Embed Size (px)
DESCRIPTION
Keynote address by Dr. Eric Goosby of UCSF, presented at CFAR HIV Research in International Settings (CHRIS) meeting in San Diego, October 1, 2014. Dr. Goosby discussed. "Global Health Delivery and Diplomacy: The Long Road to Sustainable Programs."
Citation preview

CFAR: HIV Research in International Settings, UCSD !Oct 1, 2014
Eric P. Goosby, M.D. UCSF Global Health Sciences
GLOBAL HEALTH DELIVERY AND DIPLOMACY: The Long Road to Sustainable Programs

Ebola Western African Outbreak • Liberia 52% (3280/2917), Sierra Leone 30% (1940/597), Guinea 16% (1022/635), Nigeria (20/8), Senegal (1/0) – Timeline: December 1st to September 28th
• Total Cases: 6263 (Sept 28, 2014; Confirmed Cases:3487)
• Total Deaths: 2917
• DiagnosLc Tests: IgM ELISA, PCR, Viral Culture – AnLgen ELISA test
• Experimental Treatments: – Z-‐MAPP (monocolonal Ab) – NIAID/GSK’: Vaccine phase 1 end of August – Newlink/ DOD: Vaccine – Tekmira (RNA interferring parLcles) and Biocryst Pharma (BCX4430): AnLviral drug development

Applying proven systems practices and rigorous evaluation
methodologies to global health: a partnership between academia, private sector, citizens
and governments

There are diseases we know how to prevent, diagnose and treat effectively. The fact that we are not doing so is impacting millions of lives and costing billions of dollars around the world
WE KNOW WHAT WORKS!BUT WE ARE NOT!DELIVERING

Example: Maternal Deaths Although African countries reduced their overall maternal mortality ratio from 745 deaths per 100,000 live births in 1990 to 429/100,000 in 2010, the risk of an African mother dying during pregnancy or childbirth remains 20 times greater than the risk to American women. We have the tools to reduce maternal mortality, and have used them effectively in the west, but they need to be delivered and used in smarter ways in the developing world.
Too many lives will be lost if we wait another 20 years.
DISCREPANT RESULTS AROUND THE GLOBE ARE UNACCEPTABLE

We need to change the pace of progress against diseases causing the highest burden of disease in the developing world. Although there have been notable successes in reducing new infections and treating those with HIV and TB, they remain the leading two killers of adults between 15 and 50 in Africa. In addition, over 180,000 infants are newly infected with HIV every year during pregnancy and breastfeeding in the developing world, whereas in the US and Europe infant infections are now exceedingly rare because of successful preventive treatment programs. How can we encourage and promote development when TB and HIV are still ravaging the young and productive core of many African societies?
CHANGE THE PACE OF PROGRESS AGAINST DISEASE

Childhood diarrhea, hypertension, diabetes, cervical cancer and other illnesses have a similar stories… We can’t just focus on individual diseases and conditions…we need to build upon successful disease-specific responses and develop greater effectiveness across health systems.
OTHER ILLNESSES HAVE !SIMILAR STORIES

Science has given us the tools, but most development efforts take an inordinate amount of time to implement. This is not about throwing money at the challenge. We have failed to meet most of the MDG targets – despite all of our best efforts…
IT’S NOT JUST ABOUT MONEY

IT’S NOT ABOUT TIME
Years of global health efforts have not seen the development !of enough sustainable programs that have lasting impacts.

WE ARE IN A CONSTANT STATE OF EMERGENCY
PROGRAM FAILURE We see repeated start-up efforts for the same disease that never mature into an evolved response. Programs have not developed the rigorous real-time evaluation capabilities to allow for adjustments over time as needs change.
We can no longer afford to have a sequence of unsustainable emergency programs that fail to address local communities’ health priorities.

WE ARE NOT LEARNING FROM OUR FAILURES (OR OUR SUCCESSES)
PROGRAM FAILURE OR SUCCESS Programs finish, and whether they fail or succeed they are discontinued…there is scant attention paid to carefully embedding successful programs into sustainable national programs.
and no one is outraged

WE NEED TO CHANGE THE WAY WE THINK ABOUT HEALTH SYSTEMS DELIVERY

TO CREATE LOCALLY OWNED AND SUSTAINABLE SOLUTIONS

WHAT’S THE BIG IDEA?
Health systems need all four legs of the ‘delivery stool’ Combining health diplomacy, advocacy and delivery science through academic, civil society, private sector, & government partnerships.
Health Diplomacy & Advocacy
+ Delivery Science
Academia (Rigor)
Private Sector (Efficiency)
National & Local Government
(Management)
Community (Ownership)

HOW TO DO IT: INTEGRATING GLOBAL HEALTH DELIVERY ACROSS KEY SECTORS
HEALTH DIPLOMACY AND ADVOCACY! Constructive engagement with ministries of health and other key parties to identify health priorities, critical implementation issues and barriers to success.
THE PRIVATE SECTOR!!Harness the strengths and networks of business, investors and enterprise in both the global North and South to address the identified health priorities in partnership with government
ACADEMIA! Engage across schools of medicine, public health and the physical and social sciences to lower the barriers to applying the best science, data solutions, policies, technologies and management options for in-country implementation
NATIONAL AND LOCAL GOVERNMENT Draw upon and be led by government’s natural abilities to convene and lead health responses, and seek to grow government ownership
CIVIL SOCIETY & THE INDIVIDUAL! Working with civil society to address local health priorities and needs that will lead to programs focused around patient engagement
INTEGRATED HEALTH SYSTEMS DELIVERY

WHAT DIFFERENTIATES THE INSTITUTE:!the four legs of the stool
• A comprehensive perspective of the Institute’s leaders and their networks, grounded on the premise that the best results are those desired and sought by national and local governments their stakeholders and citizens.
• The importance of cultural, political and diplomatic forces on healthcare delivery systems, and have the expertise to address them with professional diplomacy and analytic rigor.
• A balance of power among: – Government contributes legitimacy and sustainability but lacks capacity. – The Private Sector is timely, efficient and contributes hands-on know-how, but has
no desire to share its learnings and create global public goods. – Academia does capacity-building, rigorous evaluation and shares lessons globally,
but has problems with timeliness, efficiency and hands-on know-how. – Local Community and Civil Society as key players in the health systems which both
need to be aligned with government and private sector priorities and ultimately will be involved in the sustainability of any health solutions developed.
• There are many institutions that have one leg of the delivery stool. A few have two legs. all four legs are are needed to effect transformational change that doesn’t just help one client but that serves as a model that enables change to propagate.

THREE!RESULTS
FIELD ACCELERATION
RESOURCE ALIGNMENT CHANGING SCIENCE & PRACTICE

KEY RESULT 1: FIELD ACCELERATION
ACCELERATED IMPLEMENTATION Reduce the time from engagement to self-correcting and sustaining systems EVIDENCE-BASED METRICS Define and implement a framework for evaluation to assess effectiveness as well as efficiency harnessed by real-time accessible data RESULTS TO POLICY Stay in the game with local stakeholders until sustained scale-up

KEY RESULT 2: RESOURCE ALIGNMENT
DONOR ALIGNMENT Alignment of large funding motors with capacity development and program sustainability at the local level (government and civil society), e.g. Global Fund , UNITAD, WHO, UN system, World Bank, PEPFAR and the Millennium Challenge Corporation, BMGF, Bilaterals (DFID, Point-7) INDUSTRY ALIGNMENT Alignment of strategy with key industry players and the investment community

KEY RESULT 3: CHANGING SCIENCE & PRACTICE
REPLICABILITY Across individual ministries, rapidly move pilot to scale up across country KNOWLEDGE TRANSFER Changes in behavior and funding among other ministries and donors SYSTEMS BEST PRACTICE Collate and harvest country generated system tools that may be applied in other settings LEADERSHIP ECOSYSTEM: Create a cadre of expertise that may serve as technical assistance resources for the region

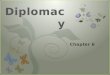
Successful task shifting: More efficient use of human resources. Significant savings in treatment: Cost of annual antiretroviral therapy reduced from $1400 per person to $335.* Massive expansion of treatment: Over the last 3.5 years, from 1.7 million to 6.7 million people.* *Ref: PEPFAR 2013 program data
WE KNOW IT WORKS: 1. Evidence-based acceleration: Optimizing PEPFAR programs " by linking expenditures " to outcomes
73% Reduction in costs

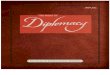
RWANDA HAS DEVELOPED A SYSTEM THAT RECEIVES DIVERGENT RESOURCES: Multiple donors and the Government of Rwanda apply funds to unmet needs with one planning process, allowing the divergent funds to be additive while still maintaining transparency and auditability. Sophisticated information systems create feedback loops that inform decision-makers. Civil society involvement in planning and implementation is growing.
WE KNOW IT WORKS: CASE STUDY RWANDA : 2. Resource alignment
RWANDA HAS ACHIEVED: 90% ART coverage 89% PMTCT ART initiation >85% drop in HIV incidence, 45% drop in Death Rwanda’s health budget is:
>90% from external donors Rwanda’s health budget is:
100% managed by the Government of Rwanda They define and prioritize unmet need and make allocation decisions.

Building from what we know works: from key results to robust health delivery systems (7examples) A government struggles to equitably improve health outcomes across regions with variable leadership and diverse economic status. Effective Global Health must bring together diplomatic and delivery elements: • Proven health interventions with well understood delivery system requirements and economics. • Strategies drawn from political science, anthropology, urban planning and business strategies
(through geo-mapping and surveys, combined with cost and health impact projections of targeted intervention strategies) delivered in partnership between the MOH system and in-country academic colleague and civil society.
• Proven and stable mobile enabled e-health technologies for diagnosis, monitoring and logistics, backed by commercial infrastructure and funding.
• Application of market research expertise (real-world consumer analytics to understand supply and demand failures, and to create and test strategies for improvement).
• Behavioral economics (rigorous academic evaluation of potential societal drivers of the market failure and consideration of economic incentives, such as pay for performance).
• Quality improvement (promotion and support for quality improvement cycles and management training).
• Large scale impact evaluation to demonstrate the effectiveness and efficiency of a new intervention package to improve outcomes.

3. Changing science and practice: The backbone of an effective Global Health model uses innovative programs based on existing technologies and interventions that work with communities and a strengthened healthcare referral system. !
Innovation Through Delivery
HOW DOES THE WORLD CHANGE?

AN INTEGRATED TEAM An integrated vision needs more than public health expertise. We are assembling a world class team of experts from across public health, industry, investment, communications, appropriate technology, policy and diplomacy, collaboration and innovation and are linking to local efforts.
TEAM | SOLVING PROBLEMS TOGETHER

GETTING IT DONE Determinants of Performance

Objective: Institute for Global Health Delivery and Diplomacy
24 MONTH OBJECTIVE | DEMONSTRATION Build a model demonstration laboratory

A DIFFERENT BUSINESS PLANNING APPROACH… We are proposing a collaborative business planning process, working together with foundations, multilateral partners, government ministries, communities, corporations and NGOs to understand what a truly integrative process would need to look like to succeed.
PLANNING TOGETHER

PLANNING TIMELINE
4 Months 18 Months
Design Feedback Systems
KEEP PLANNING THROUGH BETA
Take the integrated delivery model into two test countries where we have relaLonships with ministries [Ethiopia,
Kenya, Uganda, Rwanda and Zambia]. Take on one or two medical condiLons and gather iniLal data on effecLveness
REPLAN Use the year one
beta phase as data to re-‐engineer the
parameters of the insLtute
Evaluate for
Impact
Design on Demonstrable
Success
SYSTEM DESIGN Engage global
stakeholders from across the system to
understand needs and co plan the
institute
24 Months
A ROAD TEST TO REFINE OUR MODEL 24 Month Process

MODEL EXPLORATION: The proposed collaborative business planning process has resulted in a flexible model. Opportunities exist for traditional research institute funding as well as hybridized business models downstream including consultative services to national governments and donors. The plan will be refined with partners during the first phase of planning.
FINDING A MODEL

COLLABORATORS…
INTEGRATION DEPENDS ON COLLABORATION This work will require a variety of specialized partnership ecosystems – at the local, national and international levels. Partnerships will straddle industry, government, communications, public relations and civil society, however we expect that specific partnership needs will be emergent based on the business planning process. We have developed a sophisticated partnership engagement process for both planning and implementation.

PARTNERS
UNUSUAL PARTNERSHIP EXPLORATIONS: We have already begun a series of partnership explorations including partners from multiple schools (UCSF, UCB SPH, UCSD, UCLA, UCD) and academic disciplines as well as institutional partners that include the WHO, UN, The World Bank, Clinton Health Access Initiative, Bloomberg Foundation. ELMA Foundation the Governments of Kenya, Uganda, Ethiopia and Rwanda. We have made a commitment to DESIGN FIRST and understand partnership needs based on a more evolved set of objectives and outcomes.

• Zambia • Ethiopia • Rwanda • India • South Africa • Malawi • Zimbabwe • Uganda • Kenya
OUR INITIAL CONSORTIA OF INTERNATIONAL PARTNERS

Acknowledge the ContribuLons
• Nancy Padian • Stefano Bertozzi • Diane Havlir • Monica Ghandi • Charles Holmes • Elvin Geng • Jeff Hamaoui • Michael Kleeman
• Todd Khozein • Eliah Aronoff-‐Spencer • Deborah Von Zinkernagel • Anthony Fauci • Amy Lockwood • Jaime Sepulveda • David McKey • Julia MarLn
Improving health and reducing inequities worldwide

Eric Goosby, M.D. Professor of Medicine Global Health Sciences
PosiLve Health Program SFGH/Wd 86 UCSF School of Medicine
[email protected] +1 415 476-‐5483
THANK YOU
Improving health and reducing inequities worldwide