Embed Size (px)
Citation preview

Heart Transplantation
DR. KEWAL KRISHAN MBBS MS MCH DNB MNAMS FIACS (CTVS)ADVANCED FELLOW, MAYO CLINIC & MOUNT SINAI, USA
PROGRAM HEAD, HEART TRANSPLANT & VENTRICULAR ASSIST DEVICES
SENIOR CONSULTANT CARDIAC SURGEON
MAX SUPERSPECIALITY HOSPITAL, SAKET, NEWDELHI
1

Advanced Heart Failure - Definition
Patients have significant cardiac dysfunction and marked symptoms: dyspnea, fatigue end-organ hypoperfusion at rest or with minimal exertion despite maximal medical
therapy AHA Stage D Refractory symptoms requiring specialized
interventions to manage symptoms or prolong lifeGoodlin et al, Journal of Cardiac Failure Vol. 10 No. 3 2004Hunt SA et al JACC 2001;38:2101–13.

INTERMACS Profiles 1-3 Interagency Registry for Mechanical Circulatory Support
‘Frequent Flyer’Stevenson, JHLTX; 09:535

INTERMACS Profiles 4-7
Stevenson, JHLTX; 09:535
‘Housebound’
‘Class IIIb’

Deg
ree
of C
ircul
ator
y Su
ppor
t
IABP
PARTIAL SUPPORTCI* ↑15% CI ↑30-60%
ECMO
+
FULL SUPPORTCI ↑100%
Levitronix CentriMagAbiomed BVS 5000Abiomed AB 5000Abiomed Impella 5.0 LP Abiomed Impella 5.0 LD
TandemHeart pVADAbiomed Impella 2.5 LP
Short-term MCS Devices
*CI – cardiac index

Class I Indications for Cardiac Transplantation
Cardiogenic shock requiring mechanical assistance. Refractory heart failure with continuous inotropic infusion. NYHA functional class 3 and 4 with a poor 12 month
prognosis. Progressive symptoms with maximal therapy. Severe symptomatic hypertrophic or restrictive
cardiomyopathy. Medically refractory angina with unsuitable anatomy for
revascularization. Life-threatening ventricular arrhythmias despite
aggressive medical and device interventions. Cardiac tumors with low likelihood of metastasis. Hypoplastic left heart and complex congenital heart
disease.
When to think of Cardiac Transplantation
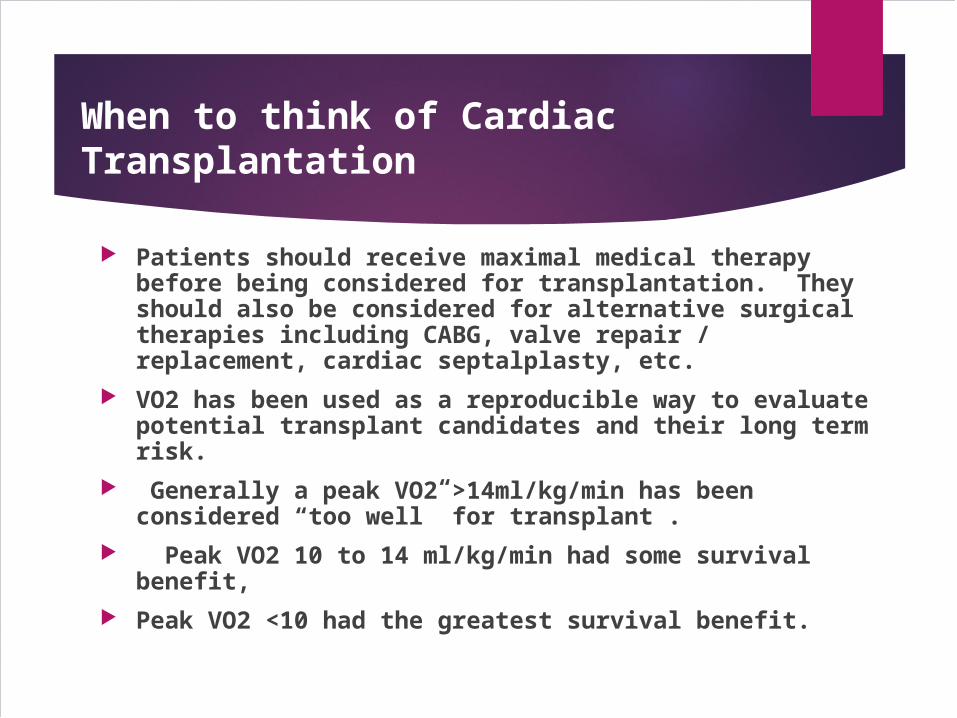
Patients should receive maximal medical therapy before being considered for transplantation. They should also be considered for alternative surgical therapies including CABG, valve repair / replacement, cardiac septalplasty, etc.
VO2 has been used as a reproducible way to evaluate potential transplant candidates and their long term risk.
Generally a peak VO2 >14ml/kg/min has been considered “too well” for transplant .
Peak VO2 10 to 14 ml/kg/min had some survival benefit,
Peak VO2 <10 had the greatest survival benefit.

Evaluation of Cardiac Transplantation Recipient
Right and Left Heart Catheterization. Cardiopulmonary testing ( VO2 max). Labs including BMP, CBC, LFT, UA, coags, TSH,
UDS, ETOH level, HIV, Hepatitis panel, PPD, CMV IgG, RPR / VDRL, PRA (panel of reactive antibodies), ABO and Rh blood type, lipids.
CXR, PFT’s including DLCO, EKG. Substance abuse history Mental health evaluation and social support. Financial support. Weight no more than 140% of ideal body weight.

Cardiac Donor
Brain death is necessary for any cadaveric organ donation. This is defined as absent cerebral function and brainstem reflexes with apnea during hypercapnea in the absence of any central nervous system depression.
There should be no hypothermia, hypotension, metabolic abnormalities, or drug intoxication.
If brain death is uncertain, confirmation tests using EEG, cerebral flow imaging, or cerebral angiography are indicated.

Matching Donor and Recipient
ABO blood type (match or compatible),
Donor weight to recipient ratio (must be 75% to 125%), Response to PRA ( Panel Reactive Antibodies) The PRA is a rapid measurement of preformed reactive
anti-HLA antibodies in the transplant recipient. In general PRA < 10 to 20% then no cross-match is necessary. If PRA is > 20% then a T and B-cell cross-match should be performed.

Case Study
A 42 yeears old gentleman with C/O EPIGASTRIC PAIN for the LAST 3 YEARS
Breathlessness for the last 2.5 yrs Orthoponea for the last 10 months ( off & on) DM(+) SINCE LAST 3 YEARS SMOKER SINCE LAST 1O YEARS
11

Case Study
FIRST EVALUATED – 1 YR BACK-HOSPITALISED DUE TO ACUTE HEART FAILURE
Due to frequent admissions ( INTERMACS 4) SUGGESTED BY CARDIOLOGIST FOR HEART TRANSPLANT DUE TO DCMP WITH SEVERE LV DYSFUNCTION
The patient first time saw me in Dec.2014.
12

Case Study
RIGHT HEART CATH-DONE WITH SWAN-GANZ CATHETER SHOWED- PVR=287
- SVR=1326 AFTER DOBUTAMINE INFUSION FOR 24 HOURS-
PVR=192 PFT-WITHIN NORMAL LIMIT DURING LAST 6 MONTHS-He HAD 3 EPISODES OF
ACUTE HEART FAILURE-HOSPITALISED and -MANAGED CONSERVATIVELY WITH INOTROPES AND DIURETCS
13

14

Case Study
CALL RECEVED FROM B.L. KAPOOR HOSPITAL FOR A+ DONOR AT 10.30PM PATIENT( Recepient) WAS CALLED TO REACH
HOSPITAL PT REACHED MAX HOSPITAL AT AROUND 11 PM AND WAS
IMMEDIATELY ADMITTED FOR HEART TRANSPLANTATION CTVS TEAM REACHED BLK HOSPITAL FOR ASSESSMENT OF
DONOR 57 YEARS MALE PATIENT ADMITTED AFTER ROAD-TRAFFIC ACCIDENT WITH HEAD
INJURY DECLARED BRAIN DEAD ON 31/7/15 AT 11 AM AND
RECONFIRMATION DONE AFTER 6 HOURS at 5.15 PM ACCORDING TO LEGAL REQUIREMENTS ( Human organ Act)
15

Case Study
ALL LAB INV. OF DONOR- with in acceptable limits 2-D ECHO- SHOWED NO REGIONAL WALL MOTION
ABNORMALITY, LVEF=50% CORONARY ANGIO=NORMAL DONOR WAS TAKEN TO O.T. AFTER MIDNIGHT AFTER PAINTING AND DRAPING-MEDIAN STERNOTOMY
WAS DONE HEART INSPECTED VISUALLY AFTER CONFIRMATION OF GOOD DONOR HEART-
RECEPIENT WAS WHEELED-IN MAX HOSPITAL O.T.
16

Case Study
AT BLK HOSPITAL UROLOGY AND HEPATOBILIARY TEAM STARTED ORGAN DISSECTION OF KIDNEYS AND LIVER
MEANWHILE LINES WERE INSERTED AND PT. WAS BEING PAINTED AND DRAPED FOR SURGERY AT MAX HOSPITAL
ONCE OTHER TEAMS WERE READY FOR ORGAN HARVESTING-HEART WAS TAKEN OUT AFTER CROSS-CLAMPING AND CARDIOPLEGIA
17

18

Case Study
RECEIPIENT CARDIECTOMY WAS DONE AND DONOR HEART WAS SUTURED IN the SEQUENCE OF
LEFT ATRIUM→IVC→PULMONARY ARTERY→AORTA →SVC
DE-AIRING WAS DONE AND CROSS-CLAMP WAS RELEASED AFTER GIVING 500MG METHYLPREDNISOLONE
HEART STARTED BEATING WEANED OFF CPB SLOWLY &DECANNULATION DONE CHEST CLOSED IN LAYERS AFTER PUTTING CHEST
TUBES PT WAS SHIFTED TO ICU AT 7.30 AM ON 1/8/15
19

Bicaval Approach
Left atrial anastomosis performed
Separate inferior and superior vena caval anastomosis
20

21

Case Study
PT WAS EXTUBATED ON 1st POD MOBILISED OUT OF BED ON 2nd POD SWAN ,SHEATH AND CHEST TUBES REMOVED ON 2nd POD INOTROPES WEANED IMMUNOSUPPRESSIVE DRUGS STARTED -TACROLIMUS
AND MYCOPHENOLATE MOFETIL METHYLPREDNISOLONE WAS PUT ON WEANING MODE PT RECOVERed DISCHARGED WITHIN A WEEK FROM
HOSPITAL
22

23

24

HEART TRANSPLANTATION Kaplan-Meier Survival (1/1982-6/2005)
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Years
Surv
ival
(%)
Half-life = 11.0 yearsConditional Half-life = 14.0 years
N=89,006
N at risk at 25 years = 98
HEART TRANSPLANTATION Kaplan-Meier Survival (1/1982-6/2009)
ISHLTISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132

Common Immunosuppressive Regimen
Primary: cyclosporine / tacrolimus(utilized in conjuction with therapeutic drug monitoring)
Adjunctive: mycophenolate mofetil Supportive: prednisone (only 20 to 30% centers
wean prednisone off if possible) Additive: statins (shown to be immunomodulatory
and associated with improved long term survival)
26

Major Post Transplant Complications
Rejection Infection Cardiac allograft vasculopathy (CAV) Hypertension Nephrotoxicity Malignancy
27

Identifying Allograft RejectionDisease Progression
Alloimmune activation Cellular invasion
Multiple genes and pathways
Cellular inflamationand myocyte necrosis
Graft Dysfunction
Heart failure andarrhythmias
Diagnostic Indicators
Gene Expression ProfilingImmune Function Assays
Endomyocardial Biopsy(intermediate)
Functional Assessment(late)

Rejection
Invasive surveillance biopsies are the best established method for following patients
Typically 13-15 biopsies are done in the first year Each biopsy requires a minimum of 3 samples from
3 different sites to be meaningful
29

30
GRADE 1A
GRADE 2
GRADE 1B
Mild

31GRADE 4
GRADE 3A GRADE 3B
ThresholdMandatory
ForTherapy

Long Term Challenges
Renal failure and metabolic adverse effects
Cardiac allograft vasculopathy
Malignancy
32
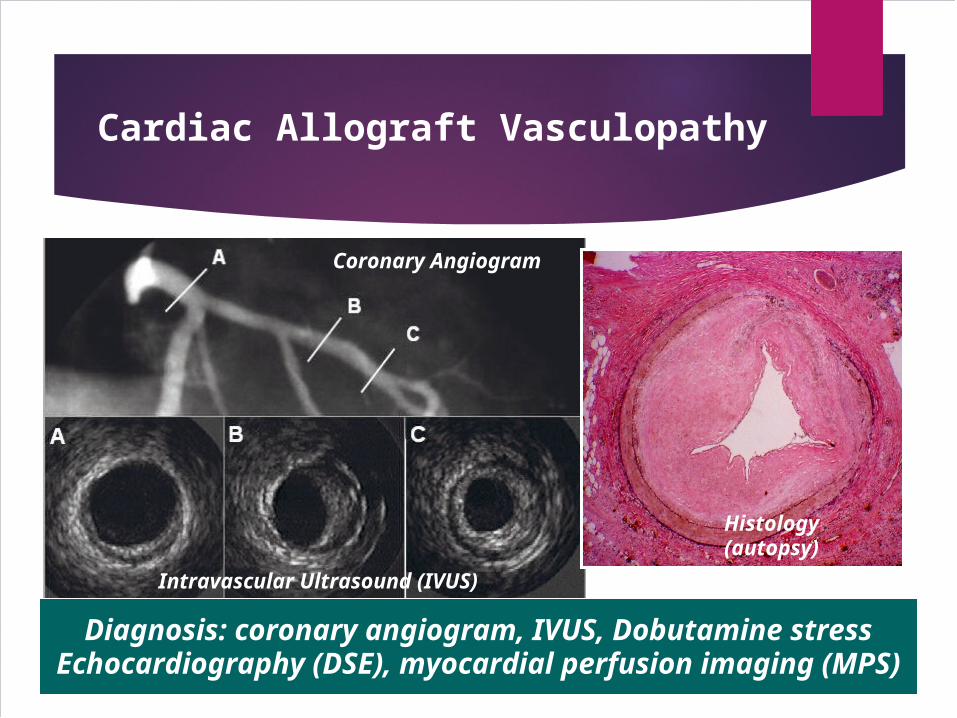
Cardiac Allograft Vasculopathy
Coronary Angiogram
Intravascular Ultrasound (IVUS)
Histology(autopsy)
Diagnosis: coronary angiogram, IVUS, Dobutamine stressEchocardiography (DSE), myocardial perfusion imaging (MPS)

VAD Components
Inflow cannula
Outflow Graft
Percutaneous drive line
Pump

HEART WARE
• Weigh 145 gms• Pumps 4-5 liter/min• No pocket required• Under clinical trial

Peripherals

37

Short-Term Extracorporeal Assist DeviceDevi
Levitronix CentriMag
Magnetically-levitated centrifugal pump Continuous-flow rotary pump Electrical actuation– magnetic coupling of
the motor and impellor Capable of 6 ~ 9 L/min at 5500 RPM Left, Right, or Biventricular support Operative placement requiring sternotomy Bridge to recovery
Courtesy of Levitronix, Inc.

Extra Corporeal Membrane Oxygenation ( ECMO)

www.kewalkrishan.com

Thank you