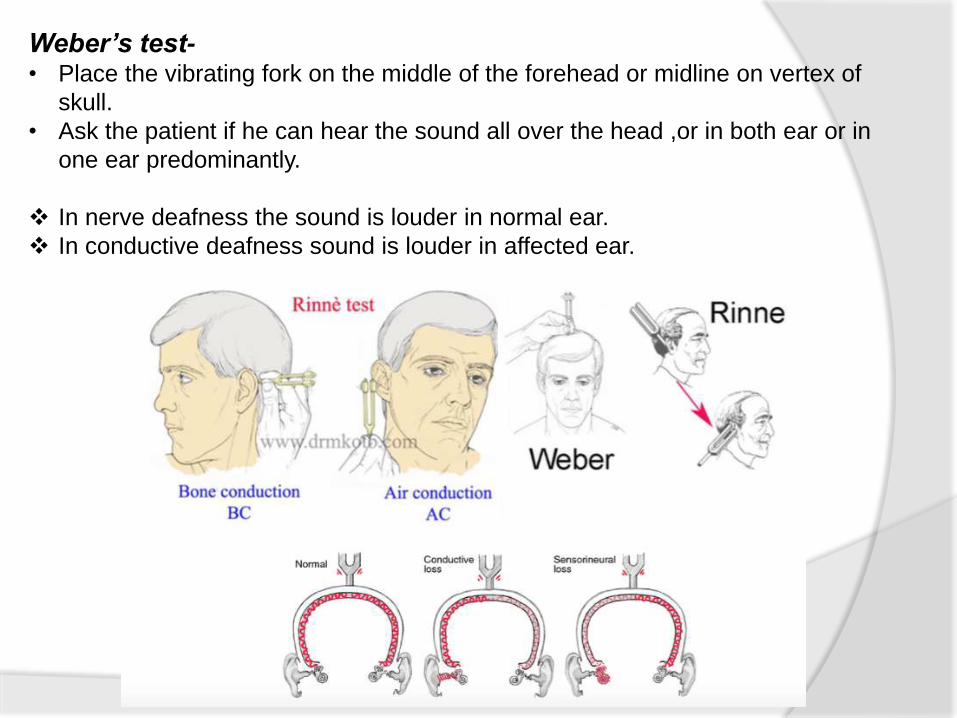
Weber’s test-• Place the vibrating fork on the middle of the forehead or midline on vertex of
skull.
• Ask the patient if he can hear the sound all over the head ,or in both ear or in
one ear predominantly.
In nerve deafness the sound is louder in normal ear.
In conductive deafness sound is louder in affected ear.
9th and 10th cranial nerves – The
Glossopharyngeal and the Vagus nerve
Function- Glossopharyngel – supplies the stylopharyngeus muscle of phrynx.
Sensory supplies to posterior one third of tongue and pharynx, tonsils ,palate,
nasopharynx.
Secretory fibre supplies parotid gland.
Vagus nerve – its sympathetic fibre supplies pharynx, Respiratory and
gastrointestinal system. Also its motor branch supply subpalate, pharynx, larynx
muscles.
Examination-Motor examination –
o Notice for pitch and quality of the patient’s voice and of his cough and ask for any
swallowing difficulty .
o High pitched or horse voice may mean vocal cord paralysis.
o A nasal tone may mean palatal paralysis.
o If the patient choke’s on his saliva while talking, there may be both palatal and
pharyngeal weakness.
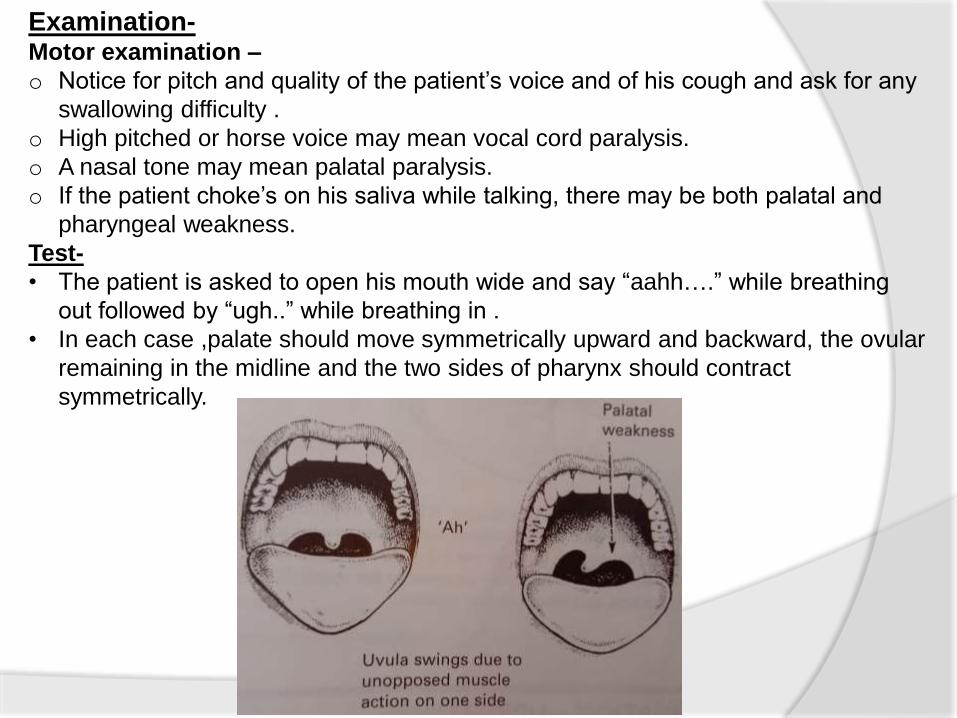
Test-
• The patient is asked to open his mouth wide and say “aahh….” while breathing
out followed by “ugh..” while breathing in .
• In each case ,palate should move symmetrically upward and backward, the ovular
remaining in the midline and the two sides of pharynx should contract
symmetrically.
Sensory examination-
Test-
• Generally test is difficult so using a galvanic current with the anode on
either side of the posterior part of tongue will produce a metallic taste.
• The patient is asked whether he is able to detect or not.
Gag reflex-
• Ask the patient to open his mouth ,now gently touch both side of
pharyngeal wall one after other and depress the tongue if necessary.
• Normally contraction of pharynx with elevation of the roof of tongue and
a feeling to vomit is seen.
• Absent of gag reflex means loss of sensation (9th nerve)and/or loss of
motor power (10th nerve).
11th cranial nerve – The assesory spinal nerve
Function:- Provide motor supply to Upper part of trapizius muscle and
sternocledomastoid muscle.
Examination-
Observation-
Trapezius weakness may be suspected if the head falls forward and SCM if it falls
downward.
.
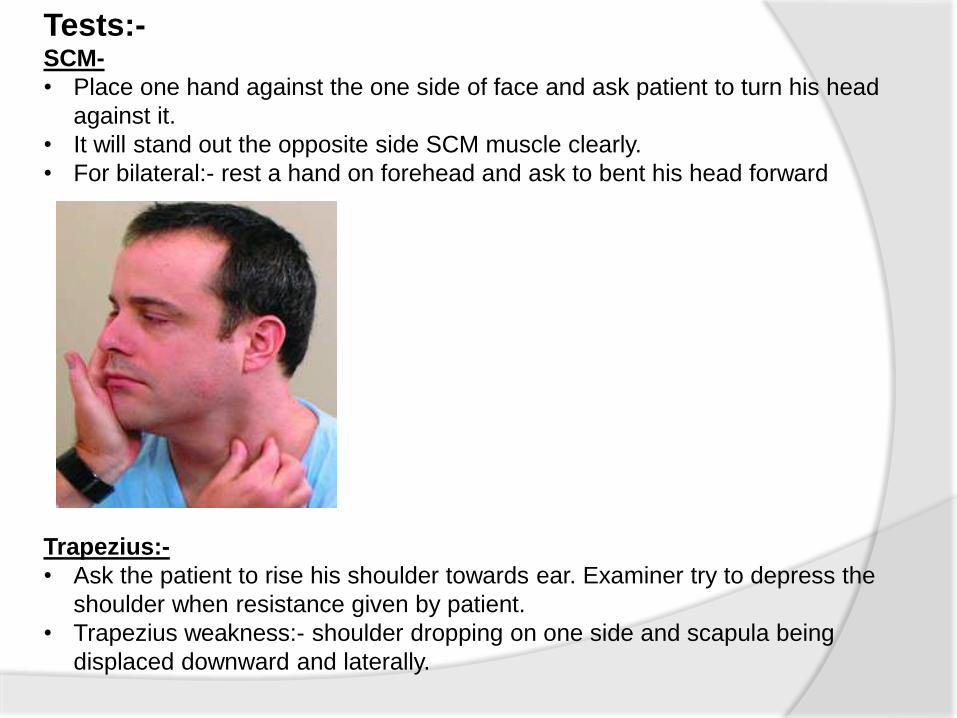
Tests:-SCM-
• Place one hand against the one side of face and ask patient to turn his head
against it.
• It will stand out the opposite side SCM muscle clearly.
• For bilateral:- rest a hand on forehead and ask to bent his head forward
Trapezius:-
• Ask the patient to rise his shoulder towards ear. Examiner try to depress the
shoulder when resistance given by patient.
• Trapezius weakness:- shoulder dropping on one side and scapula being
displaced downward and laterally.
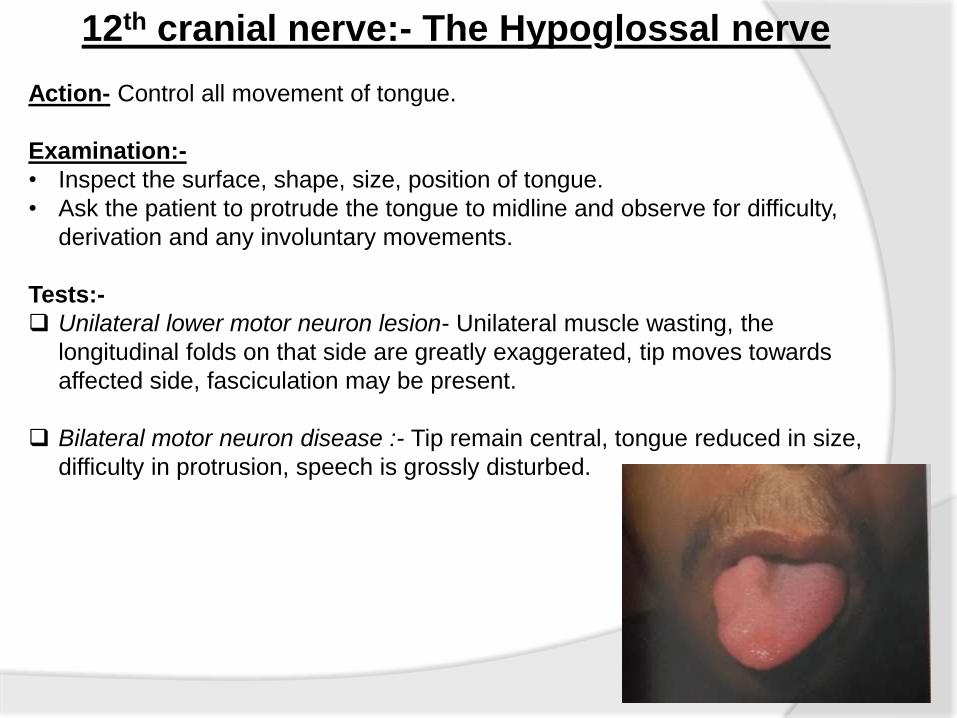
12th cranial nerve:- The Hypoglossal nerve
Action- Control all movement of tongue.
Examination:-
• Inspect the surface, shape, size, position of tongue.
• Ask the patient to protrude the tongue to midline and observe for difficulty,
derivation and any involuntary movements.
Tests:-
Unilateral lower motor neuron lesion- Unilateral muscle wasting, the
longitudinal folds on that side are greatly exaggerated, tip moves towards
affected side, fasciculation may be present.
Bilateral motor neuron disease :- Tip remain central, tongue reduced in size,
difficulty in protrusion, speech is grossly disturbed.
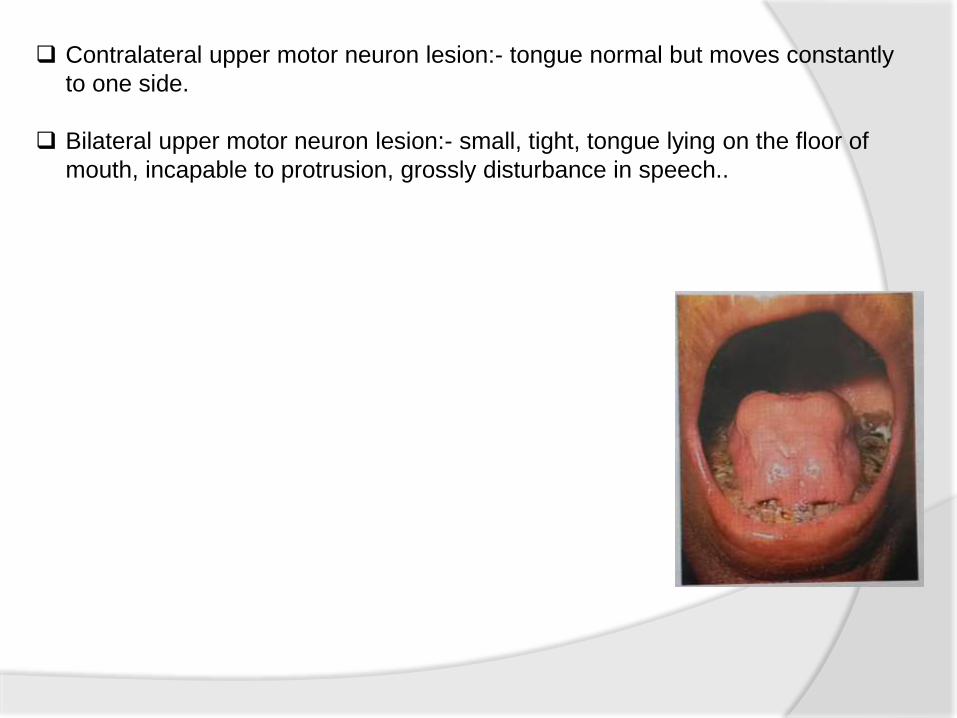
Contralateral upper motor neuron lesion:- tongue normal but moves constantly
to one side.
Bilateral upper motor neuron lesion:- small, tight, tongue lying on the floor of
mouth, incapable to protrusion, grossly disturbance in speech..
References
1. BICKERSTAFF ’s Neurological Examination by KAMESHWAR PRASAD
2. Neurological Assessment by RUBEN D. RESTREPO
3. Neurological Examination by WILLIAM HOWLETT
4. Neurological intervention for Physical Therapy by MARTIN KESSLER
5. A Concise Guide to Neurology by REMA PAI
6. Neurology Illustrated by KENNETH W LINDSAY, IAN BONE

Thank You !

![II./2.3. Examination of cranial nervesII./2.3.2. Examination of vision (Optic nerve [2nd cranial nerve]) Anatomy: The visual pathway originates from the ganglion cells of the retina,](https://img.pdfslide.us/doc/110x75/5f61f204b901471ec658d72f/ii23-examination-of-cranial-nerves-ii232-examination-of-vision-optic-nerve.jpg)