Embed Size (px)
Citation preview
OBSTRUCTION OF URINARY TRACT
Soumya Ranjan ParidaBasic B.Sc. Nursing 4th year
Sum Nursing College
Obstruction of urinary tractEtiology – Renal dysplasia, infectionClinical features – FTT, vomiting, diarrhea Acute ureteral obstruction – abdominal pain, nausea, vomiting, Chronic ureteral obstruction – vague abdominal pain, increased fluid intakeDiagnosis – Neaonatal – palpable abdominal mass Infravasical – bladder palpable , patent urachus, urinary ascitis Antenatal USG – hydronephrosis, infection, sepsis Imaging studies – USG – hydronephrosis VCUGMercapto acetyl triglycine (MAG-3) – • Recheases renal parenchyma in 2-3 minutes • lasix after 20-30 min 10-15 min – ½ radionuclide 20 min delayed 15-20 min intermittent Limitation – Newborn kidney, dehydration
Urinary tract obstruction
IVP – infravasical obstruction, ureteral obstructionWhitaker test – 10 ml/min fluid infusion – pressure difference of more than 20 cm
H2O b/w renal pelvis and bladderHydrocalycosis – • localized dilatation of calyx caused by obstruction of infundibulumUPJ obstruction – • 60% left side• M:F - 2:1• 10% bilateral• Intrinsic obstruction • Extrinsic obstruction by artery• Type 3,4 hydronephrosis without dilatated ureterClinical features – • Fetal hydronephrosis• Palpable renal mass in newborn• Abdominal, flank, back pain in older children• Febrile UTI • Hematuria without minimal UTI
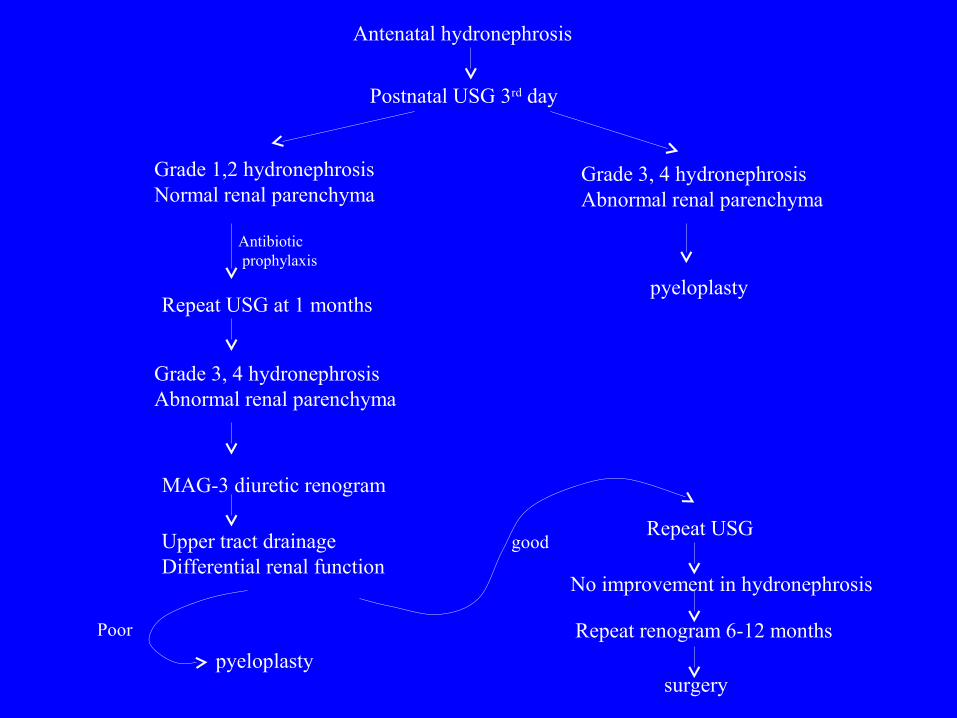
Antenatal hydronephrosis
Postnatal USG 3rd day
Grade 1,2 hydronephrosisNormal renal parenchyma
Antibiotic prophylaxis
Repeat USG at 1 months
Grade 3, 4 hydronephrosisAbnormal renal parenchyma
MAG-3 diuretic renogram
Upper tract drainageDifferential renal function
Poor
pyeloplasty
goodRepeat USG
No improvement in hydronephrosis
Repeat renogram 6-12 months
surgery
Grade 3, 4 hydronephrosisAbnormal renal parenchyma
pyeloplasty
Midureteral obstruction –
• Retrocaval ureter – Upper right ureter travels posterior to IVC
• IVP shows – right ureter deviated medially at the level of L3
• Surgical repair – only when obstruction is present.
• Acquired obstruction – retroperitonial tumors, fibrosis, inflammatory process, radiation therapy.
Ectopic ureter –
• Ureters that drain out side the bladder
• M:F 1:3
Females –
• Bladder neck – 35%
• Urethrovaginal septum – 35%
• Vagina – 25%
• Cervix , uterus, gartner duct, urethral diverticulum
• Manifests as UTI and continuous urinary incontinence
Urinary tract obstruction
Boys – • Posterior urethra – 47%• Seminal vesicval – 33%• Prostatic utrical – 10%• Ejaculatory duct – 5%• Vas deference – 55• Manifests as UTI and epididymitis• No continuous urinary incontinence.Ureterocele – • M : F 1:2• Ectopic – cystic swelling extends through bladder neck into the urethra• Orthotopic – ureterocele entirely within the bladder• Manifest as bladder neck obstruction, b/l hydronephrosis, ureterocele prolapse
through urethra• VCUG shows filling defect in bladder often shows reflux• ‘Drooping lily’ appearance of the kidney
Urinary tract obstruction
Treatment – • No function in upper pole, no reflux – excision of upper pole and
associated ureter• Function in upper pole, significant reflux, septic – transurethral
incision with catery to decompress the ureterocele
Orthotopic ureterocele – • Discovered during screening for antenatal hydronephrosis or UTI• USG – Sensitive• IVP – varying degrees of ureteral and calyceal dilation, and there is a
round filling defect in bladder• Treatment – transurethral incision
Urinary tract obstruction
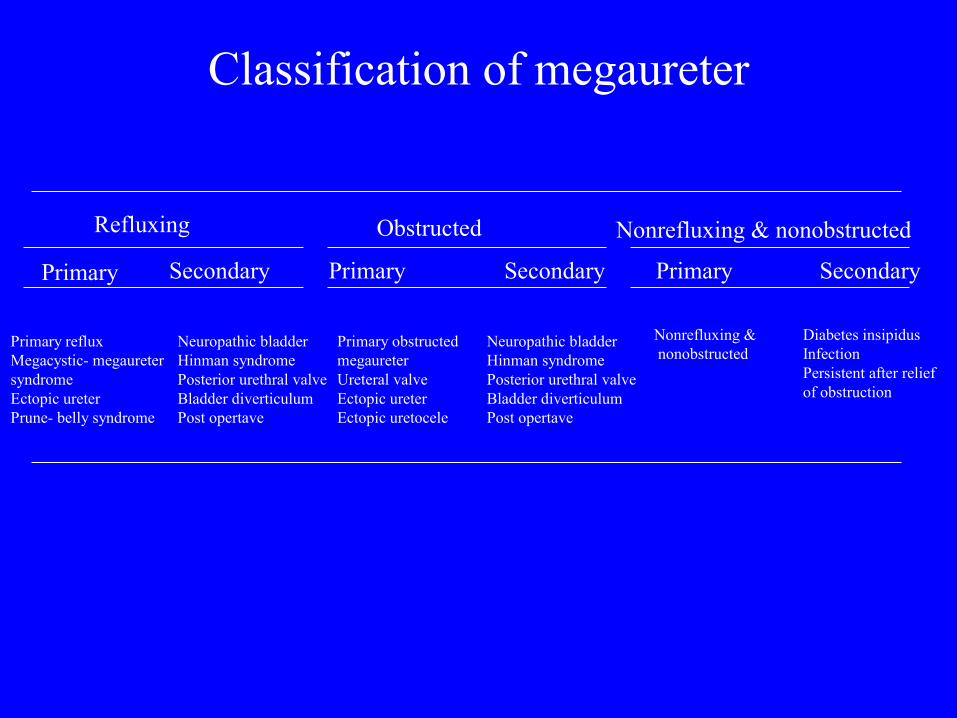
Classification of megaureter
Refluxing Obstructed Nonrefluxing & nonobstructed
Primary Secondary Secondary SecondaryPrimary Primary
Primary refluxMegacystic- megauretersyndromeEctopic ureterPrune- belly syndrome
Neuropathic bladderHinman syndromePosterior urethral valveBladder diverticulumPost opertave
Primary obstructed megaureterUreteral valveEctopic ureterEctopic uretocele
Neuropathic bladderHinman syndromePosterior urethral valveBladder diverticulumPost opertave
Nonrefluxing & nonobstructed
Diabetes insipidusInfectionPersistent after relief of obstruction
Megaureter –
• The primary obstructed nonrefluxing megaureter results from abnormal development of the distal ureter, with collagenous tissue replacing the muscle layer
• There is a disruption of the normal ureteric peristalsis, and proximal ureter widens
• IVP – Distal ureter dilated and tapers abruptly at or above the junction of the bladder
Clinical manifestation –
• UTI, urinary stones, flank pain
Treatment –
• Nonobstructed megaureters diminish in size over time
• Obstructed megaureters – excision of narrowed segment, ureteral tapering, reimplantation of ureter
Urinary tract obstruction
Prune-Belly syndrome (Eagle- Barret syndrome) –
• Incidence – 1:49000
• M: F – 9.5:1
• Defficient abdominal muscles, undescended testes, urinary tract abnormality
• Pulmonary hypoplasia
• Oligohydromnios
• Malrotation of bowel
• Cardiac anomaly
• Abnormalities of musculoskeletal system
• Anomalies of the urethra, uterus and vagina
Treatment –
• No obstruction – Antibiotic prophylaxis
• Obstruction – Vesicostomy
Urinary tract obstruction
Posterior urethral valves – • Incidence – 1:8000 boys• Tissue leaflets fanning distally from the prostatic urethra to the external
urinary sphinctor• Dilatation of prostatic urethra, bladder muscles under go hypertrophy• VUR (50%), distal ureteral obstruction• Mild hydronephrosis to renal dysplasia• Oligohydromnios, pulmonary hypoplasia• Antenatally – b/l hydronephrosis, distended bladder, oligohydromnios• Postnatally – distended urinary bladder, weak urinary stream, FTT, sepsisTreatment – • NG tube is inserted in bladder and left for several days• Sreum creatinine normal – Tranurethral ablation of valve leaflets/vesicostomy• Sreum creatinine high – vesicostomy• Uremia without infection – medical management• Uremia with infection – life saving measures, antibiotics, percutaneous
nephrostome, and hemodialysis
Urinary tract obstruction
Urethral atresia –
• Distended bladder, b/l hydronephrosis, oligohydromnios
• Infants are still birth
• Patent urachus – oligohydromnios unlikely
Treatment –
• Continent urinary diversion
Urethral hypoplasia –
• Urethral lumen is very small
• B/L hydronephrosis , distended bladder
• Passage of NG tube is diffucult
Treatment –
• Urethral reconstruction,
• Gradual urethral dilation,
• Continent urinary diversion
Urinary tract obstruction
Urethral strictures –
Males –
• Urethral trauma either accidental or iatrogenic
• Decrease in urinary stream is seldom noted
• Bladder instability, hematuria, dysuria
• Catheterization imposible
Treatment -
• Endoscopic dilation of stricture
Females –
• True urethral stricture is rare b/c urethra is protected from trauma
• ‘Spinning top’ deformity on VCUG
Urinary tract obstruction
Anterior urethral valves –
• It is rare
• No obstructive valve leaflets
• It is a urethral diverticulum in penile urethra that expands during voiding
• Soft mass on the ventral surface of the penis at the penoscrotal junction
• Weak urinary stream
Treatment –
• Open excision of diverticulum
• Trans urethral excision of the distal urethral cusp
Urinary tract obstruction
Urolithiasis
Composition –
Calcium, oxalate, uric acid, cysteine, ammonium, phosphate
crystals or combination of these substances.
Classification –
• Ca oxalate and Ca phosphate• Cystine stones• Struvite stone• Uric acid stone• Indinavir stones• Nephrocalcinosis
Stone formation – • Matrix – Mixtures of proteins, non amino sugars, glucosamines, water, organic ash. 2-9 % of dry weight• Precipitation-crystallization – Supersaturation of the urine with specific ions comprising of crystals.• Epitaxy – Aggregation of crystals of different composition but similar lattice structer• Inhibitors – Citrate, diphosphonate, Mg++Clinical manifestation – • Renal pelvis and calyx – gross or microscopic hematuria, abdominal or flank pain.• Distal ureter – Dysuria, urgency, frequency.• Bladder – Asymptomatic• Urethra – Dysuria, difficult voiding
Urolithiasis
Diagnosis –
KUB x-ray – all are radiopaque except cystine and uric acid
USG abdomen – limitation ureteric calculi
Nonenhanced spiral CT
Metabolic evaluation –
• Serum –
Calcium, phosphorus, uric acid, electrolytes
and anion gap, creatinine, alkaline phosphatase
• Urine –
Urinolysis, urine culture,
Ca:Cr ratio,
Spot test for cystinuria
24 hr urine for – Ca, PO4, oxalate, uric acid,
Diabasic amino acids (COAL)
Urolithiasis
Ca oxalate and Ca phosphate – • Hypercalciuria without hypercalcemia – Absorption , renal, resorption• Hyperoxaluria – Primary - Increased production Glycolic aciduria, L-glyceric acidosis Secondary – Increased intake Pyridoxine deficiency, intestinal malabsorption Enteric hyperoxaluria - IBD, pancreatic insufficiency, biliary disease• Hyperuicosuria• Hypocitruria – Chronic diarrhea, malabsorption, RTA• Cystinuria• Hypomagnesuria• Hyperparathyroidism• RTA type 1
Urolithiasis
• Cystine stones –
Defective renal tubular absorption – cystinuria – low
osmolality, acidic urine – stone formation
• Struvite calculi –
Magnesium ammonium phosphate, staghorn configuration
UTI by urea splitting organism – urinary alkalinization – excess
NH3 production – precipitation of MAP and CaPO4 – stone
formation
• Uric acid calculi –
Hyperuricosuria with or without hyperuricemia
Acidic urine and urate crystalluria
Lesh Nyhan syndrome, G6PD, short bowel syndrome, chronic
diarrhea, acidosis, tumor, myeloproliferative disorders
Urolithiasis
• Indinavir calculi – Radiolucent Soluble at Ph < 5.5 Urinary acidification by NH4Cl and ascorbic acid• Nephrocalcinosis – Deposition of calcium in renal parenchymaTreatment – • Removal depends upon location, size, composition, obstruction, infection• Maintain high urine output• ESWL of bladder, ureter, small renal pelvisCalcium stones –• Decrease Ca and Na in diet.• Thiazide diuretics• Potassium citrate – 1-2 meq/kg/day• Lemon juice – 120 ml ( 84 meq citric acid )
Urolithiasis
Uric acid stone –
• Allopurinol
• Alkalinization of urine – Ph > 6.5
• NaHCO3 and Na citrate
Cystine stone –
• Alkalinization of urine – Ph > 6.5
• D-Penicillamine
• N-Acetyl cystein
Primary hyperoxaluria –
• Hepatic transplant
Urolithiasis
THANKS





![Case Report Bilateral Obstructive Uropathy Secondary to ...syndrome [ ], subacute intestinal obstruction [ , ], recur-rent acute urinary retention [ ], or exceptionally bilateral hydronephrosis](https://img.pdfslide.us/doc/110x75/60f789064e4fc37e631734b3/case-report-bilateral-obstructive-uropathy-secondary-to-syndrome-subacute.jpg)