Embed Size (px)
Citation preview

Delivering Health and Care in a Digital Age
Dr Laura RyanAssociate Medical Director NHS24
Oulu May 2015
Overview
• Context• Scotland and Telehealth and Telecare• Examples• Next steps

Ageing Society
Chronicconditions
Lack of healthprofessionals
Financialunsustainability
Health inequalities
HLY vs LE
Further Statistics
• Long-term conditions are more prevalent in older people (58 % >60 compared to 14 % <40)
• people in the poorest social class have a 60 per cent higherprevalence than those in the richest social class
• 30 per cent more severity of disease• £7 out of every £10 of health and social care expenditure on long
term conditions (LTC)

Choices
• Admit to decide• Risk of Harm•

Current behaviors
• Which environment will do the following?– Increase Inpatient mortality by 20%– Increase Inpatient Length of Stay by 1-3 days– Increase likelihood of errors– Increase complaints and litigation.
Evolution!!

NHS Scotland
NHS Scotland
All Boards funded directly from Scottish GovernmentPublic Service funded through taxationFrom urban/post industrial cities to very remote and rural andislandsPrinciples of mutuality, partnership, performanceHS Funding: £12.0 billion

Scottish Strategic Context
• Quality Strategy• 2020 Vision• Integration- The Public Bodies (Joint Working) (Scotland) Bill• Scottish Patient Safety Programme• National Out of Hours Primary Care Review
“ Everyone is able to live longer healthier lives athome, or in a homely setting. We will have ahealthcare system where we have integrated healthand social care, a focus on prevention,anticipation and supported self management.When hospital treatment is required, and cannot beprovided in a community setting, day case treatmentwill be the norm. Whatever the setting, care will beprovided to the highest standards of quality andsafety, with the person at the centre of alldecisions. There will be a focus on ensuring thatpeople get back into their home or communityenvironment as soon as appropriate, with minimalrisk of re-admission”
Public Bodies (Joint Working) ( Scotland) Bill 2014
• A framework for integrating health and social care in Scotlandand has cross party political support in the Scottish Parliament
• Health Boards and Local Authorities in partnership with healthand social care professionals, the third sector, users, carers andother key stakeholders.

Technology Enabled Care (TEC)
• “where the quality of cost effective care and support toimprove outcomes for individuals in home or communitysettings is enhanced through technology as an integral part ofcare and support process”
• Integrated Care Fund• 10 million for TEC


Governance
• Scottish Government Health Department• Scottish Assisted Living Programme Board• Joint Improvement Team• National Telehealth and Telecare Advisory Board• Scottish Centre for Telehealth and Telecare• Wider agenda of public service reform using digital technology


Summary of Scotland's Strengths
• Integrated systems• Working with the NHS• Test bed environment• Digital Health Institute


From Supportive Self Management
To
Co Production



SERVICE
REDESIGNICT
Education and Training

Organisational Development
Examples
• Unscheduled Care• Long term condition• Health and Wellbeing


Aim
Provision of rapid access to senior paediatricclinical support for unscheduled care cases byvideo conferencing, initially for clinicians in ruralgeneral hospitals (and selected “no pass”healthcare facilities).

Set Up – NHS 24

Set Up – Hospital responseRecruitment of On Call
Consultants

EvaluationCRH provided a mixed methodapproach of:
• Literature scoping review by NHS HealthcareImprovement Scotland (HIS) and the ScottishHealth Technologies Group
• Site visits to 6 hospitals and qualitativeinterviews with key stakeholders
• Cost consequence analysis by HIS• Activity data analysis
Variation
• “If you’ve seen one rural hospital; you’ve seen one ruralhospital!”

Key Findings
Activity230 calls from August 2013 until July 2014
approx 4 per week
Confidence: Staff and parentsConsistencyTransfer supportLocal knowledge: Capacity and competence.Medico-legalWork arounds
Key Findings (cont)
• One RGH withdrew from PuC due togovernance issues and practical difficulties in retainingpatient’s locally.
• Requests for access to PUCs from several hospitals, ruraland remote GP practices and SAS

Key Findings (cont)Peer Review5 Clinicians
Rural GPPaediatric ED ConsultantPICU ConsultantGeneral Paeds Consultant (DGH)General Paeds Consultant (Tertiary Centre)

Peer Review
Improved care: 33% (Range 20% to 60%)Avoided transfer : 25% (Range 15% to 50%)

Future Aim
• Reduce variability of provision of care for children• Enhance capacity/competence to care for children out with
regional centres.• Increased access to specialist advice.• Improve Quality
Old Age Psychiatry ServicesFeasibility Study
• Aim - To provide specialist assessment andtreatment for care home residents withmental health problems and to offer advice,support and education to care home staffutilising video conferencing facilities.
Old Age Psychiatry Services – Aims cont’d
• To improve management of behavioral and psychiatricsymptoms of dementia
• Improve recognition and treatment of functional disorders inthe care home population.
• Improve end of life care/palliative for elderly patients withmental health problems.
Old Age Psychiatry Telemedicine Clinic• There is evidence to support using telemedicine in dementia.
– Identifying undiagnosed dementia in residential careveterans: comparing telemedicine to in-person clinicalexamination.Shores, M et alInt. J. Geriat. Psychiatry, 19: 101–108. doi:10.1002/gps.1029
– Cognitive intervention for community dwelling olderpersons with memory problems: telemedicine versus faceto face treatment. Poon, P; Hui, E; Dai, D; Kwok, T; Woo, J,International Journal of Geriatric Psychiatry

AbbeyfieldBallachulish
22 care home beds
2 intermediate carebeds
2 respite beds
Very sheltered housing
Lunch Club
Day Care
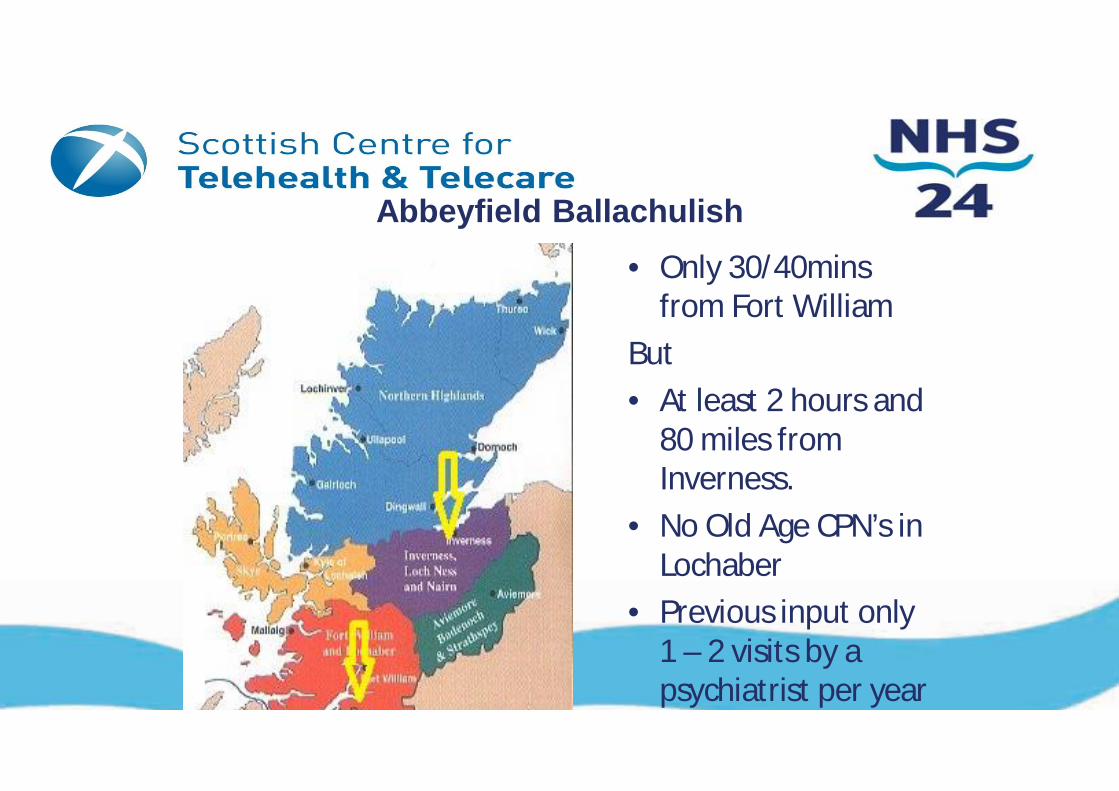
Abbeyfield Ballachulish• Only 30/40mins
from Fort WilliamBut• At least 2 hours and
80 miles fromInverness.
• No Old Age CPN’s inLochaber
• Previous input only1 – 2 visits by apsychiatrist per year

Old Age Psychiatry Telemedicine Clinic
} Nurse led clinic.} Lead nurse – Richard O’Keeffe (Nurse Team Leader of acute
dementia assessment ward)} Twice a week for 2 hours.} Patients can be referred by GP, Psychiatrist or Abbeyfield
Staff.} Any psychiatric problem not just dementia.} Patients can be interviewed, meetings with family, discuss
cases with staff and/or GP via VC.} Supervised by Consultant Psychiatrist.} 6 monthly visits to Abbeyfield (nurse and consultant)
allowing face to face reviews.

Successful??• Reduction in antipsychotic medication.• Some patients managed solely with behavioural
plans.• No new prescriptions for antipsychotics• Staff feel better supported and upskilled in
recognising and managing psychiatric symptoms• Reduction in patient, carer & staff travelling• Sustainable? Live in 2011 – still operational and
rolled out to 2 further care homes in Highland

Developments?• Secured funding from JIT for formal evaluation
– currently underway• Transferable to Community Hospitals (CHIN)• Joint working with Up & About in Care Homes
National Falls Prevention Project• Issues with roll out in NHS Lothian.• Linking with Prescription for Excellence (PfE)
work stream with Dr. John McAnaw
Helsekonferansen 2010

Helsekonferansen 2010
Summary
• Scotland• User centred design• Technology as an enabler• Service redesign and co production


[email protected]@nhs.net






























