Embed Size (px)
Citation preview
Page 0March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
American Health Lawyers AssociationInstitute on Medicare and Medicaid Payment Issues
March 25-27, 2015
ICD-10 Transition Update:
What Health Lawyers Need to Know
Page 1March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
• What is ICD‐10 and why is it important to the healthcare community?
• What is the current regulatory status of ICD‐10?
• Organizational Impact –Operational and Finance
• ICD-10 Value in the World of New Payment Models (Value-Based Purchasing and Population Health)
Learning Objectives
Page 2March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
What is ICD‐10 and Why Is It
Important to the Healthcare
Community?
Page 3March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
What Are ICD Codes?
• The International Classification of Disease (ICD) codes are the
international classifications for all diseases and many other health
problems for purposes of health management, including:
– Analysis of the general health of population groups
– Monitoring of the incidence and prevalence of diseases
– Monitoring other health problems in relation to other variables such as the
characteristics and circumstances of the individuals affected, reimbursement,
resource allocation, and quality http://www.who.int/classifications/icd/en/
• ICD codes are now a key component in reimbursement, quality and
utilization review and other data management activities
Page 4March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
• Replaces ICD-9 – Not a revised version of ICD-9
• ICD-10 represents a complete change from one
coding system to a new one structured in an
entirely new way
• Like all medical coding systems, it provides a way
to condense textual clinical information into “codes”
that can be used for billing and other data-based
applications
What is ICD-10?
Page 5March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
There is no relationship between the two code sets –
they have completely different structures and uses.
ICD-10 Is Really
Two Different Code Sets
ICD-10-CM
• International
Classification of
Diseases, 10th
Revision, Clinical
Modification
ICD-10-PCS
• International
Classification of
Diseases, 10th
Revision, Procedure
Coding System
Page 6March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
What’s ICD-10-CM?
ICD-10-CM• Diagnosis Coding System – Used to report the patient’s
condition (i.e., what’s wrong with the patient)
• Direct replacement for ICD-9-CM Volumes 1 & 2
• Will be used in all settings – hospital inpatient, hospital
outpatient, physician office, etc.
• Like ICD-9-CM, developed and maintained by the World
Health Organization (WHO) and the National Center for Health
Statistics within the Centers for Disease Control
Page 7March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
What’s ICD-10-PCS?
ICD-10-PCS
• Procedure Coding System – Used to report surgical
procedures performed
• Direct replacement for ICD-9-CM Volume 3
• Only used in a hospital inpatient setting (and only for
reporting facility services)
• Like ICD-9-CM Volume 3, ICD-10-PCS was developed
and is maintained by CMS
Page 8March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
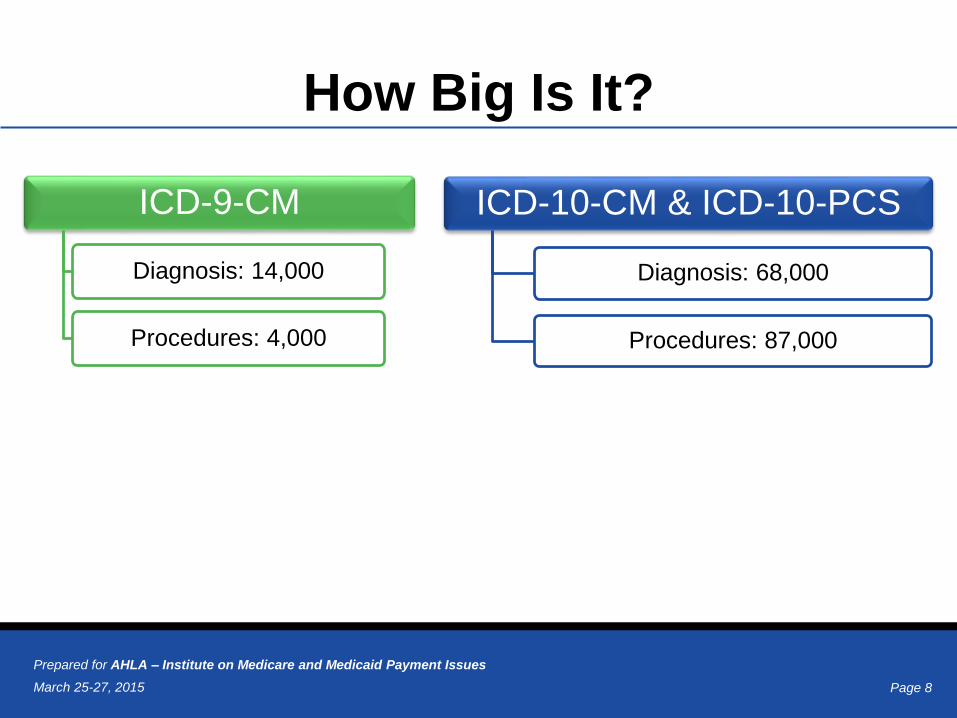
How Big Is It?
ICD-9-CM
Diagnosis: 14,000
Procedures: 4,000
ICD-10-CM & ICD-10-PCS
Diagnosis: 68,000
Procedures: 87,000
Page 9March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Key ICD-10-CM Changes
• Alphanumeric codes
• Expanded injury codes – grouped by anatomic site not injury type
• Laterality (right vs. left)
• Obstetric codes include trimester
• Diabetes codes differentiate between I, II, drug, chemical induced diabetes, or due to an underlying condition (chemotherapy)
• Intraoperative and postoperative complications
• Visits – initial or subsequent
Page 10March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
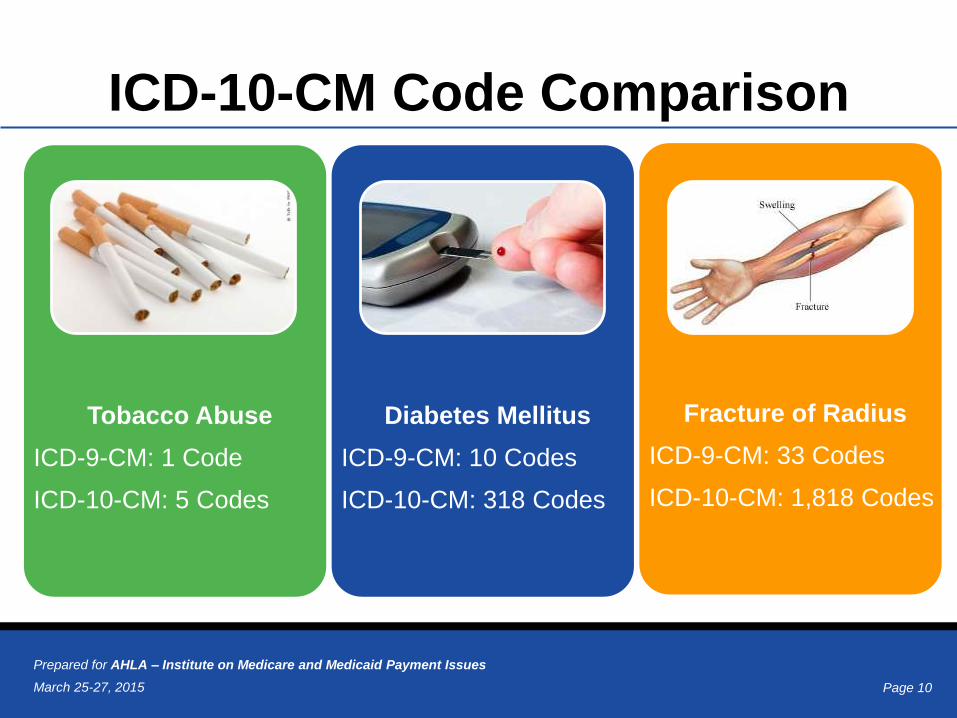
ICD-10-CM Code Comparison
Tobacco Abuse
ICD-9-CM: 1 Code
ICD-10-CM: 5 Codes
Diabetes Mellitus
ICD-9-CM: 10 Codes
ICD-10-CM: 318 Codes
Fracture of Radius
ICD-9-CM: 33 Codes
ICD-10-CM: 1,818 Codes
Page 11March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
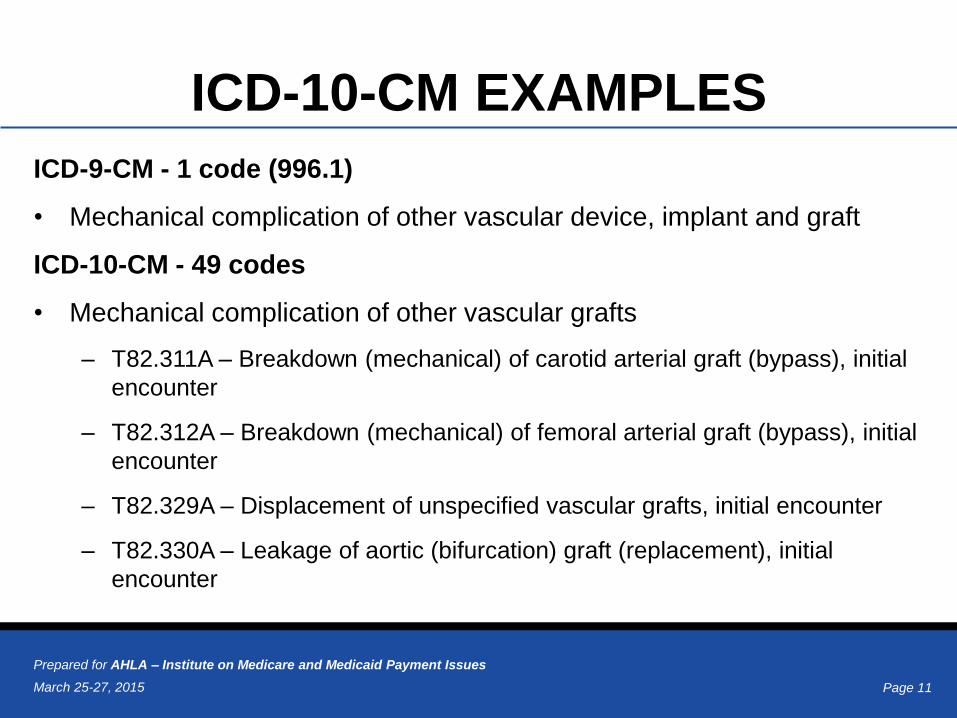
ICD-10-CM EXAMPLES
ICD-9-CM - 1 code (996.1)
• Mechanical complication of other vascular device, implant and graft
ICD-10-CM - 49 codes
• Mechanical complication of other vascular grafts
– T82.311A – Breakdown (mechanical) of carotid arterial graft (bypass), initial
encounter
– T82.312A – Breakdown (mechanical) of femoral arterial graft (bypass), initial
encounter
– T82.329A – Displacement of unspecified vascular grafts, initial encounter
– T82.330A – Leakage of aortic (bifurcation) graft (replacement), initial
encounter
Page 12March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
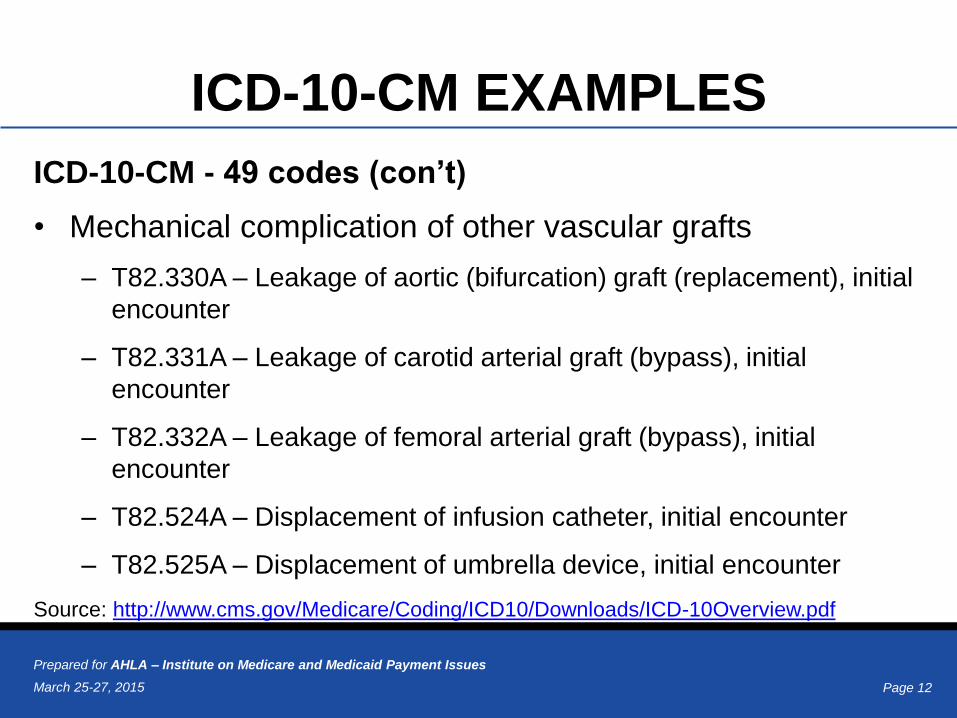
ICD-10-CM EXAMPLES
ICD-10-CM - 49 codes (con’t)
• Mechanical complication of other vascular grafts
– T82.330A – Leakage of aortic (bifurcation) graft (replacement), initial
encounter
– T82.331A – Leakage of carotid arterial graft (bypass), initial
encounter
– T82.332A – Leakage of femoral arterial graft (bypass), initial
encounter
– T82.524A – Displacement of infusion catheter, initial encounter
– T82.525A – Displacement of umbrella device, initial encounter
Source: http://www.cms.gov/Medicare/Coding/ICD10/Downloads/ICD-10Overview.pdf
Page 13March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
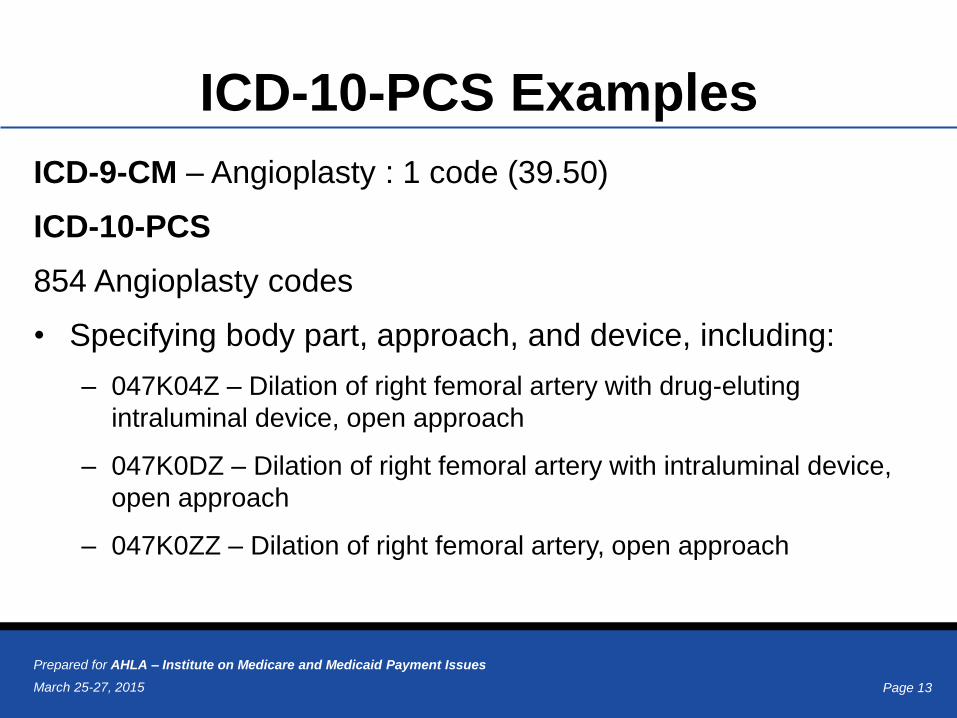
ICD-10-PCS Examples
ICD-9-CM – Angioplasty : 1 code (39.50)
ICD-10-PCS
854 Angioplasty codes
• Specifying body part, approach, and device, including:
– 047K04Z – Dilation of right femoral artery with drug-eluting
intraluminal device, open approach
– 047K0DZ – Dilation of right femoral artery with intraluminal device,
open approach
– 047K0ZZ – Dilation of right femoral artery, open approach
Page 14March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
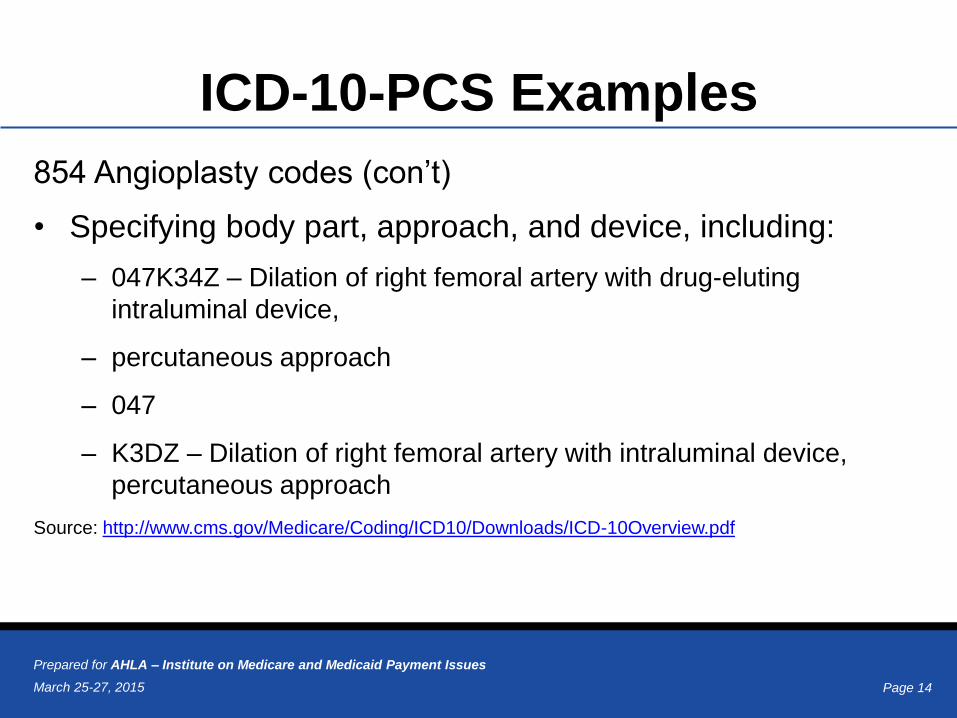
ICD-10-PCS Examples
854 Angioplasty codes (con’t)
• Specifying body part, approach, and device, including:
– 047K34Z – Dilation of right femoral artery with drug-eluting
intraluminal device,
– percutaneous approach
– 047
– K3DZ – Dilation of right femoral artery with intraluminal device,
percutaneous approach
Source: http://www.cms.gov/Medicare/Coding/ICD10/Downloads/ICD-10Overview.pdf
Page 15March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
What are the benefits of ICD-10?The new, up-to-date classification system will provide much better data needed to:
• Measure the quality, safety, and efficacy of care
• Improved quality reporting and scoring
• Reduce the need for additional documentation to explain the patient’s condition
• Design payment systems and process claims for reimbursement
• Conduct research, epidemiological studies, and clinical trials
• Set health policy
• Support operational and strategic planning
• Design healthcare delivery systems
• Monitor resource utilization
• Improve clinical, financial, and administrative performance
• Prevent and detect healthcare fraud and abuse
• Track public health and risks
Page 16March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
What Can We Learn From Other
Countries’ Implementation?• Yesterday’s Advice
– Start now to allow time to understand the impact and come up with solutions
• Today’s Advice
– Prioritize necessary activities
• Education and training are all important
– Prepare for productivity loss and longer turn around times
• Collaborate with others
– Share information and experiences to learn what works and what to avoid
Page 17March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
What is the Current Regulatory
Status of ICD‐10?
Page 18March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
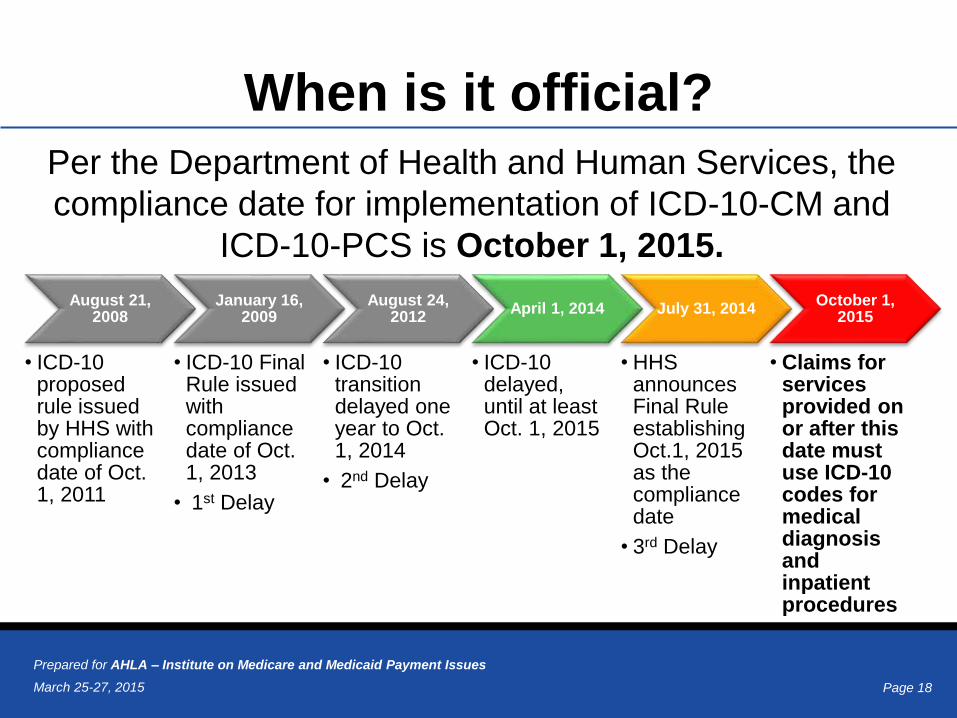
When is it official?
August 21, 2008
• ICD-10 proposed rule issued by HHS with compliance date of Oct. 1, 2011
January 16, 2009
• ICD-10 Final Rule issued with compliance date of Oct. 1, 2013
• 1st Delay
August 24, 2012
• ICD-10 transition delayed one year to Oct. 1, 2014
• 2nd Delay
April 1, 2014
• ICD-10 delayed, until at least Oct. 1, 2015
July 31, 2014
• HHS announces Final Rule establishing Oct.1, 2015 as the compliance date
• 3rd Delay
October 1, 2015
• Claims for services provided on or after this date must use ICD-10 codes for medical diagnosis and inpatient procedures
Per the Department of Health and Human Services, the
compliance date for implementation of ICD-10-CM and
ICD-10-PCS is October 1, 2015.
Page 19March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
ICD-10 Readiness:
For Real This Time?
Concern regarding physician burden last year
• Increased number and complexity of codes
• Costs for software, EHR upgrades, etc.
• Costs of training, physicians, coders, other staff
• Increased time required for more detailed documentation
CMS readiness last year
• Lack of sufficient end-to-end testing prior to Oct. 1, 2014
deadline
Page 20March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
ICD-10 Readiness Testimony
During the February 11, 2015, U.S. House Energy & Commerce Committee,
Subcommittee on Health – Testimony on feasibility of ICD-10 Transition by
Oct. 1:
• Dr. Edwin Burke (Small Practice Physician in Missouri) said: “…Delaying
ICD-10 is not blinking but closing our eyes.”
• Sue Bowman, AHIMA stated: “We have had 6 years to prepare and a
delay will only prolong readiness”
• Kristi Matus, CFO, CAO, Athena Health stated: “Pull the trigger or pull the
plug”
• Dr. John Hughes, Yale School of Medicine stated: “I have been frustrated
many times at ICD-9’s inability to specify the exact nature of a
complication, its extent, its location and how it was treated.”
Source: http://www.healthcare-informatics.com/article/icd-10-debated-capitol-hill-most-favor-2015-implementation
Page 21March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
ICD-10 Readiness Testimony
• Dr. William Terry, American
Urologic Association cited an
AMA study that costs would be up
to $250,000 for some small
practices.
• Robert Averill, Director of Public
Policy – 3M, stated that costs to
small practices will be
approximately $8,000 on
average. “ICD-9 was
implemented when you could still
smoke in a room with the patient!”
Page 22March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Physician Burden:
Fact vs. Fiction
• American Medical Association – Nachimson Study
– 2008: predicted cost to implement ICD-10 ranged from $83,290 for a
small practice, $285,195 for a medium practice and $2,728,780 for a
large practice.
– 2014: study revisited and new information identified the following cost
ranges for each practice size based on variable factors such as
specialty, vendor and software:
Small practice: $56,639 - $226,105
Medium practice: $213,364 - $824,735
Large practice: $2,017,151 - $8,018,364
Source: http://www.ama-assn.org/ama/pub/news/news/2014/2014-02-12-icd10-cost-estimates-increased-for-
most-physicians.page
Page 23March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Physician Burden:
Fact vs. Fiction
• Professional Association of Health Care Office
Management (PAHCOM)
– Surveyed 276 physician practices of fewer than 6
providers
– Asked to specify number of providers in the practice
(including PA, NP, RN’s)
– Asked for total expenditures for all ICD-10 related
activities
– ICD-10 manuals, training, superbill conversion, software
upgrades, testing, etc.
Page 24March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Physician Burden:
Fact vs. Fiction
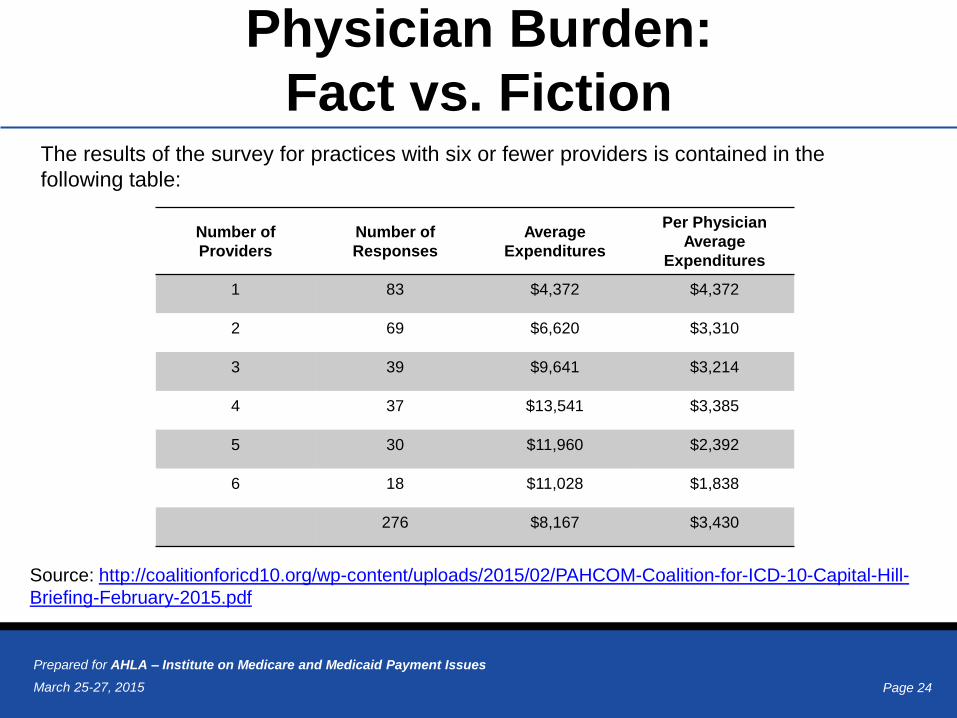
Source: http://coalitionforicd10.org/wp-content/uploads/2015/02/PAHCOM-Coalition-for-ICD-10-Capital-Hill-
Briefing-February-2015.pdf
Number of
Providers
Number of
Responses
Average
Expenditures
Per Physician
Average
Expenditures
1 83 $4,372 $4,372
2 69 $6,620 $3,310
3 39 $9,641 $3,214
4 37 $13,541 $3,385
5 30 $11,960 $2,392
6 18 $11,028 $1,838
276 $8,167 $3,430
The results of the survey for practices with six or fewer providers is contained in the
following table:
Page 25March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Factors Cited for Reduced Costs
• Free resources developed and provided by
CMS for small practices
• Vendors providing support and upgrades at
little to no cost
• Free support and resources from physician
medical societies
• Length of time preparing for ICD-10
Page 26March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Why It’s More Likely
This Time Around
AAPC Survey, ICD-10 Testing Survey - January 2015
• 2,000 Certified Professional Coders responded to AAPC Survey on ICD-
10 Readiness Testing – CMS and Commercial Payers
• 84% had participated in ICD-10 testing and considered it a success
• 72% saw no claims denied during testing
• 16% experienced a rejection rate of less than 10%
• 90% saw no payment shift on test claims
• 1 in 3 respondents performed testing with Medicare or Medicaid
Source: http://icd10monitor.com/enews/item/1349-aapc-icd-10-testing-considered-successful
Page 27March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Why It’s More Likely
This Time Around (con’t)
AAPC Survey - Cost of Implementation
• 72% reported cost of less than $5,000 per provider
• 2% reported their practice either spent nothing or
more than $10,000 per provider
• AAPC Cost Estimate $750 - $3,500 per provider
Source: http://icd10monitor.com/enews/item/1349-aapc-icd-10-testing-considered-successful
Page 28March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Why It’s More Likely
This Time Around (con’t)
• Beyer states “What we were unprepared for was
how seamless it was…”
• “…No special training, did not spend additional
money in preparation, did not see less patients…”
• “…It was not frustrating or scary. It just ‘was’…”
• Attributed success to Software and Electronic
Health Records
Source: http://energycommerce.house.gov/hearing/examining-icd-10-implementation
Page 29March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
ICD-10 Impact
Page 30March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
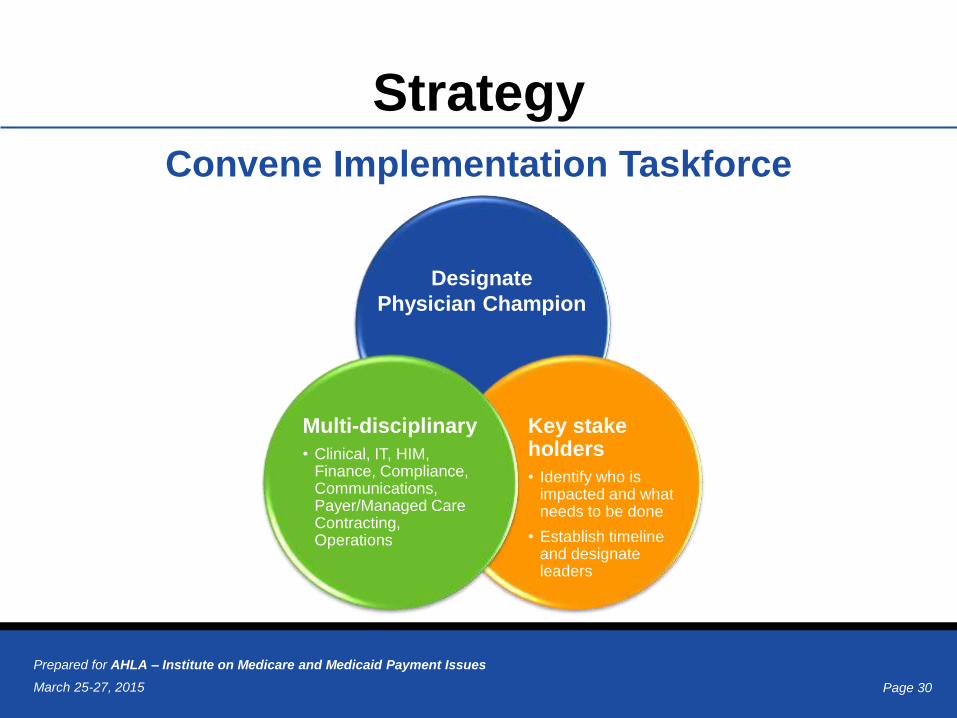
Strategy
Convene Implementation Taskforce
Multi-disciplinary
• Clinical, IT, HIM, Finance, Compliance, Communications, Payer/Managed Care Contracting, Operations
Key stake holders
• Identify who is impacted and what needs to be done
• Establish timeline and designate leaders
Designate
Physician Champion
Page 31March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Assessment
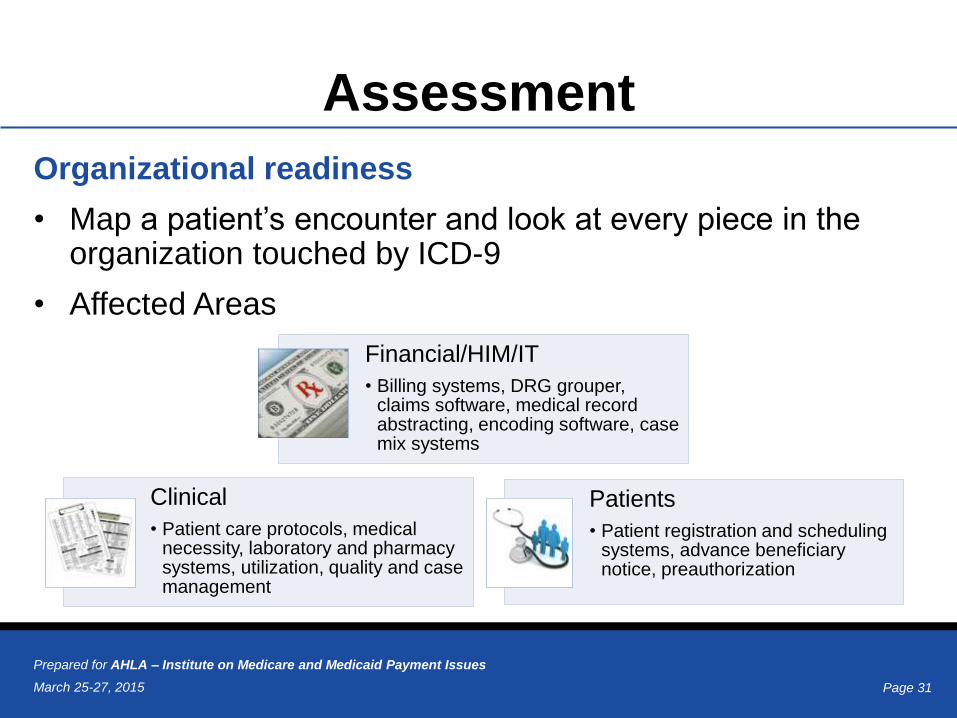
Organizational readiness
• Map a patient’s encounter and look at every piece in the organization touched by ICD-9
• Affected Areas
Financial/HIM/IT
• Billing systems, DRG grouper, claims software, medical record abstracting, encoding software, case mix systems
Clinical
• Patient care protocols, medical necessity, laboratory and pharmacy systems, utilization, quality and case management
Patients
• Patient registration and scheduling systems, advance beneficiary notice, preauthorization
Page 32March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
BudgetHow much emergency cash should providers keep in case of cash flow disruption?
• Review what happened to your organization with HIPAA 5010--this would be a good baseline; with the transition from ICD-10 there will be delays in reimbursement
• Vendors and clearinghouses have been working hard, but we will not know the true effects until Oct 1, 2015
• It is recommended that you have up to several months' cash reserves or access to cash through a loan or line of credit to avoid potential headaches
• The amount of reserves you need to set aside will be impacted by the preparation work you do for ICD-10
• Will need to cover at a minimum practice operation expenses for three to six months:
– Medical supplies
– Payroll
– Rent
Page 33March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Implementation Process
Processes Reports Work Flow Information
Systems and Software
All Forms of Documentation
Analysis of all Departments
Page 34March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Vendor Readiness
• Identify vendors affected by ICD-10 (billing companies,
medical transcription, home health, DME – start with
your Business Associate Agreements)
− What system changes/upgrades are needed?
− What costs are involved? Are they included in existing
vendor agreements?
− What customer support (implementation, testing, training)
will the vendor be offering?
Page 35March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
ICD-10 & EHR • Analyze EHR for functionality and compliance
• Review templates, interfaces, default documentation, and level of detail
• Can the system accommodate the data format changes for ICD-10?
• What is the EHR vendor’s timeline for the transition? When will its upgrades be available for installation? Make sure that installation of upgrades is far enough in advance to facilitate early testing
• Will there be additional costs for the upgrade? Will multiple upgrades be required? Is there a waiting list?
• Is the EHR vendor training its staff on ICD-10 system upgrades?
• Can it ensure that the right components are in place to select the more specific code?
• Will it have specialty specific codes?
• Will ICD-9 still be available for use and comparison?
• Does the system allow for dual coding?
Page 36March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Payer Readiness• As with vendors – establish dedicated contact
• Evaluate payer readiness
– What’s their implementation plan/timeline?
– Are they implementing new rules for claims submission or re-submission?
– Will contract terms for coverage and billing change? Will they require the provider to report the code with the highest specificity?
– Will their payment and reimbursement schedules change?
– Will the claims appeal process change?
• Add language to current contracts to require ICD-10 compliance
• Share your plans for ICD-10 changes with them
• Establish regular meetings, compare implementation plans, review and update contracts as necessary
• Medicare and Medicaid - Are they on track? When will they be ready for end-to-end testing? What are their contingency plans?
Page 37March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Low Cost Opportunities
• CMS offers “free billing
software” via its MAC
websites.
• Software requires an
internet connection and
only works for FFS
Claims to Medicare.
• Does not provide coding
assistance, but will
facilitate claim
submission.Source: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-
Network-MLN/MLNMattersArticles/Downloads/se1409.pdf
Page 38March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
There’s An App For That!
Page 39March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
• Plan for dual ICD-9 and 10 codes for a brief period to address services rendered before October 1, but discharged after October 1
• Monitor physician documentation to ensure ICD-10 compliance
• Monitor impact on claim-processing activity, claim denials, and rejections
• Audit coder productivity and accuracy
• Monitor patient satisfaction
• Post-transition Review
– What’s working?
– What needs fixing?
• Schedule 30-day post-conversion claims assessment
ICD-10 Go Live, The Day After…
Page 40March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Value in a New Payment World
Page 41March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
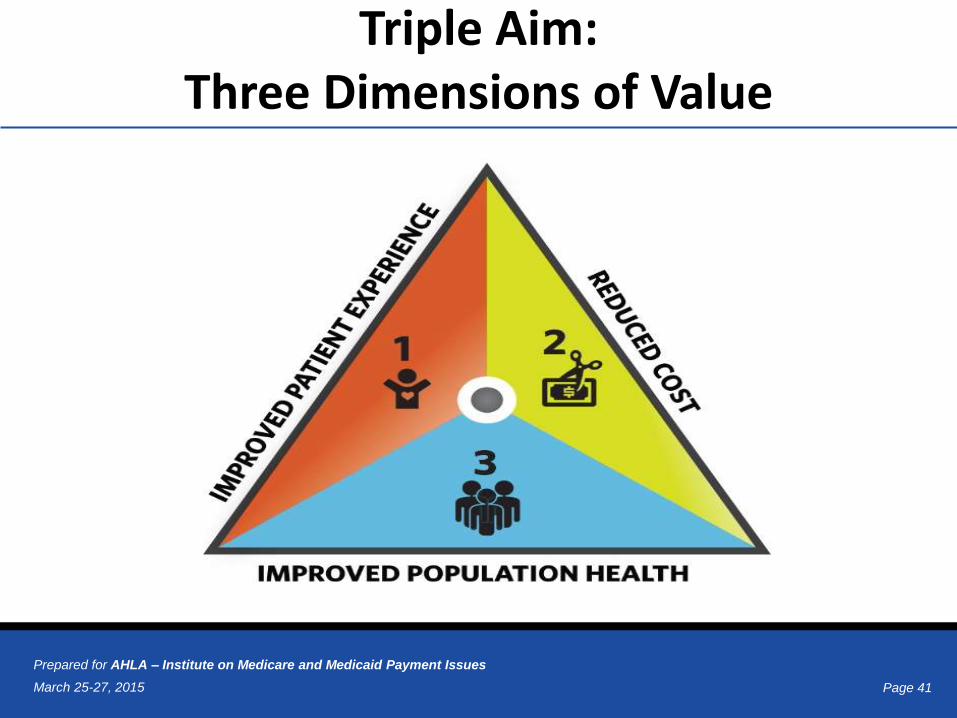
Triple Aim:Three Dimensions of Value
Page 42March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Physician Feedback/Value-Based
Payment Modifier Program
• “[S]upports the transformation of Medicare
from a passive payer to an active purchaser
of higher quality, more efficient health care”
• Four interrelated parts
– PQRS
– Physician Compare
– Value Modifier
– QRUR
Page 43March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Quality vs. Quantity
• Value-based compensation
• Healthcare is shifting from FFS model to pay-
for-performance methods
• Payers will reward value and care
coordination- rather than volume and
duplication
• HHS testing and expanding new healthcare
payment models
Page 44March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
HHS Framework
Payment Models:
• Category 1: FFS no link to quality
• Category 2: FFS with quality link
• Category 3: Alternative Payment Models built
on FFS architecture
• Category 4: Population Based PaymentSource: http://www.hhs.gov/news/press/2015pres/01/20150126a.html
Page 45March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Value-Based Payment
Two Shifts
1. Increasing accountability for quality and total cost of care
2. Timeline:
1. 30% of Medicare payments in alternative payment models
(categories 3 & 4) by the end of 2016
2. 50% of Medicare payments in alternative payment models
(categories 3 & 4) by the end of 2018
3. Overall, 85% of payments in categories 2 through 4 by 2016 and
90% by 2018
Page 46March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Value-Based Purchasing
and ICD-10 Coding
Patient Safety Indicator 15 – Accidental Puncture or Laceration Rate
ICD-9-CM
• 998.2 Accidental puncture or laceration during a procedure, not
elsewhere classified
ICD-10-CM (Classified by affected body part)
• D78.11 Accidental puncture and laceration of the spleen during a
procedure on the spleen
• D78.12 Accidental puncture and laceration of the spleen during other
procedure
• E36.11 Accidental puncture and laceration of an endocrine system organ
or structure during an endocrine system procedure
• E36.12 Accidental puncture and laceration of an endocrine system
organ or structure during other procedure
Page 47March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Value-Based Purchasing and
ICD-10 Coding and Documentation
Patient Safety Indicator 11 – Postoperative Respiratory Failure Rate
ICD-9-CM
• 96.04 Insertion of endotracheal tube
ICD-10-CM
• 0BH17EZ Insertion of Endotracheal Airway
into Trachea, Via Natural or Artificial Opening
• 0BH18EZ Insertion of Endotracheal Airway
into Trachea, Via Natural or Artificial Opening
Endoscopic
Page 48March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Value-Based Purchasing and
ICD-10 Coding and Documentation
Patient Safety Indicator 11 – Postoperative Respiratory Failure Rate
ICD-9-CM
• 96.70 Continuous invasive mechanical ventilation of unspecified
duration
• 96.71 Continuous invasive mechanical ventilation for less than 96
consecutive hours
• 96.72 Continuous invasive mechanical ventilation for 96 consecutive
hours or more
ICD-10-CM
• 5A1935Z Respiratory Ventilation, Less than 24 Consecutive Hours
• 5A1945Z Respiratory Ventilation, 24-96 Consecutive Hours
• 5A1955Z Respiratory Ventilation, Greater than 96 Consecutive Hours
Page 49March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Physician Office ICD-10
HCC Coding and Documentation
The patient presented for follow-up of labs. The physician office note
documents patient presented with diabetes mellitus type 2 with diabetic
nephropathy, diabetes mellitus type 2 with diabetic polyneuropathy, diabetes
mellitus type 2 with angiopathy.
In ICD-9-CM:
• 250.40 Diabetes mellitus with renal manifestations, type II or unspecified
type, not stated as uncontrolled
– V21 HCC 15; V22 HCC 18
• 583.81 Nephritis and nephropathy in diseases classified elsewhere
(manifestation)
– V21 HCC 132; V22 HCC 0
Page 50March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Physician Office ICD-10
HCC Coding and Documentation
• 250.60 Diabetes mellitus with neurologic manifestations, type II or
unspecified type, not stated as uncontrolled
– V21 HCC 16; V22 HCC 18
• 357.2 Polyneuropathy in diabetes (manifestation)
– V21 HCC 71; 2014 HCC 18
• 250.70 Diabetes mellitus with peripheral circulatory disorder, type II or
unspecified type, not stated as uncontrolled
– V21 HCC 15; V22 HCC 18
• 443.81 Peripheral angiopathy in diseases classified elsewhere
(manifestation)
– V21 HCC 105; V22 HCC 108
Page 51March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
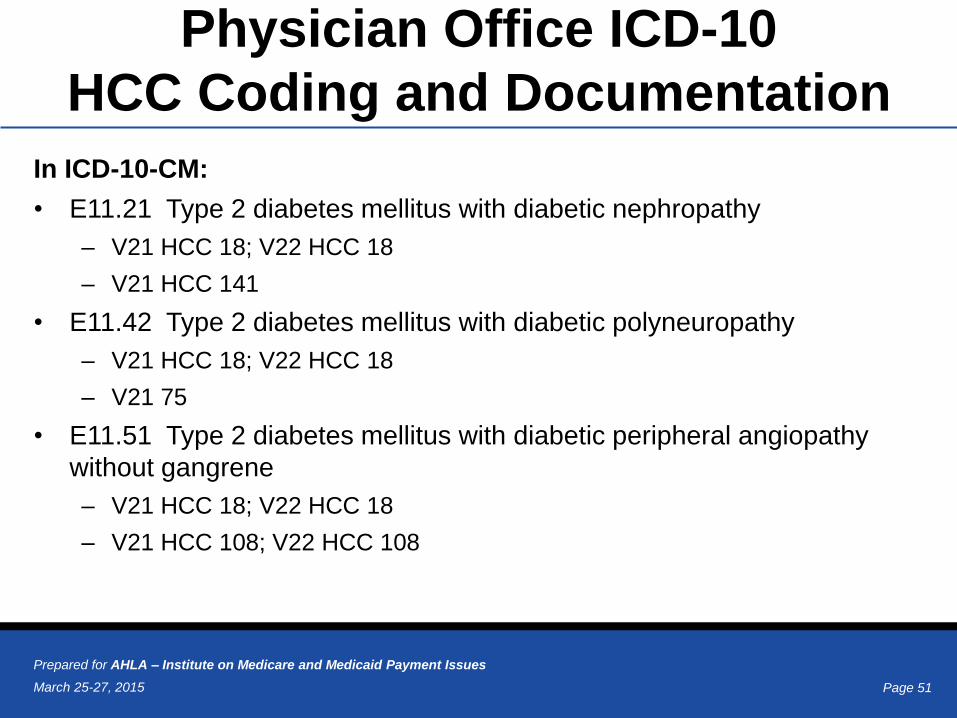
Physician Office ICD-10
HCC Coding and Documentation
In ICD-10-CM:
• E11.21 Type 2 diabetes mellitus with diabetic nephropathy
– V21 HCC 18; V22 HCC 18
– V21 HCC 141
• E11.42 Type 2 diabetes mellitus with diabetic polyneuropathy
– V21 HCC 18; V22 HCC 18
– V21 75
• E11.51 Type 2 diabetes mellitus with diabetic peripheral angiopathy
without gangrene
– V21 HCC 18; V22 HCC 18
– V21 HCC 108; V22 HCC 108
Page 52March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
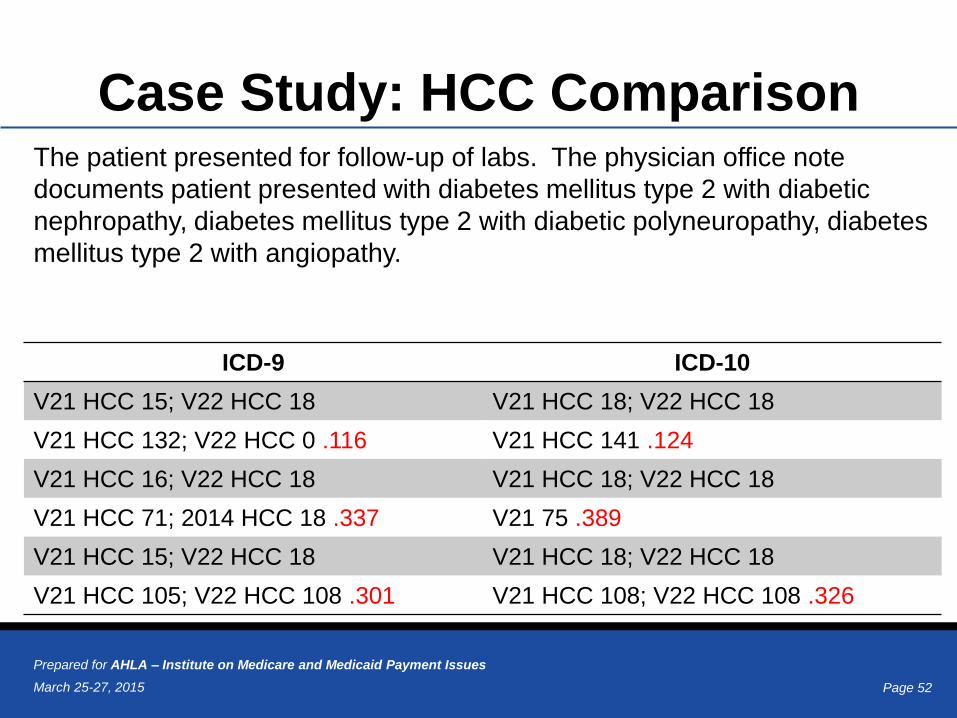
Case Study: HCC Comparison
ICD-9 ICD-10
V21 HCC 15; V22 HCC 18 V21 HCC 18; V22 HCC 18
V21 HCC 132; V22 HCC 0 .116 V21 HCC 141 .124
V21 HCC 16; V22 HCC 18 V21 HCC 18; V22 HCC 18
V21 HCC 71; 2014 HCC 18 .337 V21 75 .389
V21 HCC 15; V22 HCC 18 V21 HCC 18; V22 HCC 18
V21 HCC 105; V22 HCC 108 .301 V21 HCC 108; V22 HCC 108 .326
The patient presented for follow-up of labs. The physician office note
documents patient presented with diabetes mellitus type 2 with diabetic
nephropathy, diabetes mellitus type 2 with diabetic polyneuropathy, diabetes
mellitus type 2 with angiopathy.
Page 53March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
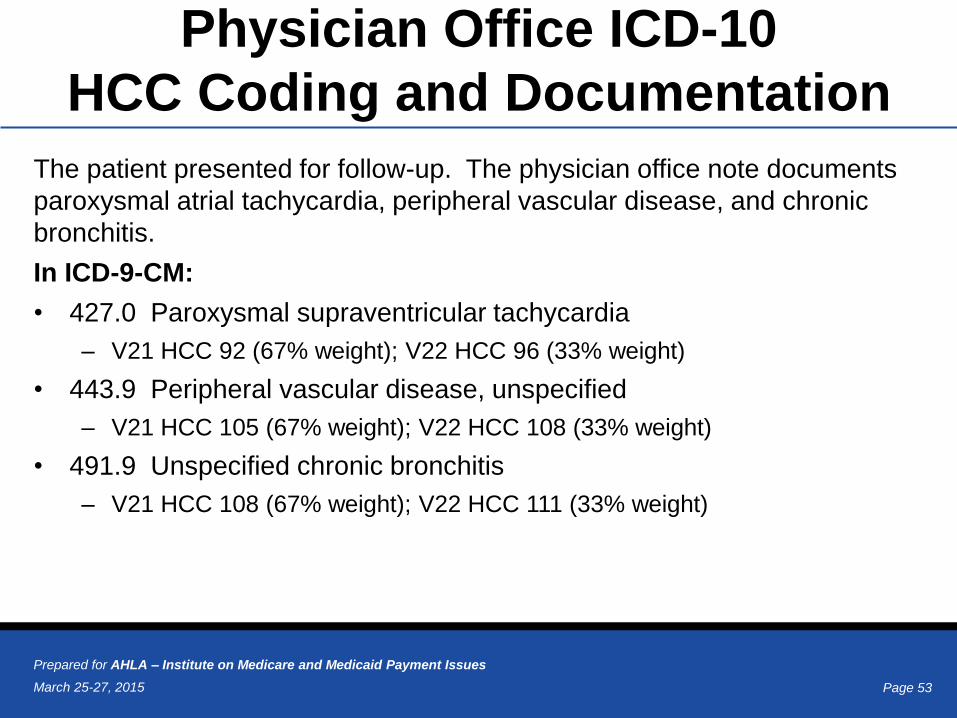
Physician Office ICD-10
HCC Coding and Documentation
The patient presented for follow-up. The physician office note documents
paroxysmal atrial tachycardia, peripheral vascular disease, and chronic
bronchitis.
In ICD-9-CM:
• 427.0 Paroxysmal supraventricular tachycardia
– V21 HCC 92 (67% weight); V22 HCC 96 (33% weight)
• 443.9 Peripheral vascular disease, unspecified
– V21 HCC 105 (67% weight); V22 HCC 108 (33% weight)
• 491.9 Unspecified chronic bronchitis
– V21 HCC 108 (67% weight); V22 HCC 111 (33% weight)
Page 54March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
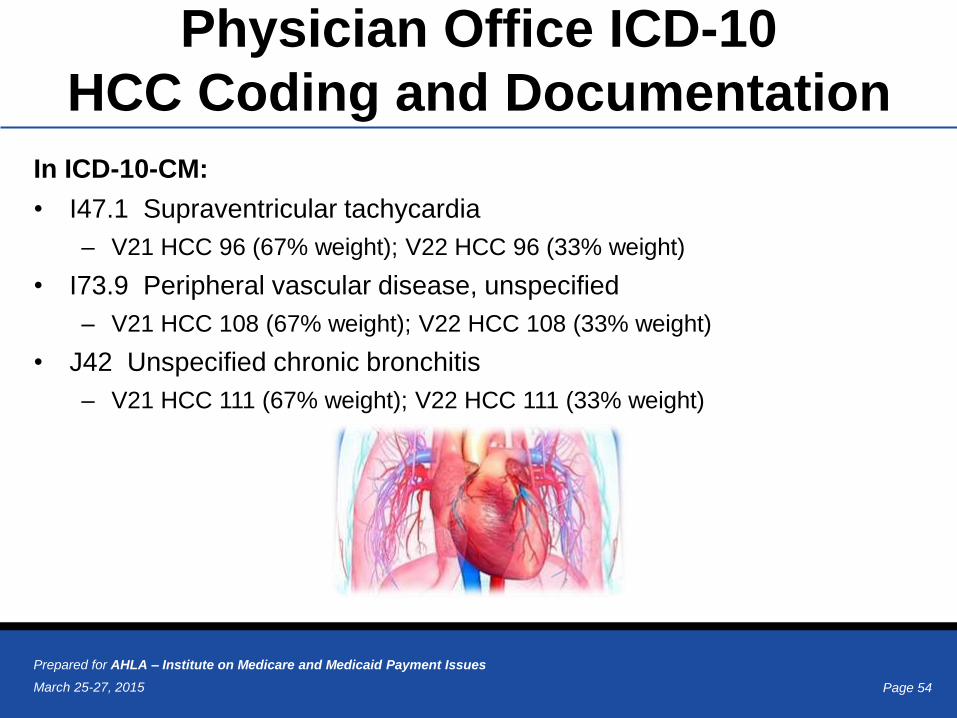
Physician Office ICD-10
HCC Coding and Documentation
In ICD-10-CM:
• I47.1 Supraventricular tachycardia
– V21 HCC 96 (67% weight); V22 HCC 96 (33% weight)
• I73.9 Peripheral vascular disease, unspecified
– V21 HCC 108 (67% weight); V22 HCC 108 (33% weight)
• J42 Unspecified chronic bronchitis
– V21 HCC 111 (67% weight); V22 HCC 111 (33% weight)
Page 55March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
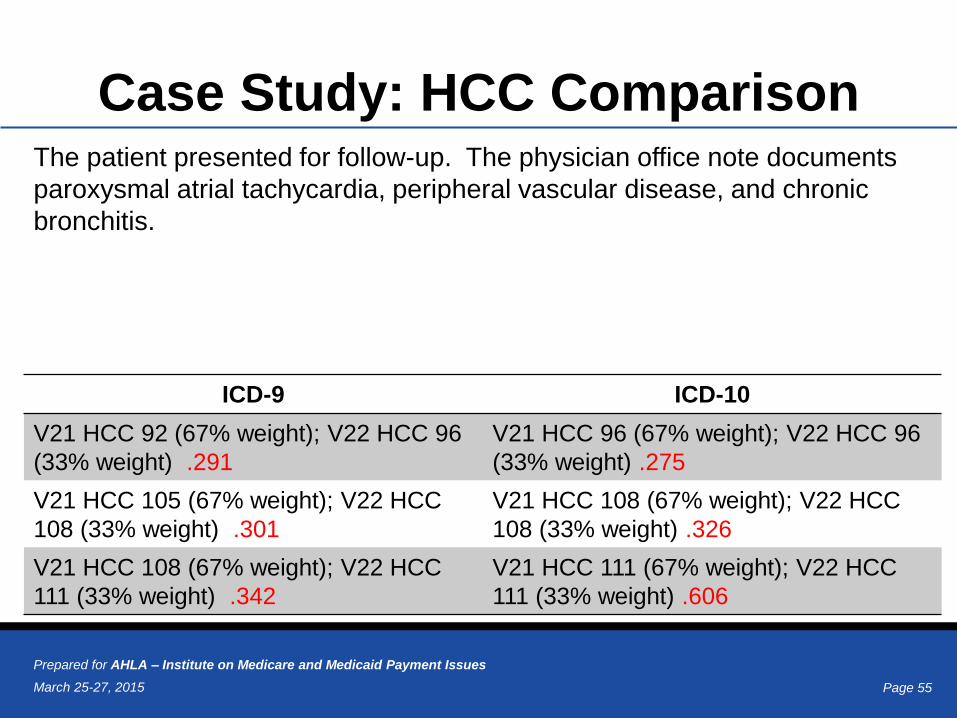
Case Study: HCC Comparison
ICD-9 ICD-10
V21 HCC 92 (67% weight); V22 HCC 96
(33% weight) .291
V21 HCC 96 (67% weight); V22 HCC 96
(33% weight) .275
V21 HCC 105 (67% weight); V22 HCC
108 (33% weight) .301
V21 HCC 108 (67% weight); V22 HCC
108 (33% weight) .326
V21 HCC 108 (67% weight); V22 HCC
111 (33% weight) .342
V21 HCC 111 (67% weight); V22 HCC
111 (33% weight) .606
The patient presented for follow-up. The physician office note documents
paroxysmal atrial tachycardia, peripheral vascular disease, and chronic
bronchitis.
Page 56March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Training
Clinicians
• Physicians – focus on codes germane to their practice and typical service offerings
• Review clinical documentation improvement efforts and develop new strategies
• Incorporate documentation improvement as component to compliance training
• Ancillary staff – identify needs and level of training needed, nursing, financial services, quality, utilization, ancillary departments…
Information Technology
• Training to ensure that codes are accurately cross-walked in organization’s IT systems
Page 57March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
The future?
WHO is currently working on ICD-11
• It will build upon ICD-10
• The first draft was made available
online in July 2011 for review
• The final draft is expected to be
submitted to WHO's World Health
Assembly for official endorsement
by 2017
Page 58March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Key Resources
• ICD-10 Proposed and Final Rules– http://edocket.access.gpo.gov/2008/pdf/E8-19298.pdf
– http://edocket.access.gpo.gov/2009/pdf/E9-743.pdf
• CMS Website on ICD-10– https://www.cms.gov/ICD10/
• CDC Website on Classification of Diseases– http://www.cdc.gov/nchs/icd.htm
• CMS ICD-10 Quick Reference Guide- http://www.cms.gov/Medicare/Coding/ICD10/2015-ICD-10-PCS-
and-GEMs.html
Page 59March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
There’s A Code For That!
Source: http://www.youtube.com/watch?v=GWJQSmqRLRk
Page 60March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Questions?
Page 61March 25-27, 2015
Prepared for AHLA – Institute on Medicare and Medicaid Payment Issues
Contact Information
Denise Hall, RN, BSN
Principal
Pershing Yoakley & Associates, P.C.
678-441-0645
www.pyapc.com
Julie Chicoine, Esq., RN, CPC, CPCO
Wexner Medical Center at
The Ohio State University
614-293-2007
www.medicalcenter.osu.edu
Thank you for allowing us to share our thoughts and
expertise with you.