Embed Size (px)
Citation preview
Managing Symptoms in EOL
Residential Network Meeting November 2016
Eimear McCormack
Clinical Nurse Specialist Palliative Care
BsC Nursing Studies
GradDip Palliative Nursing
MsC End of Life Health Care Ethics
Outline
• Defining end of life
• What is a Good death
• Trajectories of Dying
• Recognising dying
• Communicating diagnosis of dying
• Truth telling and collusion
Challenges in caring at the very end of life
• When does EOL care begin
• How do we know when someone is dying?
• How can we manage this (as a team)
Resources to plan ahead
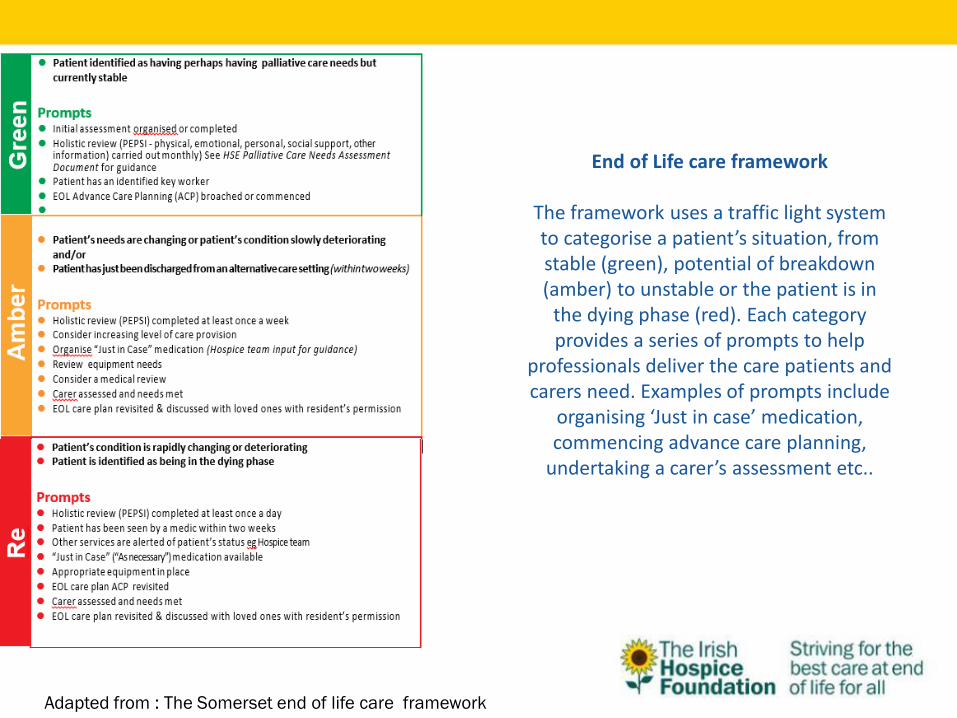
Adapted from : The Somerset end of life care framework
End of Life care framework
The framework uses a traffic light system to categorise a patient’s situation, from stable (green), potential of breakdown (amber) to unstable or the patient is in
the dying phase (red). Each category provides a series of prompts to help
professionals deliver the care patients and carers need. Examples of prompts include
organising ‘Just in case’ medication, commencing advance care planning,
undertaking a carer’s assessment etc..
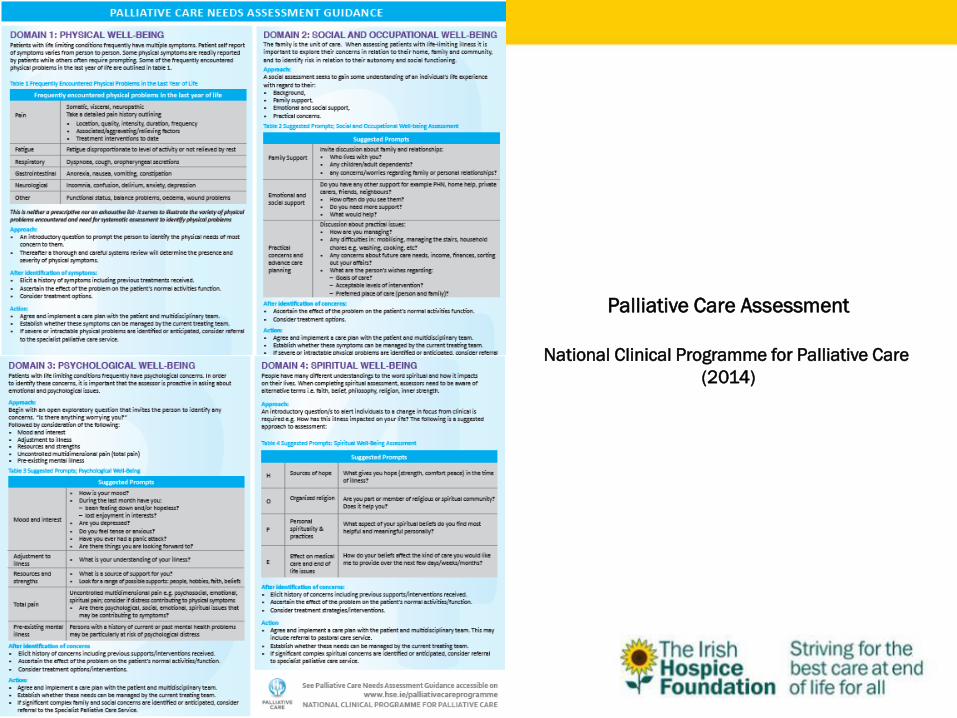
Palliative Care Assessment
National Clinical Programme for Palliative Care
(2014)
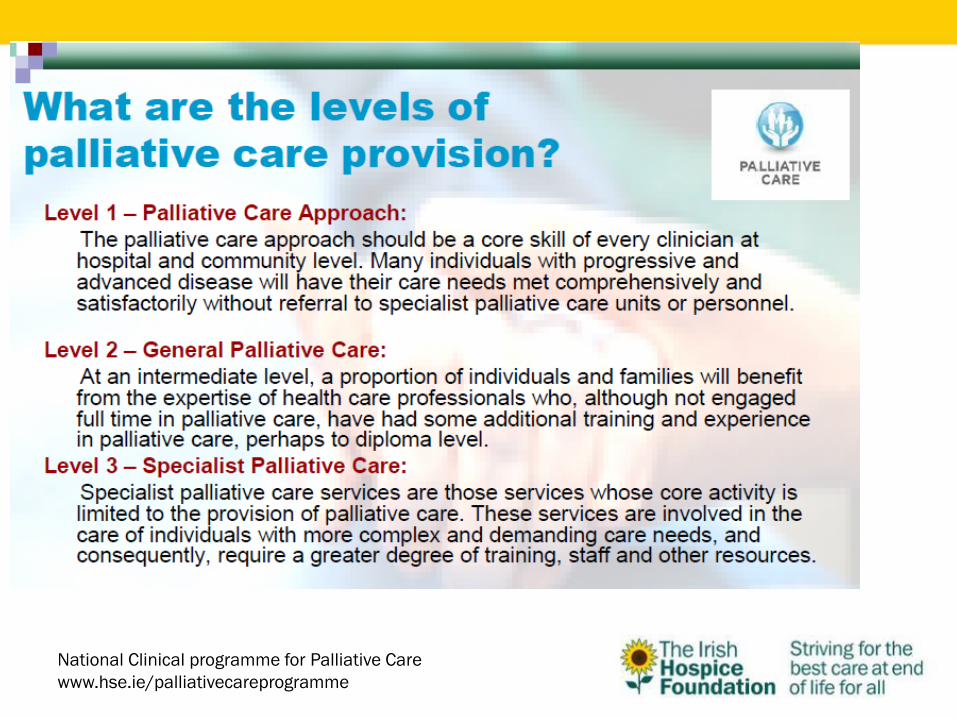
National Clinical programme for Palliative Care
www.hse.ie/palliativecareprogramme
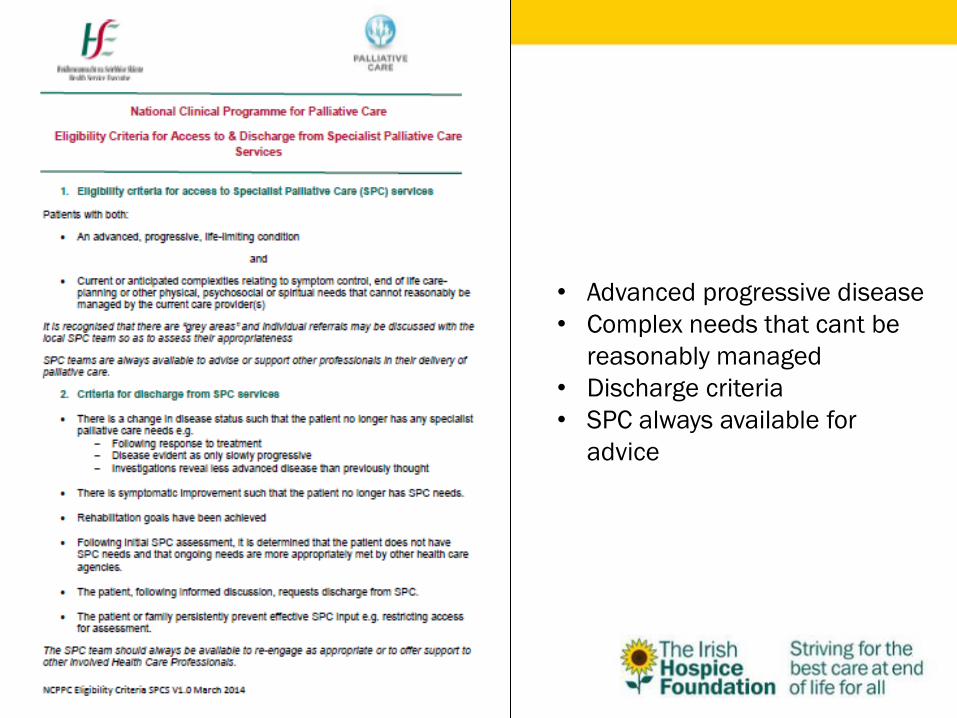
• Advanced progressive disease
• Complex needs that cant be
reasonably managed
• Discharge criteria
• SPC always available for
advice
When does EOLC begin
Good end of life care is not just about death and dying but quality of life until the end
EOL Care Plans
• Assessing current needs
• Promoting & preserving choice & autonomy
• Predicting likely problems
• Planning for the future
EOLC is about quality of life as well as quality of dying…
Planning for EOL- The Traffic light approach
“In a care home setting all residents are assessed using an
traffic light coding system based on an expectation of
prognosis”
• (blue)=years+
• (green)=months
• (yellow)=weeks
• (red)=days
Gold Standards Framework, UK
NHS End of Life Strategy
NICE
“We cannot take away the whole hard thing that is happening, but we can help to bring the burden into manageable proportions”
Dame Cecily Saunders,1963
spiritual
Psycho-social
physical
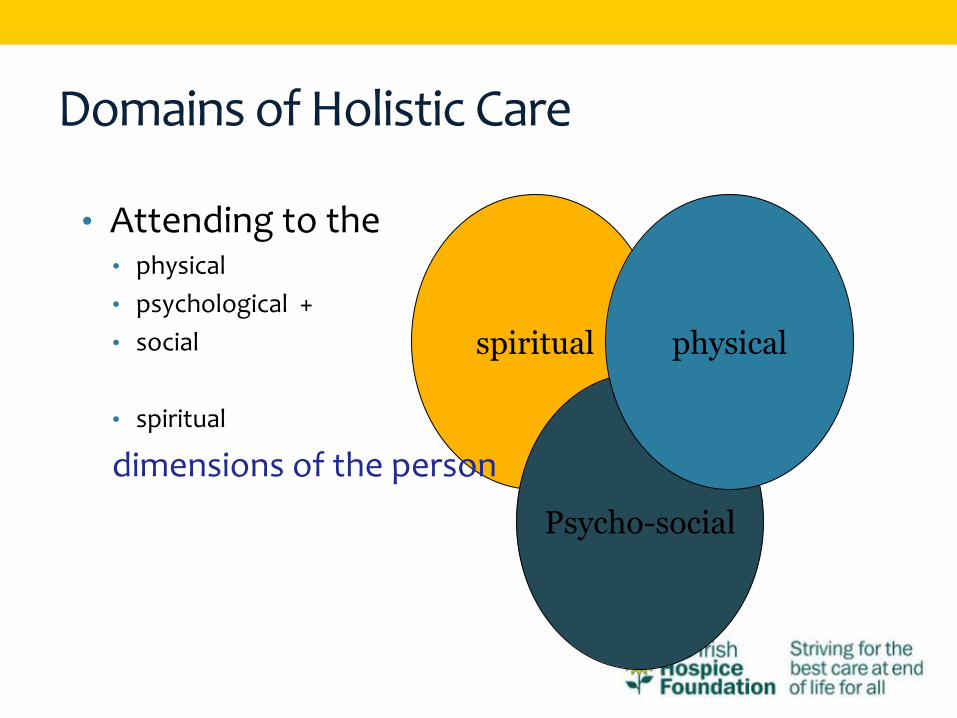
Domains of Holistic Care
• Attending to the • physical
• psychological +
• social
• spiritual
dimensions of the person
What is a good death? Definitions of a good death differ between health
professionals, patients, and even between patients and families. How death is experienced can be based on past/present experiences and emotions.
Important not to impose on patients and families our values regarding a good death
Good death generally regarded as • Pain and symptom free
• Involved in decision making
• Completed any unfinished business
• Privacy
• Loved ones present
• Open communication
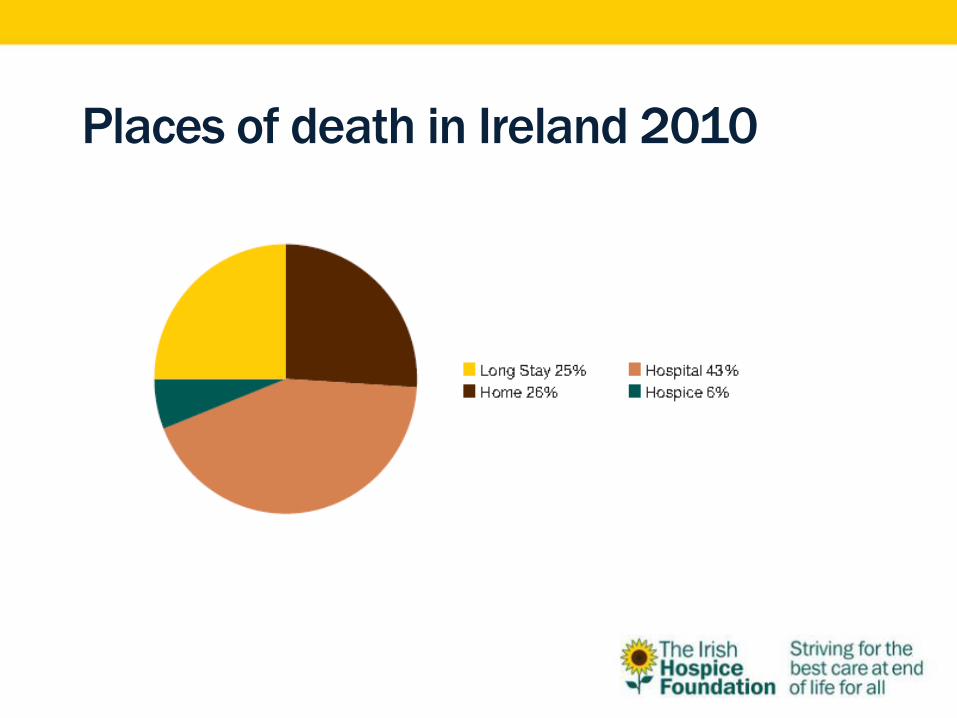
Places of death in Ireland 2010
• Always complex
• Culture often focuses on “cure”
• Often there is a reluctance to diagnose dying due to the uncertainty of the dying process.
• Cancer patients have a predictable disease trajectory but in non-cancer patients dying is more difficult to predict
Recognising ‘dying’
• There are misperceptions about the point at which a person
becomes a ‘dying person’, at which treatment might end and care become palliative and about the level of certainty surrounding such judgements.
• It is not always possible or helpful to people who may be dying and their families to seek to make a definitive diagnosis of ‘dying’.
• Care for people who are potentially in the last few days and hours should be a continuum, focusing on continually assessing their condition, needs and wishes and responding appropriately.
• However, professionals must make clear to the dying person and those who are important to them when it is thought that the person is likely to be dying and they should explain to them why they think this, what it is likely to entail and the uncertainties round this. Where a person’s condition changes, this should be a ‘trigger’ for making decisions to change care and treatment .
• Focus on recognition of patients who are clinically unstable and may not recover despite medical treatment, so that those patients and those important to them are as involved as much as possible in decisions being made about their care, rather than focusing on a ‘diagnosis of dying’.
• Focusing on changes in the condition of someone who is likely to be dying, rather than diagnosing dying only.
• If someone is likely to be dying, this is clearly explained to the dying person (if conscious) and those important to them.
• There are various prognostic tools that may help clinicians assess whether someone is in the last few days and hours of life, but at the moment, there is insufficient evidence base for any specific tool to be endorsed.
Trajectory of Dying Sudden Death
•No plan of care
•No preparation for grief
•Complex issues for relatives and staff
Anticipated death
•Integrated plan of care is possible
•Difficult to predict exact time
•Important time for patient family and carer.
Series of lapses and recoveries
•Highly emotive for the family
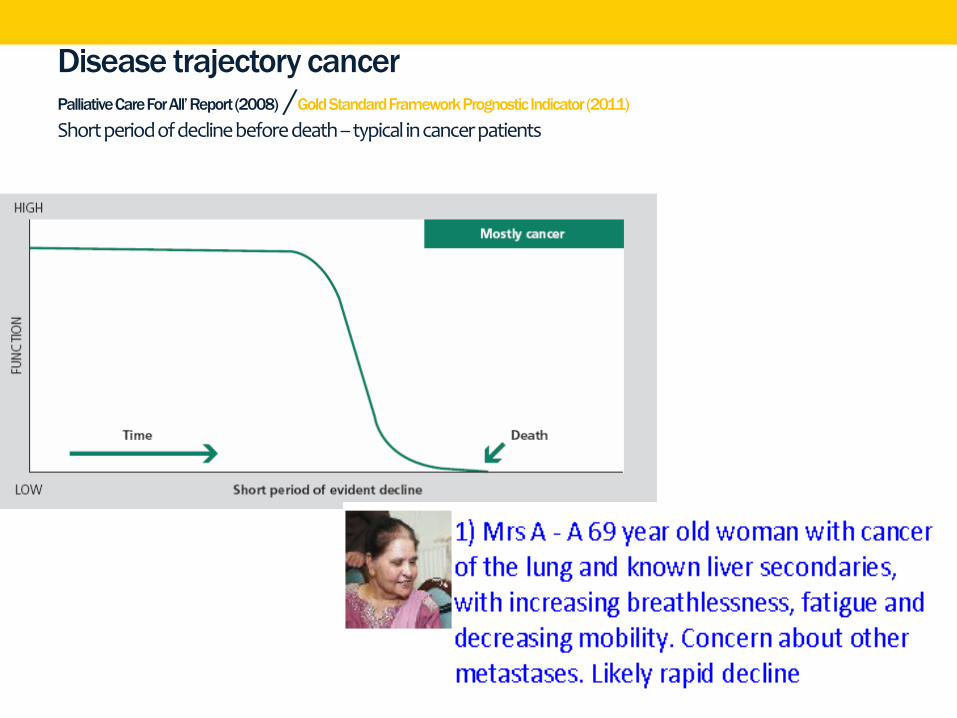
Disease trajectory cancer Palliative Care For All’ Report (2008) /Gold Standard Framework Prognostic Indicator (2011)
Short period of decline before death – typical in cancer patients
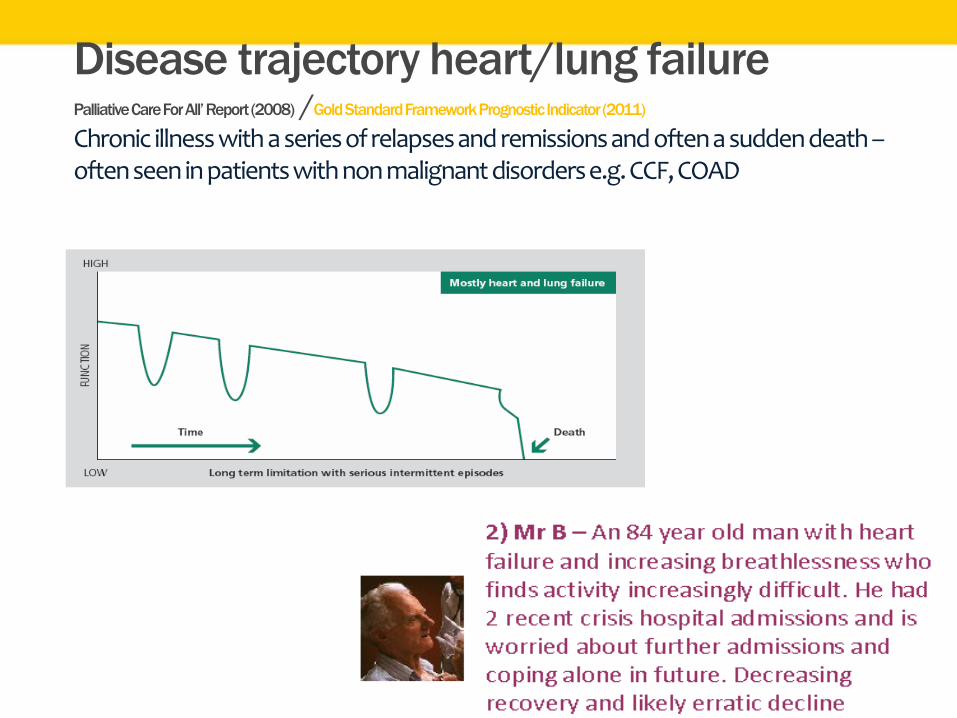
Disease trajectory heart/lung failure Palliative Care For All’ Report (2008) /Gold Standard Framework Prognostic Indicator (2011)
Chronic illness with a series of relapses and remissions and often a sudden death –often seen in patients with non malignant disorders e.g. CCF, COAD
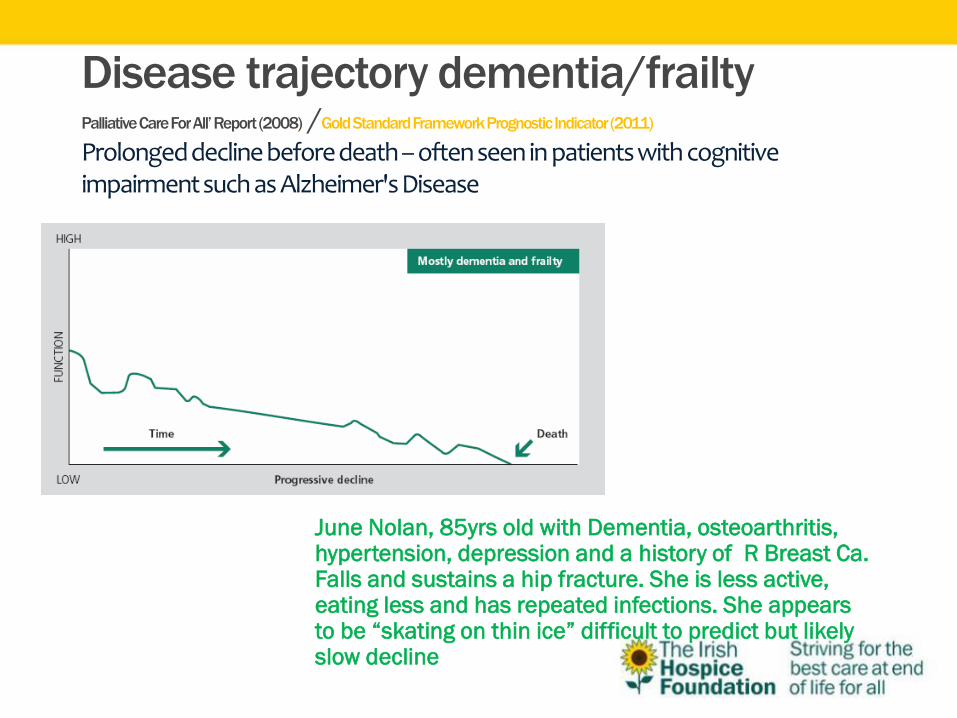
Disease trajectory dementia/frailty Palliative Care For All’ Report (2008) /Gold Standard Framework Prognostic Indicator (2011)
Prolonged decline before death – often seen in patients with cognitive impairment such as Alzheimer's Disease
June Nolan, 85yrs old with Dementia, osteoarthritis, hypertension, depression and a history of R Breast Ca. Falls and sustains a hip fracture. She is less active, eating less and has repeated infections. She appears to be “skating on thin ice” difficult to predict but likely slow decline
• Recognising that a person is entering the dying or terminal phase is critical to appropriate, responsive care, planning and, possibly, a complete shift in the emphasis of care from intervention to comfort.
• Failure to recognise and respond to the dying phase can lead to
• Sub-optimal care
• Inappropriate interventions
• Missed opportunities for patient and family
• Confusion for health care providers
Barriers to Diagnosing Dying
• Fears of hastening death • Unrealistic expectation that the patient may get better • Disagreement within the team or with the family that the
patient is dying • No definitive diagnosis • Lack of knowledge of the management of pain and other
symptoms at the end of life • Poor communication skills • Concerns about withdrawing or withholding treatment • Misinterpretation of the principle of double effect • Concerns about resuscitation • Cultural and spiritual barriers • Legal complexities (Ellershaw & Ward 2003, O’Leary, in Walsh et al, Palliative Medicine, 2009)
• Diagnosing dying should prompt an integrated plan focusing on holistic aims of care • maximize comfort for patient
• enhance support and communication with patient and families
• Key aspects of care are • Multi-disciplinary teamwork
• Discontinuing inappropriate interventions. All possible reversible causes for the current condition have been considered: now considered irreversible – requires medical opinion.
• requires a shift in the focus of care with a need redefine the goals of care
• Neither prolongs nor shortens life
How to diagnose dying – initial signs & symptoms
• Weak/weary • Limited attention span • Unable to sustain conversation • Bed bound • Drowsy for long periods • Disorientated to time/ place/person • Disinterested in family/friends • Anorexia – disinterested in food/fluids • Unable to swallow (Glare, Dickman & Goodman 2011)
Signs & symptoms of the imminent dying process (O’Leary, in Walsh et al, Palliative Medicine, 2009)
Profound progressive weakness bed- bound, sleeping much of the
time Indifference to food and fluid Difficulty swallowing Disorientation to time, with
increasingly short attention span Low or lower blood pressure, weak
pulse Urinary incontinence or retention Loss of ability to close eyes
Oliguria
Hallucinations of previously deceased important individuals
References to going home or similar themes
Changes in respiratory rate and pattern (Cheyne-Stokes breathing, apnoea)
Noisy breathing, airway secretions
Mottling and cooling of the skin
Mental status changes (delirium, restlessness, agitation, coma)
Communication
• For this system to work effectively, a team must
communicative effectively to come to the decision what
stage a resident is at.
• This communication is with
• Resident & family
• ALL nursing home staff
• Wider team (GP)
• Even wider team (specialists)
Communication around dying
• Every effort should be made to communicate with patients regarding
death and dying before they are too frail to have a meaningful conversation
• Can be very challenging for clinicians to assess what patients want to know
• Too much information – induce fear and reduce hope
• Inadequate information – frustrate and diminish trust
Communicating a diagnosis of dying
• Once the patient is thought by the team, to be in the dying phase (hours-days to live) then this should be communicated to the patient, if appropriate.
• Assess the patients insight; issues re death and dying should be explored appropriately and sensitively.
• Afford the opportunity to ask questions
• Care should be taken to illicit the patient’s own preference re end of life and should be documented and implemented where possible. Every effort should be made to ensure that choices such as to the place of death, including the option of a single room or returning home, is identified and respected
(Ellershaw & Ward 2003, HIQA 2009)
Handling difficult questions Examples of difficult questions –
How long have I got?, Is there no hope?, will I have pain?, what does it feel like to die?
Before you answer consider -
•the meaning of the question
•the importance of the question
•why it is being asked
•whether they really want to know
•what the patient may be thinking
•Is there a clear answer
•Will the answer leave uncertainty
Communicating dying to the family
• Assess family’s insights into the patients condition
• Issues regarding death and dying should be explored appropriately and sensitively
• Avoid the use of ambiguous language
• If relatives are told clearly that their loved one is dying, they can
• Ask appropriate questions re time, plan of care
• Stay with the patient/resident
• say their goodbyes
• contact relevant people
• Prepare themselves
(Ellershaw &Ward 2003)

It is often very difficult to predict when the death will happen. This needs to be acknowledged with the family, while at the same time giving them a best guess so that they can prepare themselves for the death.
A useful phrase is
When we see changes on a week to week basis we are usually talking in terms of weeks…and when we see changes on a day to day basis we are usually talking days…
Communicating dying to the family
Truth telling and the dilemmas of collusion
• Most patients with a life threatening illness want to know the truth regarding their situation to enable them to plan their remaining time.
• Truthfulness is a fundamental moral value
• Extending this value to the health care context suggests that a person has an implicit right to information about their body and health in order to maintain emotional and psychological wellbeing
In practice dilemmas and conflicts frequently arise
regarding divulging to patients the seriousness of
their condition
• Often because of the sensitive nature of the information ,
concerns about how the patient may react and prognostic
uncertainty
• “It would kill him if he knew he was dying “
• Families often act like bouncers/gatekeepers trying to protect their loved one
• “Don’t tell him you are from the hospice “ • Requests from relatives to withhold information are most likely to be
motivated by an act of love and the desire to protect • Distress is experienced by relatives regarding their loved one’s potential
reaction to bad news • Fear that the patient may deteriorate faster with the knowledge that time
is limited
Professional responsibility
• Respect the patients desire for more or less information
• Collusion undermines the nurse patient relationship, patient
autonomy and can negatively impact on relationships with
family
Mrs A, A 69 year old woman with cancer of
the lung and known liver secondary's with
increasing breathlessness, fatigue and
decreasing mobility. Concern about other
metastases. Likely rapid decline
• Case 1
• June Nolan, 85yrs old with Dementia, osteoarthritis,
hypertension, depression and a history of R Breast Ca. Falls
and sustains a hip fracture. She is less active, eating less
and has repeated infections. She appears to be “skating on
thin ice” difficult to predict but likely slow decline
Any Questions?