Embed Size (px)
Citation preview

Pseudonymised GP data extraction for risk stratification
CCIO Leaders Network Annual Conference04 November 2014
Dr Brendan O’BrienConsultant Clinical Informatics Specialist (CCIO)Regional Health & Social Care Board, NI.
NI ContextPopulation: 1.8 million
Integrated Health & Social Care
Budget ~ £4.5 billion
Purchaser provider split
Commissioners: HSCB & PHA
Providers: 5 Acute Trusts, Regional Ambulance Service351 GP practices

Clinical Priority AreasPatients risk stratified according to complexity of needs.Four priority areas set by DHSSPS.• Frail elderly patients• Respiratory patients• Diabetic patients• Patients with a history of stroke / TIA
Approach• Data pseudonymised at source (only the GP practice know the patients identity)• MIQUEST approach used for the data extraction• Only coded information extracted• HSCB writes the HQL code for the data extraction• GP practices run the HQL queries• HSCB conducts analysis on pseudonymised data set from GP practices• Stratified list for each clinical area returned to practices• Practice re-identify patients, add soft knowledge and proactively manage those
patients with greatest number of factors associated with unplanned admissions• HSCB will aggregate the extract for public health and commissioning uses
Agreement between HSCB & each Practice
Covers sharing ofanonymised andpseudonymisedpatient level data.

MIQUEST• Free software for extracting and aggregating data
from all GP systems• Incorporates strong security and confidentiality
safeguards• Adopted as standard within the NHS for data
extraction• Part of RFA99 (requirements for Accreditation)

LOCAL ENQUIRER QUERY
• Import query• Run query• Output response• Use the data
GP Practice
REMOTE ENQUIRER QUERY
• Import the query• Authorise the query• Run query• Authorise response• Output response• Use the data
HSCB or other enquirer
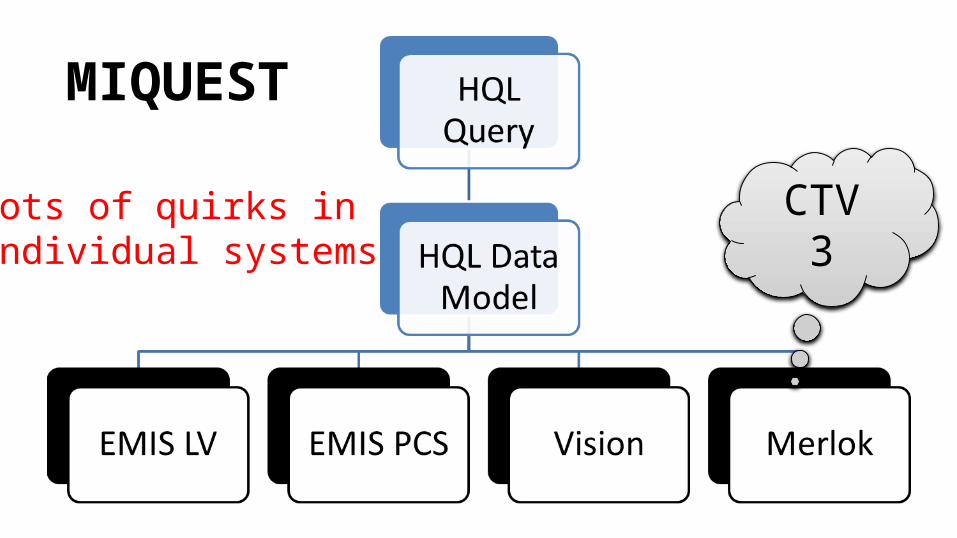
MIQUEST
CTV 3Lots of quirks inIndividual systems
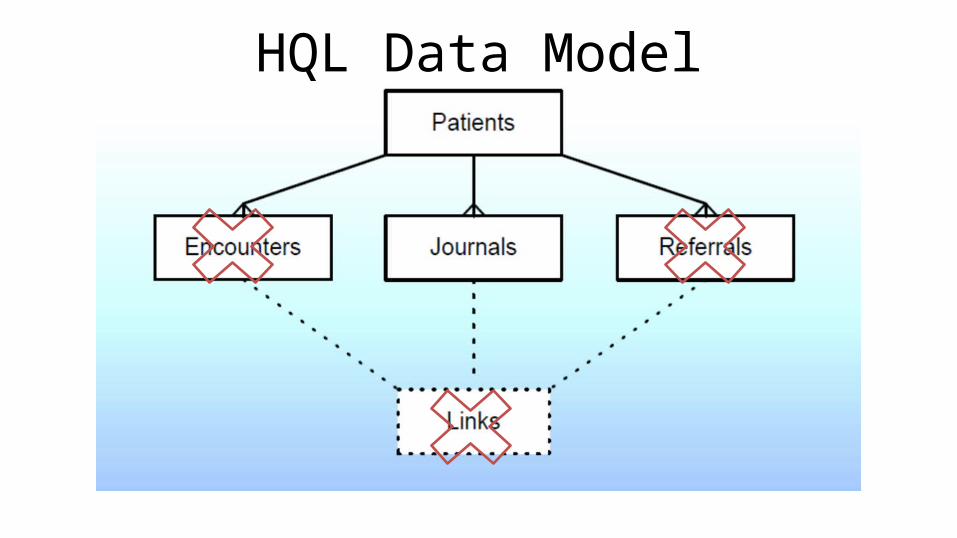
HQL Data Model
Main Factors• Emergency admissions in past 12 months• Polypharmacy• High risk drugs: NSAIDs, diuretics, anticoagulants,
antiplatelets• Number of comorbidities (20 registers)• Test results• Smoking status, alcohol intake• ‘Soft knowledge’ added by GP Practice

Challenges• No validated risk prediction algorithm for NI population• Care.data = increased stakeholder concern• 4 GP Systems, 3 coding schemes– Vision: Read Version 2– EMIS PCS: Read Version 2– EMIS LV: Read Version 2 + proprietary codes– Crosscare (Merlok): Clinical Terms Version 3

Pseudonymisation At SourceWe’re not
Brazil CARE.DATA
We’re Northern Ireland.
Progress to date• 1,124,040 patients records extracted so far• 1,692 patients excluded from extract (0.15%)
– Due to controversy around care.data the decision was made to exclude data on patients whose clinical record contained a Read code opting them out of the Emergency Care Summary (ECS) extract.
• 92% of GP practices signed up to the enhanced service– Covering 93% of NI population– EMIS LV and Merlok extractions this month
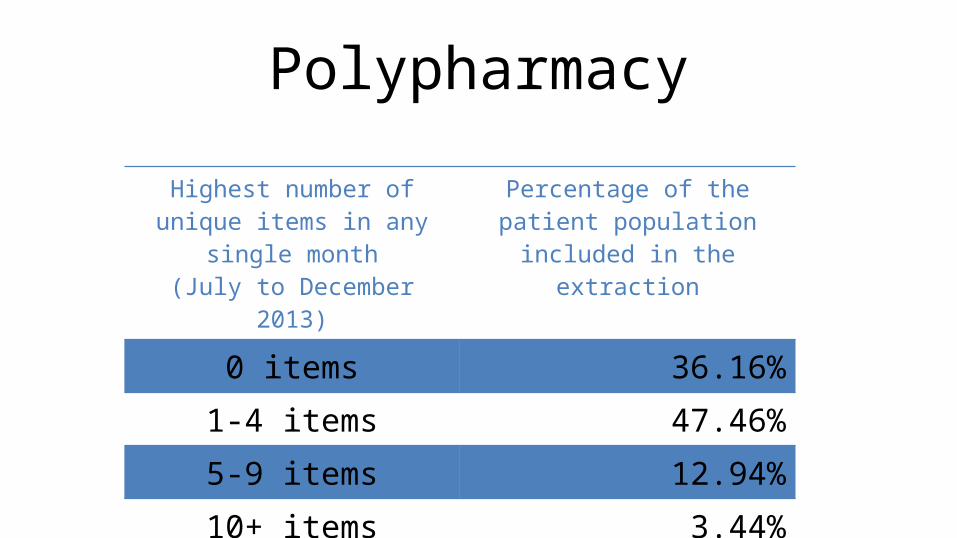
Highest number of unique items in any single month
(July to December 2013)
Percentage of the patient population included in the
extraction
0 items 36.16%1-4 items 47.46%5-9 items 12.94%10+ items 3.44%
Polypharmacy
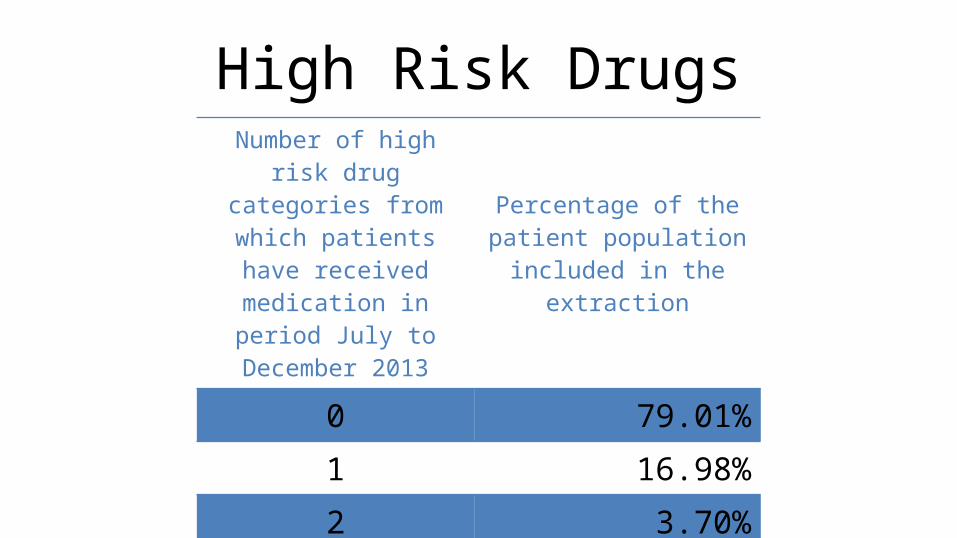
High Risk DrugsNumber of high risk drug
categories from which patients have received
medication in period July to December 2013
Percentage of the patient population included in the
extraction
0 79.01%1 16.98%2 3.70%3 0.30%4 0.01%
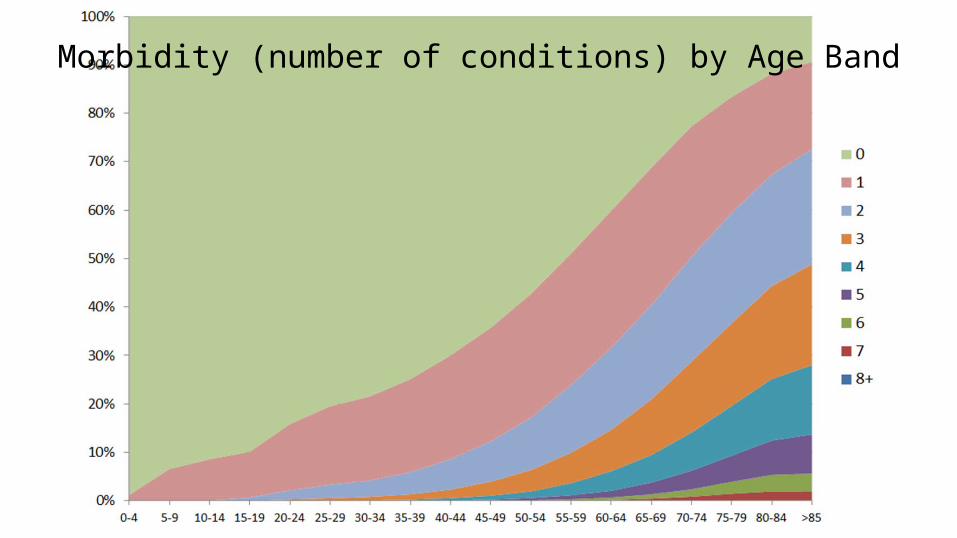
Morbidity (number of conditions) by Age Band
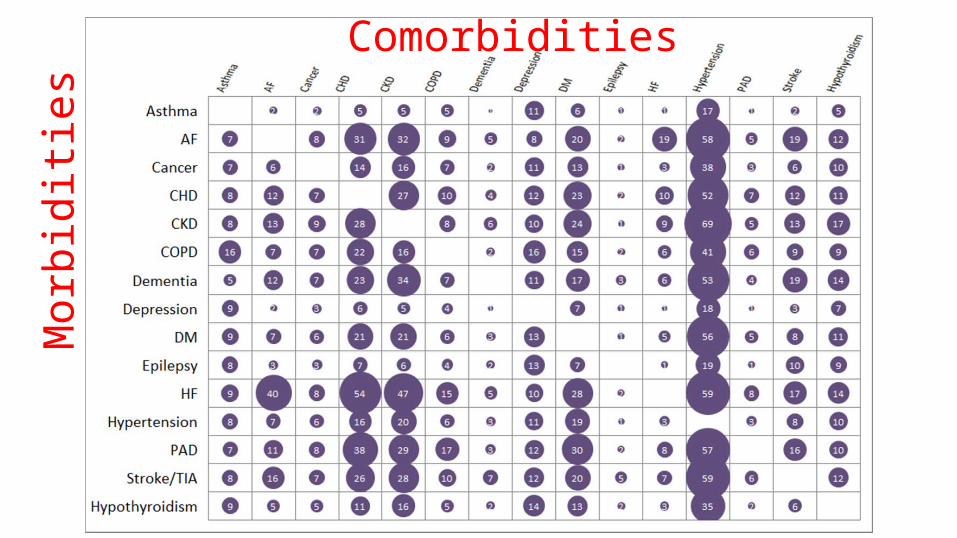
Mor
bidi
ties
Comorbidities


![Courses / Instructors - 2011/2012 [Fall Term] | (Id: OPAS …...Jaffer Sheyholislami Natalia Artemeva Waltraud O'Brien Waltraud O'Brien Jaffer Sheyholislami € Waltraud O'Brien €](https://img.pdfslide.us/doc/110x75/61378f230ad5d2067648b2ea/courses-instructors-20112012-fall-term-id-opas-jaffer-sheyholislami.jpg)