Embed Size (px)
Citation preview
The MOPACT Coordination Team The University of Sheffield
Department of Sociological Studies Northumberland Road
Sheffield, S10 2TU, UK T: +44 (0)114 222 6458 F: +44 (0)114 276 8125
www.mopact.group.shef.ac.uk
This project has received funding from the European Union’s Seventh Framework Programme for research, technological development and demonstration under grant agreement no 320333
Social Support and Long-term Care for Older People –Potentials for Social Innovation and Active Ageing
The CARER+ Final Conference Paris27 March 2015

www.mopact.group.shef.ac.uk
• Objectives of research• Background and definitions• The status of social support and long-term
care for older people in different ‘care regimes’• Potential and innovative practice• Future research
Contents
www.mopact.group.shef.ac.uk
• To analyse the status quo of active ageing strategies in long-term care
• To identify potentials for, drivers of and barriers to social innovation in long-term care– quantitative: financial incentives– qualitative: case studies of innovative practices
• To provide indicators for active ageing scenarios
Objectives
www.mopact.group.shef.ac.uk
Active Ageing as the process of optimising opportunities for health, participation and security in order to enhance quality of life as people age. It allows people to realise their potential for wellbeing throughout their lives and to participate in society according to their needs, desires and capabilities, while providing them with adequate protection, security and care when they need assistance” (WHO, 2002: 12).
Long-term care (LTC) as a system at the interface between health and social care, and between formal and informal care, is only just emerging as a specific area of social protection and support (Leichsenring et al., 2013).
Active Ageing and LTC – the often omitted part of ‘Active Ageing’
www.mopact.group.shef.ac.uk
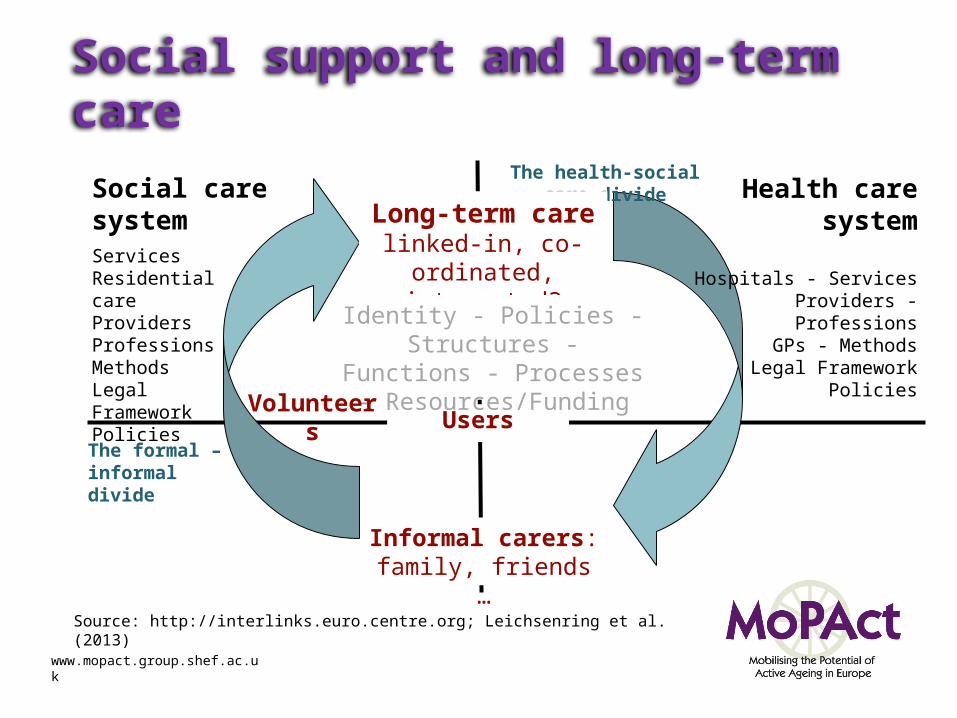
Informal carers:family, friends …
Social caresystemServicesResidential careProvidersProfessionsMethodsLegal FrameworkPolicies
The health-social care divide
Long-term carelinked-in, co-ordinated,
integrated?
Users
Identity - Policies - Structures - Functions - Processes -
Resources/FundingVolunteers
The formal – informal divide
Health caresystem
Hospitals - ServicesProviders - Professions
GPs - MethodsLegal Framework
Policies
Social support and long-term care
Source: http://interlinks.euro.centre.org; Leichsenring et al. (2013)
www.mopact.group.shef.ac.uk
Linking active ageing & long-term care
• A large number of older people are already very active in caring for a partner with LTC needs.
• Access to prevention, rehabilitation and other formal care services is unevenly distributed among European countries.
• Active ageing in the context of LTC is highly dependent on social investment strategies across a range of policy fields.

www.mopact.group.shef.ac.uk
‘Social Innovation’ in the context of long-term care• They are oriented towards exceptional societal challenges/social issues.• They suggest new solutions in the respective societal, cultural and economic context.• They create new patterns of social practices to overcome shortcomings of traditional
arrangements.• They tend to overcome the traditional dichotomy between technological and social
innovations.• They promote the integration and/or collaboration of heterogeneous stakeholders that
have hitherto not co-operated.• They include reflective and multidisciplinary approaches towards the key goal of societal
usefulness.• They create structures and processes that are sustainable and realise new growth
potentials in terms of regular employment.• It involves end-users as co-producers of services or products. (cf. Heinze and Naegele,
2012)

www.mopact.group.shef.ac.uk
Long-term carepolicies and practice in
national contexts
Social Innovation
new ideas,social ties and
collaborations
Active ageingrealising potential for well-being
Testing potential of active ageing strategies in social innovation
www.mopact.group.shef.ac.uk
A typology of European long-term care regimes • Governance• Needs and coverage• Agency
Preliminary clusters of care regimes:
• Care mix (Western): AT, DE, FR, UK• Universal (Nordic): DK, FI, SE, NL• Family-based (Mediterranean): EL, ES, IT, PT• Transition (Central and East Europe, New Member
States): BG, CZ, EE, HU, LT, LV, SK, RO
www.mopact.group.shef.ac.uk
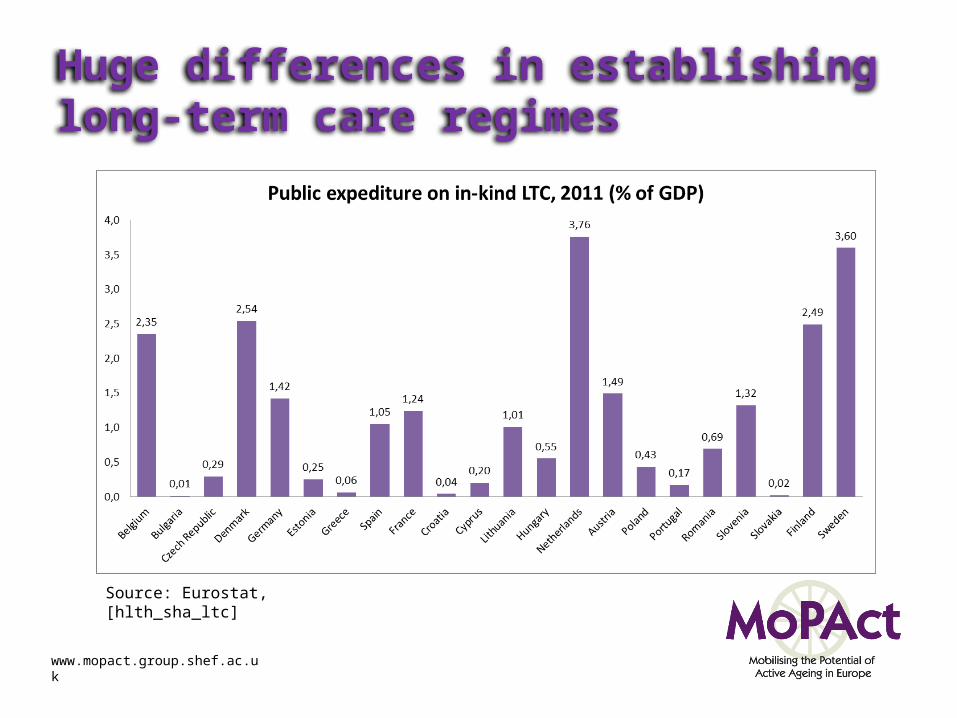
Huge differences in establishing long-term care regimes
Source: Eurostat, [hlth_sha_ltc]
www.mopact.group.shef.ac.uk
Potential and innovative practiceThe methodological process has three different steps:
1. Literature review and social innovation initiatives overview:
• A literature review was carried out in order to provide an overview of country-specific, regional and international sources contributing to the discourse on the key factors, drivers and barriers in social innovation in long-term care.
• 18 innovative initiatives representing 12 EU countries were analyzed individually to determine the drivers of and barriers to its development. In a later stage, in the course of a collaborative workshop in which the work package partners participated, these barriers and drivers were grouped into key themes/factors.
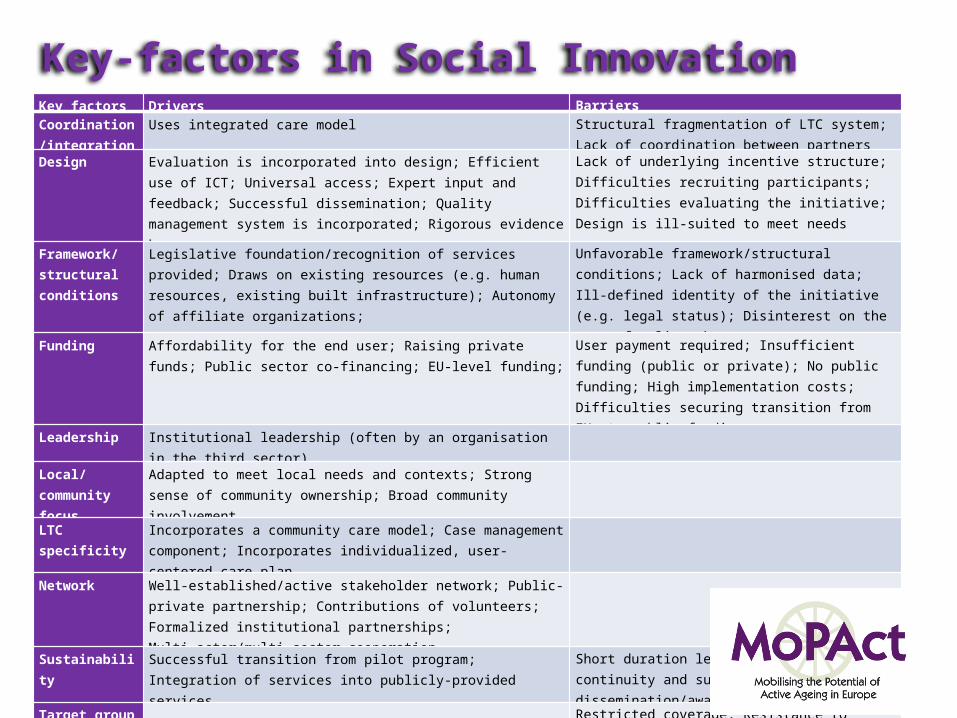
Key-factors in Social Innovation
www.mopact.group.shef.ac.uk
Key factors Drivers Barriers Coordination/integration
Uses integrated care model Structural fragmentation of LTC system; Lack of coordination between partners
Design Evaluation is incorporated into design; Efficient use of ICT; Universal access; Expert input and feedback; Successful dissemination; Quality management system is incorporated; Rigorous evidence base
Lack of underlying incentive structure; Difficulties recruiting participants; Difficulties evaluating the initiative; Design is ill-suited to meet needs
Framework/structural conditions
Legislative foundation/recognition of services provided; Draws on existing resources (e.g. human resources, existing built infrastructure); Autonomy of affiliate organizations;
Unfavorable framework/structural conditions; Lack of harmonised data; Ill-defined identity of the initiative (e.g. legal status); Disinterest on the part of policymakers
Funding Affordability for the end user; Raising private funds; Public sector co-financing; EU-level funding;
User payment required; Insufficient funding (public or private); No public funding; High implementation costs; Difficulties securing transition from EU- to public funding
Leadership Institutional leadership (often by an organisation in the third sector)
Local/community focus
Adapted to meet local needs and contexts; Strong sense of community ownership; Broad community involvement
LTC specificity Incorporates a community care model; Case management component; Incorporates individualized, user-centered care plan
Network Well-established/active stakeholder network; Public-private partnership; Contributions of volunteers; Formalized institutional partnerships; Multi-actor/multi-sector cooperation
Sustainability Successful transition from pilot program; Integration of services into publicly-provided services
Short duration leading to lack of continuity and sustainability; Lack of dissemination/awareness-raising
Target group Restricted coverage; Resistance to participation; Lack of computer literacy
User involvement User-led components; User input and feedback during development and implementation
Workforce Multi-disciplinary project team; Built-in element to ensure workforce sustainability
Unskilled/ill-supported informal care workforce; Insufficient (human) resources
Curent research
www.mopact.group.shef.ac.uk
2. Analysis of implementation at national level
• To verify whether and how the key factors typologies identified in the previous step are applied in each different care regime area.
• Consultation of experts and relevant stakeholders at national level (only in partner countries).
• This consultation is carried out by focus groups/expert interviews or via the contribution of the mushrooming ‘innovation hubs’, to check out whether LTC is on their radar and how they address it in terms of drivers and barriers.
3. Analysis of the implementation at a European level
• Same methodology as that applied for the national level.• Consultation with case experts and stakeholder representatives selected among
organisations and professionals operating at European level. • This consultation is carried out during the recurrent stakeholders forum (April
2015).
Building future scenarios
www.mopact.group.shef.ac.uk
Integration of qualitative and quantitative analyses into a limited number of highly innovative and realistically implementable scenarios of social support and long-term care in EU Member states.
Targets:
• The reduction of poverty risks and social exclusion caused by long-term care needs in older family members
• The quantitative increase of employed and unpaid carers of older people• The improvement of health and quality of life of older people in need of care
and their caregivers• The quality and integration of social, health and long-term care services,
including a more user-centred implementation of new technologies.

Thank you for your attention!
www.mopact.group.shef.ac.uk
www.mopact.group.shef.ac.uk





























