Embed Size (px)
Citation preview

Viral arthritis : chikungunya and
beyond ARVIND CHOPRA
CENTER FOR RHEUMATIC DISEASESPUNE
www.rheumatologyindia.org
IRACON 2016, KOCHI

EVIDENCE DATA BASE• Venugopalan A, Ghorpade RP, Chopra A. Cytokines in Acute Chikungunya. PLoS ONE 2014
9(10): e111305. doi:10.1371/journal.pone.0111305• Chopra A, Saluja M, Venugopalan A. Chloroquine effectiveness and inflammatory cytokine
response in early persistent post chikungunya musculoskeletal pain and arthritis. Arthritis Rheum 2014;66(2):319-326.
• Chopra A, Anuradha V, Ghorpade R, Saluja M. Acute chikungunya and persistent musculoskeletal pain following the 2006 Indian epidemic: a 2-year prospective rural community study. Epidemiol Infect 2012;140(5):842-50.
• Chopra A, Venugopalan V. Persistent rheumatic musculoskeletal pain and disorders at one year post- chikungunya epidemic in south Maharashtra- a rural community based observational study with special focus on naïve persistent rheumatic musculoskeletal cases and selected cytokine expression. Indian J Rheumatol 2011;6:5-11
• Mathew AJ, Goyal V, George E, Thekkemuriyil DV, Jayakumar B, Chopra A. Rheumatic-musculoskeletal pain and disorders in a naïve group of individuals 15 months following a Chikungunya viral epidemic in south India: A population based observational study. Int J Clin Pract 2011;65(12):1306-1312.
• Chopra A, Anuradha V, Lagoo-Joshi V, Kunjir V, Salvi S, Saluja M. Chikungunya virus aches and pains: an emerging challenge. Arthritis Rheum 2008;58(9):2921-22.

CHIKV: MCQ 1The virus isA. Single stranded RNA alphavirus transmitted from
anophelesB. Single stranded DNA alphavirus transmitted from
anophelesC. Single stranded RNA flavivirus transmitted from
monkeysD. Single stranded DNA flavivirus transmitted from
chicken

Chikungunya virus (CHIKV) is a mosquito borne, single-stranded,
positive-sense RNA virus (genus alphavirus) that
has caused sporadic and epidemic
outbreaks of predominantly rheumatic disease
every 2–50 years, primarily in Africa and Asia;
In 2006, it returned to INDIA after 34 years & refuses to EXIT

Acute CHIKUNGUNYA-My Story, My CV
• Onset 7 pm. 04 Sept 16- Bolt from the Blue
• Fever, chills, pain/stiffness multiple joints
• Severe phase lasted for 3 days
• Lab: 3rd day PCR +, transient dip in platelets & TLC
• Asymptomatic from 6th-10th day; IgM +
• Later, Sub-acute mild chronic phase till date
• More of tenderness, stiffness, some tasks difficult
• Resumed exercises (+jogging) for 30 minutes 5th post onset
• Never lost a single day of work
• Travelled to The Netherlands, Iran, Singapore, USA, Chennai and now IRACON
• Other Sufferers: Wife, son, Wife’s parents, Cook, House help

From onset (04 Sept 2016) till date (10 weeks)
Other sites: (i) ANKLES: dorso lateral joint margin/ peroneal region tender (painVAS upto 3/10), mild
puffiness, episodic aggravation and difficulty pronounced in coming down the stair case, pain VAS 0-4/10
(ii) KNEESS: Episodic lateral joint margin
Note: Moderately severe persistent MSK pains & STIFFNESS (MOSTLY DISTAL LEGS) lasted for 3-4 days post
onset, later mild –moderate flares with low grade persistent discomfort for 5-6 weeks followed by
infrequent mild flares; Not taken any NSAID/analgesic/local therapy in the last 8 weeks or so; NO AXIAL
PAINS
PATHOPHYSIOLOGY: Very Focal; tenosynovitis, arthralgia/arthritis (minimal overt synovitis), ?osteitis, ?
neuropathic (acute phase)

Acute CHIKUNGUNYA-My Family Story• Wife- onset next day; Fever (2 days), severe MSK pains, reduced in
time but continues moderately severe• No definite arthritis but lower limb pains (standing) and RA like hands (?CTS)
• Response to steroids begun 3 weeks late till date: FAIR
• In-lwas- one week later, dominantly lower limb much settled after 2 weeks of
illness; mother in law gets frequent ankle lower limb pain & stiffness
• Son- 3 weeks later- typical episode mostly in knees but not yet pain free
• All had similar blood profile to me: PCR +, IgM +, negative for dengue

ACUTE CHIKUNGUNYA• Complete resolution is equally dramatic
• Within 2-5 days, fever settles down
• Thereafter, pain and stiffness rapidly settle down
• ??The majority recover completely within 10 days
• ??About 10% go on to develop chronic inflammatory
arthritis

CHIKUNGUNYA-SEQUEL & ATYPICAL FEATURES (described in literature post 2006 epidemic: case series, case reports, retrospectvive, tertiary center)• Gastrointestinal 21%- diarrhea, vomiting, hepatitis
• Neurological 12%- encephalitis, meningo-encephalitis
• Cardiac 5%- myopericariditis, pericarditis
• Mortality 0.1%- elderly and with comorbidity
• Maternal-neonatal viral transmission-3/1000 live births
• 50%–75% of CHIKV-infected adults had joint aches and pains
and ?arthralgia/arthritis 1 year after infection

Chopra Arvind et al. Chikungunya Virus Aches And Pains: An Emerging Challenge.Arthritis & Rheumatism 2008, 58(9): 2921 – 2922
METHODS
Retrospective analysis of clinical cases July-Dec 2006
Community based large referral practice (CRD, Pune, India)
156 patients with Post Chikv persistent arthritis (MSK)
95 patients (45 women) naïve for MSK or rheumatic disorder
61 patients had pre-existing MSK or rheumatic disorder
Anti-CHIKV IgM antibodies tested by MAC ELISA at NIV, Pune
70 % seropositive (two third tested within 12 weeks onset illness)

Chopra A et al. Arthritis & Rheumatism 2008, 58(9): 2921 - 2922
POST CHIKUNGUNYA RHEUMATIC DISORDER (naïve patients): CLASSIFICATION (percent shown)

Can lead to a wide SPECTRUM OF RHEUMATIC DISORDERS
NO OTHER VIRUS SEEMS TO HAVE SUCH PROPENSITY
Arthritis can be disabling, chronic & difficult to treat
NEEDS EARLY RHEUMATOLOGIC CARE RESEARCH AGENDA
WHAT IS THE ETIOPATHOGENETIC LINK BETWEEN CHIKV & RMSK?
HOW DOES CHIKY BEHAVE IN A COMMUNITY?
WILL CHIKV EPIDEMIC LEAD TO HIGHER INCIDENCE OF ARTHRITIS
POST CHIKV ARTHRITIS & RHEUMATISM (MSK)
Chopra A et al. Arthritis & Rheumatism 2008, 58(9): 2921 - 2922

Arthritis Rheum 2011

How many patients in a
community who suffer from acute
CHIKV eventually develop chronic
RMSK/ arthritis?
POST CHIKV RHEUMATISM: CONCLUSIONRESEARCH AGENDA

A Rural Population Based Study Of Chikungunya (CHIKV) Infection With Special
Reference To Persistent ‘Rheumatic Musculoskeletal Disorders (RMSK)’
Principle Investigator: Dr Arvind Chopra, MDCo-Investigator: Ms Anuradha V, MSc, PhD
CENTER FOR RHEUMATIC DISEASES, PUNE(CHIKV-ICMR PROJECT 05/8/7/20/2006-ECD-I, sponsored by Indian Council of Medical Research,
Government of India)


SURVEY
BAVI CHIKV PROJECT 2006-2008: CLASSIFICATION BREAK UP
1 YEAR FOLLOW-UP
IA: Inflammatory Arthritis; NSA: Non Specific Arthralgia; STR: Soft Tissue Rheumatism; OA: Osteoarthritis
Chopra Arvind et al. Epidemiol Infect 2011

Almost one third cases continued to suffer rheumatic pains, mostly non specific, beyond one month. In 1.6% population, it persisted at two years and the profile was clinically benign.
BAVI RURAL SURVEY 2006 & FOLLOW UP: CLINICAL CHIKV Proportion (percent) of patients with persistent RMSK pains following the
onset of CHIKV.
Chopra Arvind et al. Epidemiol Infect 2011

Hoarau J-J, Jaffar Bandjee M-C, Krejbich Trotot P, Das T, Li-Pat-Yuen G, Dassa B, et al. Persistent chronic inflammation and infection by chikungunya arthritogenic alphavirus in spite of a robust host immune response. J Immunol 2010;184:5914–27.
• Using conventional flow cytometry during acute CHIKV infection, one prior
study documented T cell activation that resolved 6 months after infection
• CHIKV has not been cultured from synovial fluid, but viral RNA can be
detected in the synovium, suggesting that CHIKV may directly invade and
persist within joints

Management• Acute phase: Symptomatic & supportive
• Identify risk factors and threatening co-morbidity
• Early Post Chikv rheumatism: NSAIDs, intermittent
steroids, ?DMARD
• Late Post Chikv arthritis: NSAIDs, Steroids, DMARD
• Prevention is the best policy (…but failing in current times)
• Mosquito targeted
• Vaccine

• CHIKUNGUNYA Management Algorithm II/II (Javelie et al. PloS Neglected Tropical Dis 2015)

Suhrbier A, Mahalingam S. The immunobiology of viral arthritides. Pharmacol Ther 2009;124:301–8.
• there is no good evidence to support the
notion that viral arthritides lead to
autoimmune disease

Andreas Suhrbier, Suresh Mahalingam. The immunobiology of viral arthritides. Pharmacology & Therapeutics 124 (2009) 301–308
Key elements in the development of alphavirus arthritis. A mouse model suggests Bindarit a potential new treatment. Bindarit did not affect viremia and so MCP 1 may not have any anti viral effect .

*Proinflammatory molecule **membrane receptor binds to MIF


CONCLUSIONS
In this first ever community based evaluation, chloroquine was not
superior to meloxicam in the prolonged symptomatic treatment of
persistent MSK-P and polyarthralgias of more than 4 weeks
duration following CHIKV illness.
Both the treatment groups improved significantly
14 patients (44%) and 15 patients (40%) in the meloxicam and
chloroquin groups respectively became asymptomatic on
completion at week 24

Chronic Chikungunya Arthritis Management: Selected Indian Data
• Pandya S et al, Ahmedabad – Controlled favouring RA like approach to DMARD
• Ganu et al, Latur – Case series favouring RA like approach to DMARD
• Ravindran Vinod & Alias George, Kerala
– 72 patients with persistent arthritis > 1 year post illness randomized 2
arms/6 mths duration/ Combo (MTX+SZP+HCQS) versus Mono (HCQS)/ all
recd pred upto 7.5 mg daily for initial 6 weeks; Significant DAS 28 response
with Combo (Cl Rheumatol 2016)

• 147 patients, median lapse post onset 8 mths
• 13% epidemic influenced Chikv ?EXCLUDED
• Remaining Patterns:
• Reactivation Pain Mechancical=32%
• Fibromyalgia=6.1%
• Axial SpA Flare=31%
• De-novo Inf Polyarthritis= 18.4%
• Methotrexate up to 25 mg/ wk
• Anti TNF in 13 resistant cases


• Patient received Rituximab 1 gm injection on 19/05/2015
JCPT JCSW PAIN VAS(10 cm scale)
CRD PUNE VERSION HAQ SCORE
ESR(mm at the end of 1st hour)
1/09/2015 0 0 3 1 48
16/10/2015 4 2 0.5 0 13


This may be the basis of current DMARD/Biologic therapy for chronic chikv arthritis

Cytokine / Chemokine
Anuradha V et al2014
(HC=80)
Ng et al 2009
(HC=9)
Kelvin et al 2011
(HC=10)
Chaaithanya et al 2011
(HC=6)
El-Gabalawy et al 2012 (HC=200)
Acute(n=23)
Subacute (n=22)
Extended Symptomatic
(n=65)
2-19 days
(n=10)
Acute (n=35)
Acute (n=6)
RA (n=105)
IFN-α 8.9 3.6 3.0 1.5 ND ND 2.8IFN- 8.4 3.5 2.9 ND ND ND NDIFN- 50.1 17.2 15.8 + 0.9 ND 2.7
CXCL-10/IP-10 26.9 23.3 25.0 1000 2.3 33.9 1.2
IL1- 2.3 1.7 1.7 + 0.82 ND 4.9TNF- 4.4 4.6 5.2 + 1.5 ND 3.7MCP-1 49.0 37.9 33.2 ND ND 1.9 1.1
IL-4 108.7 392.6 170.5 + 0.07 ND 6.5IL-6 3.8 7.0 7.5 4.0 2.0 196.7 9.3
IL-10 6.4 23.1 38.5 1.5 0.4 1.9 3.3IL-13 3.3 2.5 3.2 + ND ND 10
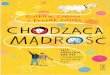
Comparison of the cytokine profile in CHIKV cases with healthy controls in different studies reported. [Values expressed as ratio of medians of cases to controls].
Anuradha V, R Ghorpade, Chopra A. PLoS ONE 2014, 9(10): e111305.
HC= Healthy controls; ND=Not Done; + = Higher than Healthy controls;


Case 4: MSR, 57 year woman….cont 3• Onset 2006; typical acute illness with partial relief
• Persistent polyarthralgias, episodic flares with few swollen joints
• Several DMARD regimens, intermittent steroids
• Bilateral total hip replacement in 2009
• Referral 15 April 2013; severe knees & shoulders arthritis; in wheelchair
• ESR 55 mm, CRP 20 mg/dl, Hb 11.6 gm/dl, detail biochemistry normal
• Seronegative for RF, a-CCP and ANA
• Seropositive for specific anti-CHICK IgM & IgG
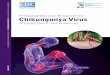
• Bilateral knee replacement in May 2013Chikungunya

MSR, 57 year woman with Chikungunya Arthritis (onset 2006)
Xrays taken in April 2013
Chikungunya

CD3 – Focal Lymphoid cells Positive
MPO- Granulocytes Positive
CD-20 Scattered occasional cells positive
CD5 – Focal aggregates of Lymphoid cells
CD21 – Few Scattered Lymphocytes positive
CD23 -Negative
IMMUNOHISTOCHEMISTRY - SYNOVIAL BIOPSY : (MR F/57 yrs) Post CHIK – Persistent
CHIKV IgM and IgG Neg; RF Neg; Anti CCP Neg

GUESTS LIVE IN THE BACKYARD

Mosquito Control is the key issue:
Swach Bharat

Viral arthritis : chikungunya and
beyond Believe me. We have not seen the last of Chikungunya and neither the fury of Zika or even Dengue which kills people
Viruses and Microbes are amongst the earliest creation and are ubiquitous. They are more of a host to this World than
us. We live at their mercy.
And I know that for sure. Thank you Chikungunya! I know your might but leave me
alone now

IS THERE A DISTINCT ENTITY OF POST CHIKV RHEUMATISM ?
• ?Seronegative Inflammatory Arthritis
• Virus persistence
• ?pauci-immune cytokine driven inflammation
• ?erosive arthritis
• Probably somewhere On The RA-SSA Axis
• No Specific Drugs Yet though use of DMARDs empirical
• Steroids effective
• Long Term Follow Up Required

Chikv versus Dengue
• Absolute clinical differentiation is difficult• All patients with acute onset will need to be
tested for dengue also or at least blood cell counts during the first week of illness
• Risk factors of severe dengue complications-NSAID use, elderly age, other co-morbdity
• Diligent watch during first 10 days

DISCLOSURES• No conflict of interest• Funding
– Indian Council of Medical Research, Govt of India Project
– Arthritis Research Care Foundation- Center for Rheumatic Diseases, Pune

ZIKA IS STARING AT US…………….• Close cousin of dengue and chikungunya
• Acute exanthematous infection
• Neurological complications- GBS ?autoimmune disorder
• Pregnancy and microcephaly
• uveitis


• CHIKV is a global disease
• Currently it seems to be a rheumatological
nightmare

CHIKV: MCQ 2The current evidence suggests that treatment for post chikungunya arthritis A. Symptomatic pain relief plus NSAID for all forms of
arthritisB. Steroids + NSAIDs for all forms of arthritisC. Methotrexate plus chloroquine for arthritis > 6
weeks post acute phaseD. Empirical treatment based on clinical phenotype
and duration lapsed since onset