Embed Size (px)
Citation preview

The Role of Advanced Technology In the Office-Based Medical Practice (Or Practical IT: IT in
Practice)
David Lee Scher, MD, FACP, FACC, FESC, FHRS
Twitter: @dlschermd
May, 2011

“The most valuable commodity that I know of is information”.
-Gordon Gekko

Electronic Health Record: Hub of Office Technology

Say Goodbye

Say Hello

Not the Goal!!

The Benefits Of Health Information Technology: A Review Of The Recent Literature Shows Predominantly
Positive Results
Health Aff March 2011 30:3464-471
• Meta analysis July 2007-Feb 2010
• 278 outcome measures were evaluated across all studies included in final sample.
• 62% found positive results.
• 30% found mixed, predominantly positive results.
• 8% found negative or mixed, but predominantly negative results
Health Aff March 2011 30:3464-471

EHRs
• The Health Information Technology for Economic and Clinical Health Act (HITECH)
• The Electronic Health Record (EHR) is a longitudinal electronic record of patient health information generated by one or more encounters in any care delivery setting.
– Important: EHR is not EMR: an EHR is an EMR with interoperability (i.e. integration to other providers’ systems).

HIT and Government :ONC Releases Five Year Strategic Plan
1.Achieve adoption and
information exchange through
Meaningful Use of health IT.
2.Improve care, improve
population health, and reduce
health care costs.
3.Inspire confidence and trust in
health IT (Privacy /Security).
4.Empower individuals with health
IT (PHR).
5.Achieve rapid learning and
technological advancement.

What Electronic Healthcare Records Do and Don’t Do
International Healthcare Technology News:
Healthcare IT and Technology News Blog
FRIDAY, 22 JULY 2011 20:56
David Lee Scher, MD, FACP, FACC, FESC, FHRS
http://healthcaretechnologymagazine.com/blogs

Ten Ways Healthcare Providers Can Get the Most out of EHRs
Theehrproject.com

Health Information Exchange – The Regional Model?
Standards-based communication; regionally and beyond

Health Information Exchange – The National Model?

The Ideal Office IT Network• Inexpensive.
• Shallow learning curve.
• No dedicated personnel required, easy maintenance.
• Eternally guaranteed and secure.
• Includes medical records, office clinical and administrative operations, and communication network.
• Interacts seamlessly with hospital, government agencies, outside labs, referral physician EMRs, and device company remote monitoring systems.
• Mhealth accessible (mobile communications).

Clinical Benefits of an IT Network
– Facilitates better patient coordination/management among office staff and providers.
– Easier access to health information exchanges (HIEs).
– Facilitates clinical research (patient recruitment, follow-up, outcomes).
– Better and more efficient implantable device follow-up/management.
– Working data base (able to be mined).

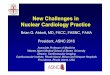
Remote Monitoring of Cardiac Rhythm Devices

Aspects of Remote Patient
Management
Remote Monitoring
• Device safety alerts
• Arrhythmia alerts
1
Remote Follow-Up
• Patient convenience
•Improves efficiency
2
On Demand Interrogation
• Determine rhythm/device function
• Reduce office/ER visits
3

Arrhythmia Monitoring: Clinical Information
• Atrial tachyarrhythmias
– Duration
– Associated symptoms
• Ventricular Arrhythmias
– Therapeutic efficacy
– Therapy-induced acceleration

Arrhythmia Monitoring: Clinical Implications
• Ventricular arrhythmias– Reprogramming of ICD
– Therapeutic changes• Electrolyte monitoring
• Adjuvant AA drug therapy/ablation
• Atrial arrhythmias– Anticoagulation?
– AA drug therapy
– Ablation

Advantages of Remote F/U
Safety alert notification
Arrhythmia detection
Integration with electronic health records
Cost savings
Secondary utilization of data

Patient Follow-Up Compliance
• Randomization gp 3mo 6mo 9mo 12mo
• Remote (%) 88 90 88 84
• Conventional F/U(%) 91 78 73 65
TRUST Study: Varma N, et al. AHA 2008

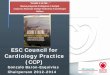
The Clinical Evaluation of Remote NotificatioN to
REduCe Time to Clinical Decision (CONNECT)
Trial: The Value of Remote Monitoring
Crossley G, Boyle A, et al Am Heart J 2008:156;840-6

Time from Event to Decision by Alert Type (median days)
Device Event
No. of Events (No. of Patients)
No. of Days from Event Onset To Clinical Decision
Median (InterquartileRange)
Remote In-office Remote In-office
AT/AF burden at least 12 hrs 437 (107) 280 (105) 3 (1, 15) 24 (7, 57)
Fast V rate at least 120 bpmduring at least 6 hrs AT/AF
41 (26) 47 (37) 4 (2, 13) 23 (5, 40)
At least 2 shocks delivered in an episode
44 (35) 32 (23) 0 (0, 1.5) 0 (0, 2)
Lead impedances out of range 26 (18) 12 (6) 0 (0, 9) 17 (5.5, 45)
All therapies in a zone exhausted for an episode
16 (12) 11 (6) 0 (0, 1) 9 (0, 36)
VF detection/therapy off 10 (10) 8 (8) 0 (0, 0) 0 (0, 84)
Low battery 1 (1) 1 (1) 30 0
Total 575 (172) 391 (145) 3 (0, 13) 20 (4, 52)




Randomized Multicenter Comparison of Home Monitoring vs Regular F/U in MADIT II Pts
• 115 pts, 110 single chamber, 5 dual chamber ICDS
• Randomized after 3 months to 1 office f/u with HM or Q 3 month office f/u with HM
• Endpoints:
– primary-number of unplanned visits
– Secondary- total costs, QOL, total mortality
Elsner CH et al. Proceedings Computers Cardiology 2006;33:241-244

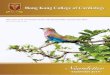
Randomized Multicenter Comparison of Home Monitoring vs Regular F/U in MADIT II Pts:
Results
• Mean F/U time 117 days (23-513)
• No significant difference in hospitalization or mortality rates.

Office Visits
Elsner CH et al. Proceedings Computers Cardiology 2006;33:241-244

Transportation Costs
Elsner CH et al. Proceedings Computers Cardiology 2006;33:241-244

Physician Time
Elsner CH et al. Proceedings Computers Cardiology 2006;33:241-244

Clinic Costs
Elsner CH et al. Proceedings Computers Cardiology 2006;33:241-244

Economic Advantages of Remote Monitoring
• Provider:– Reduced office utilization
– Increased Reimbursement
• Patient: Reduce patient visits– Travel costs
– Eliminates of patient loss of work costs
• CRM Company:– Personnel for office follow-ups and troubleshooting

The Ideal Patient for Remote Monitoring
• Single chamber ICD for primary prevention.
• NO ICD shocks or arrhythmias first three months post implant.
• Rare or controlled atrial fibrillation.
• Clinically stable CHF and coronary artery disease.

In Office Follow-up
• Frequent nonsustained VT.
• AF with many high ventricular rate episodes.
• Unstable or changing impedances and/or thresholds.
• CHF with associated arrhythmias.
• Multiple ICD shocks or inappropriate shock.
• After changes in AA drugs.

Interoperability of Remote Monitoring Data With EMRs
• A natural progression of technology.
• Both shown to increase efficiency, eliminate paper, improve patient management, and outcomes.
• “Obstacles”:
Cost to companies:• A: Cost of doing business, both standard of care in
2010.
Proprietary nomenclature• A: Most device features now equivalent, addressed by
IDCO (Implantable Device-Cardiac Observation)
“Not enough demand from customers”

Ideal IT Cardiac Implantable Electronic Device Management
• Incorporates remote monitoring data and in-office data.
• Easily viewed settings, arrhythmias, and therapies delivered.
• Clinical and device data on same screen.





SUMMARY
• EHRs are the hub of office IT.
– May incorporate EHR, practice management tools.
• Remote monitoring of CRM devices is economically and clinically beneficial.
• Interoperability of CRM devices and EHRs still challenged but will happen seamlessly.
• Get with both programs: they’re here to stay and are standards of care!

“If you ask me a question I don’t know,
I’m not going to answer”
------Yogi Berra