Embed Size (px)
Citation preview
Evidence Based Medicine
Presenter : Dr. Suhasini K.Dept. Community MedicineJ.N.M.C., Belagavi
23 January 2015 1Evidence Based Medicine
Heading
• Introduction
• Definition of Evidence Based Medicine
• Evidence-based health care practice
• Importance of EBM
• Evolution of EBM
• Decision making in EBM
• Five-Step Approach to Practicing EBM
• Benefits of adopting EBM
• Misconceptions in EBM
• Evidence-based Public Health
• Conclusion
23 January 2015 Evidence Based Medicine 2
Which doctor do you want?
23 January 2015 3Evidence Based Medicine
Which doctor do you want?
23 January 2015 4Evidence Based Medicine
Bloodletting
3000years ago
Egyptians, Greeks then Romans, Arabs and so on.
The cure for (hot, moist diseases) several medical conditions.
Galen was able to propagate his ideas through the force of personality and the power of the pen
23 January 2015 5Evidence Based Medicine

Pierre Louis (1787-1872)Inventor of the “numeric method” and the “method of
observation”
French physician who wanted to analyze the efficacy of bloodletting in the treatment of acute pneumonia
Examined the clinical
course and outcomes of 77 patients
23 January 2015 6Evidence Based Medicine
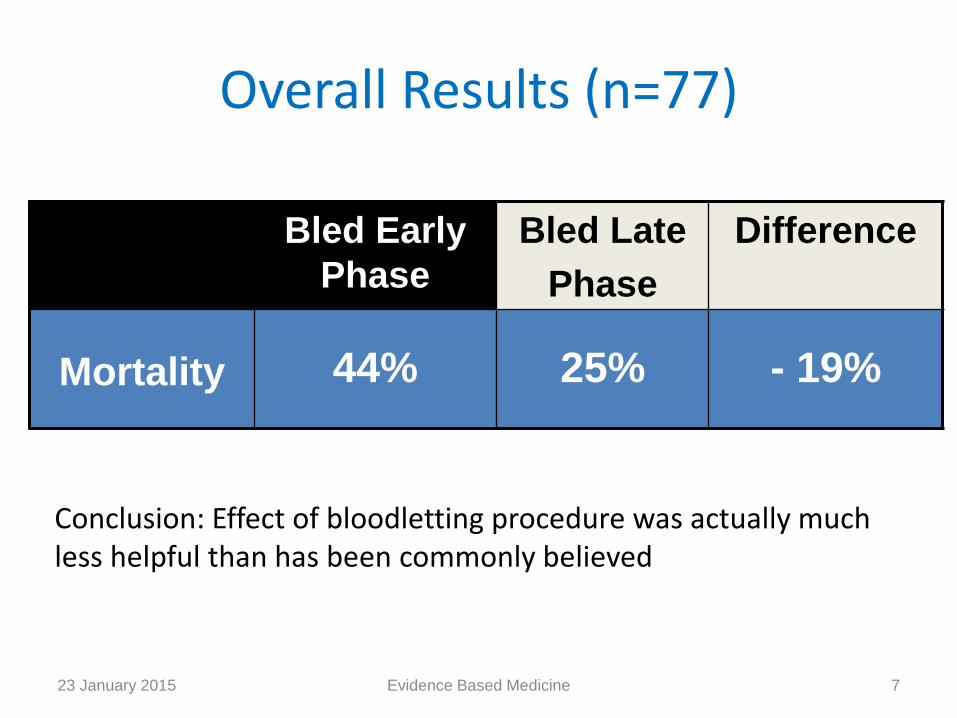
Overall Results (n=77)
“Experimental”
oup
Comparision
Group Absolute
Risk Reduction
Bled Early
Phase
Bled Late
Phase
Difference
Mortality 44% 25% - 19%
Conclusion: Effect of bloodletting procedure was actually much less helpful than has been commonly believed
23 January 2015 7Evidence Based Medicine

William Osler (1849 -1919)First “attending physician” at Johns Hopkins
Author of hugely influential textbook, 'The Principles and Practice of Medicine'believed that most drugs in his day were useless, but still advocated blood-lettingin some cases
23 January 2015 8Evidence Based Medicine
Bloodletting todayToday phlebotomy therapy is primarily used in Western medicine for a few conditions such as hemochromatosis, polycythemia vera, and porphyriacutanea tarda.
Why did it persist?It resulted from the dynamic interaction of social, economic, and intellectual pressures, a process that continues to determine medical practice
23 January 2015 9Evidence Based Medicine
But….
We practice EBM today
23 January 2015 10Evidence Based Medicine

Patient: Mr. A
Mr. A is a 60 year old presenting with 1 hour of retrosternal chest pain. ECG shows lateral ST-elevation consistent with acute MI.
QUESTION: In patients with acute MI,
does treatment with aspirin reduce mortality?
What is the best evidence?
23 January 2015 11Evidence Based Medicine
Evidence: 1988
• Reduction of mortality in acute myocardial infarction with streptokinase and aspirin therapy. Results:
– Patients with acute MI treated with Aspirin vs. placebo had a significant 23% relative risk reduction in five-week cardiovascular mortality, with an absolute risk reduction of 11.8% to 9.4%
– The combination of SK and Aspirin resulted in a 42% relative risk reduction in cardiovascular mortality after five weeks compared with the placebo
23 January 2015 12Evidence Based Medicine
Application: 1997• How many patients receive ASA following acute
myocardial infarction?
– Aspirin was not given to 55%!!!
– 78% of patients who did receive aspirin received it more than 30 minutes after arrival to the emergency department.
Annals of Intern Medicine. Jul 1997;127(2):12623 January 2015 13Evidence Based Medicine
• But as late as 2000, even in the US, aspirin was being prescribed for at most one third of patients with coronary artery disease (for whom there were no contraindications to its use)
• Relatively simple, and cheap practices shows that we have a problem in getting providers to apply knowledge gained through research
• The paradigm for the translation of new information from research bench to bedside has been conceptualized as a “translational highway”.
23 January 2015 14Evidence Based Medicine
What is evidence-based medicine?
“Evidence-based medicine is the integration of best research evidence with clinical expertise and patient values”
- David Sackett
• “Explicit, judicious, and conscientious use of current best evidence from medical care research to make decisions about the medical care of individuals”
23 January 2015 15Evidence Based Medicine
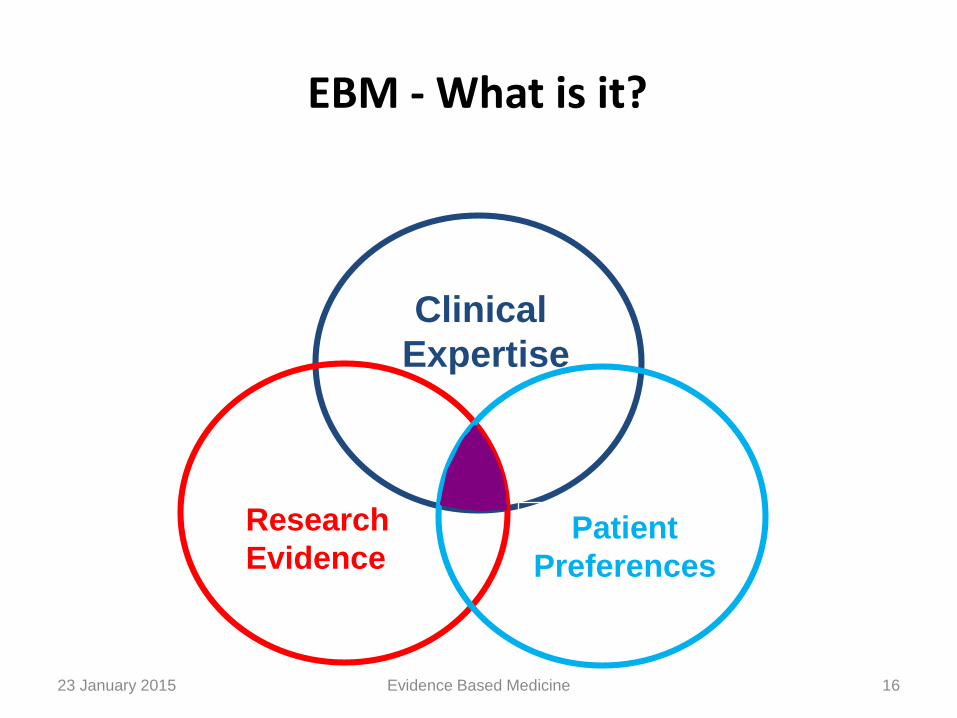
EBM - What is it?
Clinical
Expertise
Research
EvidencePatient
Preferences
23 January 2015 16Evidence Based Medicine
Evidence-based health-care practice
• The integration of:
– individual clinical expertise
– best available external clinical evidence from systematic research
Evidence Based Medicine 1723 January 2015
I - Individual clinical expertise
• Skills
• Judgement
– which individual health care workers acquire through
– clinical experience and clinical practice
Evidence Based Medicine 1823 January 2015
II - Best available clinical evidence
• Clinically relevant research derived from:
– basic medical sciences and
– patient-centred clinical research into the safety and efficacy of therapeutic interventions.
– Systematic Reviews
Evidence Based Medicine 1923 January 2015

Why is EBM important?
New types of evidence are being generated which can create changes in the way patients are treated
Although evidence is needed on a daily basis, usually physicians don’t get it.
How much is actually being applied to patient care?
lack of time
out-of-date textbooks
the disorganization of the up-to-date journals
23 January 2015 20Evidence Based Medicine
Importance of EBM for practicing clinicians?
TIME AVAILABLE TO READ:
Less than
1 Hour per Week
TIME NEEDED TO KEEP CURRENT
ON GENERAL MEDICINE:
19 Articles per DAY
365 Days per Year
Source: Davidoff F, Haynes B, Sackett D, Smith R. BMJ. 1995;310:1085-1086.
21Evidence Based Medicine
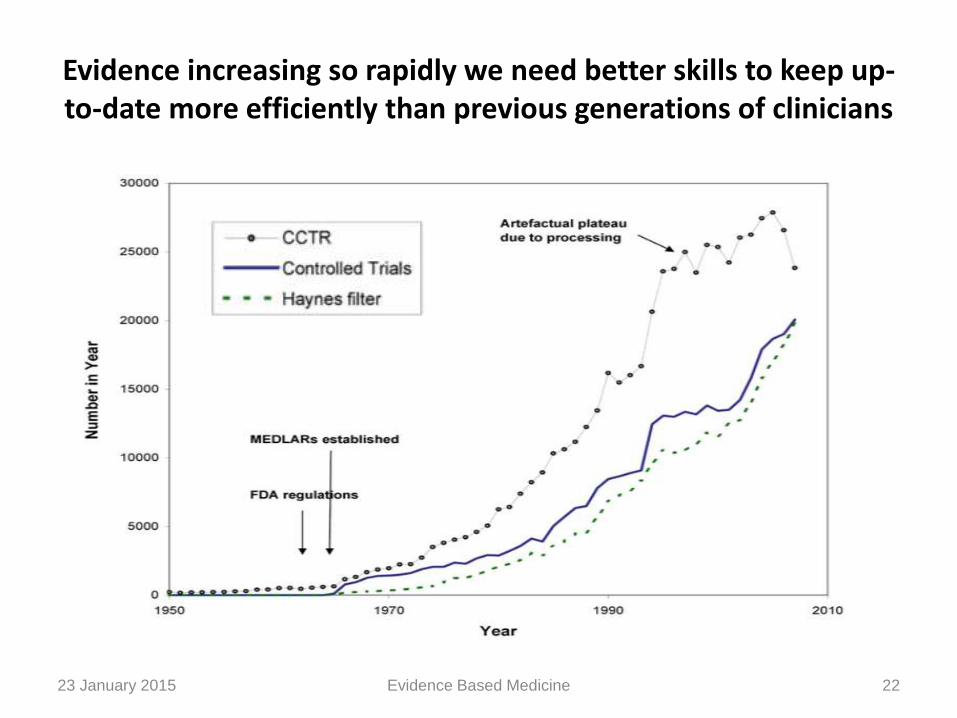
Evidence increasing so rapidly we need better skills to keep up-to-date more efficiently than previous generations of clinicians
23 January 2015 22Evidence Based Medicine
0
500000
1000000
1500000
2000000
2500000
Biomedical MEDLINE Trials Diagnostic?
Me
dic
al A
rtic
les
pe
r Y
ea
r
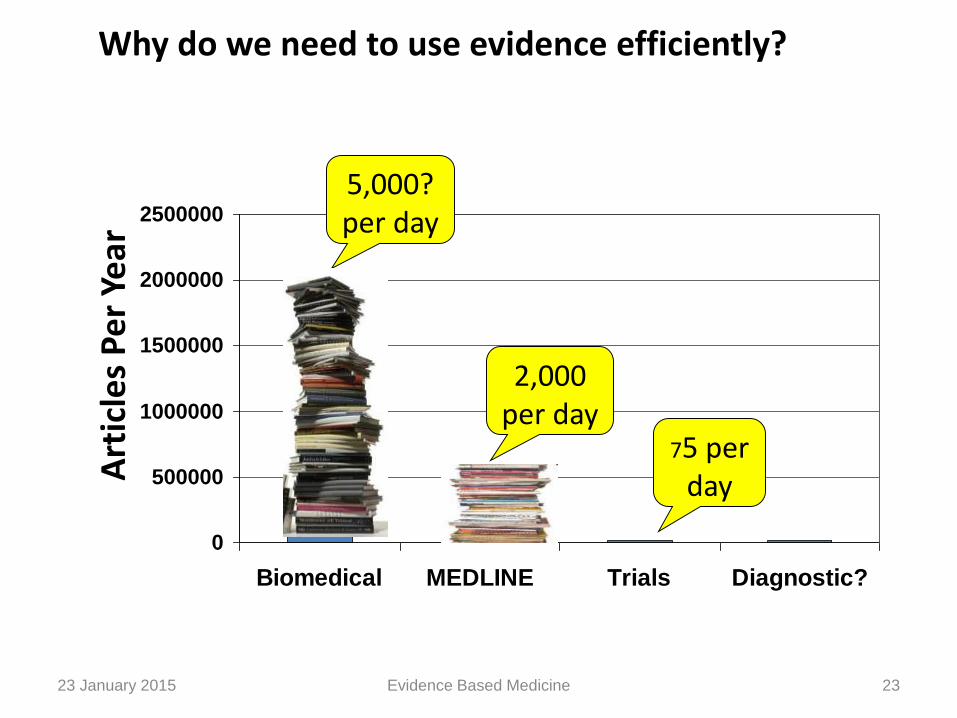
5,000?per day
2,000 per day
75 per dayA
rtic
les
Pe
r Ye
ar
Why do we need to use evidence efficiently?
23 January 2015 23Evidence Based Medicine
Time-poor clinician suffering from Information Overload
23 January 2015 24Evidence Based Medicine

Gets worse with “duration in practice”
23 January 2015 25Evidence Based Medicine
Evolution of EBM
Pre EBM: Passive diffusion (“publish it and they will come”)
Early EBM: Pull diffusion (“teach them to read it and they will come”)
Current EBM: Push diffusion (“read it for them and send it to them”)
Future EBM: Prompt diffusion (“read it for them, connect it to their individual patients”)
23 January 2015 26Evidence Based Medicine
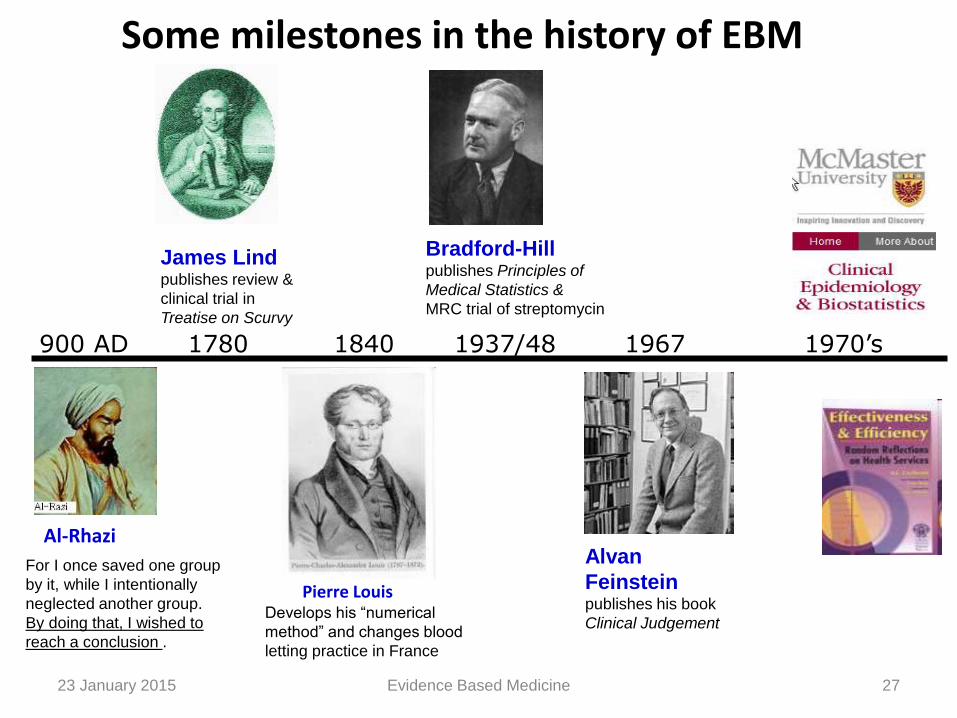
For I once saved one group
by it, while I intentionally
neglected another group.
By doing that, I wished to
reach a conclusion .
Al-Rhazi
900 AD 1780 1840 1937/48 1967 1970’s
Alvan
Feinsteinpublishes his book
Clinical Judgement
James Lindpublishes review &
clinical trial in
Treatise on Scurvy
Pierre LouisDevelops his “numerical
method” and changes blood
letting practice in France
Bradford-Hillpublishes Principles of
Medical Statistics &
MRC trial of streptomycin
Some milestones in the history of EBM
23 January 2015 27Evidence Based Medicine
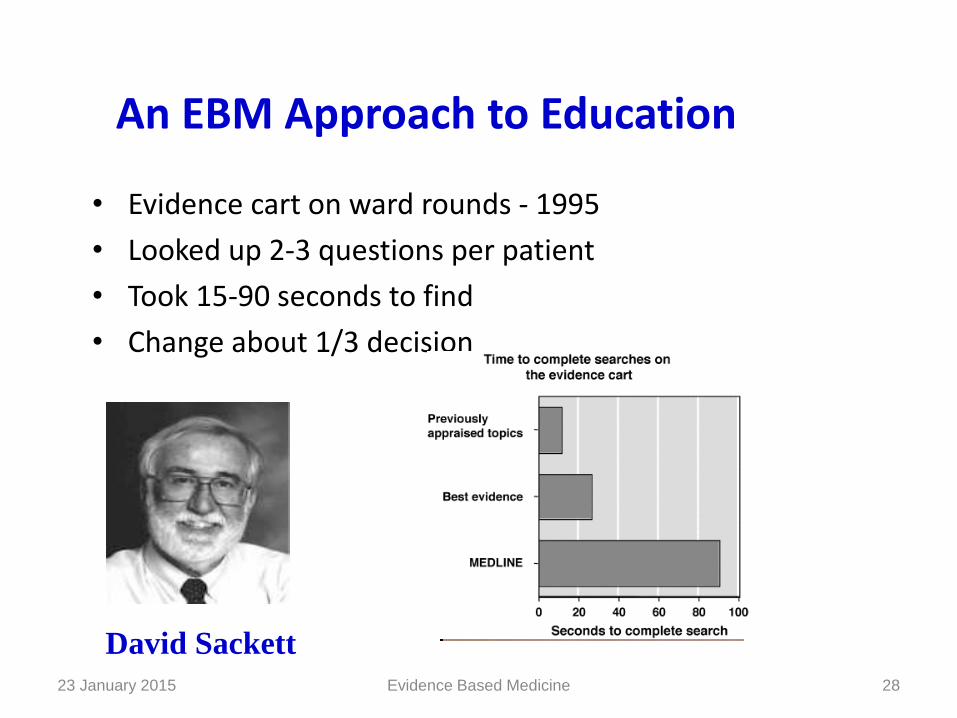
An EBM Approach to Education
• Evidence cart on ward rounds - 1995
• Looked up 2-3 questions per patient
• Took 15-90 seconds to find
• Change about 1/3 decision
David Sackett
23 January 2015 28Evidence Based Medicine
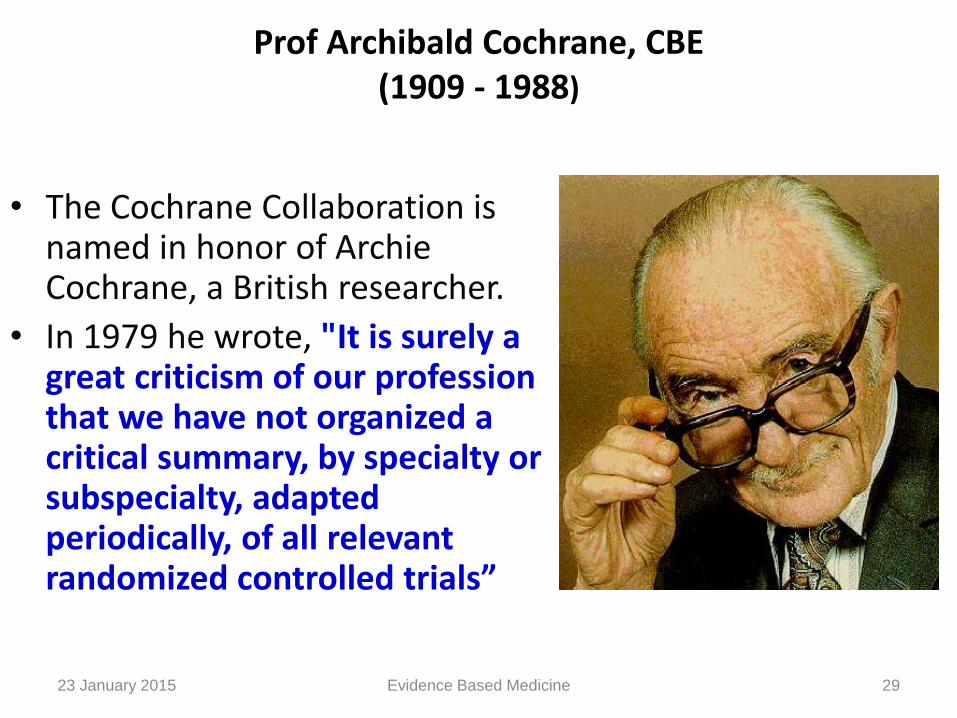
Prof Archibald Cochrane, CBE (1909 - 1988)
• The Cochrane Collaboration is named in honor of Archie Cochrane, a British researcher.
• In 1979 he wrote, "It is surely a great criticism of our profession that we have not organized a critical summary, by specialty or subspecialty, adapted periodically, of all relevant randomized controlled trials”
23 January 2015 29Evidence Based Medicine

Why the sudden interest in EBM?
• Increasing realization among clinicians that years of experience unaccompanied by updating of knowledge can result in decline of clinical performance
• The need for valid information about diagnosis, therapy, prognosis, and prevention in this era of consumer activism
23 January 2015 30Evidence Based Medicine

• The common man has access to the very same medical literature as the clinicians through numerous sources
• Limited time available to the clinician for acquiring information is a major impediment for updating the knowledge from traditional sources
23 January 2015 31Evidence Based Medicine
Assumptions of evidence-based practices
• Not all evidence is equivalent
• There is a hierarchy of study design
• External evidence can inform but can never replace individual clinical expertise (Sackett et al., 1996)
• Starting from the best external evidence and work from there.
• Values always influence decisions
23 January 2015 32Evidence Based Medicine
Where do we go for help with decisions when we are not sure how to proceed?
23 January 2015 Evidence Based Medicine
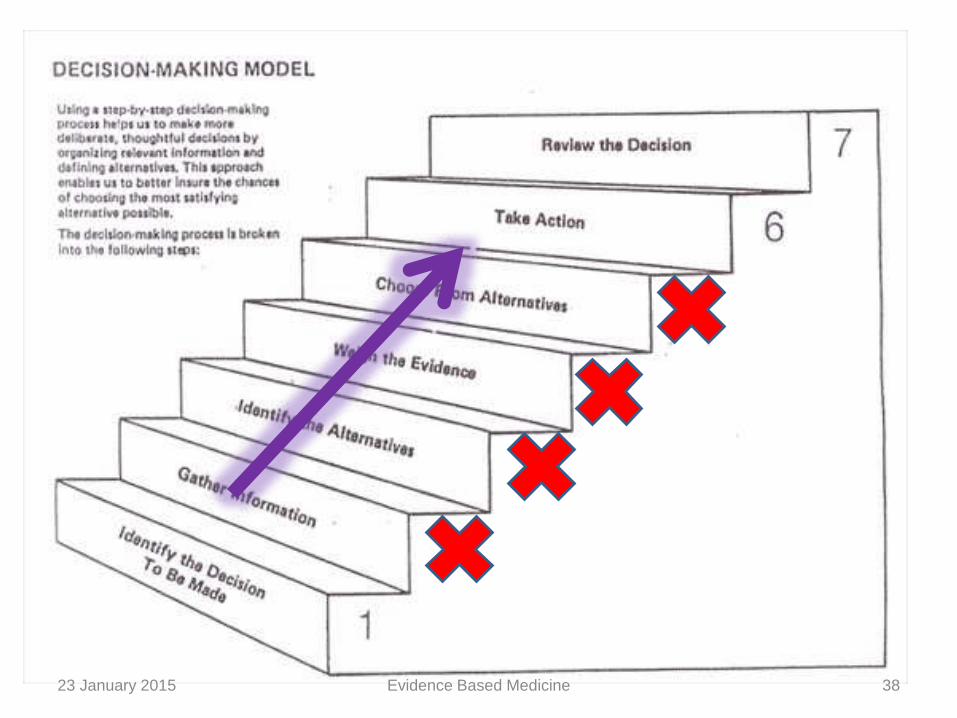
Decision making in clinical practice using evidence
Decision-making is the cognitive process resulting in the selection of a course of action among several alternative possibilities
23 January 2015 Evidence Based Medicine
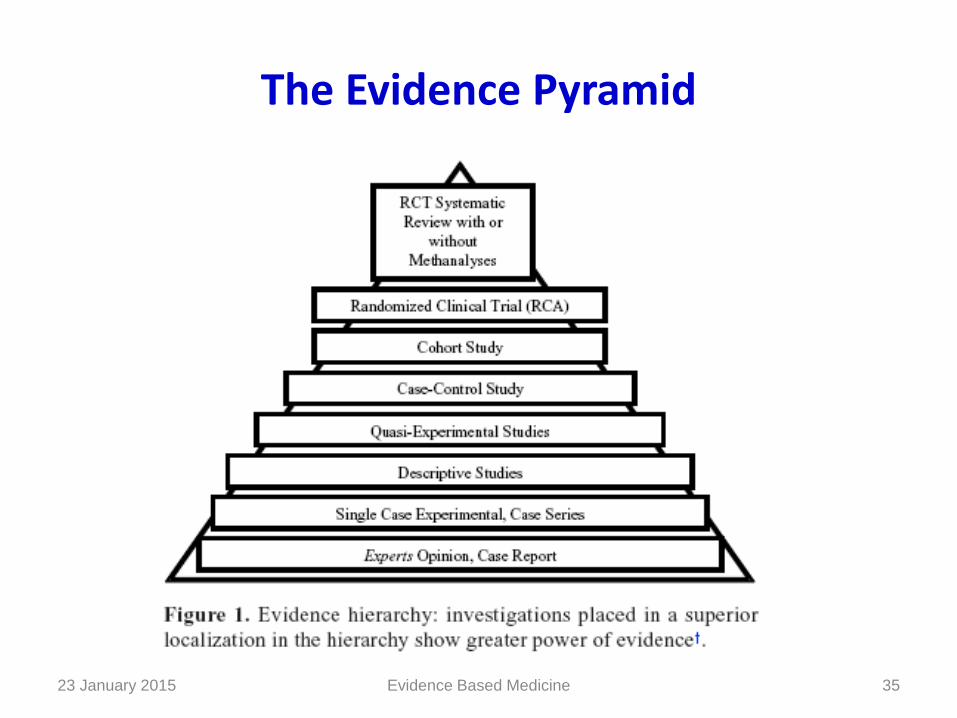
The Evidence Pyramid
23 January 2015 35Evidence Based Medicine

Type of Question Suggested best type of Study
Therapy RCT>cohort > case control > case series
Diagnosis Prospective, blind comparison to a gold standard
Etiology/Harm RCT > cohort > case control > case series
Prognosis Cohort study > case control > case series
Prevention RCT>cohort study > case control > case series
Clinical Exam Prospective, blind comparison to gold standard
Cost Economic analysis
Identifying the Best Study
23 January 2015 36Evidence Based Medicine
23 January 2015 37Evidence Based Medicine
23 January 2015 38Evidence Based Medicine

So in clinical practice
Disease
Treatment
options
23 January 2015 39Evidence Based Medicine
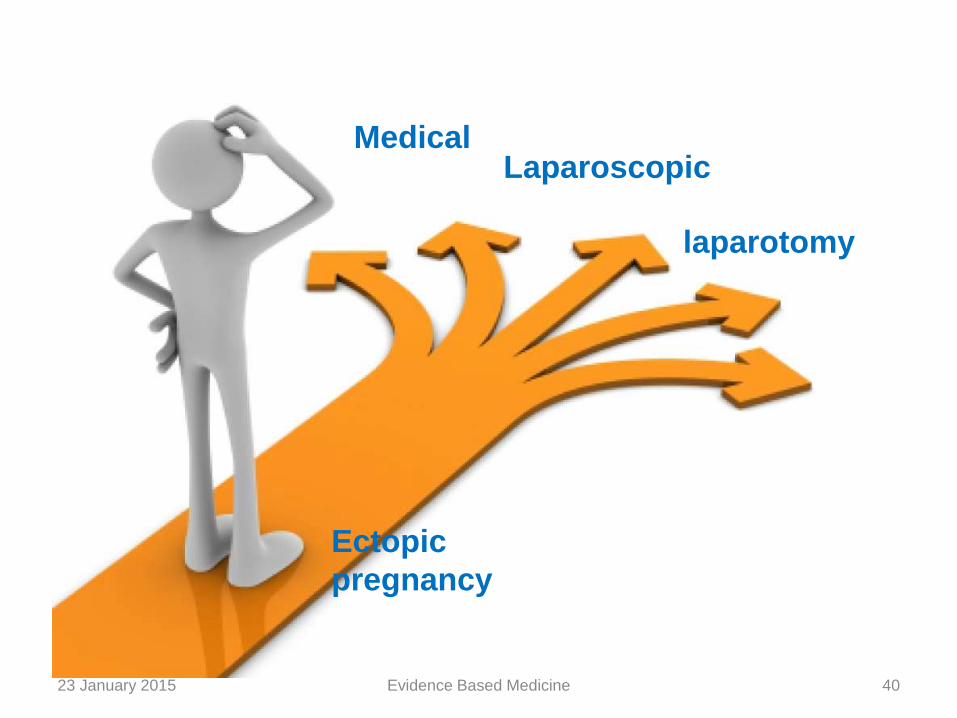
Ectopic
pregnancy
MedicalLaparoscopic
laparotomy
23 January 2015 40Evidence Based Medicine
Outcome – the only thing that matters
23 January 2015 41Evidence Based Medicine

What EBM additionally provides is
Opportunity for change Opportunity for better treatment
23 January 2015 42Evidence Based Medicine

How evidence affects clinicians
•Happy !!!
•I am the best !!!
•Will the patient recover or
not??
•Will they sue me??
•What about my reputation ??23 January 2015 43Evidence Based Medicine

23 January 2015 44Evidence Based Medicine
Think 100 times before refuting an old time tested method of treatment
• Classic example is vaginal hysterectomy for benign diseases
• “Give me 2 retractors, 2 scissors , 2 clamps, one tissue holding forceps and one needle holder, I will do a vaginal hysterectomy in any setup”
Surgeon
23 January 2015 45Evidence Based Medicine
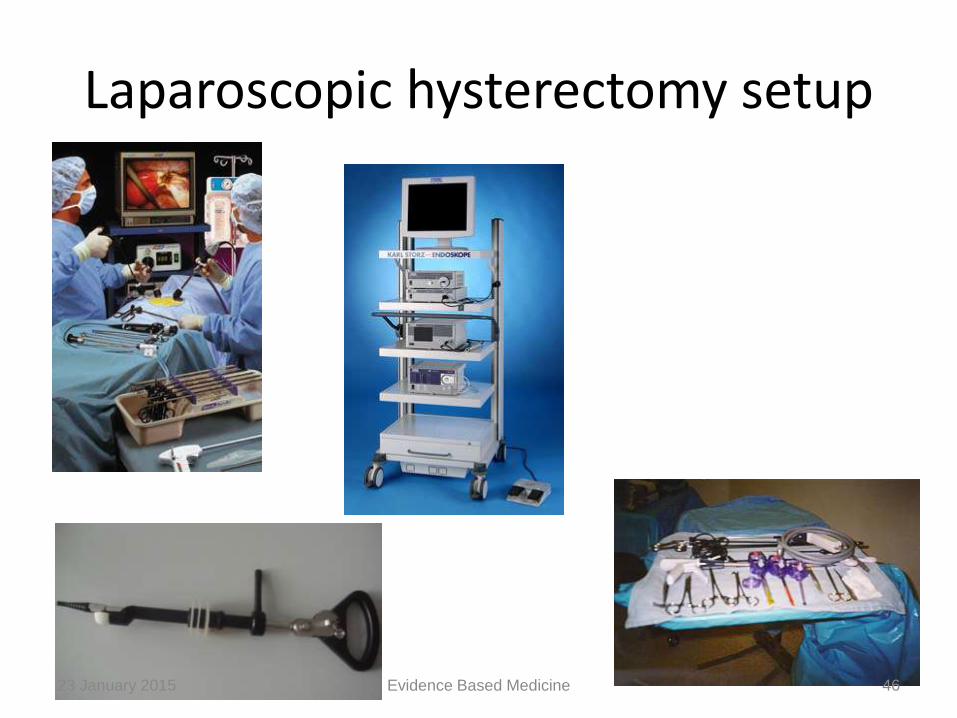
Laparoscopic hysterectomy setup
23 January 2015 46Evidence Based Medicine
• New developments ( unnecessary) in minimally invasive surgery
• Studies sponsored by pharma companies
• Use of meshes in different clinical conditions
• Mesh Erosion in bladder or bowel, infection or rejection of mesh, vaginal pain or painful intercourse, groin infection/abscess, extrusion , obstruction , voiding dysfunction and erosion.
23 January 2015 47Evidence Based Medicine

Changes in clinical practice shouldn’t be like this
23 January 2015 48Evidence Based Medicine
Changes should be like this
23 January 2015 49Evidence Based Medicine

The Five-Step Approach to Practicing EBM
• Step 1- Framing a Proper, Pertinent, Focused and Answerable Question
• Step 2 - Searching the Literature
• Step 3 - Critical Appraisal of the Literature
• Step 4 –Integrating the Evidence with Clinical Expertise and Patient Values
• Step 5 – Evaluating the Process23 January 2015 50Evidence Based Medicine
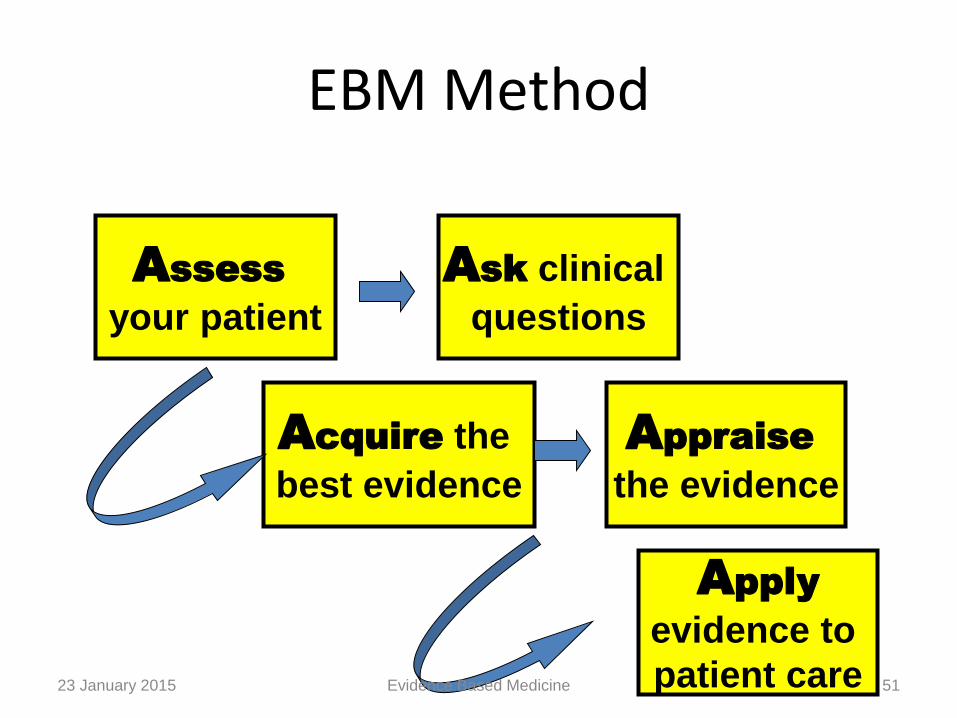
Acquire the
best evidence
Appraise
the evidence
Apply
evidence to
patient care
Assess
your patient
Ask clinical
questions
EBM Method
23 January 2015 51Evidence Based Medicine
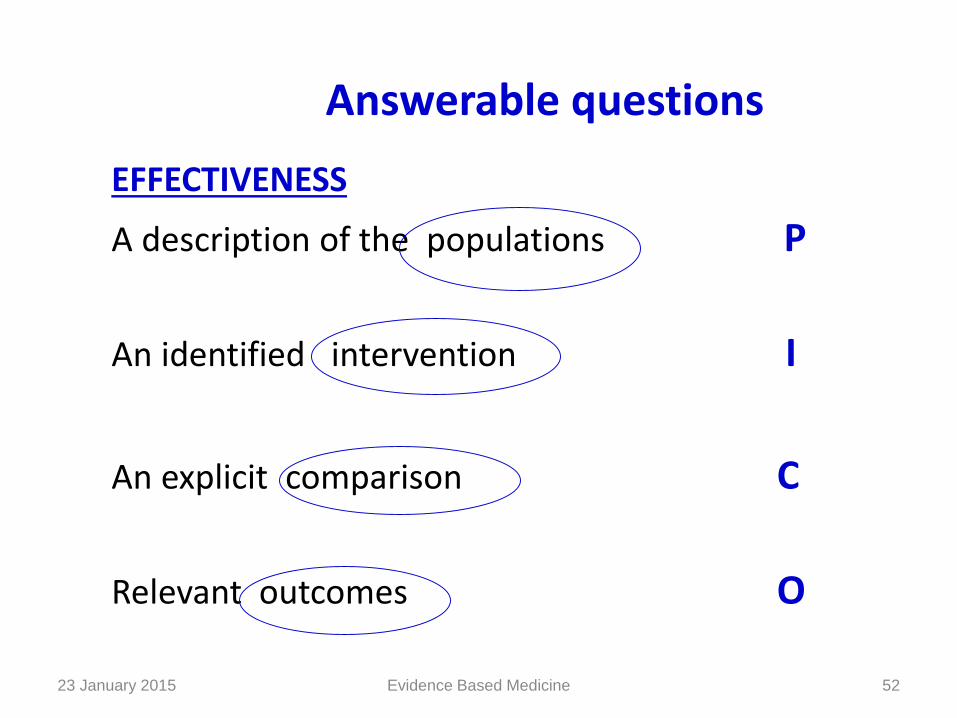
Answerable questions
EFFECTIVENESS
A description of the populations P
An identified intervention I
An explicit comparison C
Relevant outcomes O
23 January 2015 52Evidence Based Medicine
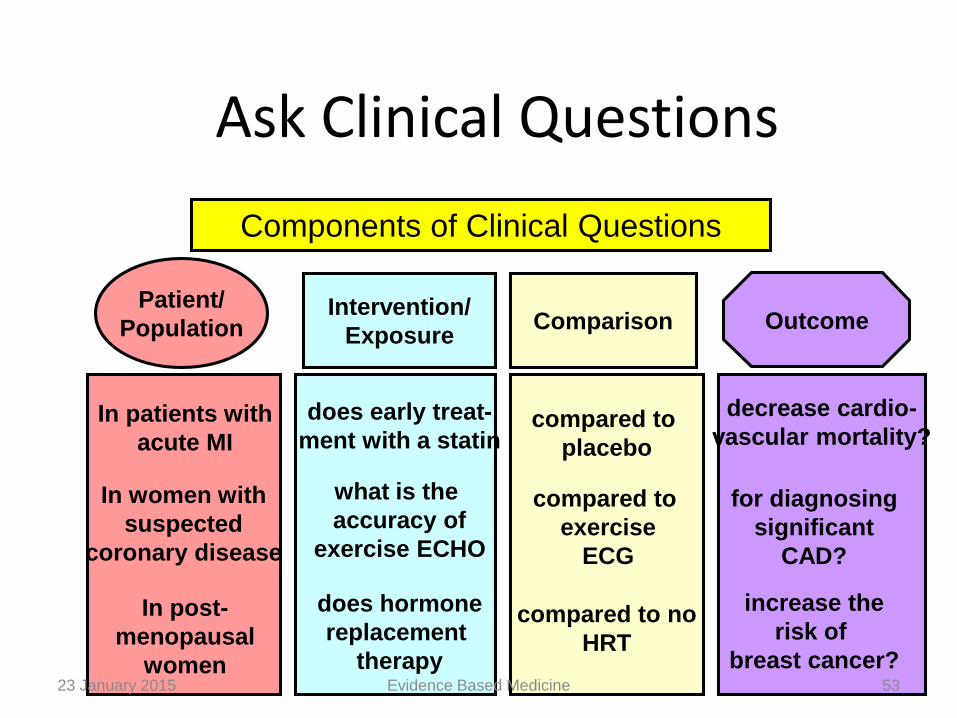
Ask Clinical Questions
Patient/
Population OutcomeIntervention/
ExposureComparison
Components of Clinical Questions
In patients with
acute MI
In post-
menopausal
women
In women with
suspected
coronary disease
does early treat-
ment with a statin
what is the
accuracy of
exercise ECHO
does hormone
replacement
therapy
compared to
placebo
compared to
exercise
ECG
compared to no
HRT
decrease cardio-
vascular mortality?
for diagnosing
significant
CAD?
increase the
risk of
breast cancer?23 January 2015 53Evidence Based Medicine
Step-1
Clinical Scenario :
• 12 years old only male child
• admitted to ICU
• history of accidental ingestion of OP compound 4 hours back
• On admission the patient was comatose but hemodynamically stable
23 January 2015 54Evidence Based Medicine
• The anaesthesiologist used his past experience, knowledge, skill & expertise and treated the patient with an infusion of atropine
• Inspite of that patient developed respiratory paralysis in the next 2 hours
• The clinician used his expertise puts him on mechanical ventilation
23 January 2015 55Evidence Based Medicine
• Now, the consultant understands the gap in his knowledge & he identifies the same.
• The consultant wanted to administer Inj Pralidoxime.
• But he was not sure of the dosage and the mode of administration (a single bolus dose or an infusion).
23 January 2015 56Evidence Based Medicine

• ‘P’ — Patient Problem: How would I describe a group of patients similar to mine?
In this clinical situation it is a male pediatric patient (12 years) who has developed organophosphorouspoisoning following its ingestion.
• ‘ I ’ — Intervention strategy: Which main intervention, prognostic factor or exposure am I considering?
Here the intervention is the therapy with Pralidoxime in optimum dosage.
23 January 2015 57Evidence Based Medicine
• ‘C’ — Comparison: What is the main alternative to compare with the intervention?
In his patient the clinical dilemma pertains to the dosage and mode of administration of Pralidoxime(low dose infusion vs. single large bolus dose)
• ‘O’ — (Outcome): - What can I hope to accomplish?
Recovery from OP poisoning and decrease in morbidity & mortality
23 January 2015 58Evidence Based Medicine
Step-2 Literature Search
• ‘Traditional’ print resources like textbooks or journals
• ‘Browse’ online electronic databases
23 January 2015 59Evidence Based Medicine
Step 3 - Critical Appraisal of the Literature
1. Screening for internal validity and relevance
2. Determining the intent of the article
3.Evaluating the validity based on its intent
23 January 2015 60Evidence Based Medicine
• The article that was tracked down is Prospective randomized placebo controlled clinical trial of Pralidoxime in two similar groups of patients. (Control group-low dose and study group-high dose)
• Block randomization was used
• The investigators were not blinded
23 January 2015 61Evidence Based Medicine
• The intent of the article is to evaluate two treatment regimes of PAM in the management of OP poisoning
• The next thing to determine is the strength of the outcome. How large was the treatment effect?
• Low dose group fared better than high dose group
23 January 2015 62Evidence Based Medicine
• PAM is a very expensive imported drug requiring considerable amount off foreign exchange and there are difficulties in procuring it.
• It is imperative for the clinician to find a cost-effective
• and yet effective treatment.
• Patient’s father, being a primary school teacher, cannot afford the exuberant cost of the drug.
• The out come of this research study is very much relevant and beneficial in solving the clinical dilemma
23 January 2015 63Evidence Based Medicine
Step 4 –Integrating the Evidence with ClinicalExpertise and Patient Values
• The best documented critically appraised research evidence is already with the clinician
• Take into consideration the patient values for example:
The patient is a precious, lone male child of the
parents.
The economical/financial status of the parents does not permit expensive therapies
No contraindications for the drug to be administrated
Low dose regime requiring 1/16 of the high dose has better effect
23 January 2015 64Evidence Based Medicine
Step 5 – Evaluating the Process
• Was he able to formulate a focused question?
• Was he able to devise a precise search strategy for locating the evidence?
• Did he use the most appropriate resource?
• Were more pertinent resources like practice guidelines available to him?
• Did the ‘evidence’ work in his patient?
• The clinician should document the outcomes of the application of the evidence and based on his experiences
• Those of his colleagues should be able develop management protocols
23 January 2015 65Evidence Based Medicine
What are the benefits of adopting EBM?
• Minimize the errors in patient care
• Reduces the cost of treatment to the patient
• Optimizes the quality of patient care
• Skills learnt in practicing EBM are the very same ones needed for being a lifelong, self-directed learner
• Habit of accessing literature on a daily basis is the best guarantor of ensuring advancement of knowledge and keeping abreast of scientific progress
23 January 2015 66Evidence Based Medicine
EBM Misconceptions
FALLACY FACT
EBM is useless when
there is no good
evidence
EBM means
appropriately using the
best available evidence
to care for patientsEBM is algorithms that
ignore clinical judgment/expertise
Clinical judgment must be
used in deciding how to apply the evidence
EBM is just numbers
and statistics
EBM is not numbers in a
vacuum – the evidence
must be individualized to
each patient23 January 2015 67Evidence Based Medicine

Who benefits?
Practitioners current knowledge to assist with decision making
Researchers reduced duplication identify research gaps
Community recipients of evidence-based interventions
Funders identify research gaps/priorities
Policy maker current knowledge to assist with policy formulation
23 January 2015 68Evidence Based Medicine

Evidence-based Public Health
• “The development, implementation, and evaluation of effective programs and policies in public health through application of principles of scientific reasoning, including systematic uses of data and information systems, and appropriate use of behavioral science theory and program planning models”
Source: Brownson, R.C. et al, Evidence-based public health, Oxford University Press, 2003.
23 January 2015 69Evidence Based Medicine

Clinical vs. Public health interventions
Clinical
• Individuals
• Single interventions
• Outcomes only (generally)
• Often limited consumer input
• Quantitative approaches to research and evaluation
Public health
• Populations and communities
• Combinations of strategies
• Processes as well as outcomes
• Involve community members in design and evaluation
• Qualitative and quantitative
• Health promotion theories and beliefs
Evidence Based Medicine23 January 2015 70

Challenges - The research-practice gap
Research Evidence Practice
Diffusion
/Adoption
Information overload
Application to other populations
Lack of consideration of local
community groups, agencies and
governments role and needs
Cultural factors
Economic factors
Social factors
Evidence Based Medicine23 January 2015 71
Research Evidence Policy making
Challenges: The research-policy gap
Service level
National policy level
Evidence Based Medicine23 January 2015 72
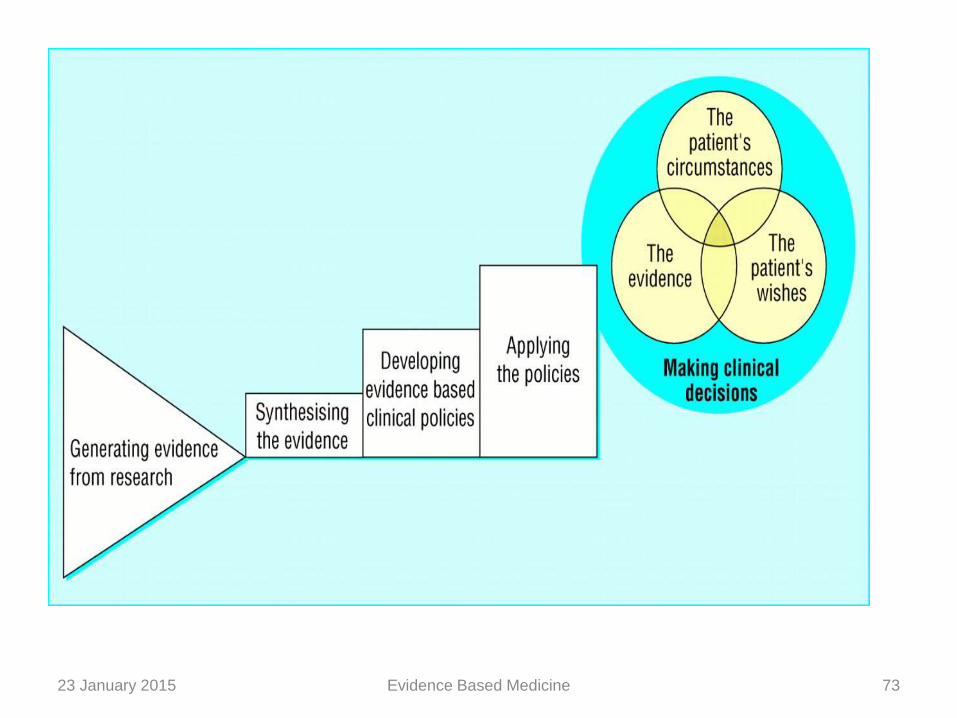
Evidence Based Medicine23 January 2015 73
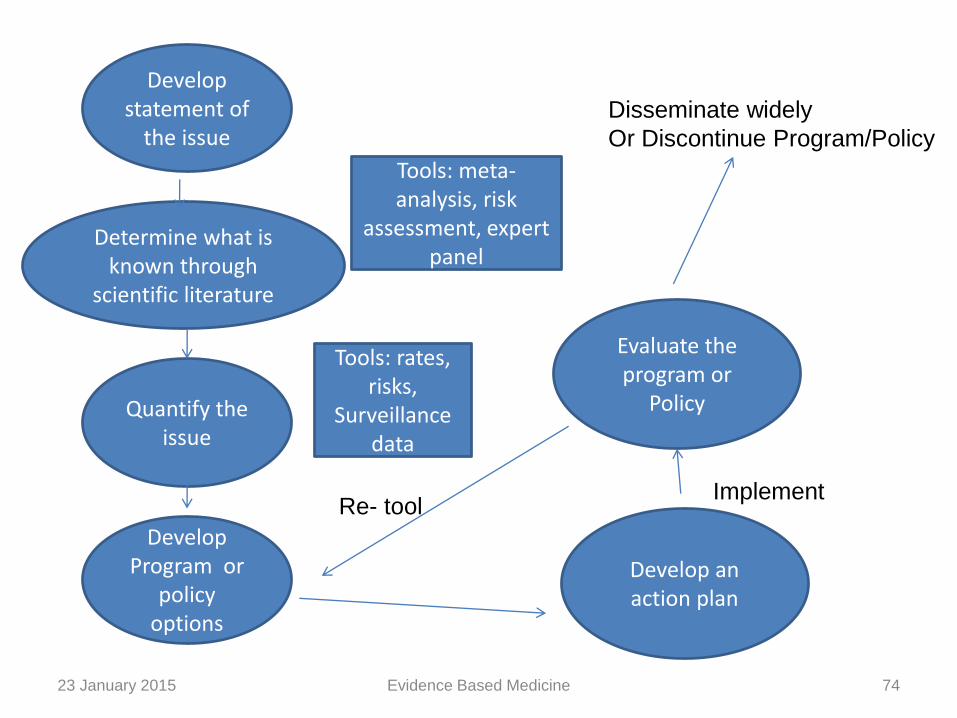
23 January 2015 Evidence Based Medicine 74
Develop statement of
the issue
Determine what is known through
scientific literature
Quantify the issue
Develop Program or
policy options
Evaluate the program or
Policy
Develop an action plan
Tools: meta-analysis, risk
assessment, expert panel
Tools: rates, risks,
Surveillance data
ImplementRe- tool
Disseminate widely
Or Discontinue Program/Policy
Conclusion
• Medicine is not an exact science, but a science of probability
• The challenge to physicians is to provide up to-date medical care
• The ultimate goal for clinicians should be to help patients live long, functional, satisfying, and pain and symptom free life
• By adopting the principles of Evidence Based Medicine, it will be possible to maximize the benefits of scientific research for patient care
23 January 2015 Evidence Based Medicine 75
• Medical educators and medical colleges have the singular responsibility of indoctrinating the principles of EBM
as a concept,
a philosophy,
a religion necessary for being efficient, compassionate, caring, and responsible clinician among the future physicians during their formative years of training
23 January 2015 Evidence Based Medicine 76
References1. Evidence-based Medicine Workbook-Finding and applying the better
research , Paul Glasziou, Chris Del Mar and Janet Salisbury
2. Sackett, D. L., Straus, S. E., Richardson, W. S., Rosenberg,W., Haynes, R. B.: Evidence- Based Medicine – How to Practice and Teach EBM 2nd Ed., Churchill. Livingstone, 2000.
3. Sackett DL, Rosenberg WMC, Gray JA, Haynes RB Richardson WS. Evidence based medicine: What it is and what it isn’t Br. Med J 1996;312:71-72.
4. Evidence Based Medicine And Its Impact On Medical Education Dr. H. B. Rajashekhar1 Dr. B. S. Kodkany2 Dr. Vijaya A. Naik3 Dr. P. F. Kotur4 Dr. Shivaprasad S. Goudar5:Indian J. Anaesth. 2002; 46 (2) : 96-103
5. Guyatt GH, Evidence–based Medicine. Ann Intern Med. 1991;114(ACP J Club. Suppl 2): A-16
23 January 2015 Evidence Based Medicine 77
23 January 2015 Evidence Based Medicine 78
23 January 2015 Evidence Based Medicine 79