Embed Size (px)
Citation preview

Stroke, or cerebrovascular accident (CVA), refers to a number of different circula-tory brain disorders that temporarily or permanently impair brain function. It is the second most common cause of death worldwide and a major cause of disability in the western industrialised world1. Nonetheless, the prognosis for a substantial proportion of applicants who have suffered some type of stroke is good. The key to identifying these “good” risks is to determine precisely what type of stroke the applicant has experienced. To achieve this, MIRA’s new stroke distribution page now groups strokes into subtypes with distinctly different aetiologies and long-term outcomes (see Figure 1). In addition, associated risk factors (e.g. arterial hypertension and severe neurological deficits following stroke) that lead to sub-stantially increased mortality with all stroke types must be taken into account.
Understanding the condition
About 80% of all strokes in western societies are caused by focal cerebral ischae-mia due to arterial occlusion.2 Ischaemic cerebrovascular disease can be divided into two main groups: transient ischaemic attacks (TIA) and cerebral infarction.
Depending on the rate of residual blood flow and the duration of ischaemia, the damage can be transient (TIA) – i.e. reversible – or it can result in an infarc-tion (ischaemic stroke). The definition of TIA has been recently modified, as many TIAs causing symptoms for less than 24 hours can be linked to evidence of brain infarction using today’s superior neuroimaging technologies. From an underwriting point of view, it is more important to differentiate between TIA/minor strokes and more severe strokes, because stroke severity with subsequent need for support in daily activities is one of the strongest predictive factors in long-term prognosis (see Figure 2).3
Neuroimaging allows reliable differentiation between TIA and cerebral infarction
Stroke severity is one of the strongest predictive factors in long-term prognosis
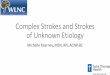
Figure 1: Stroke subtypes
Different stroke subtypes aetiologically classified
Source: Munich Re
TIAMinor stroke
Ischaemic stroke
Spontaneous intra -cerebral haemorrhage
Secondary intra- cerebral haemorrhage
Aneurysmal sub-arachnoid haemorrhage
Nonaneurysmal sub-arachnoid haemorrhage
Stroke
Ischaemic
Haemorrhagic
Intracerebral
Subarachnoidhaemorrhage
One stroke is not necessarily the same as another. The disorder includes many subtypes and even more causes. In recent decades, medical and technological improvements have led to new treatment options for different stroke sub types. As a result, the prognoses of applicants who have suffered strokes can vary widely.
MIRA RISK REVIEW
Stroke Better differentiation, better business

Munich ReMIRA RISK REVIEWStroke
Page 2/4
The main causes of death are the initial stroke event, a recurrence of stroke or a following cardiovascular event, as is the case in all stroke types. The risks are especially high within the first year after the initial event.4, 5 This underscores the importance of rating for additional cardiovascular risk factors (particularly arterial hypertension) and adhering to the recommended postponement period. Although the absolute survival probability in younger stroke patients with cardio-vascular risk factors is higher than in older patient groups, the extramortality rate in younger stroke patients is higher due to the very low mortality rate of this age group in the general population.6, 7
Since studies indicate lower long-term mortality after ischaemic infarction in association with migraines than in general stroke population, we place mortal-ity risk for this condition on the same level as for TIA/minor stroke.8
Clinical trials with today’s standard low-dose estradiol oral contraceptive for-mulations have not confirmed an association between ischaemic stroke and oral contraceptive use.9 For this reason the rating category “oral contraceptive use” was abandoned.
Nontraumatic intracerebral haemorrhage (ICH) is the second most common cause of stroke, following ischaemic stroke, comprising up to 15% of all strokes. Bleeding into the brain tissue, which may extend into the ventricles, is the hallmark of ICH. Mortality and morbidity are highest of all stroke subtypes.11 Spontaneous ICH is divided into primary ICH due to chronic hypertension or amyloid angiopathy (80%) and secondary ICH due to structural causes (20%) such as intracranial arteriovenous malformations, cavernous angioma or tumours.
Study results regarding the long-term life expectancy of patients with ICH relative to that of general population are inconsistent, yet agreement exists that reduction in survival time is mostly driven by short-term mortality (see Figure 3).12, 13 Patients who survive the acute period follow a different prog-nosis, depending on the severity of disability after stroke.14 Severely disabled applicants have a significantly higher mortality rate than those who have ex- perienced a good recovery.
Overall extramortality is higher in younger stroke patients than in older individuals
Spontaneous ICH has a poor short- and long-term outcome
Mortality is highest within the year after the occurrence of an ICH
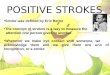
Figure 2: Influence of stroke severity on survival
0 1 2 3 4 5 6 7 8
100
80
60
40
20
0
Independent Dependent
The chart shows the long-term survival of patients who were dependent (needing help in everyday activities) at six months after suffering a stroke compared to those who were independent after the same period.
Source: Bruins Slot K. et al., 2008, see footnote 10
Percentage of patients alive after stroke
Years since stroke

Munich ReMIRA RISK REVIEWStroke
Page 3/4
In young adults, hypertension is responsible for a low number of spontaneous ICH. However, the cardiovascular mortality and morbidity risk in this age group is especially high. Compared with other causes, this produced the most negative outcome.16
Common causes of secondary ICH are arteriovenous malformations and cerebral cavernomas (also termed cavernous angioma), but there are other infrequent aetiologies. In general, the outcome after surgically treated arterio-venous malformations ICH is better than after primary spontaneous ICH.17 Definitive surgical care is thus essential.18 Operated cerebral cavernomas have excellent prognoses, subject to event-free peri- and post-operative course.19
Subarachnoid haemorrhage accounts for 2% to 5% of all new strokes. It is characterised by the extravasation of blood into the spaces between the brain and the surrounding membrane. The leading cause of non-traumatic subarach-noid haemorrhage is rupture of an intracranial aneurysm, which accounts for about 80% of cases. Subarachnoid haemorrhage not caused by an aneurysm is called nonaneurysmal subarachnoid haemorrhage (NASAH).
Survivors of aneurysmal subarachnoid haemorrhage (SAH), which was pre-viously thought to be a once-in-a-lifetime event, have an increased risk of developing new intracranial aneurysms and new episodes of SAH resulting in increased mortality compared to that of the general population. Mortality after rebleeding is estimated to be as high as 70%. Aneurysm repair is the only effective treatment to prevent this occurrence. Case fatality rates have shown declining trends over the last three decades20, but the outcome has improved only among those patients who survive the initial bleeding and are eligible for interventions.21 Most deaths occur in the initial period, with subsequent mortal-ity risk relatively stable over the next ten years.22 The observed reduced life expectancy is not only caused by the initial or recurrent SAH but also by higher risk of cardiovascular diseases. This increased risk of vascular diseases applies not only to older but also to younger patients.23
In general, NASAH has a more benign prognosis than untreated aneurysmal subarachnoid haemorrhage, but life expectancy differs due to the different possible causes.24
Extramortality is stable over course of ten years after SAH
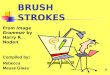
Population Study group
Reduction in survival time in ICH patients compared to general population was mostly driven by acute in-hospital mortality.
Source: Munich Re own calculations, based on McGuire A.J. et al., 2007, see footnote 15
Figure 3: Median survival time in ICH patients
Young adults with primary ICH have the worst prognosis
0 1 2 3 4 5 6 7 8 9 10
100
80
60
40
20
0
Percentage of patients alive after stroke
Secondary ICH is a rare event
Years since stroke

© 2011Münchener Rückversicherungs-GesellschaftKöniginstrasse 107, 80802 München, Germany
Order number 302-07066
Munich ReMIRA RISK REVIEWStroke
Page 4/4
Benefits
A close look at stroke reveals that it should not be regarded as a single impair-ment, but rather a group of disorders with a number of subgroups. The new MIRA guidelines allow you to assess with significantly improved accuracy the quality of risk for applicants who have suffered a stroke.
Literature
1 WHO. The top 10 causes of death. Fact sheet No 310, Updated June 2011 (http://www.who.int/mediacentre/factsheets/fs310/en/index.html)
2 Feigin V.L. et al. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. The Lancet Neurology, 2009; 8 (4): 355–369
3, 10 Bruins Slot K. et al. Impact of functional status at six months on long term survival in patients
with ischaemic stroke: prospective cohort stud-ies. BMJ, 2008; 336 (7640): 376
4 Van Vijk I. et al. Long-term survival and vascular event risk after transient ischaemic attack or minor ischaemic stroke: a cohort study. The Lancet, 2005; 365: 2098–104
5 Greisenegger S. et al. Clinical predictors of death in young and middle-aged patients with ischemic stroke or transient ischemic attack: long-term results of the Vienna Stroke Registry: Clinical predictors of ischemic stroke mortality in patients <60 years. J Neurol, 2011; 258 (6): 1105–13
6 Marini C. et al. Long-Term Prognosis of Cerebral Ischemia in Young Adults. Stroke, 1999; 30: 2320–2325
7 Putaala J. et al. Causes of Death and Predictors of 5-Year-Mortality in Young Adults After First Ever Ischemic Stroke: The Helsinki Young Stroke Registry. Stroke, 2009; 40: 2698–2703
8 Varona J.F. Long-term prognosis of ischemic stroke in young adults. Stroke Res Treat, 2010
9 Siritho S. et al. Risk of ischemic stroke among users of the oral contraceptive pill: The Melbourne Risk Factor Study (MERFS) Group. Stroke, 2003; 34 (7): 1575–80
11 Hankey G.J. et al. Five-Year Survival After First-Ever Stroke and Related Prognostic Factors in the Perth Community. Stroke, 2000; 31: 2080–2086
12 Andersen K.K. et al. Hemorrhagic and Ischemic Strokes Compared: Stroke Severity, Mortality, and Risk Factors. Stroke, 2009; 40: 2068–2072
13, 15 McGuire A. J. et al. Long-Term Mortality, Morbidity and Hospital Care following Intra-
cerebral Haemorrhage: An 11-Year Cohort Study. Cerebrovasc Dis, 2007; 23: 221–228
14 Saloheimo P. et al. The Impact of Functional Sta-tus at Three Months on Long-Term Survival After Spontaneous Intracerebral Hemorrhage. Stroke, 2006; 37: 487–491
16 Ruiz-Sandoval J. et al. Hypertensive Intracerebral Hemorrhage in Young People. Stroke, 2006; 37: 2946–2950
17 Van Beijnum J. et al. Outcome after spontaneous and arteriovenous malformation-related intra-cerebral haemorrhage: population-based studies. Brain, 2009; 132: 537–543
18 ApSimon HT et al. A population-based study of brain arteriovenous malformation: long-term treatment outcomes. Stroke, 2002; 33 (12): 2794–800
19 Bertalanffy H. et al. Cerebral cavernomas in the adult. Review of the literature and analysis of 72 surgically treated patients. Neurosurg Rev, 2002; 25 (1–2): 1–53
20 Lovelock CE et al. Time trends in outcome of subarachnoid haemorrhage: Population-based study and systematic review. Neurology, 2010; 74 (19): 1494–501
21, 23 Ronkainen A. et al. Evidence for Excess Long- Term Mortality After Treated Subarachnoid
Haemorrhage. Stroke, 2001; 32: 2850–285322 Nieuwkamp D.J. et al. Excess Mortality and Car-
diovascular Events in Patients Surviving Sub-arachnoid Haemorrhage: A Nationwide Study in Sweden. Stroke, 2011; 42: 902–907
24 Greebe P. et al. Life Expectancy After Perimesen-cephalic Subarachnoid Hemorrhage. Stroke, 2007; 38: 1222–1224
Dr. Alban Senn Medical Consultant Centre of Competence for MIRA and Expert Underwriting Rules Tel.: +49 89 38 91-93 27Fax: +49 89 38 91-7 93 [email protected]
Contact
Not if, but how
Evidence-based underwriting
MIRA is dedicated to efficient, evidence-based risk assessment in a changing world. For this reason, Munich Re continuously revises and updates the online tool to reflect the latest scientific findings and risk trends. MIRA thus provides maximum legal security regarding underwriting decisions. At the same time, it serves as a solid basis for writing new business and optimising risk management. The MIRA Risk Review series gives clients a clear overview of each revision and its scientific background.