Embed Size (px)
Citation preview
Hepatitis C Treatment 2017- 2018
By
DR MONKEZ M YOUSIF
Professor of Internal MedicineMember of AGA, EASL, ISC-Hepatitis WG
2017
Sources
1. Recommendations for Testing, Managing, and Treating Hepatitis C AASLD 2015. Updated September 21, 2017.
2. EASL Recommendations for management of HCV September 23, 2016.
3. National Committee for Control of HCV. Updated December 26, 2016.
Where HCV Therapy Stands Now
• Interferon is gone; ribavirin . . . not quite
• SVR in > 95% of pts
• “Difficult-to-cure” populations no longer difficult
– HIV coinfection -- Cirrhosis
– Persons who inject drugs (PWID)
– Renal failure and kidney transplant
– Liver transplant -- Old age
• Emergent issues and controversies:
– HBV reactivation
– HCC recurrence after DAA therapy
• Cost and access issues persist but improving
Hepatitis C Treatment in 2017

CDC Recommended Testing Sequence for Identifying Current HCV Infection
• Persons with current (active) HCV infection
should receive education and interventions
aimed at:
−Reducing progression of liver disease
−And preventing transmission of HCV.
Patient Education and Linkage to Care
• “All persons with current active HCV infection should be linked to a practitioner who is prepared to provide comprehensive management”
• “Improvement in identification of HCV infection and advances in treatment will have limited impact on HCV morbidity and mortality without concomitant improvement in linkage to care”
AASLD/IDSA HCV Guidelines.
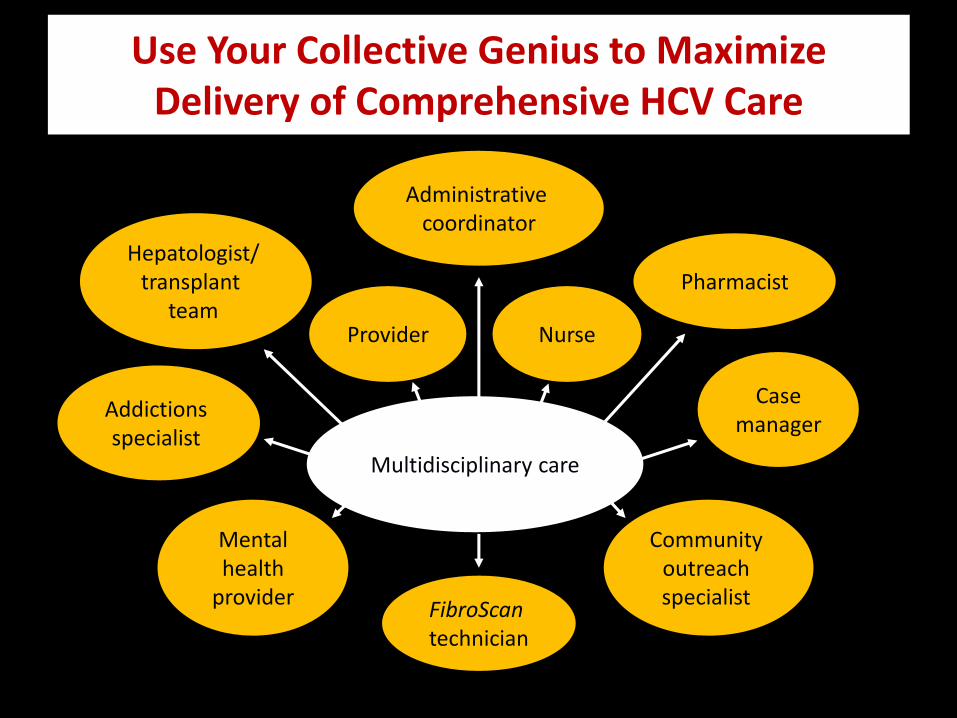
Use Your Collective Genius to Maximize Delivery of Comprehensive HCV Care
Multidisciplinary care
Provider Nurse
Hepatologist/ transplant
team
Casemanager
Addictions specialist
Mental health
provider
Community outreach specialist
Administrative coordinator
FibroScan technician
Pharmacist
WHEN AND IN WHOM TO INITIATE HCV THERAPY
Goal of treatment
• The goal of treatment of HCV-infected persons
is to reduce all-cause mortality and liver-
related health adverse consequences,
including end-stage liver disease and
hepatocellular carcinoma, by the achievement
of virologic cure as evidenced by an SVR.
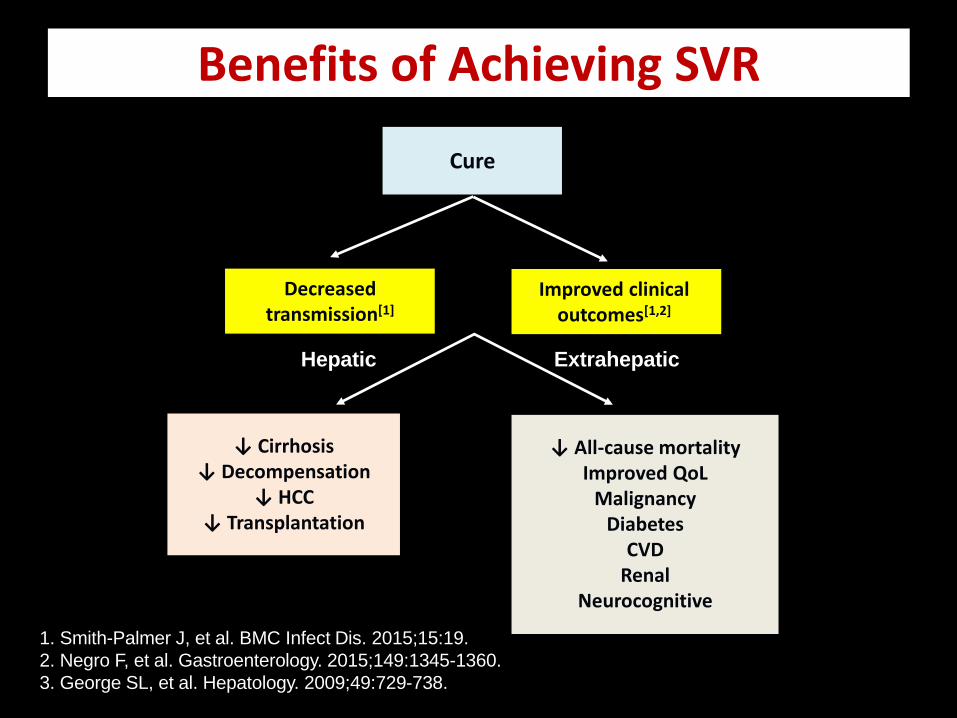
Benefits of Achieving SVR
↓ Cirrhosis↓ Decompensation
↓ HCC↓ Transplantation
↓ All-cause mortalityImproved QoL
MalignancyDiabetes
CVDRenal
Neurocognitive
Cure
Improved clinical outcomes[1,2]
1. Smith-Palmer J, et al. BMC Infect Dis. 2015;15:19.
2. Negro F, et al. Gastroenterology. 2015;149:1345-1360.
3. George SL, et al. Hepatology. 2009;49:729-738.
Hepatic Extrahepatic
Decreased transmission[1]
Recommendations for when and in whom to initiate treatment
• Treatment is recommended for all patients with chronic HCV infection, except those with short life expectancies owing to comorbid conditions.

Available Therapies
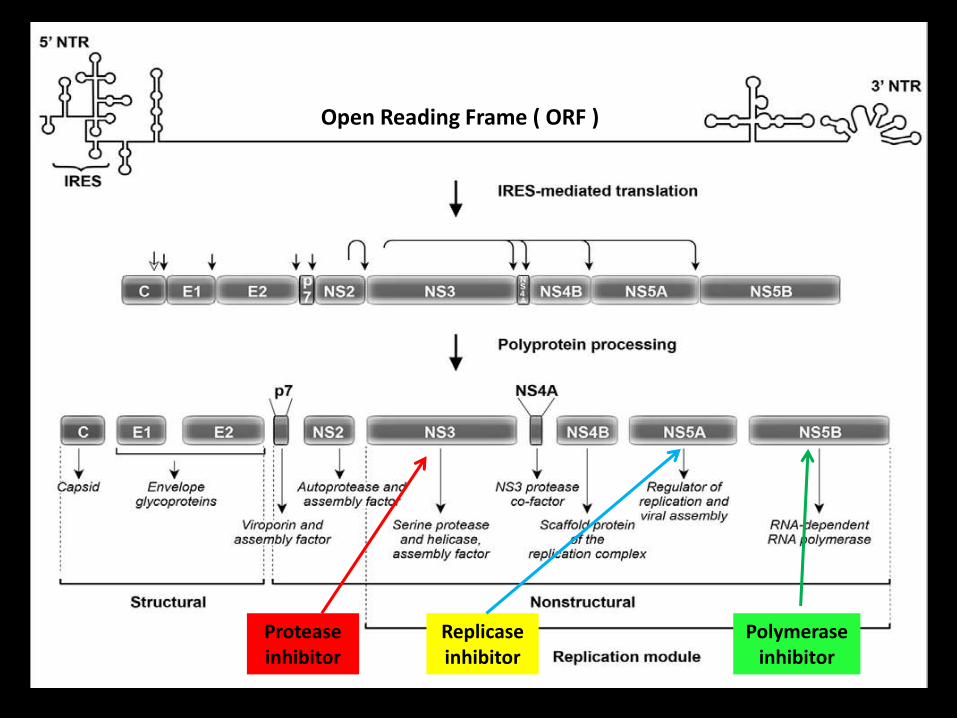
Open Reading Frame ( ORF )
Protease inhibitor
Replicaseinhibitor
Polymerase inhibitor
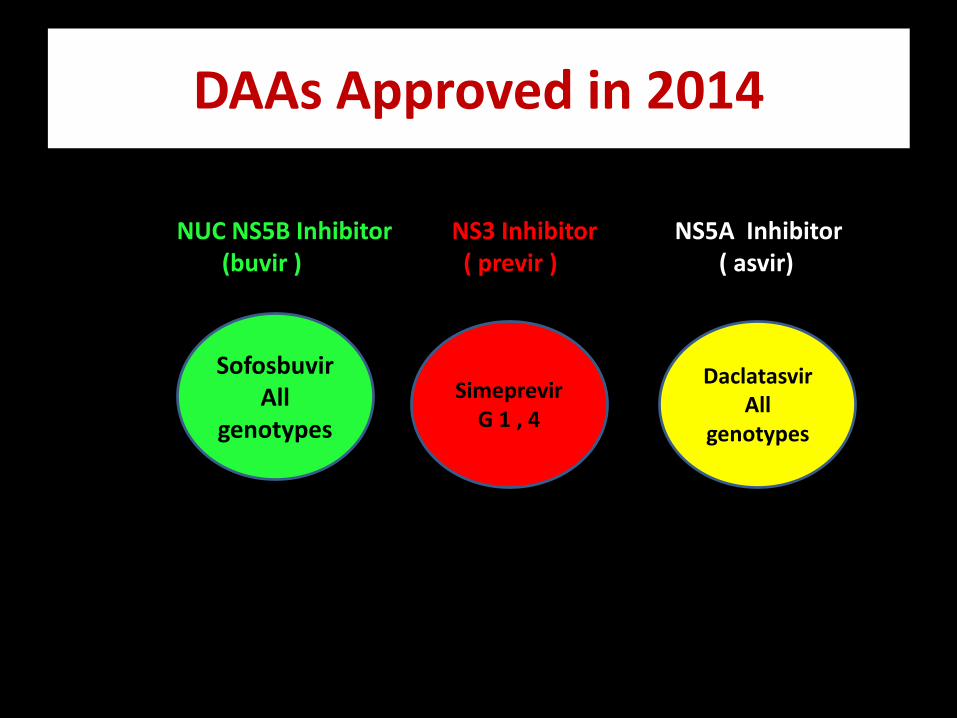
DAAs Approved in 2014
SofosbuvirAll
genotypes
SimeprevirG 1 , 4
DaclatasvirAll
genotypes
NUC NS5B Inhibitor NS3 Inhibitor NS5A Inhibitor(buvir ) ( previr ) ( asvir)
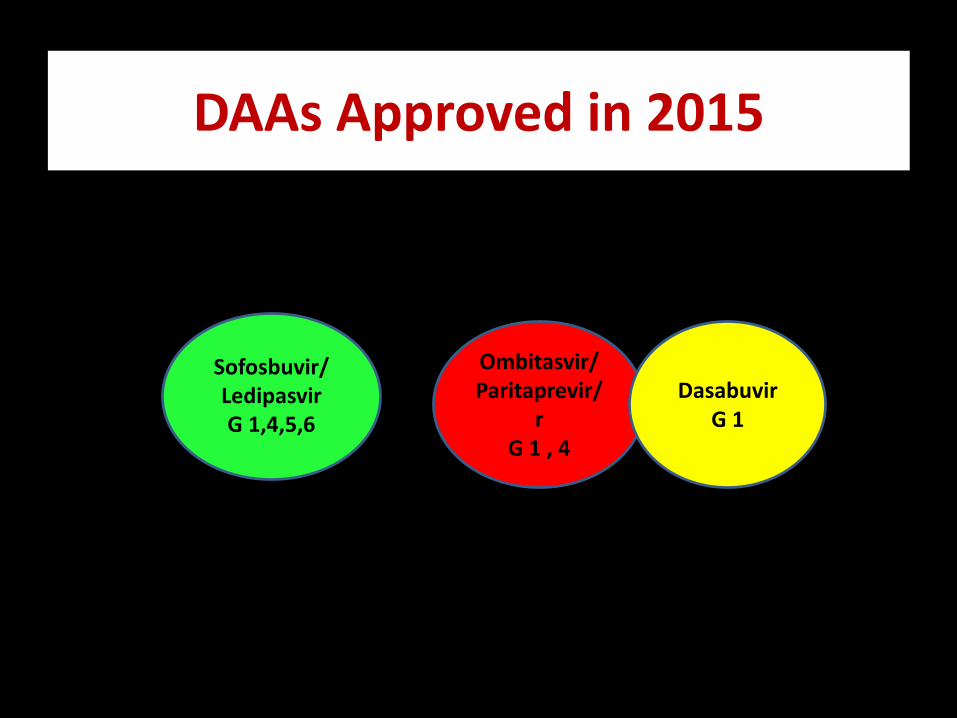
DAAs Approved in 2015
Sofosbuvir/ LedipasvirG 1,4,5,6
Ombitasvir/Paritaprevir/
rG 1 , 4
DasabuvirG 1
DAAs Approved in 2016
Sofosbuvir/ Velpatasvir
All Genotypes
Grazoprevir/ Elbasvir
G 1 , 4

DAAs Approved in 2017
Sofosbuvir/ Velpatasvir/Voxilaprevir
All Genotypes
Glecaprevir/ Pibrentasvir
All Genotypes
Investigational DAA
Ruzasvir
All Genotypes
Uprifosbuvir
All Genotypes

DAA Available In Egypt’s Market 2017
• Sofosbuvir
• Simeprevir
• Daclatasvir
• Sofosbuvir/Ledipasvir
• Ombitasvir/Paritaprevir/r
• Ribavirin
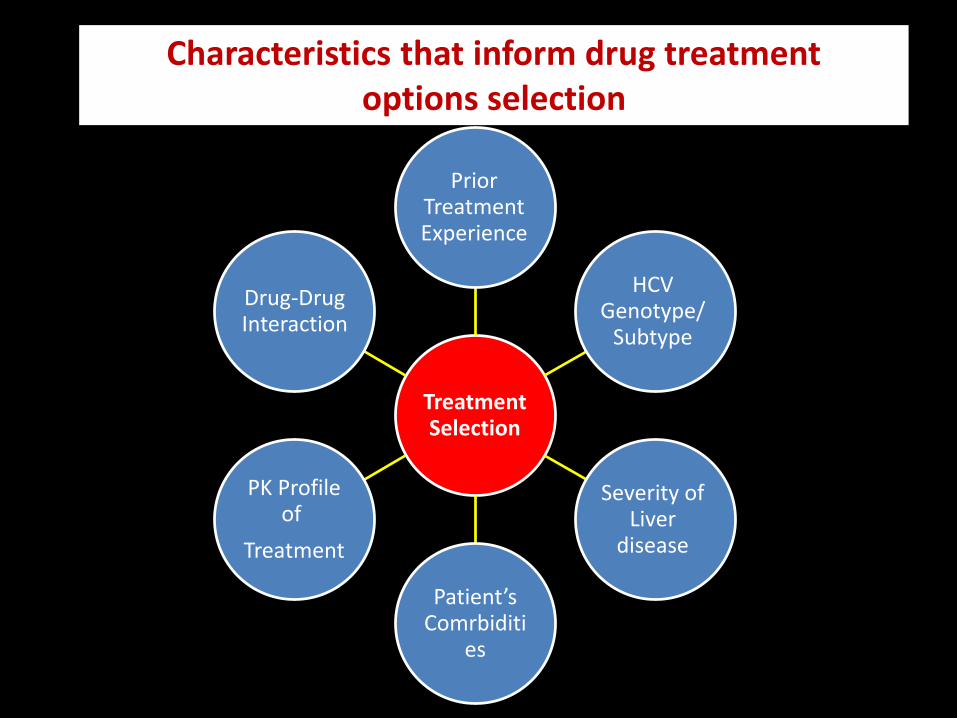
Treatment Selection
Prior Treatment Experience
HCV Genotype/
Subtype
Severity of Liver
disease
Patient’s Comrbiditi
es
PK Profile of
Treatment
Drug-Drug Interaction
Characteristics that inform drug treatment options selection
Hepatitis C Treatment
Al-Ahrar VHTC
CHC Patient’s treatment Pathway
• Preparatory Clinic
• Evaluation Clinic
• Revision Committee
• Treatment Clinic
• Awareness Clinic
• Follow up Clinic
Preparatory Clinicالعيادة التحضيرية
• Operator: Medical or Paramedical employee
• Functions:مراجعة الفحوصات المطلوبة1.
» HCV RNA PCR» HBsAg » LFTs» S.creatinine» CBC» PT» αFP» FBS» HbA1c» ABD US» ECG» Echocardiography For patients >65 y

أخذ بيانات المريض2.
Age
Weight
Height
BMI
مالها في حالة نقصان أي من هذه البيانات يوجه المريض الستك
و الرجوع للعيادة في أسرع وقت
Evaluation Clinicعيادة التقييم
• Operator: Certified Physicians of the Center
• Functions::أخذ التاريخ المرضي مع التركيز علي البيانات االتية:أوال
Naïve or T. Experienced Comorbid diseases ( DM, HTN, IHD, COPD, Malignancies, Neuropsychiatric
diseases …etc)
عمل قائمة باألدوية التي يستخدمها المريض:ثانيا
مراجعة التحاليل و األشعات:ثالثا
CTP Score & FIB-4تقييم حالة الكبد :رابعا Inclusion & Exclusion Criteriaمراجعة :خامسا: تصنيف المريض:سادسا
Easy to Treat Difficult to Treat Special Population
كتابة استمارة العالج ووضع بروتوكول العالج: سابعا

Revision Committeeلجنة المراجعة
مرسل تقوم بمراجعة استمارة التعريف و كتابة طلب العالج ال
للمجالس الطبية للموافقة علي التغطية المالية
Treatment Clinicعيادة العالج
للمرض بعد صدور قرار العالج يقوم الطبيب المعالج بفتح ملف العالج•بعد مراجعة متأنية ألي مستجدات في فحوصات المريض أو أدوية
جديدة يستخدمها ألي سبب
مريض علي عند فتح الملف يراعي استيفاء كافة البيانات خاصة موافقة ال•دويةالبروتوكول و نموذج العلم بكافة األعراض الجانبية الشائعة لأل
.فق عليهثم يقوم الطبيب بكتابة وصفة العالج حسب البروتوكول المت•
حوصات كذلك يتولي الطبيب المعالج التنبيه علي المريض بعمل الف•باعا الالزمة في المواعيد المحددة و يقوم بتدوينها في ملف المريض ت
اثناء المراجعات الشهرية
م الخاص به يقوم الطبيب المعالج بالتوقيع علي البيانات مع و ضع الخت•بصورة واضحة عند كل زيارة
عيادة يوجه المريض بعد ذلك للصيدلية لصرف الروشتة ثم يوجه لل•التثقيفية
Awareness Clinicالعيادة التثقيفية
• Operators:• Clinical Pharmacist
• Dedicated Nurse
• Educator
• Functions:مراجعة العالج المنصرف من الصيدلية و التأكد من مطابقته لقرار العالج•
مراجعة لستة األدوية التي يستخدمها المريض ألمراض أخري ثم ادخالها علي • D-D Interactionبرنامج كشف التداخالت بينها و بين أدوية عالج الفيروس
Checkerة من في حالة و جود تحذيرات يتم الرجوع للطبيب المعالج بتوصي.العيادة موضحا بها التداخل و كيفية التصرف
إعطاء المريض ارشادات و اضحة عن كيفية و مواعيد استخدام عالج الفيروس•

و إرشاد المريض ألهميتها و توقيت PCRمراجعة شيكات ال •استخدامها
هاون التنبيه علي المريض بأخذ األدوية في مواعيدها و عدم الت•ب في ذلك حيث أن ترك جرعة من العالج دون استشارة الطبي
سببا المعالج بالمركز يؤثر في االستجابة النهائية و قد يكون.لالنتكاسة
يوم قبل 3-2الحضور للمركز لصرف الجرعة التالية من العالج •.نهاية الجرعة الحالية
في حالة حدوث أي طارئ يمنع المريض من بدء العالج وذلك •48الل بعد صرفه من المركز يتم إبالغ الطبيب المعالج بذلك خ
أن ساعة علي األكثر ويتم اثبات ذلك في ملف المريض عليلبدء الجديد يراجع الطبيب بعد انتفاء سبب التأجيل إلثبات موعد ا
.قطاعوإال يعرض المريض نفسه لعدم تجديد صرف العالج لإلن
ارج إذا تعرض المريض لمشكلة صحية و نصحه طبيبه المعالج من خ•بد من المركز بإيقاف عالج الفيروس مؤقتا حتي يبرأ من هذه المشكلة الابالغ الطبيب المعالج داخل المركز بواسطة المريض نفسه أو أحد
ح أقاربه علي أن يقوم الطبيب بالمركز بمراجعة الموقف و ال ينص.بإيقاف العالج إال في ظروف محددة و بضوابط واضحة
اعطاء ارشادات واضحة بضرورة منع الحمل اثناء العالج خاصة إذا •رورة منع اشتمل العالج علي عقار ريبافيرين و في هذه الحالة ينبه بض
شهور بعد نهاية العالج علي األقل منعا لحدوث تشوهات6الحمل مدة .جنينية
ة في ارشادات عامة عن كيفية تجنب منع انتقال العدوي لآلخرين خاص•محيط األسرة
ارشادات خاصة بضرورة تغيير األدوات الشخصية كل شهر أثناء •وف ل, المقص, القصافة, عدة الحالقة, السواك, فرشة األسنان)العالج
.مع عدم استخدام أدوات الغير( االستحمام

Follow Up Clinicعيادة المتابعة
Operators: Trained Physician, Filing and IT Personnel.
Functions: تختص هذه العيادة بمتابعة و رصد تحاليل المريض خاصةHCV RNA PCR
أسبوع بعد نهاية العالج12و 4
و االتصال بالمرضي المنقطعين عن المتابعة لحثم علي مراجعة المركزعالج و اعطاء استكمال البيانات الناقصة و ذلك للتعرف علي النتيجة النهائية لل
.فرصة عالج أخري للمنتكسين
شهور بواسطة اشعة تليفزيونية و فحوصات6-4متابعة مرضي التليف كل(HCC)معملية لمتابعة كفاءة الكبد الوظيفية و ترصد حدوث أورام الكبد
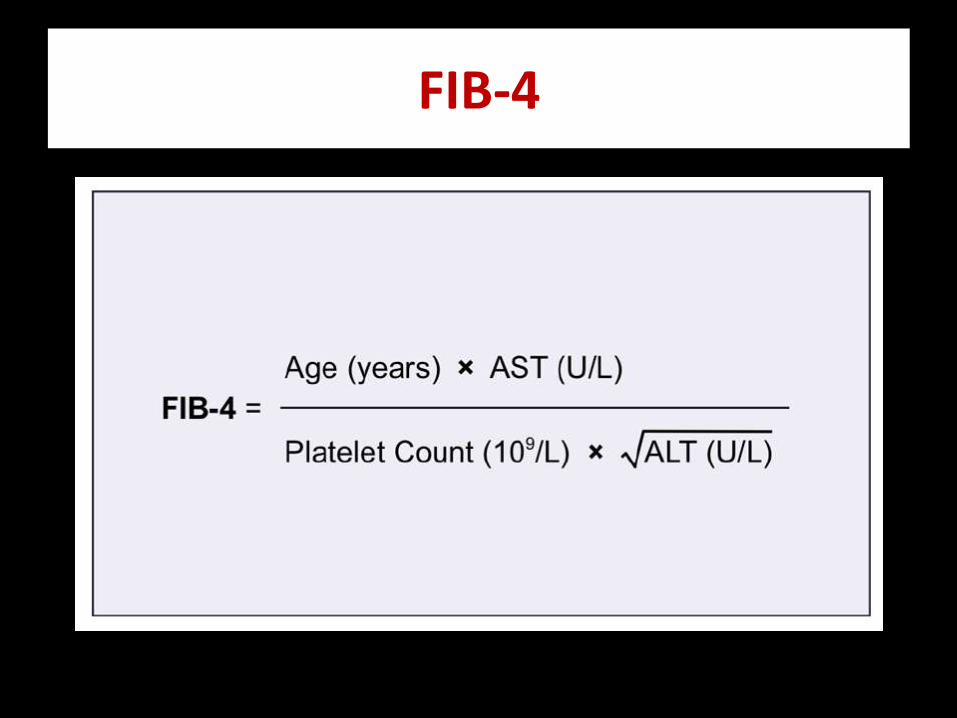
FIB-4
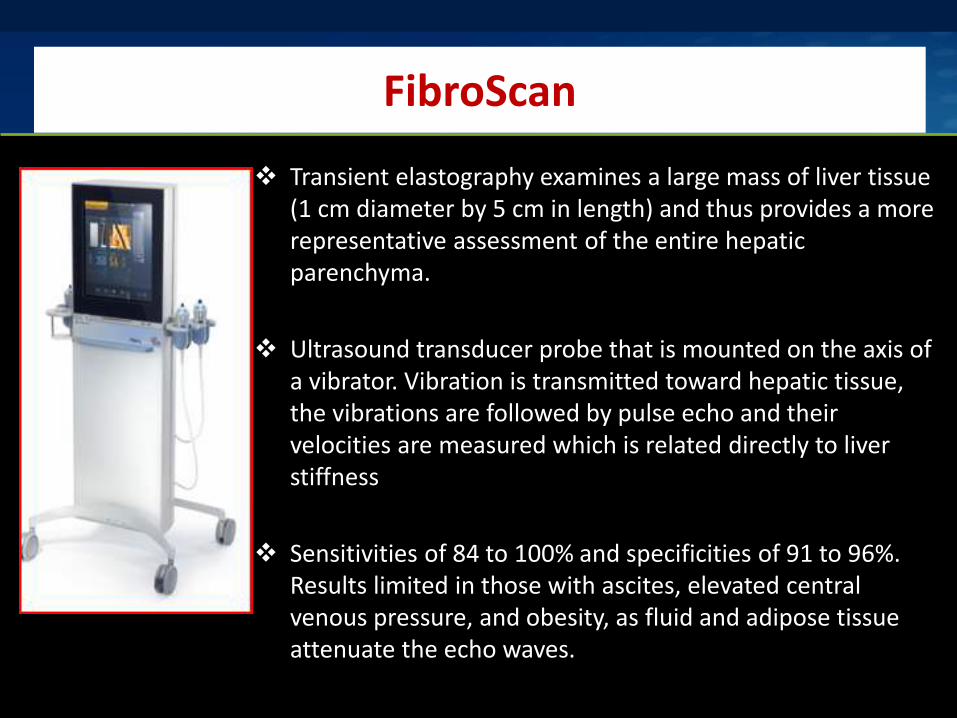
FibroScan
Transient elastography examines a large mass of liver tissue (1 cm diameter by 5 cm in length) and thus provides a more representative assessment of the entire hepatic parenchyma.
Ultrasound transducer probe that is mounted on the axis of a vibrator. Vibration is transmitted toward hepatic tissue, the vibrations are followed by pulse echo and their velocities are measured which is related directly to liver stiffness
Sensitivities of 84 to 100% and specificities of 91 to 96%. Results limited in those with ascites, elevated central venous pressure, and obesity, as fluid and adipose tissue attenuate the echo waves.

Cut-offs for the diagnosis of cirrhosis
kPa HCV-HIV HCV HBV
Sensitivity 95% 14.6 10 6
Specificity 95% 17.6 14.1 14.3
Sensitivity + specificity 10.4 10.3
Ganne-Carrié N et al. Hepatology 2006;44:1511-7
Vergara S et al. Clin Inf Dis2007;45:969-74
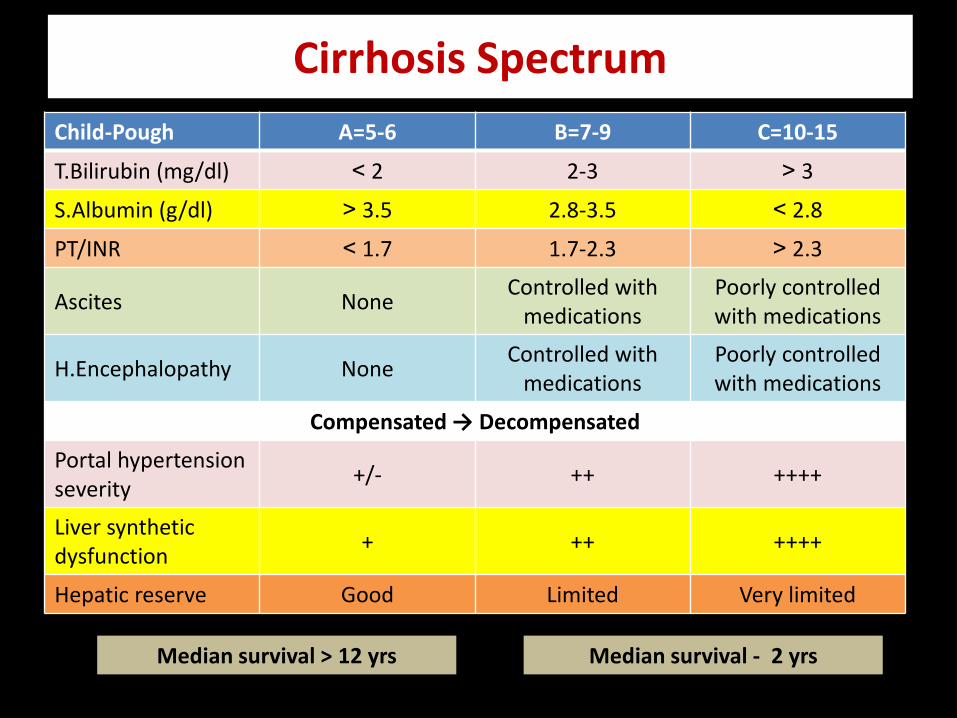
Cirrhosis Spectrum
C=10-15B=7-9A=5-6Child-Pough
< 32-3> 2T.Bilirubin (mg/dl)
> 2.82.8-3.5< 3.5S.Albumin (g/dl)
< 2.31.7-2.3> 1.7PT/INR
Poorly controlled with medications
Controlled with medications
NoneAscites
Poorly controlled with medications
Controlled with medications
NoneH.Encephalopathy
Compensated → Decompensated
+++++++/-Portal hypertension severity
+++++++Liver synthetic dysfunction
Very limitedLimitedGoodHepatic reserve
Median survival > 12 yrs Median survival - 2 yrs

Drug-Drug Interactions
INITIAL TREATMENT OF HCV G4 INFECTION
NCCVH Hepatitis C Treatment ProtocolUpdate December 2016

Inclusion criteria
1. HCV RNA Positivity
2. Age: ≥ 18
– Patients ≥ 65 years old should undergo cardiological assessment prior to therapy by ECG, echocardiography and cardiological consultation.
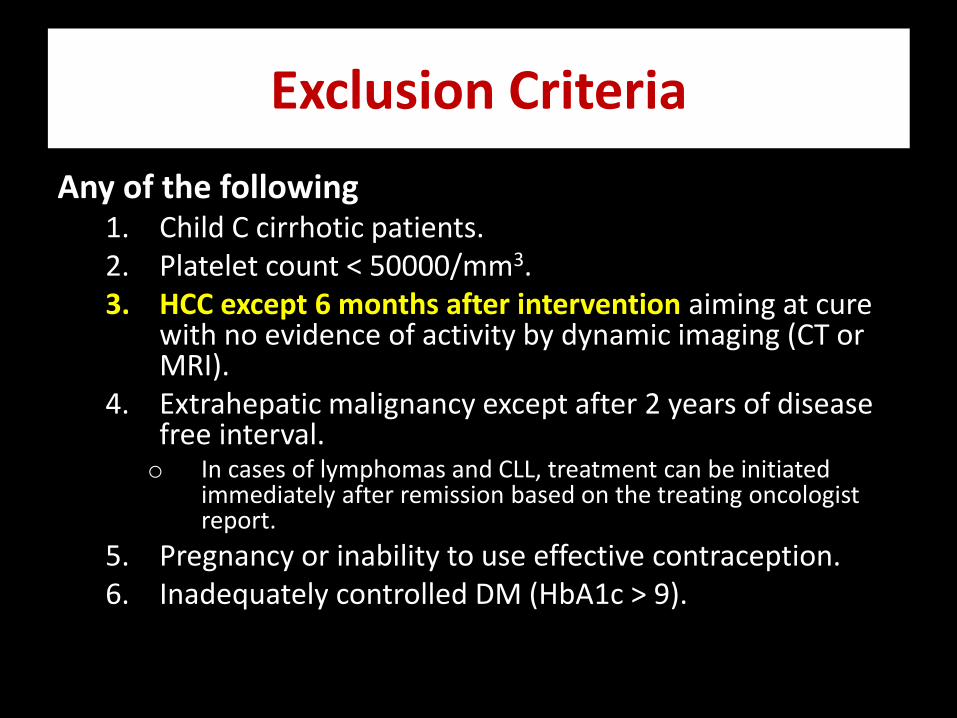
Exclusion Criteria
Any of the following1. Child C cirrhotic patients.2. Platelet count < 50000/mm3.3. HCC except 6 months after intervention aiming at cure
with no evidence of activity by dynamic imaging (CT or MRI).
4. Extrahepatic malignancy except after 2 years of disease free interval.o In cases of lymphomas and CLL, treatment can be initiated
immediately after remission based on the treating oncologist report.
5. Pregnancy or inability to use effective contraception.6. Inadequately controlled DM (HbA1c > 9).
Patient Categories
• Easy to treat group:– Treatment naïve.– T.Bil ≤ 1.2 mg/dl.– Serum Albumin ≥ 3.5 g/dl– INR ≤ 1.2.– Platelet count ≥ 150000 /mm3.
• Difficult (not easy)to treat group:– Peg-Interferon treatment experienced.– Total serum bilirubin > 1.2 mg/dl.– Serum albumin < 3.5 g/dl.– INR > 1.2– Platelet count < 150000/mm3
• Special Population Group:
– Non-responders to previous DAAs regimens
– Advanced liver disease (Child ≥ 9)
– Post-organ transplantation
– Chronic kidney disease (CKD)
– HCV coinfection with HBV and HIV
• Assessment of fibrosis:
– With FIB-4 is a must
• Treatment monitoring:
– HCV Viral load estimation at any time point between 12 and 24 weeks post-treatment to confirm successful eradication of the virus
Treatment Protocol
• Easy to treat group: eligible to be treated by any of the following regimens for 12 weeks:
– Paritaprevir-r/Ombitasvir + RBV
– Sofosbuvir + Daclatasvir
• Difficult to treat group: eligible to be treated by any of the following regimens for 12 weeks:
– Sofosbuvir + Daclatasvir + RBV– The starting dose of RBV is 600 mg/day. A trial should be done
to reach a dose of 1000 mg/day based on the patient tolerability.

Treatment of special populations
1. Non-responders to previous DAAs regimens
2. Advanced liver disease (Child ≥ 9)
3. Post-organ transplantation
4. Chronic kidney disease (CKD)
5. HCV coinfection with HBV and HIV
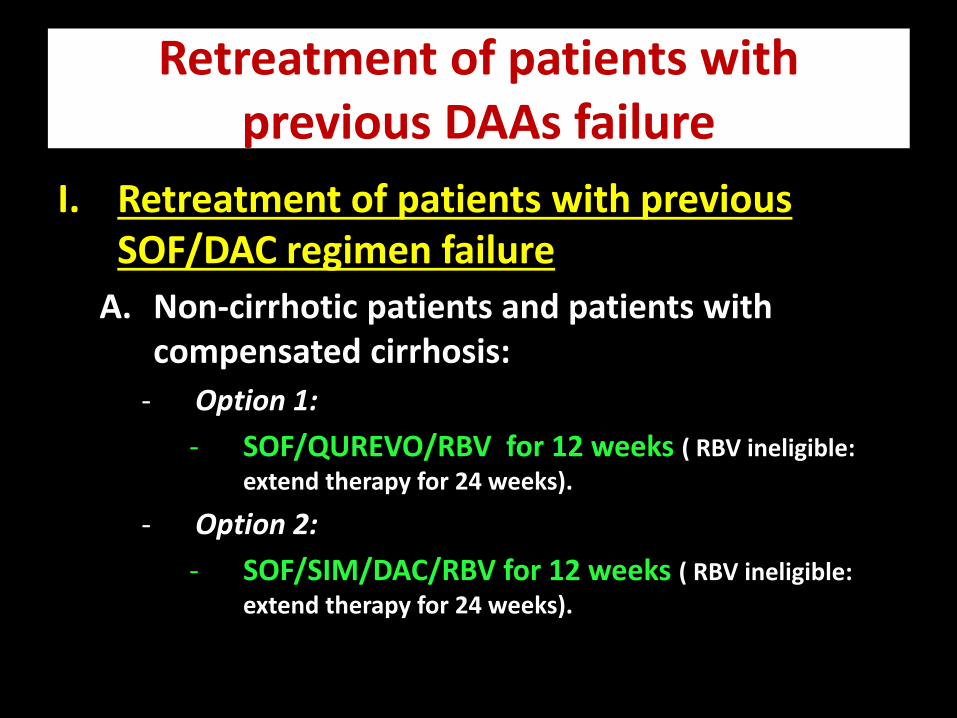
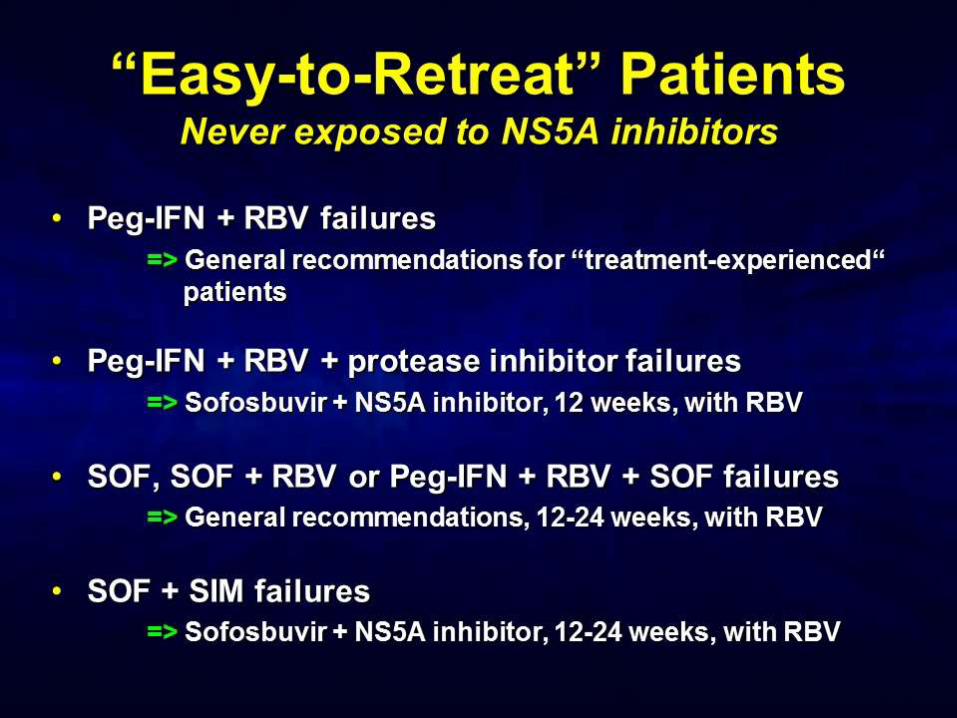
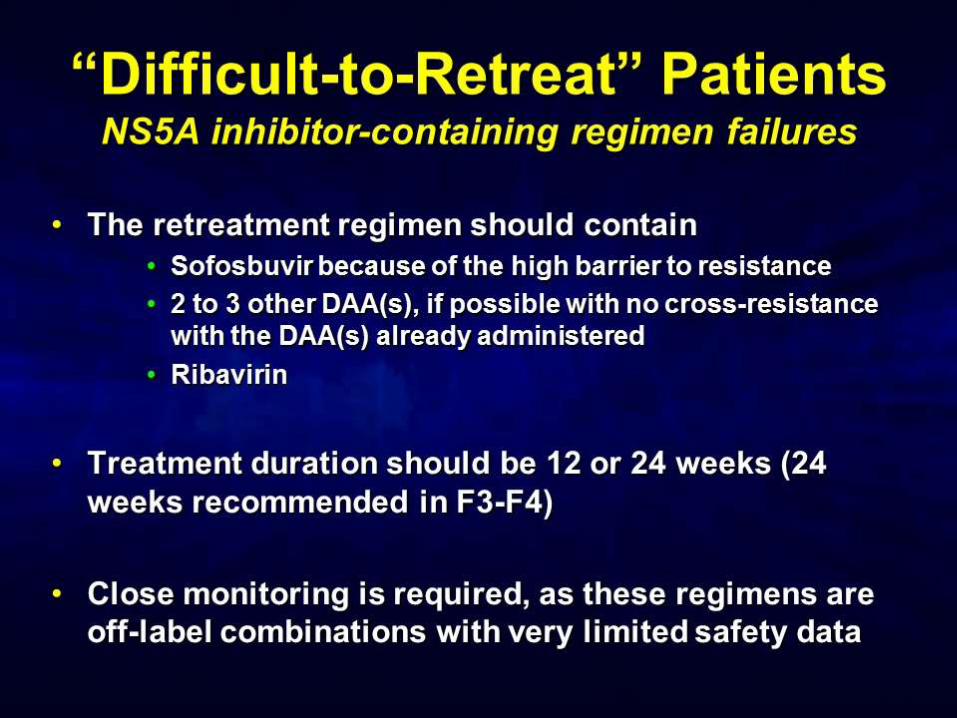
Retreatment of patients with previous DAAs failure
I. Retreatment of patients with previous SOF/DAC regimen failure
A. Non-cirrhotic patients and patients with compensated cirrhosis:
- Option 1:
- SOF/QUREVO/RBV for 12 weeks ( RBV ineligible:
extend therapy for 24 weeks).
- Option 2:
- SOF/SIM/DAC/RBV for 12 weeks ( RBV ineligible:
extend therapy for 24 weeks).
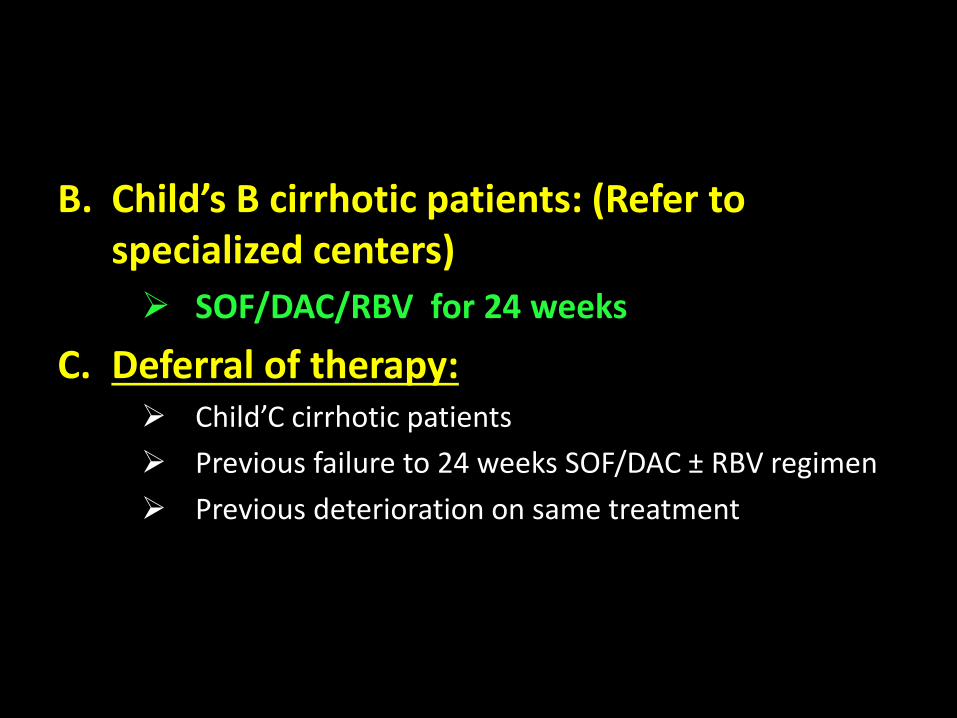
B. Child’s B cirrhotic patients: (Refer to specialized centers)
SOF/DAC/RBV for 24 weeks
C. Deferral of therapy: Child’C cirrhotic patients
Previous failure to 24 weeks SOF/DAC ± RBV regimen
Previous deterioration on same treatment
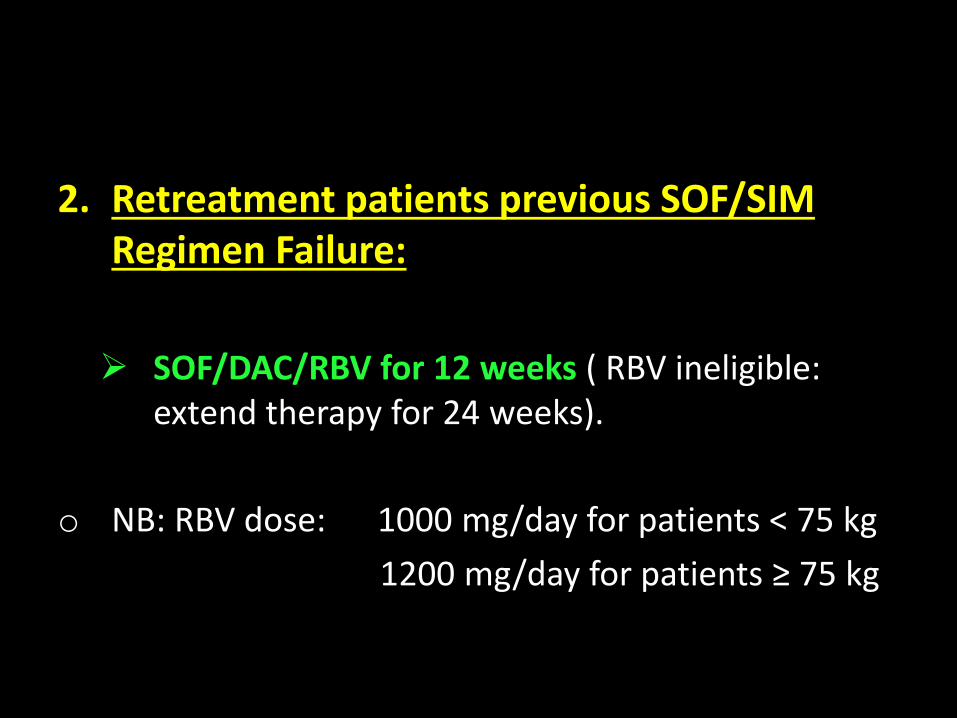
2. Retreatment patients previous SOF/SIM Regimen Failure:
SOF/DAC/RBV for 12 weeks ( RBV ineligible: extend therapy for 24 weeks).
o NB: RBV dose: 1000 mg/day for patients < 75 kg
1200 mg/day for patients ≥ 75 kg
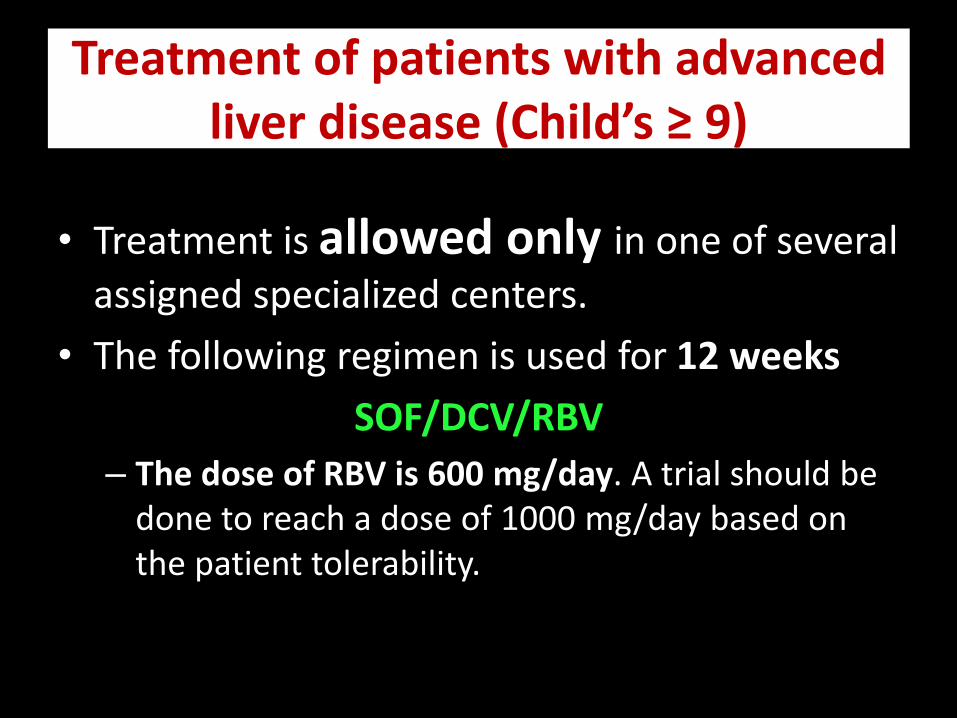
Treatment of patients with advanced liver disease (Child’s ≥ 9)
• Treatment is allowed only in one of several
assigned specialized centers.
• The following regimen is used for 12 weeks
SOF/DCV/RBV
– The dose of RBV is 600 mg/day. A trial should be done to reach a dose of 1000 mg/day based on the patient tolerability.
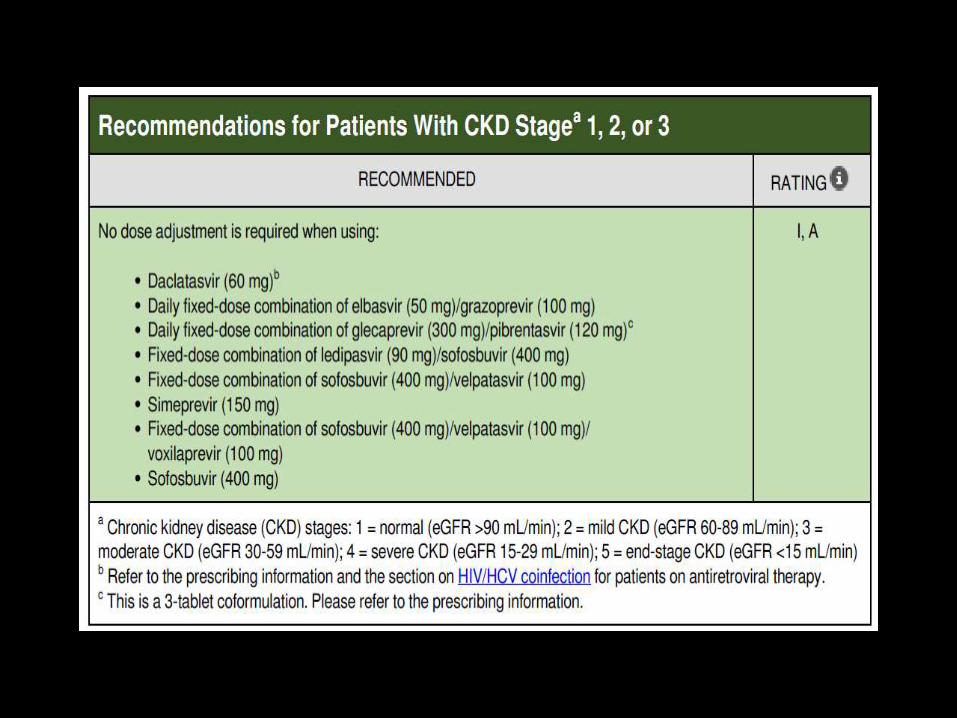
Treatment of Patient with Chronic Kidney Disease (CKD)
• In patients with serum creatinine exceeding the upper limit of normal, eGFR is calculated and accordingly:1. eGFR > 30 ml/min treat by the usual regimens.2. eGFR ≤ 30 ml/min treat by:
Paritaprevir/retonavir/ombitasvir + RBV
Provided the following are fulfilled:1. Patients have compensated liver (cirrhosis Child A or no cirrhosis)2. Hb level at least 10 gm/dl3. The patient has no associated uncontrolled co-morbidity (cardiac,
neuropsych;..)4. A nephrologist consultation is done. A report determining the
treatment eligibility and necessity and the exact RBV recommended dosage (and time of administration in relation to dialysis).
5. In case of dialysis, the patient should be aware of the high risk of reinfection by signing a consent form.
Treatment of Patients with Post organ Transplantation
SOF/DCV ± RBV for 24 weeks
Treatment of combined HCV and HBV
• Patients should be treated with the same regimens, following the same rules as HCV mono-infected patients.
• If HBV replicates at significant levels before, during or after HCV clearance, concurrent HBV nucleoside/neocleotide analogue therapy is indicated.
Treatment of Patients with Combined HCV and HIV:
• Co-management by the hepatologist and the treating infectious disease physician is needed.
• SOF should not be received in combination with tipranavir.


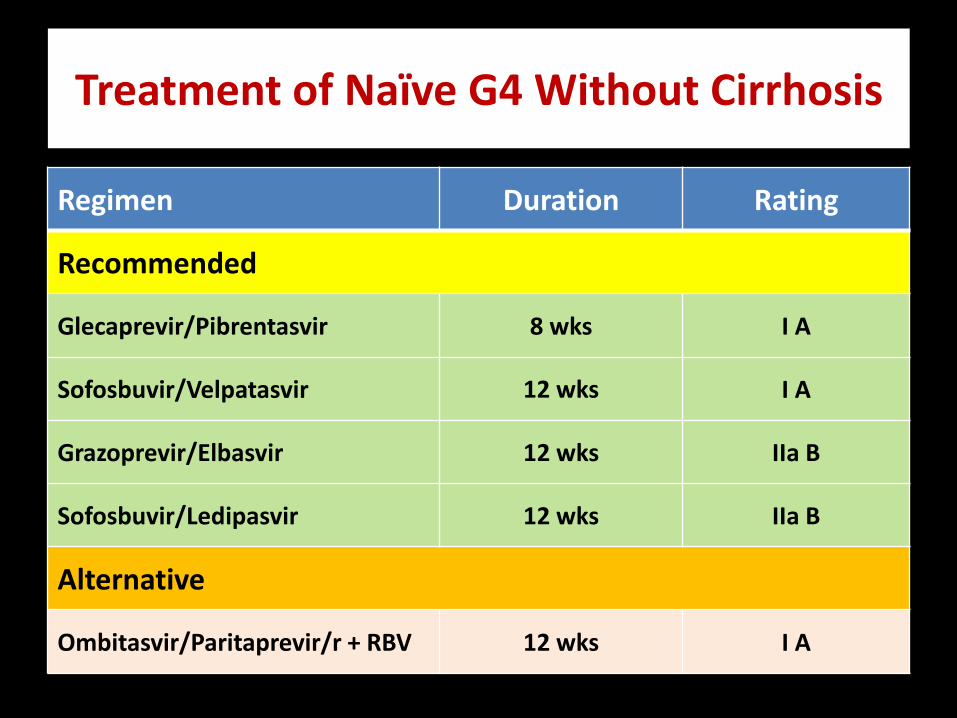
RatingDurationRegimen
Recommended
I A8 wksGlecaprevir/Pibrentasvir
I A12 wksSofosbuvir/Velpatasvir
IIa B12 wksGrazoprevir/Elbasvir
IIa B12 wksSofosbuvir/Ledipasvir
Alternative
I A12 wksOmbitasvir/Paritaprevir/r + RBV
Treatment of Naïve G4 Without Cirrhosis

RatingDurationRegimen
Recommended
I A12 wksSofosbuvir/Velpatasvir
I B12 wksGlecaprevir/Pibrentasvir
IIa B12 wksGrazoprevir/Elbasvir
IIa B12 wksSofosbuvir/Ledipasvir
Alternative
I A12 wksOmbitasvir/Paritaprevir/r + RBV
Treatment of Naïve G4 With Compensated Cirrhosis
RatingDurationRegimen
Recommended
I A12 wksSofosbuvir/Velpatasvir
I B8 wksGlecaprevir/Pibrentasvir
IIa B12 wksGrazoprevir/Elbasvir (for relapsers)
IIa B12 wksSofosbuvir/Ledipasvir
Alternative
I A12 wksOmbitasvir/Paritaprevir/r + RBV
Iia B16 wksGrazoprevir/Elbasvir (for breakthrough and null responders)
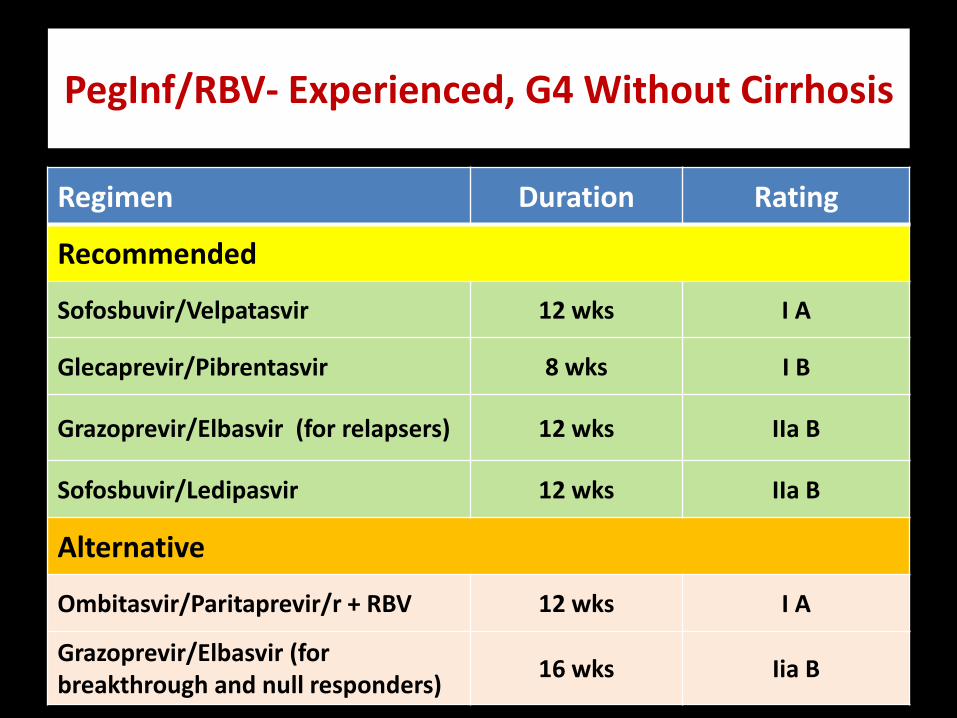
PegInf/RBV- Experienced, G4 Without Cirrhosis

RatingDurationRegimen
Recommended
I A12 wksSofosbuvir/Velpatasvir
I B12 wksGlecaprevir/Pibrentasvir
IIa B12 wksGrazoprevir/Elbasvir (for relapsers)
Alternative
I A12 wksOmbitasvir/Paritaprevir/r + RBV
Iia B16 wksGrazoprevir/Elbasvir (for breakthrough and null responders)
IIa B12 wksSofosbuvir/Ledipasvir
PegInf/RBV- Experienced, G4 With Compensated Cirrhosis
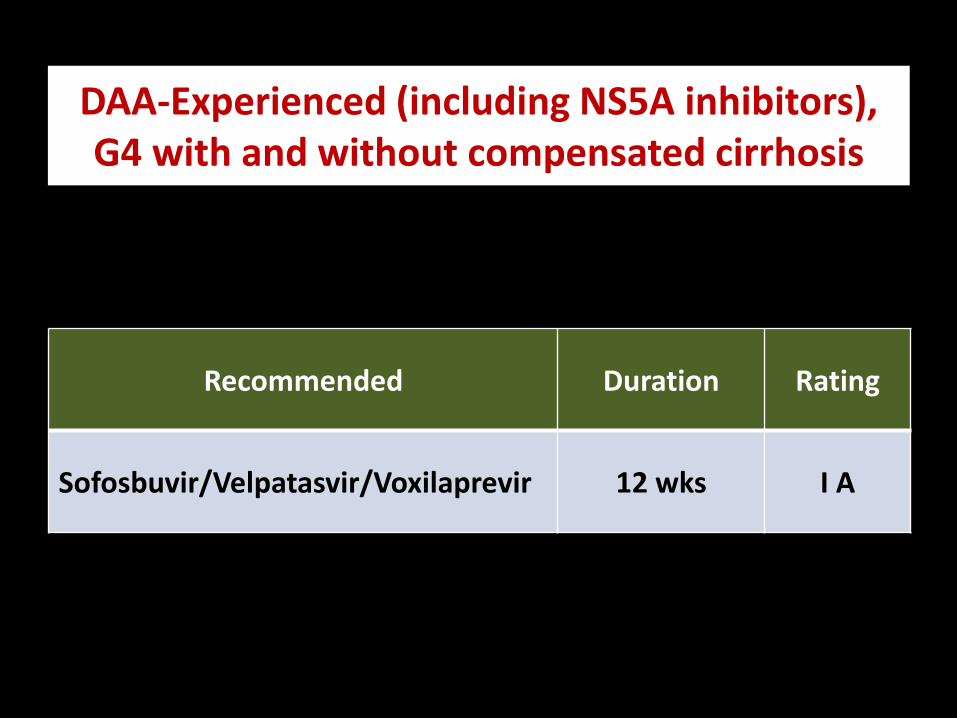
DAA-Experienced (including NS5A inhibitors), G4 with and without compensated cirrhosis
RatingDuration Recommended
I A12 wksSofosbuvir/Velpatasvir/Voxilaprevir

Patients with Decompensated Cirrhosis G 1,4,5,6 (RBV-Eligible)
RatingDurationRecommended
I A12 wksSofosbuvir/Ledipasvir/RBV (Initial dose 600)
I A12 wksSofosbuvir/Velpatasvir/RBV (weight-based)
I B12 wksSofosbuvir/Daclatasvir/RBV (Initial dose 600)( G 1, 4 only)
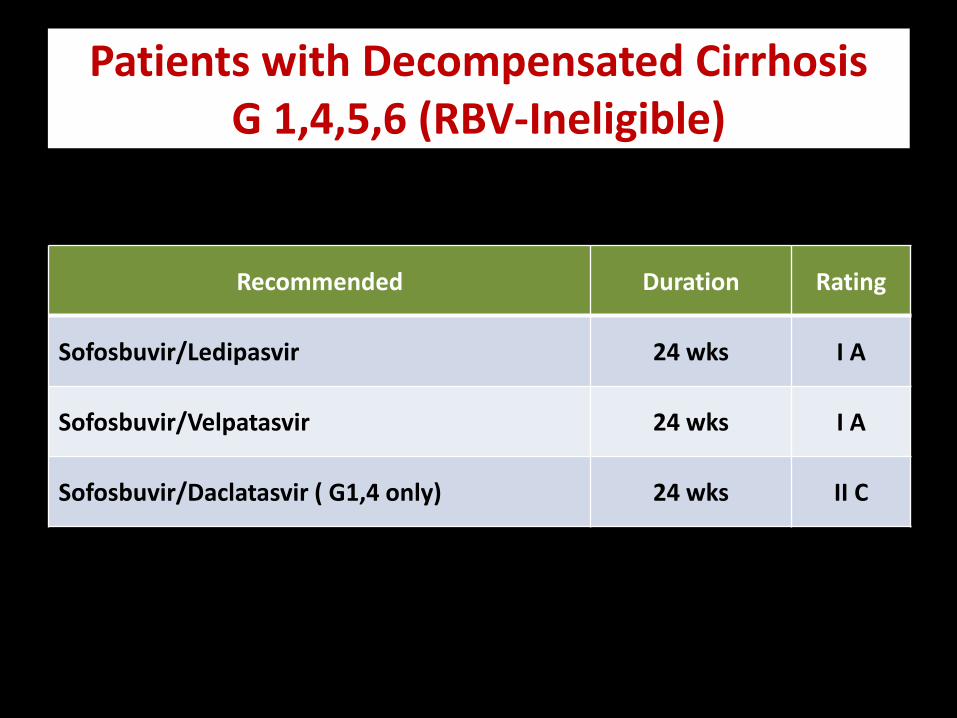
Patients with Decompensated Cirrhosis G 1,4,5,6 (RBV-Ineligible)
RatingDurationRecommended
I A24 wksSofosbuvir/Ledipasvir
I A24 wksSofosbuvir/Velpatasvir
II C24 wksSofosbuvir/Daclatasvir ( G1,4 only)
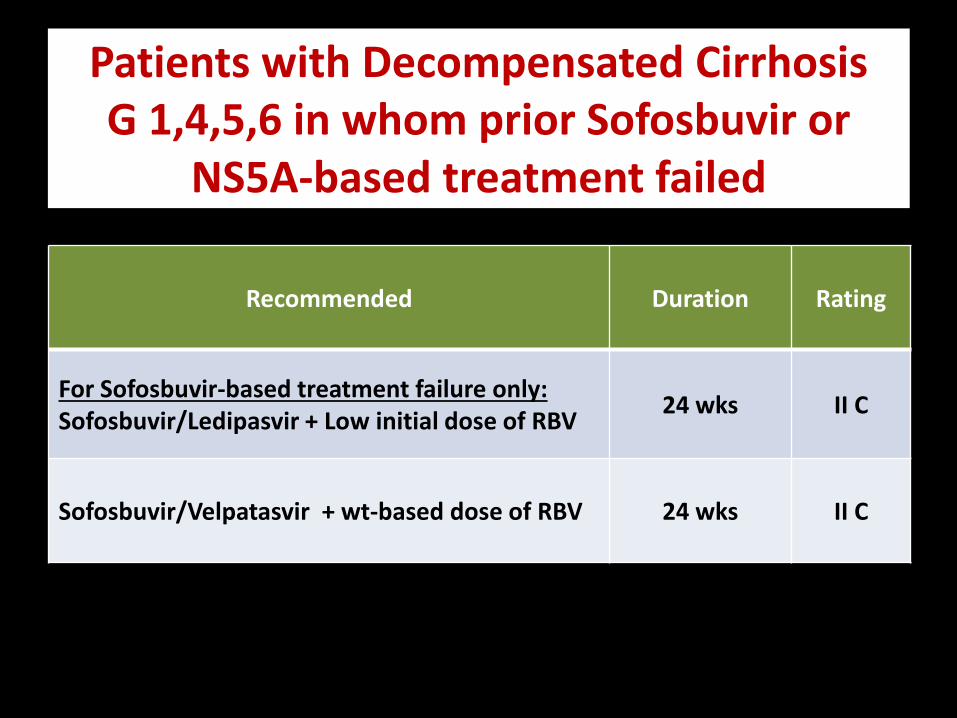
Patients with Decompensated Cirrhosis G 1,4,5,6 in whom prior Sofosbuvir or
NS5A-based treatment failed
RatingDurationRecommended
II C24 wksFor Sofosbuvir-based treatment failure only:Sofosbuvir/Ledipasvir + Low initial dose of RBV
II C24 wksSofosbuvir/Velpatasvir + wt-based dose of RBV



Conclusions
• The multiple current regimens are highly effective and safe across genotypes; confirmed in “real-world” studies.
• The available DAAs in Egypt’s Market , especially the generics are very effective with high safety profile (SVR more than 95%).
• However, new medications for retreatment of prior DAA – failure (particularly NS5A-based therapy) are needed and should be introduced in the market.
• GLE/PIB and SOF/VEL/VOX appear poised to be an 8-wk pangenotypic regimen for DAA-naive noncirrhoticpts

74
Monkez M Yousif