Embed Size (px)
Citation preview

INFLUENZA A EMERGENCY
PREPAREDNESS
BYDR. MOUSTAPHA A. RAMADANMDINFECTION CONTROL DOCTOR & HOSPITAL EPIDEMIOLOGIST

OBJECTIVES OF THE SESSION
I. Introduction/ Facts
II. Seasonal / Pandemic/ Zoonotic-variant Flu
III. Emergent types
IV. Risk Assessment
V. Preparedness / Infection control and prevention of
influenza

INTRODUCTION The flu is a contagious respiratory illness caused by
influenza viruses that infect the nose, throat, and lungs. It can cause mild to severe illness, and at times can lead to death.
The incubation period is 1-3 days, and the period of communicability among adults is 1 day before onset of symptoms up to 5 days after becoming sick.
MOT : Contact (Droplet/Direct/Indirect) Airborne

INTRODUCTION Morbidity tends to be high and mortality low (1–4%).
Global estimates are 30-50 millions are affected yearly, 250 000-500 000 deaths yearly
Influenza hospitalizations rates (20.3/100,000 to 321.1/100,000, depending on age group)

INFLUENZA VIRUS
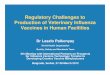
A/Fujian/411/2002 (H3N2)
NeuraminidaseHemagglutinin
Type of nuclearmaterial
Virustype
Geographicorigin
Strainnumber
Year of isolation
Virus subtype

INFLUENZA ANTIGENIC CHANGES
Antigenic Shift• major change, new subtype• caused by exchange of gene segments• may result in pandemic
Example of antigenic shift• H2N2 virus circulated in 1957-1967• H3N2 virus appeared in 1968 and completely replaced
H2N2 virus

INFLUENZA ANTIGENIC CHANGES
Antigenic Drift• minor change, same subtype• caused by point mutations in gene• may result in epidemic
Example of antigenic drift• in 2002-2003, A/Panama/2007/99 (H3N2) virus was
dominant• A/Fujian/411/2002 (H3N2) appeared in late 2003 and
caused widespread illness in 2003-2004


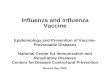
SubType People Poultry Pigs Bats / Other
H1
H2
H3
Other Animals
H4
Other Animals
H5
H6
H7
Other Animals
H8
H9
H10
H11
H12
H13
H14
H15
H16
H17
H18
SubType People Poultry Pigs Bats / Other
N1
N2
N3
N4
N5
N6
N7
Other Animals
N8
Other Animals
N9
N10
N11

SEASONAL INFLUENZA Seasonal influenza viruses circulate and cause
disease in humans every year.
In temperate climates, disease tends to occur seasonally in the winter months, spreading from person-to-person through sneezing, coughing, or touching contaminated surfaces.

SEASONAL INFLUENZA Seasonal influenza viruses can cause mild to severe
illness and even death, particularly in some high-risk
individuals (pregnant women, the very young and
very old, immune-compromised people, and people
with chronic underlying medical conditions).

PANDEMIC INFLUENZA A pandemic is a global outbreak when an influenza
virus which was not previously circulating among
humans and to which most people don't have
immunity emerges, infects and spreads easily
among humans in an efficient and sustained way.

PANDEMIC INFLUENZA As the majority of the population has no immunity to
these viruses, the proportion of persons in a population getting infected may be quite large.
Some pandemics may result in large numbers of severe infections while others will result in large numbers of milder infections, but the reasons behind these differences are not completely understood.

ZOONOTIC/VARIANT INFLUENZA Influenza viruses that are routinely circulating in
animals, such as avian influenza virus subtypes A(H5N1) and A(H9N2), swine influenza virus subtypes A(H1N1) and (H3N2) and other species including horses and dogs.
These viruses are distinct from human influenza viruses and do not easily transmit between humans.

ZOONOTIC/VARIANT INFLUENZA Occasionally humans can acquire these infections
through direct contact with infected animals or contaminated environments, and may cause disease ranging from mild conjunctivitis to severe pneumonia and even death.
If such a virus acquired the capacity to spread easily among people either through adaptation or acquisition of certain genes from human viruses, it could start an epidemic or a pandemic.


EMERGENT TYPES

AVIAN INFLUENZA A (H5N1)

AVIAN INFLUENZA A (H5N6)
Since 2014, a total of 16 laboratory-confirmed cases of human infection with influenza A(H5N6) virus, including six deaths, have been reported to WHO from China.
Although other influenza A(H5) subtype viruses have the potential to cause disease in humans, no human cases, other than those with influenza A(H5N1) and A(H5N6), have been reported so far.
Influenza A(H5N8) have been detected in wild birds and domestic poultry in several countries in Africa, Asia and Europe.

AVIAN INFLUENZA A (H7N9) Since 2013, a total of 1223 laboratory-confirmed human
infections with avian influenza A(H7N9) virus were reported to WHO including 380 deaths.
Human infections with the A(H7N9) virus are unusual and need to be monitored closely in order to identify changes in the virus and/or its transmission behaviour to humans as it may have a serious public health impact.
Public health risk assessment found the risk from avian influenza A(H7N9) viruses has not changed

AVIAN INFLUENZA A (H7N9) Though small clusters of cases have been reported,
including those involving healthcare workers, current epidemiological and virological evidence suggests that this virus has not acquired the ability of sustained transmission among humans.
WHO advises travellers to countries with known outbreaks of avian influenza should avoid, poultry farms, contact with animals in live bird markets, entering areas where poultry may be slaughtered, or contact with any surfaces that appear to be contaminated.

AVIAN INFLUENZA A (H7N9)

AVIAN INFLUENZA A (H7N9)
Experts from (WHO) and (GISRS) reviewed available epidemiologic and virologic data related to influenza A(H7N9) viruses to evaluate the need to produce additional CVVs to maximize influenza pandemic preparedness.
Two additional H7N9 CVVs were recommended for development: a new CVV derived from an A/Guangdong/17SF003/2016-like virus ;and a new CVV derived A/Hunan/2650/2016-like virus.
At this time, CDC is preparing a CVV derived from an A/Hunan/2650/2016-like virus using reverse genetics.

AVIAN INFLUENZA A (H7N2) Since 2002, a total of 3 laboratory-confirmed human
infections with avian influenza A(H7N2) virus were detected in USA. ( Latest December 2016)
In 2007, UK reported 4 human cases linked to l an outbreak of avian influenza in poultry at a smallholding in Wales.
No human-to-human transmission was detected

AVIAN INFLUENZA A (H7N2) One associated human infection in a person who
had close, prolonged unprotected exposure to the respiratory secretions of infected, sick cats. A Second infection was associated with exposure to infected poultry and third was undetermined.
Cats are not the typical host of avian influenza viruses; however, cats have been infected in the past with such viruses (avian and human seasonal).

AVIAN INFLUENZA A (H9N2)
Up to date around 35 cases of laboratory confirmed human infections with avian influenza A(H9N2) virus were reported to WHO including ONE death.
Most human cases are exposed to the A(H9N2) virus through contact with infected poultry or contaminated environments.
No case clusters have been reported.

SWINE INFLUENZA
In USA since 2005, 9 laboratory-confirmed human infections with influenza A v(H1N2) virus were detected; 4 during 2016.
December 2016, the first human case of A/Indiana/08/2011-like H3N2v influenza virus infection reported to WHO from Canada.
No human-to-human transmission was detected

CANINE INFLUENZA Also known as dog flu is a contagious respiratory disease
in dogs caused by specific Type A influenza viruses known to infect dogs.
No human infections with canine influenza have ever been reported.
There are two different influenza A dog flu viruses: one is an H3N8 virus and the other is an H3N2 virus
Canine influenza H3N8 virus originated in horses, has spread to dogs, and can now spread between dogs.
The H3N2 canine influenza virus is an avian flu virus that adapted to infect dogs

BAT FLU Bat flu was first discovered in Guatemala during a study
conducted in 2009 and 2010.
The surface protein coding genes were found to be
extraordinary different from know flu viruses.
CDC had classified these genes into H17, H18 and
N10,N11.
No human infections with bat flu have ever been reported.

RISK ASSESSMENTMay 2016, WHO has launched Tool for Influenza Pandemic Risk Assessment (TIPRA) version I.
(TIPRA) is an influenza hazard assessment tool designed to assess the likelihood and potential impact of a virus becoming a pandemic strain.

TIPRA a standardized, streamlined, transparent hazard assessment
tool designed for influenza A viruses with pandemic potential; a tool to assist global and Member State pandemic influenza
planning and preparedness, particularly states affected by viruses of concern;
a tool for informing comprehensive influenza and public health risk assessment, risk management and risk communication; and
a tool designed to allow hazard assessment with incomplete data, providing a robust means of identifying information gaps, which may direct surveillance and research resources.

TIPRAThe objectives of TIPRA are to:
support a timely, updatable virological risk assessment for influenza
viruses with pandemic potential;
transparently document features of the virus that might pose
threats to a human population;
identify knowledge gaps and prompt further investigations
including research and surveillance;
facilitate information-sharing among scientists, policy-makers and
other stakeholders

TIPRA Initiating a TIPRA application requires a known human
case, development of a virus profile, and engagement of appropriate expertise to score all TIPRA risk elements.
The availability of data and ability to infer on high-weight risk elements should be considered prior to the initiation of a TIPRA run.

TIPRAScoring consistencyIn order to ensure comparability between viruses, it is essential that experts score viruses consistently.TIPRA risk element definitions and scoring strata attempt to minimize ambiguityViruses assessed must be clearly defined, as risk may vary depending on the level at which viruses are differentiated.

TIPRAPopulation immunity gatewayThe gateway is based on preexisting population serological immunity to the virus. If 30% of the population aged 18 years has evidence of cross-reactive antibodies, the virus is considered to have low pandemic risk, so assessment of other factors of pandemic risk is not essential.Experts devised this gateway cut-off based on review of previous pandemic data.

TIPRATimeliness: To maximize utility, risk assessment outputs must be timely.WHO estimated that each virus profile required approximately eight days of input -- four days epidemiology, four days virology -- with additional time for expert review and refinement.

TIPRANational capacity:National stakeholder awareness and involvement in TIPRA is essential. This involves awareness among International Health Regulations (IHR) National Focal Points (NFPs), National Influenza Center teams, influenza disease program managers and outbreak emergency risk assessment and management teams.
National capacity is required to incorporate findings into more comprehensive risk assessments that also consider exposure and context

TIPRADocumentation and Replication:TIPRA provides a snapshot at a point in time based on historical and the most up-to-date data. It is critical to document when the assessment was conducted and what information was available at the time.
TIPRA should be repeated for key viruses as new information comes to light. This is equally true for context and exposure assessments and risk management strategy development and option evaluation.

INFECTION PREVENTION The first and most important step in preventing flu is to get a
flu vaccination each year.
There are two forms for influenza vaccine Inactivated Form and Live attenuated Form.
The nasal spray flu vaccine (live attenuated influenza vaccine or LAIV) should not be used during 2016-2017.
This is based on data showing poor or relatively lower effectiveness of LAIV from 2013 through 2016.

INFLUENZA VACCINEFor 2016/2017 winter (Northern Hemispere)
an A/California/7/2009 (H1N1)pdm09-like virus;
an A/Hong Kong/4801/2014 (H3N2)-like virus;
a B/Brisbane/60/2008-like virus
++ B/Phuket/3073/2013-like virus.
For 2017 winter Season Southern Hemishpere
an A/Michigan/45/2015 (H1N1)-like virus; replace the A/California/7/2009.

HEALTHCARE PREPAREDNESSHealth-care facilities should prepare for communicable disease emergencies by : organizing permanent IPC activities, surveillance and training of dedicated personnel and clinical staff; creating a multidisciplinary group within the health-care facility to develop a preparedness plan; performing a plan evaluation and monitoring exercise, and updating the plan as necessary; and strengthening liaison with other levels of the health-care system and public health authorities.

HEALTHCARE PREPAREDNESSThe main goals of the plan are :
identify, isolate and report early cases of a putative
epidemic or pandemic ARI virus;
keep the health-care system functioning for pandemic and
non-pandemic patients; and
reduce the risk of pandemic ARI transmission associated
with health care.

HEALTHCARE PREPAREDNESS
1- Surveillance
2- Triage
3- Surge capacity
4-Access
5- Infection prevention and control
6- Occupational health program
7- Patient flow and discharge plan
8- Mortuary
9- Risk communication policy
10- Promotion of outpatient care of ARI patients
Components of health-care facility pandemic acute respiratory infection preparedness plan

INFECTION PREVENTION AND CONTROL Minimize Exposures Implement Engineering Control Implement Infection Control Precautions Monitor and mange ill and exposed healthcare workers Train and Educate healthcare workers Implement Environmental Infection Control Manage visitor access and movement within the facility

MINIMIZE EXPOSURES prompt screening and triage of symptomatic patients,
provide space and encourage persons with symptoms of
respiratory infections to sit as far away from others as
possible
implementation of respiratory hygiene and cough
etiquette

MINIMIZE EXPOSURES placement of a facemask on symptomatic patients upon
entry to the facility,
rapid implementation of airborne isolation precautions, in
additional to standard and contact precautions
Provide supplies to perform hand hygiene to all patients
upon arrival to facility and throughout the entire duration
of the visit to the healthcare setting.


IMPLEMENT ENGINEERING CONTROL
Installing physical barriers such as partitions in triage areas, curtains that are drawn between patients in shared areas.
Reducing exposures related to specific procedures such as using closed suctioning systems for airways suction in intubated patients.
Ensuring that appropriate air-handling systems (with appropriate directionality, filtration, exchange rate, etc.) are installed and maintained in healthcare facilities.

IMPLEMENT INFECTION CONTROL PRECAUTIONS
Patient should be isolated in AIIR, single bed room.
Standard, Contact and Airborne precautions should be implemented for patients with suspected or confirmed novel influenza for the period of illness/stay.
Remove PPE at doorway or in anteroom. Remove respirator after leaving patient room and closing door.
Cleaning environmental surfaces with water and detergent and applying commonly used disinfectants (such as hypochlorite) is effective and sufficient.

PRECAUTIONS FOR AEROSOL-GENERATING PROCEDURES
Only performing these procedures if it cannot be postponed
Limiting the number of HCP present during the procedure to
only those essential for patient care and support
Perform the procedures in an AIIR when feasible
Consider use of portable HEPA filtration units to further
reduce the concentration of contaminants in the air

PRECAUTIONS FOR AEROSOL-GENERATING PROCEDURES
Unprotected HCP should not be allowed in a room where
an aerosol-generating procedure has been conducted
HCP should adhere to standard and airborne precautions
including wearing gloves, a gown, a face shield and N95
Conduct environmental surface cleaning following
procedures

MANAGEMENT OF ILL HCW Stop patient-care activities.
Notify their supervisor, preventive medicine and infection
control personnel
Excluded from work until for 10 days and monitor S/S
Don a facemask, Perform Cough Etiquette, Hand Hygiene
Start treatment

MANAGEMENT OF ILL HCW Facilities should consider dedicating HCWs caring for
suspected and confirmed cases.
Facilities should keep track of all HCWs who care for or
enter the rooms of these patients
Facilities should implement sick leave policies for HCWs
Facilities should provide medical consultation and
prompt treatment for HCWs

TRAINING AND EDUCATIONHCW should be knowledgeable about :
Influenza signs, symptoms, and risk factors for complications.
Vaccination, ways to minimize exposure including respiratory hygiene and cough etiquette.
Infection prevention and control precautions specially during aerosol generating procedures

ENVIRONMENTAL CONTROL MEASURES Standard cleaning and disinfection procedures are
adequate for influenza virus environmental control in all settings within the healthcare facility.
Management of laundry, food service utensils, and medical waste should also be performed in accordance with infection control policies and standard procedures.

MANAGE VISITOR ACCESS AND MOVEMENT WITHIN THE FACILITY Limit visitors for patients in isolation to persons who are
necessary for the patient’s emotional well-being and care. All visitors should follow respiratory hygiene and cough
etiquette precautions Facilities should consider tracking (e.g., log book) all
visitors who enter patient rooms. Visitors should not be present during aerosol-generating
procedures. Visitors should be instructed to limit their movement within
the facility.

MANAGE VISITOR ACCESS AND MOVEMENT WITHIN THE FACILITY Facilities should provide instruction, before visitors enter
patients’ rooms, on hand hygiene, limiting surfaces touched, and use of PPE according to current facility policy while in the patient's room.
Visitors are advised to change personal clothes every day
Exposed visitors should be advised to report any signs and symptoms of acute illness to their health care provider for a period of at least 10 days after the last known exposure to the sick patient.

REFERENCES https://www.cdc.gov/flu/index.htm http://www.who.int/influenza/en/ Launching the tool for Influenza Pandemic Risk assessment (TIPRA)
meeting report. WHO 2016 Infection prevention and control of epidemic-and- pandemic prone acute
respiratory infections in healthcare WHO guidelines 2014. Pandemic Influenza preparedness Framework for the sharing of influenza
viruses and access to vaccines and other benefits. WHO 2011. Occupational Safety and Health Administration (OSHA) 2009: Pandemic
Influenza Preparedness and Response Guidance for Healthcare Workers and Healthcare Employers.
Influenza Update N° 283 20 Feb 2017 WHO “Influenza at the human-animal interface” last update 14 Feb 2017