Embed Size (px)
Citation preview
DR NARENDER SAINIASS IST. PROF,
UN IT OF HAND SURGERY,DEPARTMENT OF ORTHOPAEDIC S,
SMS MEDICAL COLLEGE AND AT TACHED GROUPS OF HOSP ITALS ,
JA IPUR .
Overview ofElbow Trauma & Infections.
Sunday,May 1, 2016PG Teaching RRC
Sunday,May 1, 2016PG Teaching RRC
Elbow Overview
Trauma Infection
Elbow Trauma
6% of all fractures and dislocations involve elbow
Most common fractures differ between adults and children M.C. in adults- radial head and neck Fracture M.C. in children- supracondylar fracture.
Complex anatomy requires 4 views for adequate interpretation AP in extension, medial oblique, lateral and axial
olecranon (Jones view)
Sunday,May 1, 2016PG Teaching RRC
Elbow Trauma
Pediatric Adult
Sunday,May 1, 2016PG Teaching RRC
Pediatric Elbow Injuries
Condylar Fractures
Lateral Medial
Supracondylar fractures
Inter/ Epi Condylar Fracture
Sunday,May 1, 2016PG Teaching RRC
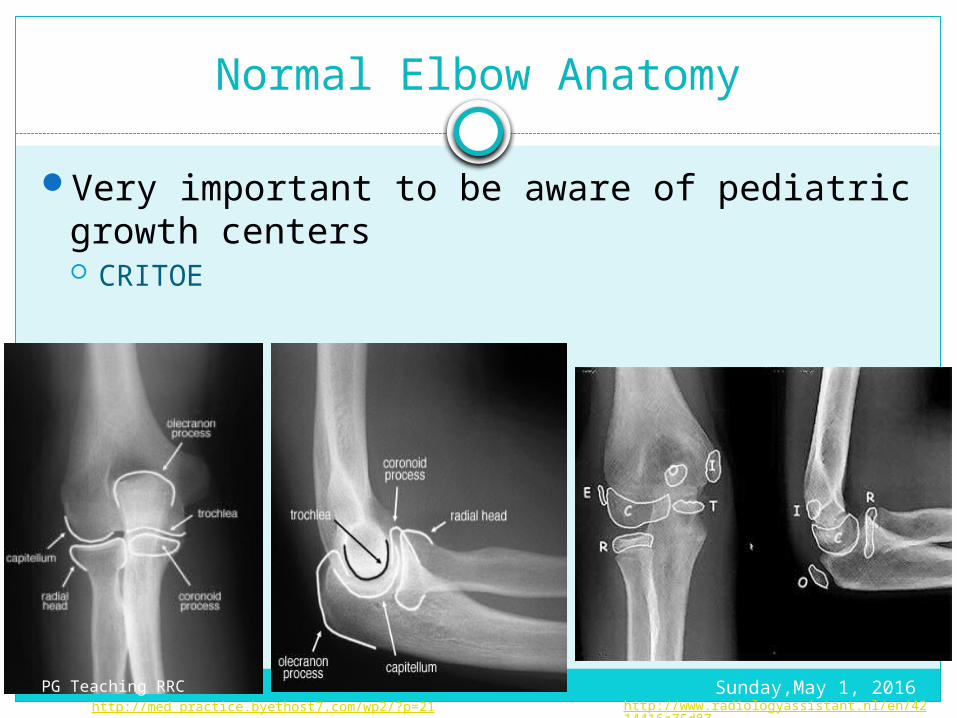
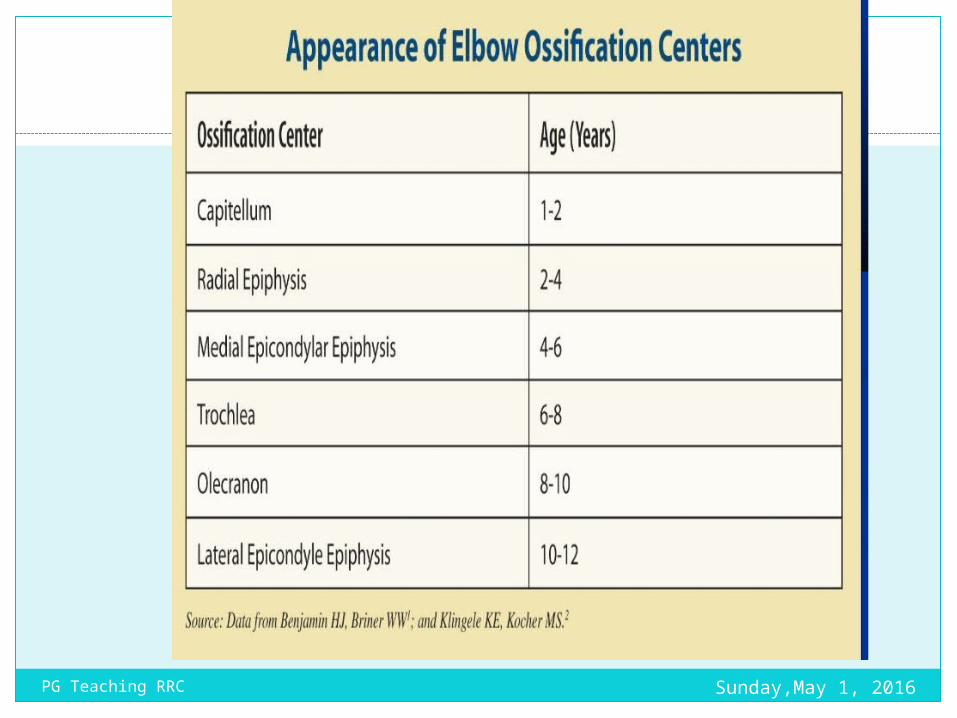
Normal Elbow Anatomy
Very important to be aware of pediatric growth centers CRITOE
http://med_practice.byethost7.com/wp2/?p=21 http://www.radiologyassistant.nl/en/4214416a75d87
Sunday,May 1, 2016PG Teaching RRC
Sunday,May 1, 2016PG Teaching RRC
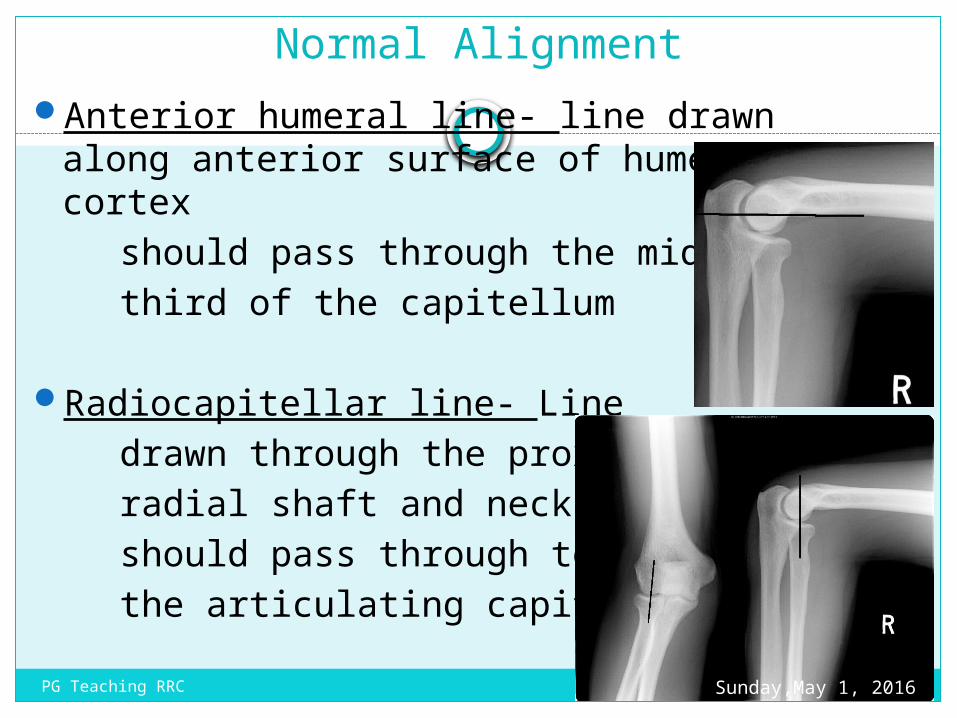
Normal AlignmentAnterior humeral line- line drawn along
anterior surface of humeral cortex should pass through the middle third of the capitellum
Radiocapitellar line- Line drawn through the proximal radial shaft and neck should pass through to the articulating capitellum
Sunday,May 1, 2016PG Teaching RRC
Signs of Fracture
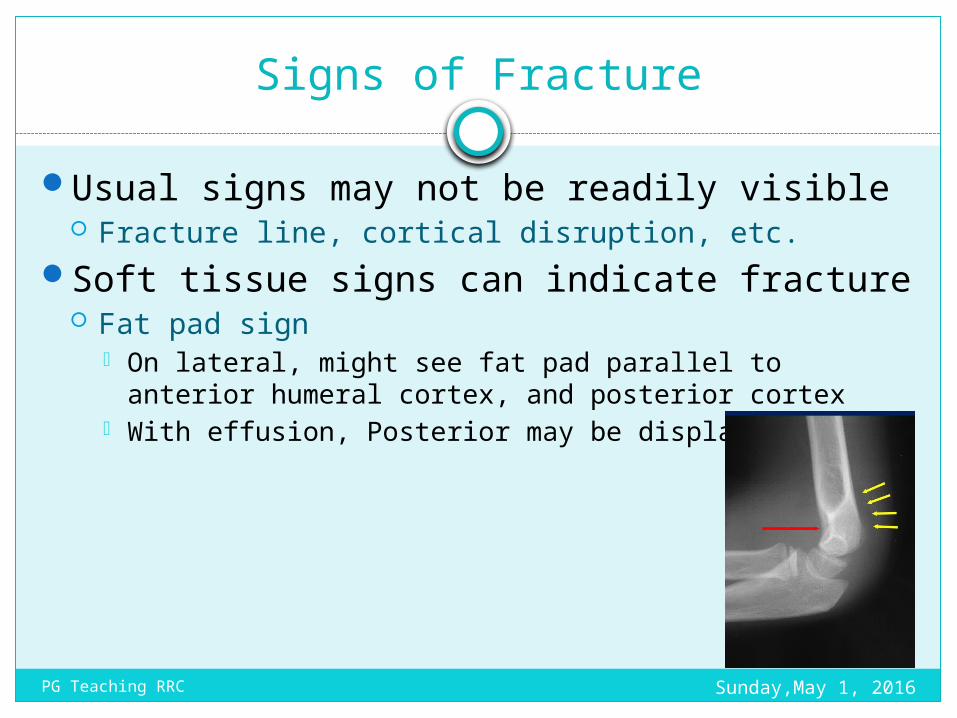
Usual signs may not be readily visible Fracture line, cortical disruption, etc.
Soft tissue signs can indicate fracture Fat pad sign
On lateral, might see fat pad parallel to anterior humeral cortex, and posterior cortex
With effusion, Posterior may be displaced
Sunday,May 1, 2016PG Teaching RRC
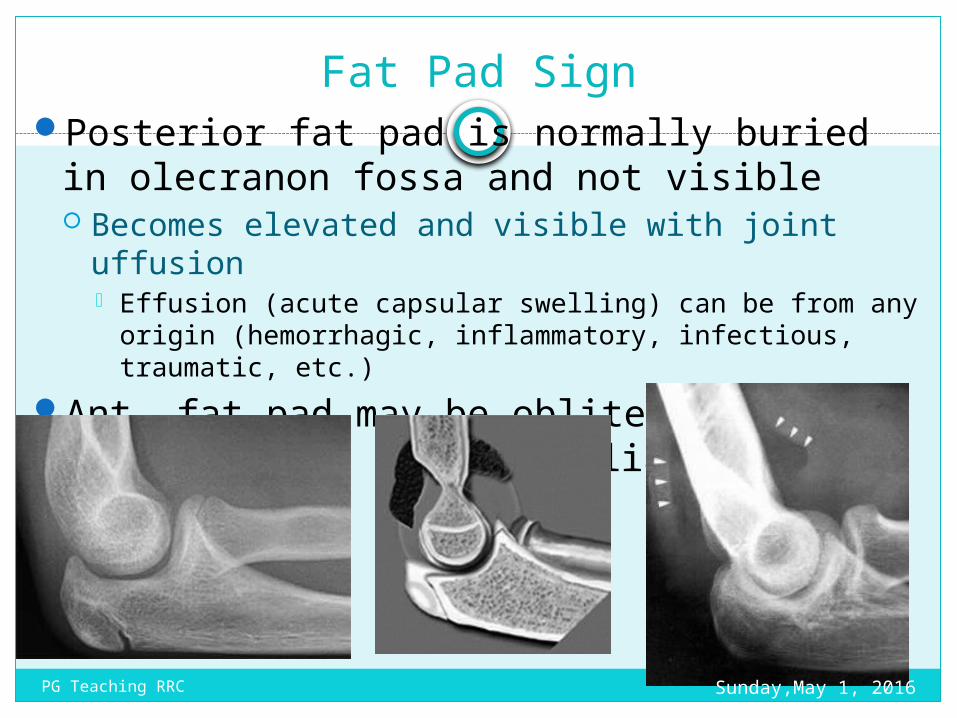
Fat Pad SignPosterior fat pad is normally buried in
olecranon fossa and not visible Becomes elevated and visible with joint uffusion
Effusion (acute capsular swelling) can be from any origin (hemorrhagic, inflammatory, infectious, traumatic, etc.)
Ant. fat pad may be obliterated, so post. Fat pad is more reliable when visible
Sunday,May 1, 2016PG Teaching RRC
Distal humerus fractures
95% extend to articular surfaceClassified according to relationship with
condyle and shape of fracture line Supracondylar, intercondylar, condylar and epicondylar
Sunday,May 1, 2016PG Teaching RRC
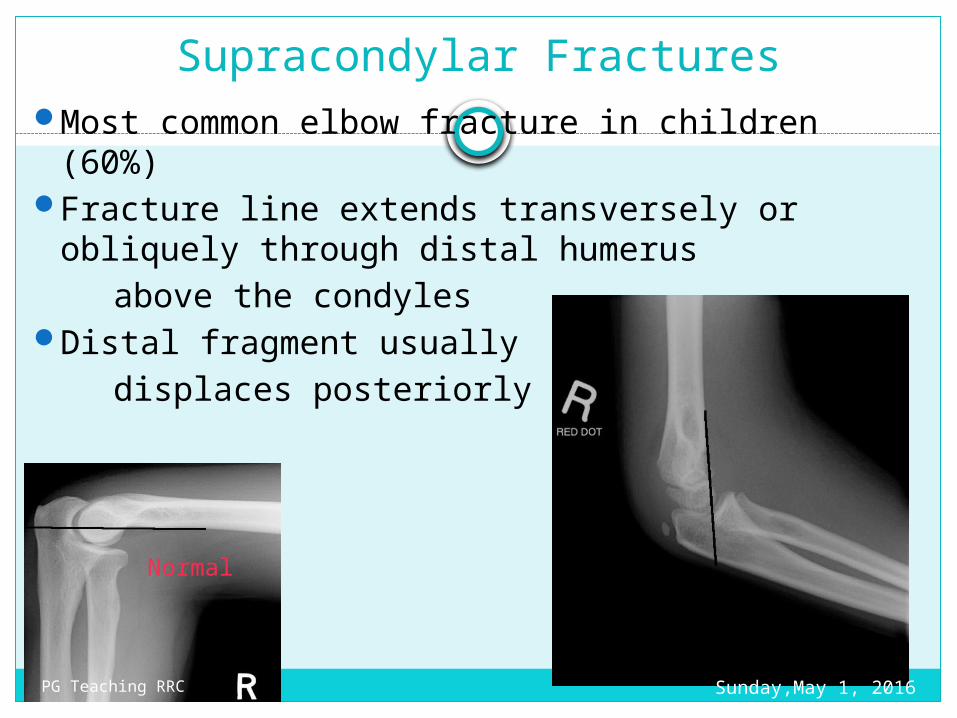
Supracondylar FracturesMost common elbow fracture in children (60%)Fracture line extends transversely or obliquely
through distal humerus above the condyles Distal fragment usually displaces posteriorly
Normal
Sunday,May 1, 2016PG Teaching RRC
Intercondylar fracture
Fracture line extends between medial and lateral condyles and extends to supracondylar region Results and T or Y shaped configuration for fracture
Called trans-condylar if it extends through both condyles
Sunday,May 1, 2016PG Teaching RRC
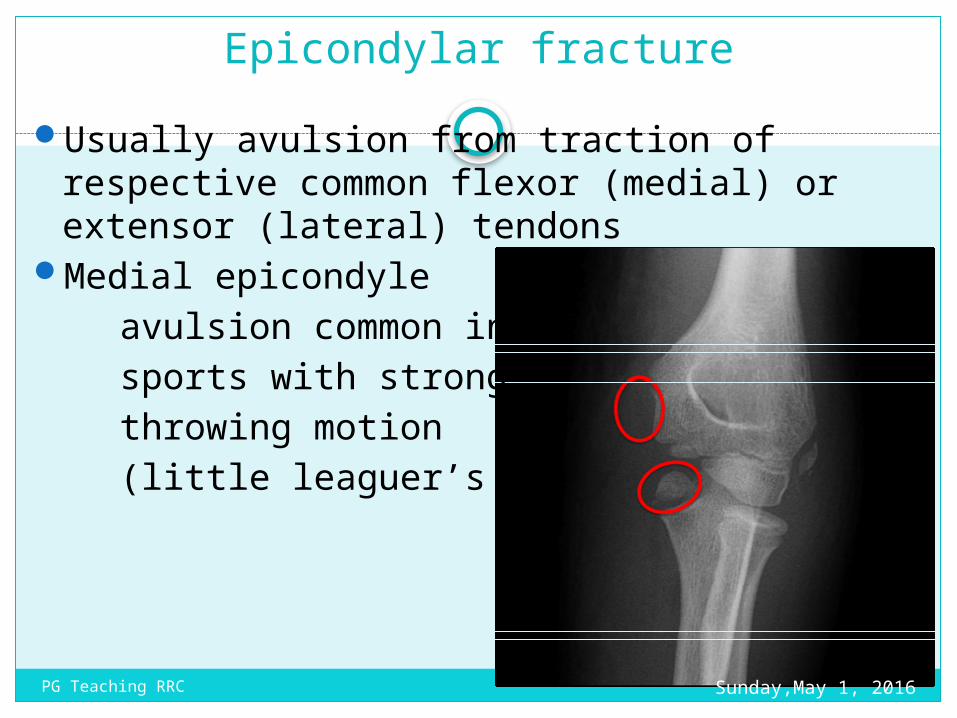
Epicondylar fractureUsually avulsion from traction of respective
common flexor (medial) or extensor (lateral) tendons
Medial epicondyle avulsion common in sports with strong throwing motion (little leaguer’s elbow)
Sunday,May 1, 2016PG Teaching RRC
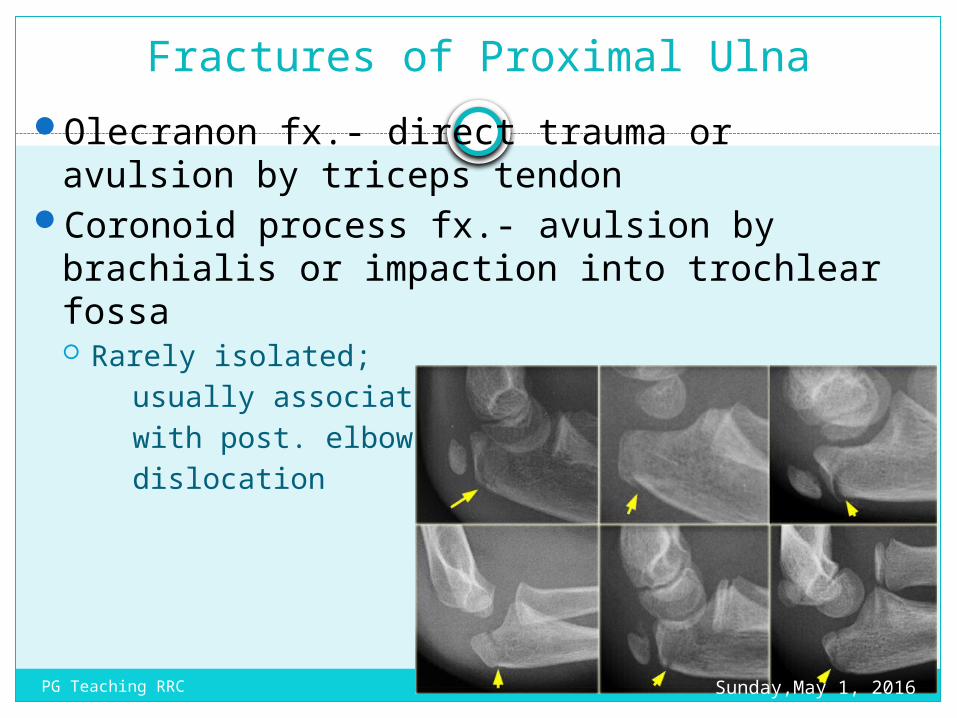
Fractures of Proximal UlnaOlecranon fx.- direct trauma or avulsion by
triceps tendonCoronoid process fx.- avulsion by brachialis or
impaction into trochlear fossa Rarely isolated; usually associated with post. elbow dislocation
Sunday,May 1, 2016PG Teaching RRC
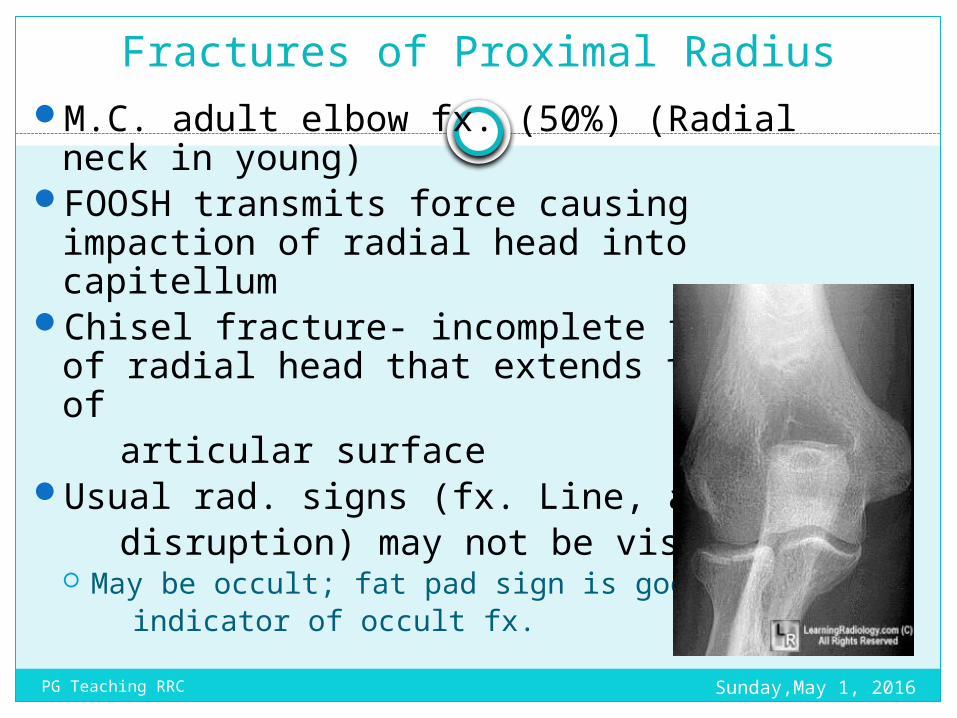
Fractures of Proximal RadiusM.C. adult elbow fx. (50%) (Radial neck in
young)FOOSH transmits force causing impaction of
radial head into capitellumChisel fracture- incomplete fracture of radial
head that extends to center of articular surfaceUsual rad. signs (fx. Line, articular disruption) may not be visible
May be occult; fat pad sign is good indicator of occult fx.
Sunday,May 1, 2016PG Teaching RRC
Dislocations of Elbow
3rd m.c. dislocation in adults behind shoulder and interphalangeal joints More common in children
Classified according to displacement of radius an ulna relative to humerus Posterior, posterolateral, anterior, medial and
anteromedialPosterior and posterolateral or more most
common 85-90% of all elbow dislocations 50% have associated fractures
Sunday,May 1, 2016PG Teaching RRC
Pulled Elbow
Nursemaid’s elbowOccurs when child’s hand is pulled, traction
causes radial head to slip out from under annular ligament and trapping the ligament in the radiohumeral articulation
Immediate pain; stuck in mid-pronation due to pain
No radiographic signSupination reduces the dislocation and ends
pain, usually during positioning of lateral radiograph Sunday,May 1, 2016PG Teaching RRC
Adult Elbow Injuries
Distal Humerus
Type ASupracon
dylar
Type RUnicondyl
ar
Type CBicondyla
r
Proximal Ulna
CoronoidFractures
Olecranon
Proximal Radius
Head Radius
Neck of Radius
Dislocations
Sunday,May 1, 2016PG Teaching RRC
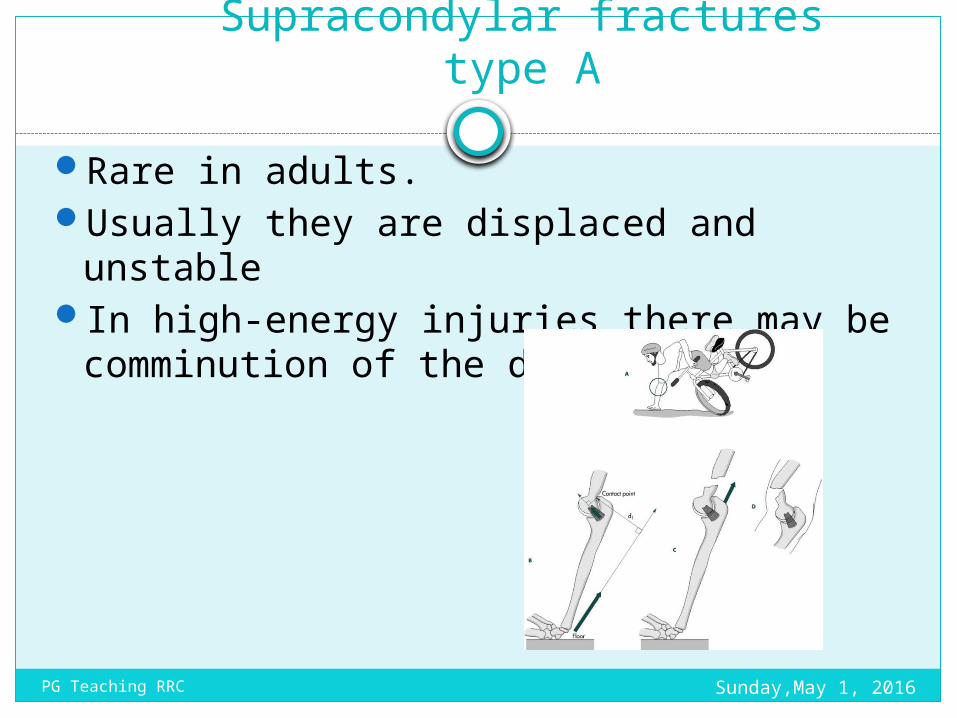
Supracondylar fractures type A
Rare in adults. Usually they are displaced and unstableIn high-energy injuries there may be
comminution of the distal humerus
Sunday,May 1, 2016PG Teaching RRC
Treatment
Open reduction and internal fixation.Mostly plates and screws are used
Closed reduction is unlikely to be stableK-wire fixation is not strong enough to permit
early mobilization.
Sunday,May 1, 2016PG Teaching RRC
Types B and C intra articular fractures
High-energy traumaAssociated with soft-tissue damage. A severe blow on the point of the elbow
drives the olecranon process upwards, splitting the condyles apart.
Swelling is considerable. The patient should be checked for
i. Pulselessnessii. Palloriii. Painiv. Paresthesiav. Paralysis
Sunday,May 1, 2016PG Teaching RRC
X-ray
T- or Y shaped break, or else there may be (comminution).
Sunday,May 1, 2016PG Teaching RRC
Treatment type Undisplaced fractures
Joint damage- prolonged immobilization will certainly result in a stiff elbow.
Early movement is a prime objective.Treated by applying a posterior slab with
the elbow flexed almost 90 degrees; movements are commenced after 2
weeks.
Sunday,May 1, 2016PG Teaching RRC
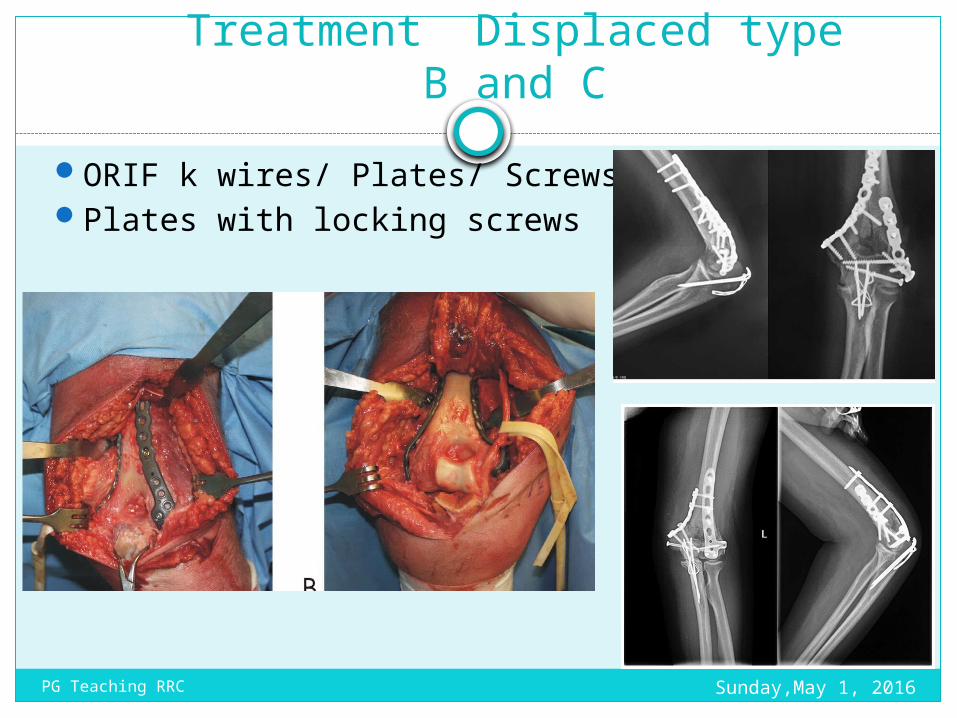
Treatment Displaced type B and C
ORIF k wires/ Plates/ ScrewsPlates with locking screws
Sunday,May 1, 2016PG Teaching RRC
Sunday,May 1, 2016PG Teaching RRC
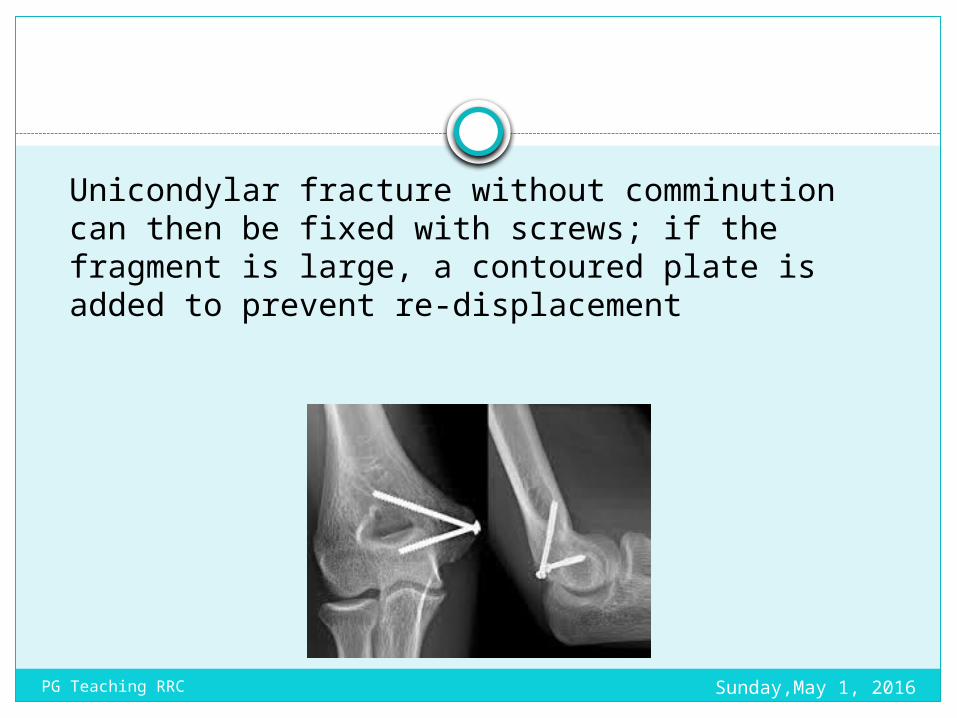
Unicondylar fracture without comminution can then be fixed with screws; if the fragment is large, a contoured plate is added to prevent re-displacement
Sunday,May 1, 2016PG Teaching RRC
Postoperatively the elbow is held at 90 degrees with the arm supported in a sling. Movement is encouraged but should never be forced.
Fracture healing usually occurs by 12 weeks. patient often does not regain full extension
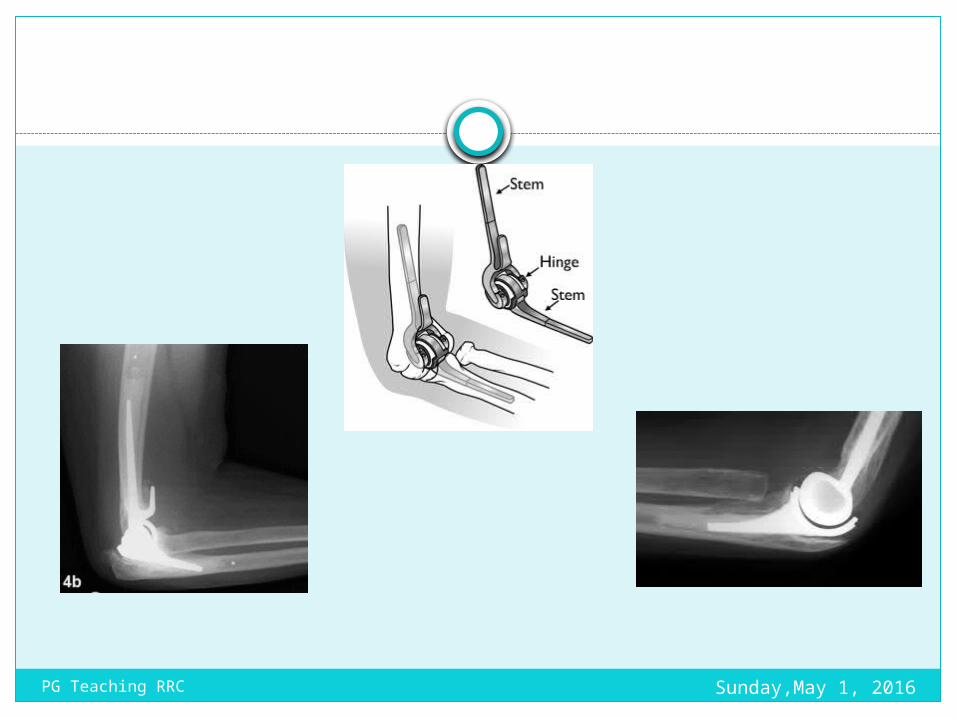
Alternative treatmentsElbow replacementThe ‘bag of bones’ technique.
The arm is held in a collar and cuff or, better, a hinged brace, with the elbow flexed above a right angle; active movements are encouraged as soon as the patient is willing. The fracture usually unites within 6–8 weeks, but exercises are continued far longer. A useful range of movement (45–90 degrees) is often obtained.
Skeletal traction the patient remains in bed with the humerus
held vertical, and elbow movements are encouraged.
Sunday,May 1, 2016PG Teaching RRC

Complications of supracondylar fractures
Vascular injuryNerve injury median nerveVolkmann’s ischemic contractureMalunion leading to gunstock deformity Myositis ossificansStiffness
Sunday,May 1, 2016PG Teaching RRC
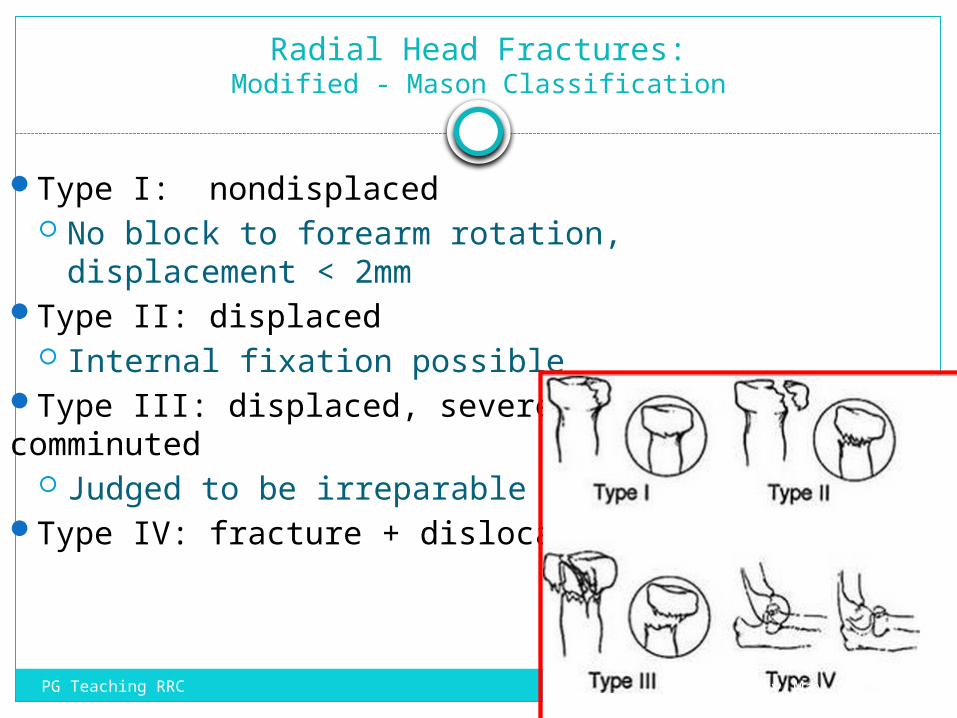
Radial Head Fractures:Modified - Mason Classification
Type I: nondisplaced No block to forearm rotation, displacement
< 2mmType II: displaced
Internal fixation possibleType III: displaced, severely comminuted
Judged to be irreparableType IV: fracture + dislocation
Sunday,May 1, 2016PG Teaching RRC
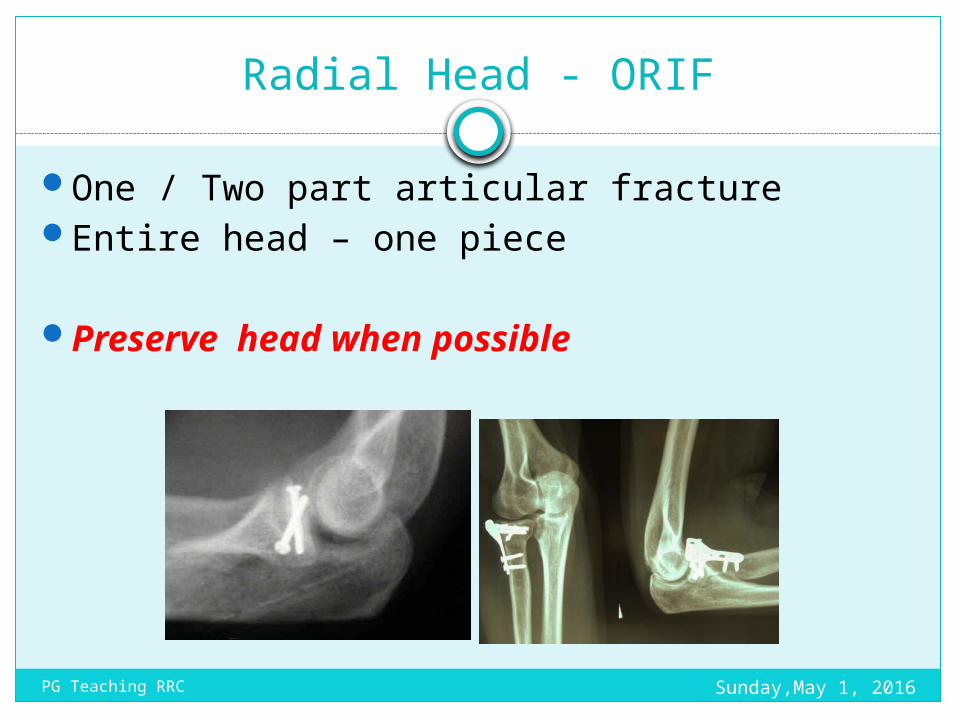
Radial Head - ORIF
One / Two part articular fractureEntire head – one piece
Preserve head when possible
Sunday,May 1, 2016PG Teaching RRC
Radial Head – Excise / replace
Fracture not reducable Osteoporotic Extraarticular
Elbow stable Elbow Unstable
Excise ReplaceSunday,May 1, 2016PG Teaching RRC
Do not excise without replacement
Restore radial head If not possible replace Repair lateral collateral ligOrif of coronoid
Sunday,May 1, 2016PG Teaching RRC
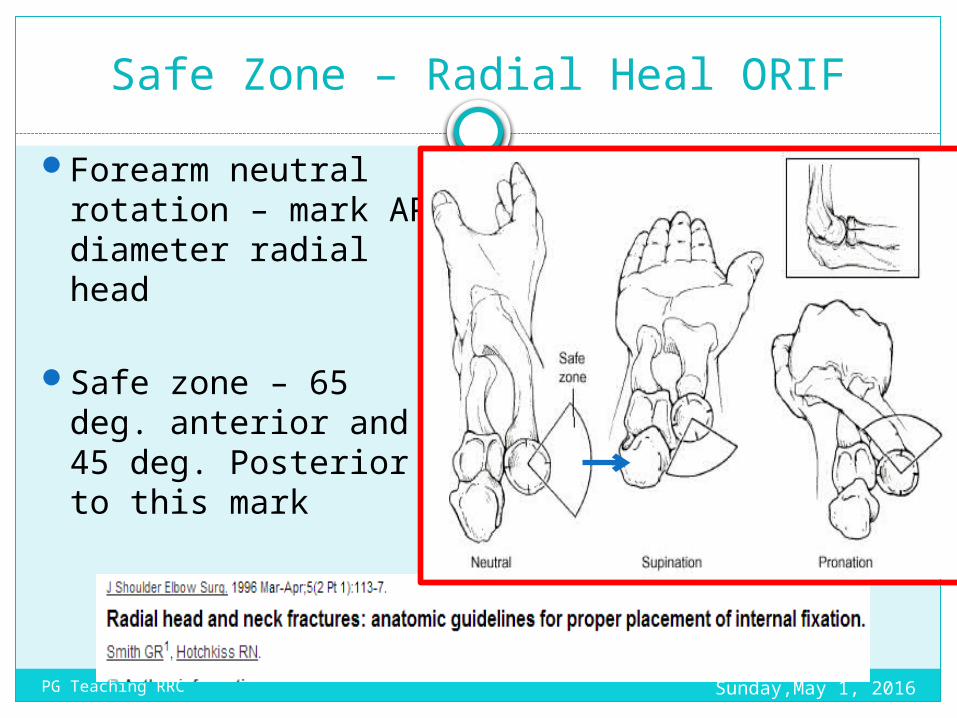
Safe Zone – Radial Heal ORIFForearm neutral
rotation – mark AP diameter radial head
Safe zone – 65 deg. anterior and 45 deg. Posterior to this mark
Sunday,May 1, 2016PG Teaching RRC
Radial head replacement
Overstuffing – early joint degeneration
Understuffing – Valgus instability
Intraop – visible ulnohumeral gap – suggests radial lengthening.
Sunday,May 1, 2016PG Teaching RRC
Sunday,May 1, 2016PG Teaching RRC
Coronoid fracture
Classification
Regan and Moorey
O’ Driscoll
Sunday,May 1, 2016PG Teaching RRC
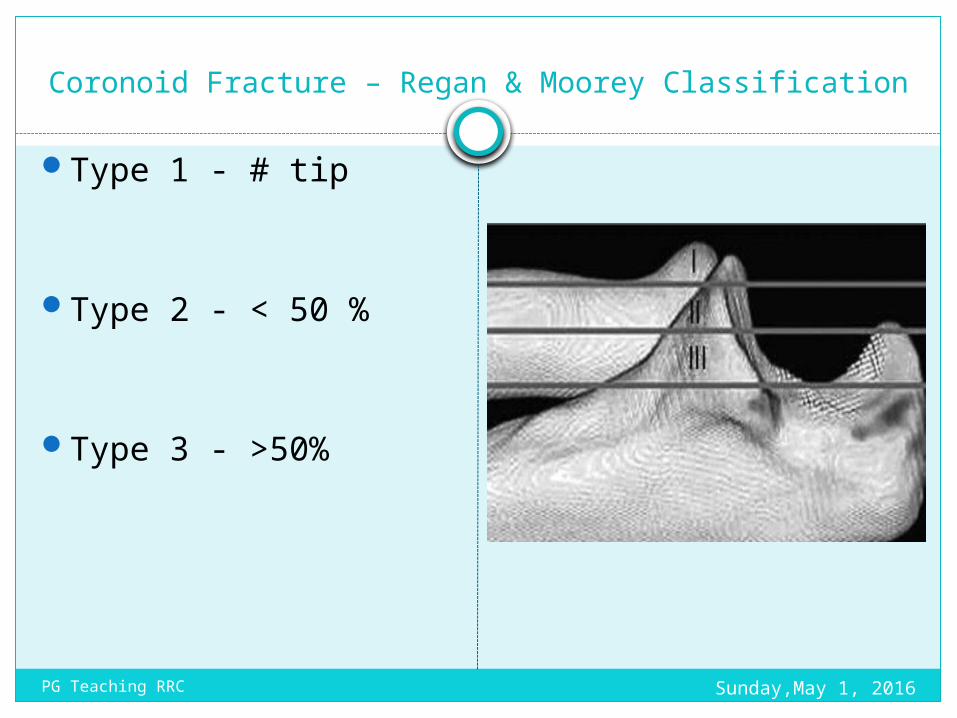
Coronoid Fracture – Regan & Moorey Classification
Type 1 - # tip
Type 2 - < 50 %
Type 3 - >50%
Sunday,May 1, 2016PG Teaching RRC
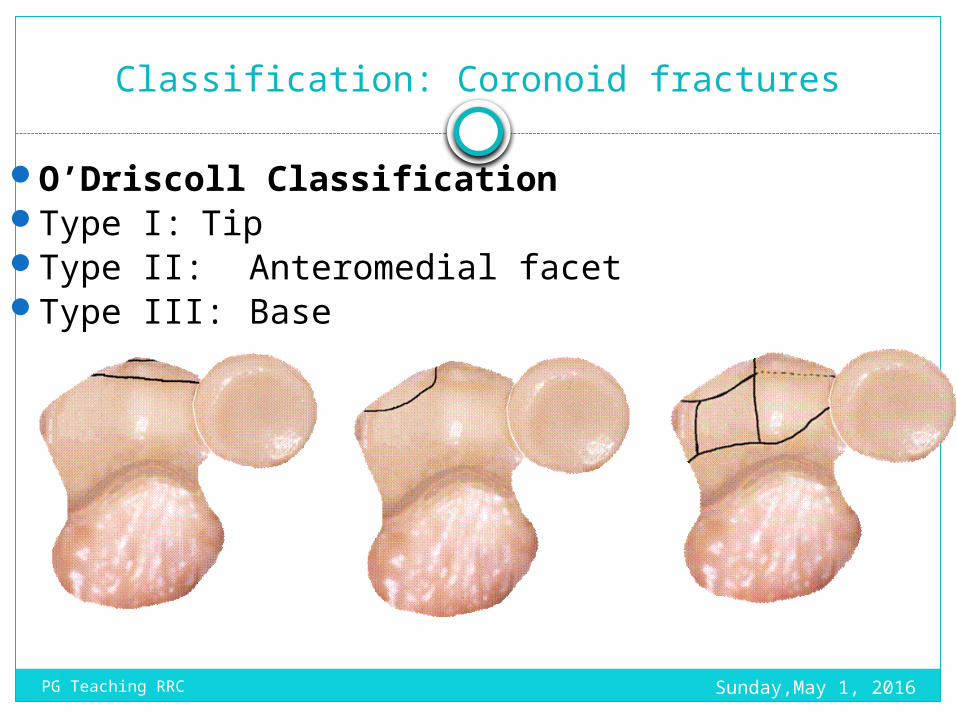
Classification: Coronoid fractures
O’Driscoll ClassificationType I: TipType II: Anteromedial facetType III: Base
Sunday,May 1, 2016PG Teaching RRC
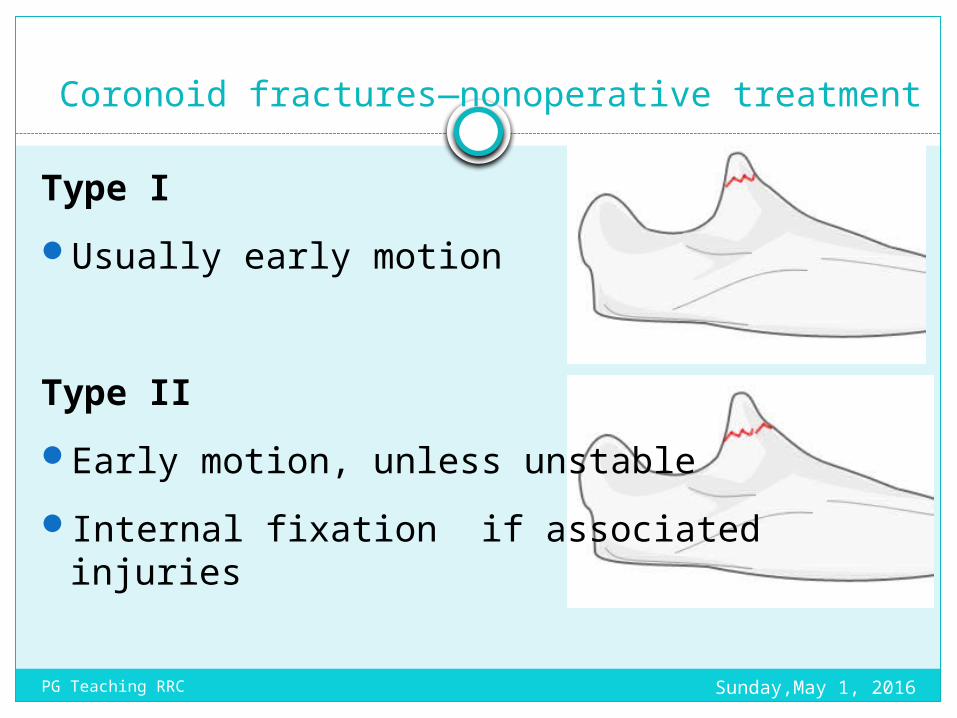
Coronoid fractures—nonoperative treatment
Type I Usually early motion
Type II Early motion, unless unstableInternal fixation if associated injuries
Sunday,May 1, 2016PG Teaching RRC
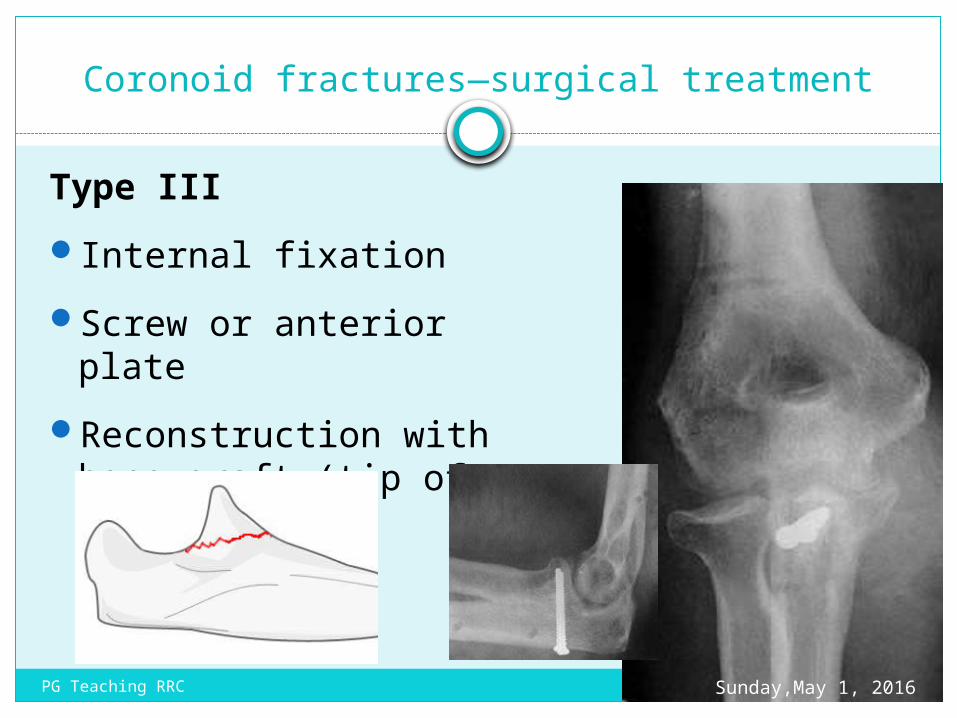
Coronoid fractures—surgical treatment
Type IIIInternal fixationScrew or anterior
plateReconstruction with
bone graft (tip of olecranon)
Sunday,May 1, 2016PG Teaching RRC
Coronoid fracture – Associated condition
Posteromedial rotatory instability
Posterolateral rotatory instability
Terrible triad
Large fracture of olecranon
Sunday,May 1, 2016PG Teaching RRC
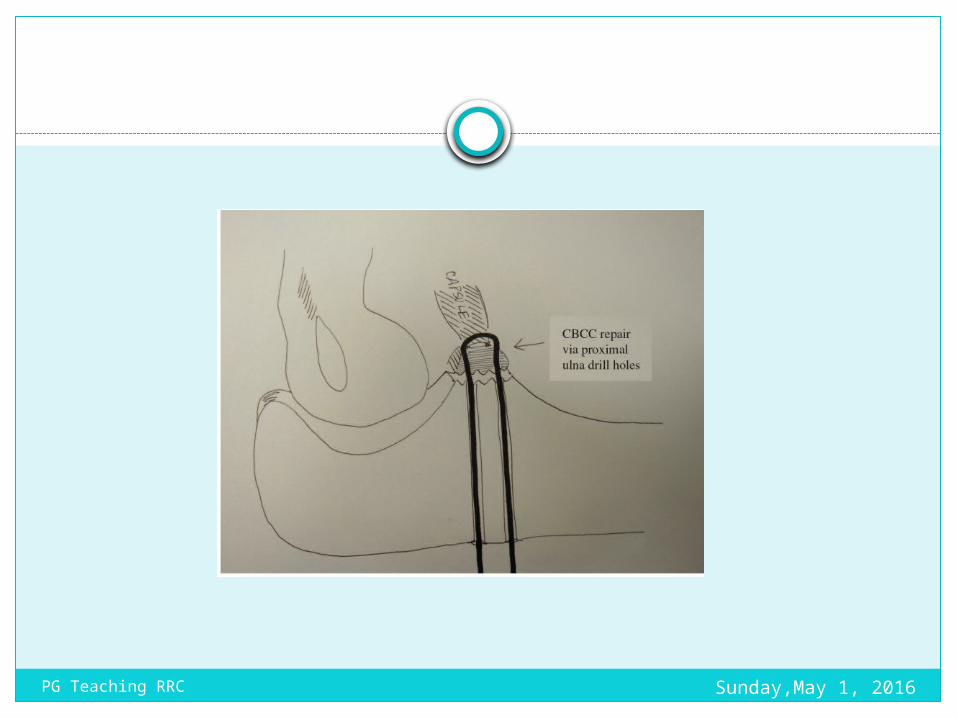
Coronoid fracture
Small fragments – Type 1
Fix with suture - non absorbale suture
Sunday,May 1, 2016PG Teaching RRC
Sunday,May 1, 2016PG Teaching RRC
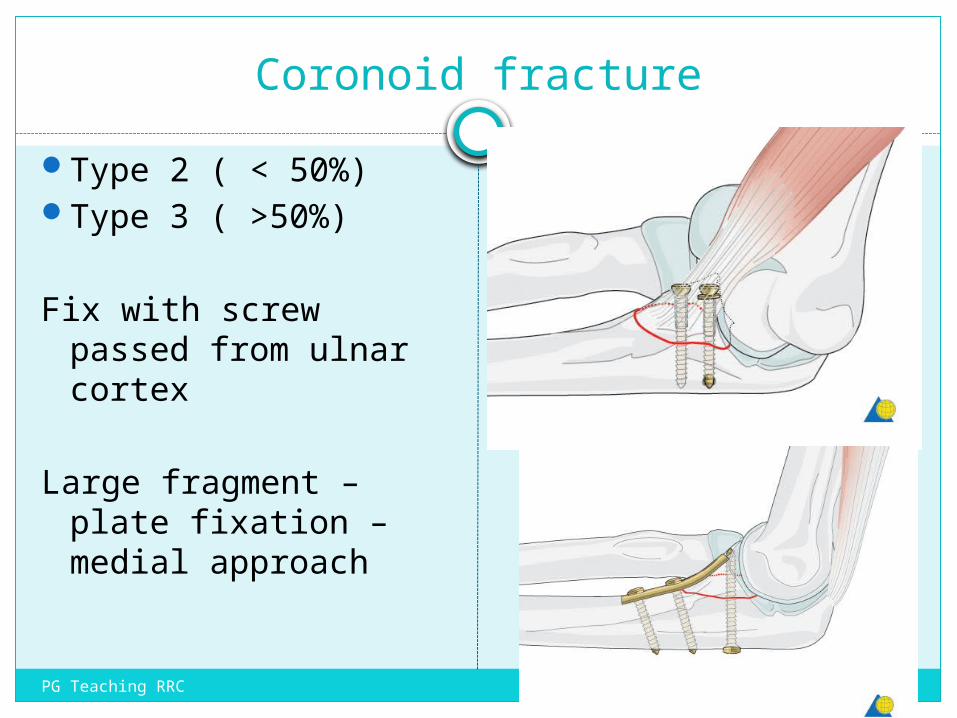
Coronoid fractureType 2 ( < 50%)Type 3 ( >50%)
Fix with screw passed from ulnar cortex
Large fragment – plate fixation – medial approach
Sunday,May 1, 2016PG Teaching RRC
Lateral Collateral Ligament Complex
Avulsed from lateral condyle along with common extensor
Unstable elbow to varus test
Local bruising
Sunday,May 1, 2016PG Teaching RRC
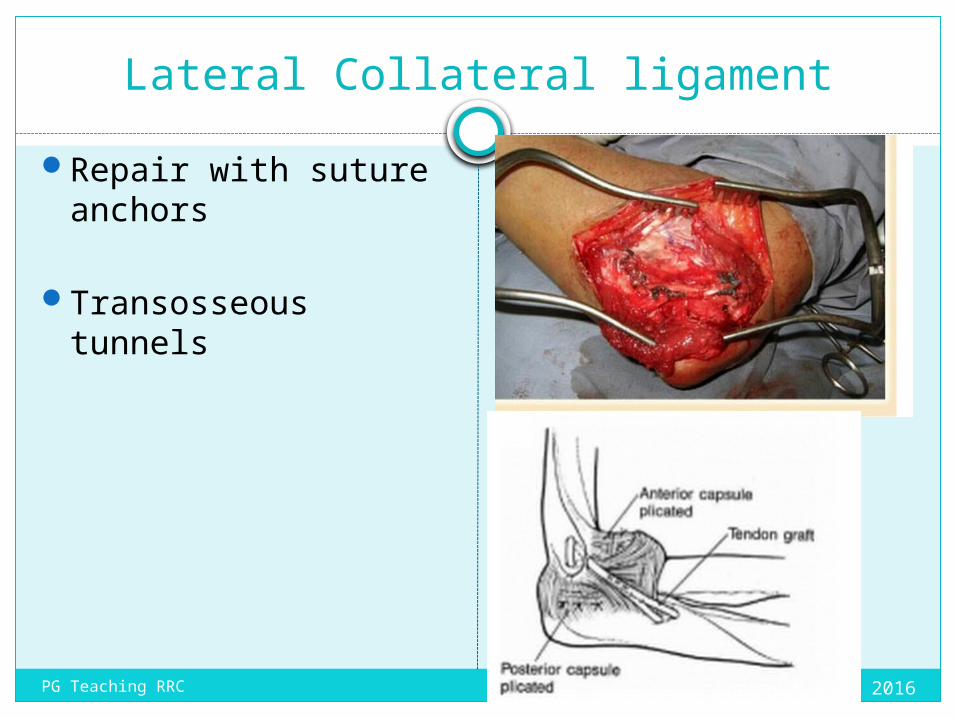
Lateral Collateral ligamentRepair with suture
anchors
Transosseous tunnels
Sunday,May 1, 2016PG Teaching RRC
Medial Collateral ligament
After repairing radial head Coronoid LCL
Test elbow stability – Fluoroscopically
Elbow unstable from 30 to 130 – repair MCL
Sunday,May 1, 2016PG Teaching RRC
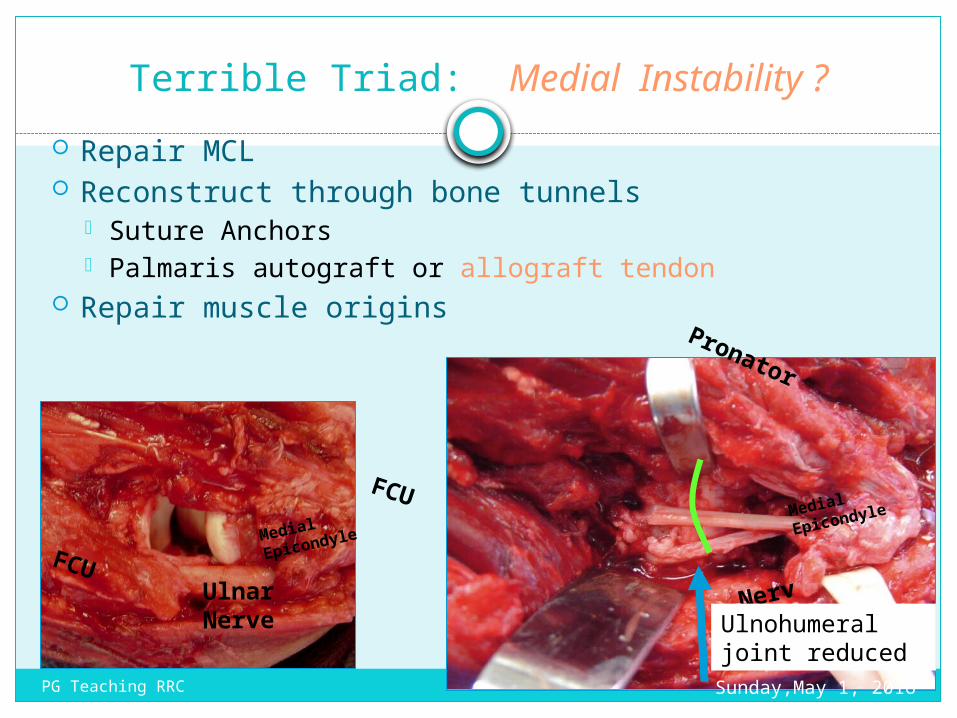
Terrible Triad: Medial Instability ? Repair MCL Reconstruct through bone tunnels
Suture Anchors Palmaris autograft or allograft tendon
Repair muscle originsPronator
FCU
Nerve
Medial Epicondyle
FCU Ulnar
Nerve
Medial Epicondyle
Ulnohumeral joint reducedSunday,May 1, 2016PG Teaching RRC
Sunday,May 1, 2016PG Teaching RRC
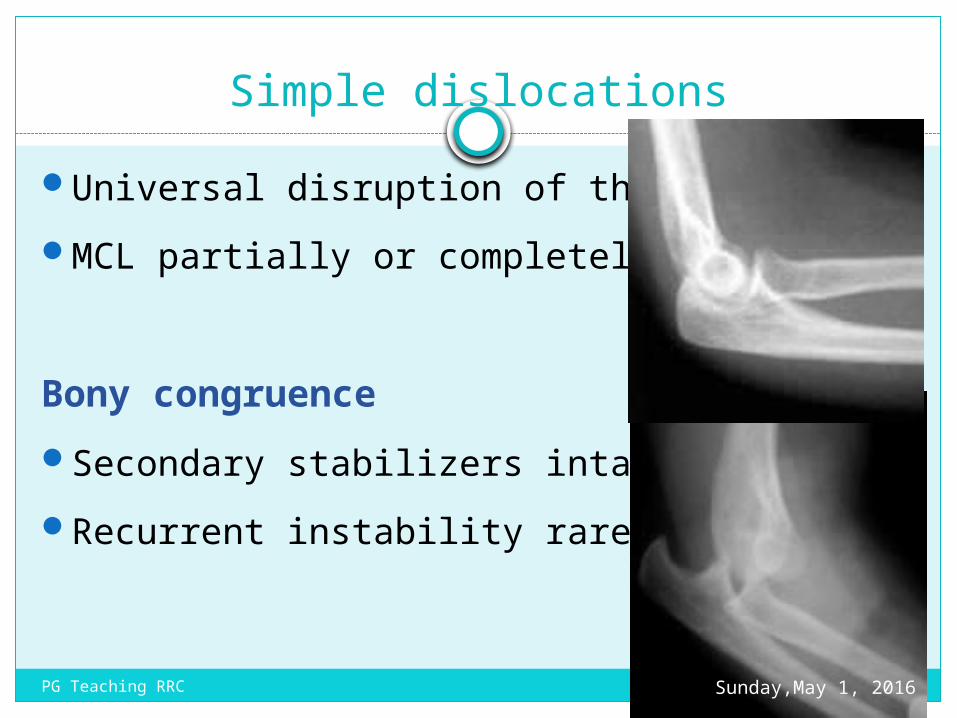
Simple dislocationsUniversal disruption of the LCLMCL partially or completely torn
Bony congruence Secondary stabilizers intactRecurrent instability rare
Sunday,May 1, 2016PG Teaching RRC
Stabilizers of elbowPrimary stabilizers
Ulnohumeral jointMCL -( Ant. Bundle)LCL - lateral ulnar
collateral ligament (LUCL),
Secondary stabilizers
Radiohumeral jointCapsuleOrigin of flexor &
extensor tendons
Dynamic stabilizers - Muscle crossing elbowAnconeusBrachialis
TricepsSunday,May 1, 2016PG Teaching RRC
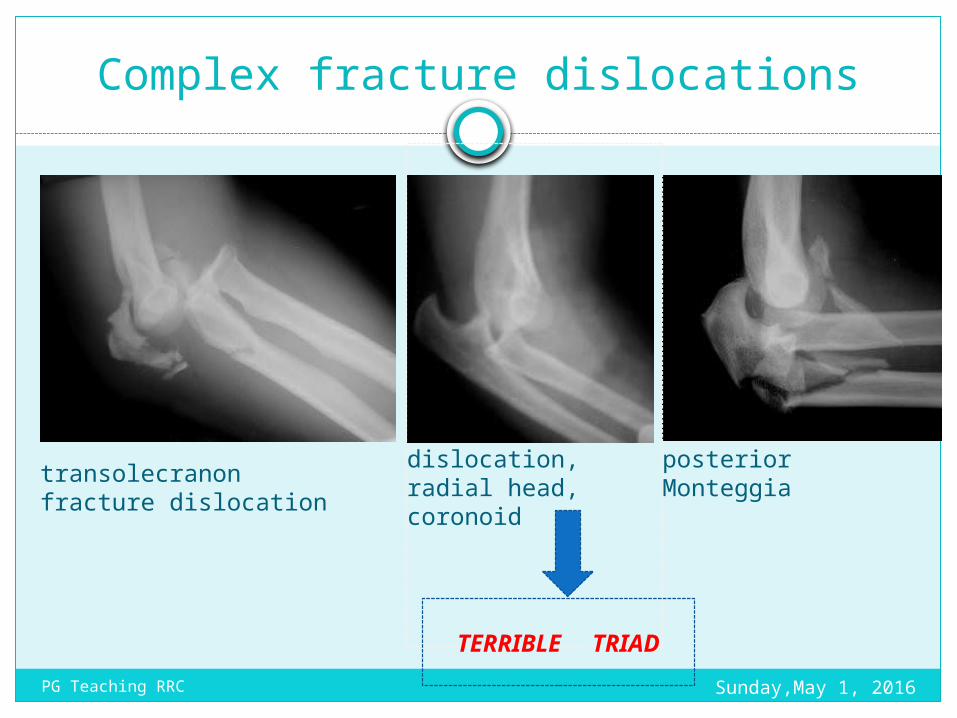
Complex fracture dislocations
transolecranon fracture dislocation
posterior Monteggiadislocation, radial
head, coronoid
TERRIBLE TRIADSunday,May 1, 2016PG Teaching RRC
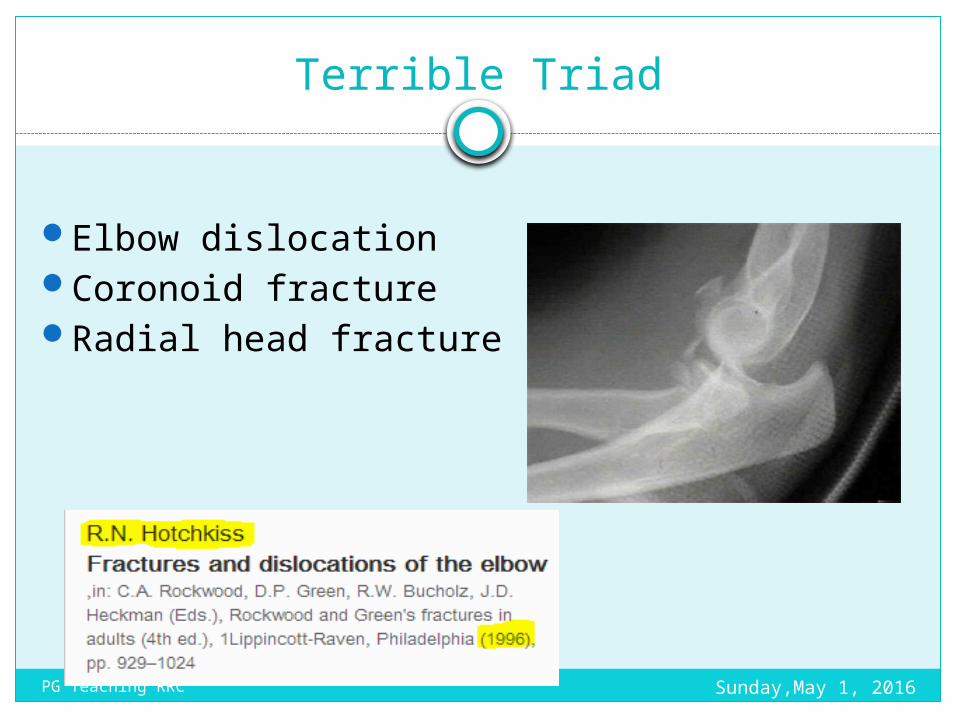
Terrible Triad
Elbow dislocation Coronoid fracture Radial head fracture
Sunday,May 1, 2016PG Teaching RRC

Sunday,May 1, 2016PG Teaching RRC
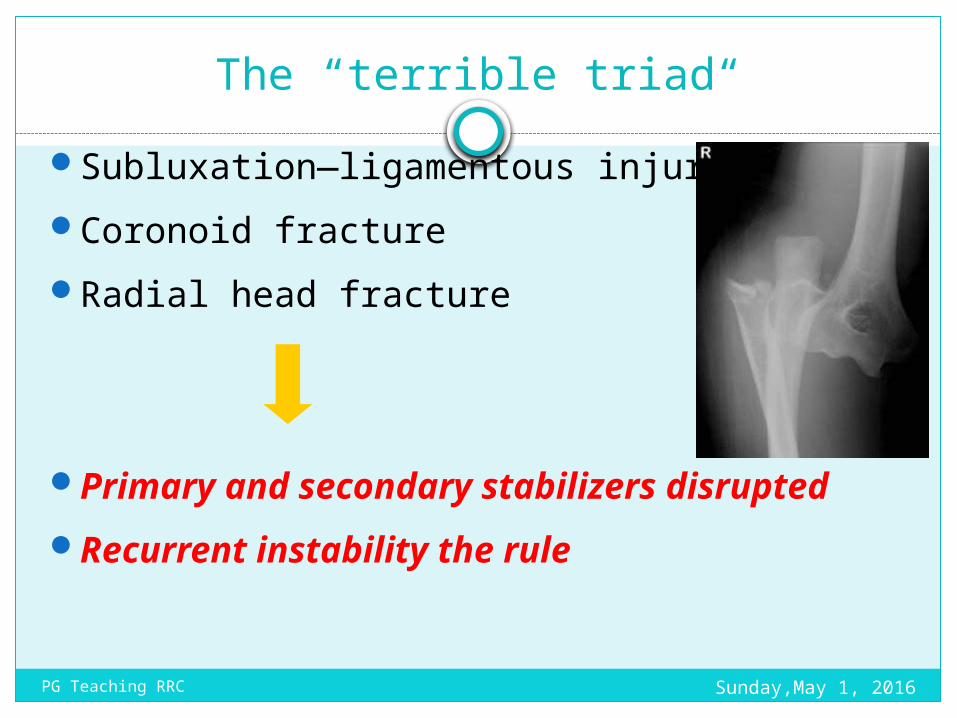
The “terrible triad“
Subluxation—ligamentous injuryCoronoid fractureRadial head fracture
Primary and secondary stabilizers disrupted
Recurrent instability the rule
Sunday,May 1, 2016PG Teaching RRC
Why terrible
Recurrent / persistent subluxation or dislocation
Chronic instability
Arthrosis and pain
Sunday,May 1, 2016PG Teaching RRC
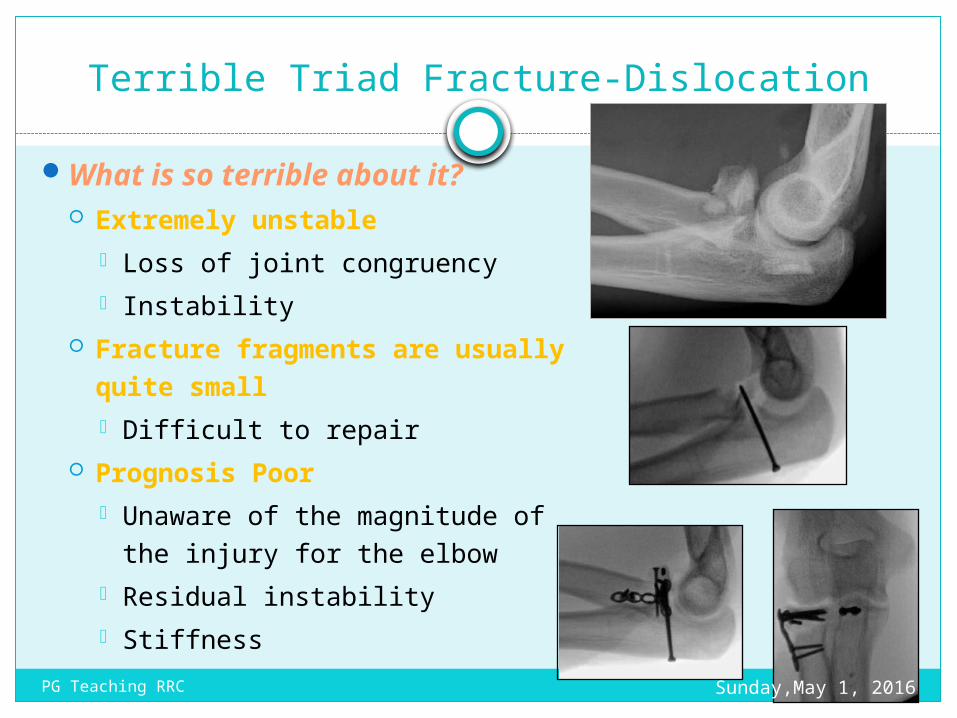
Terrible Triad Fracture-Dislocation
What is so terrible about it? Extremely unstable
Loss of joint congruency Instability
Fracture fragments are usually quite small Difficult to repair
Prognosis Poor Unaware of the magnitude of the
injury for the elbow Residual instability Stiffness
Sunday,May 1, 2016PG Teaching RRC
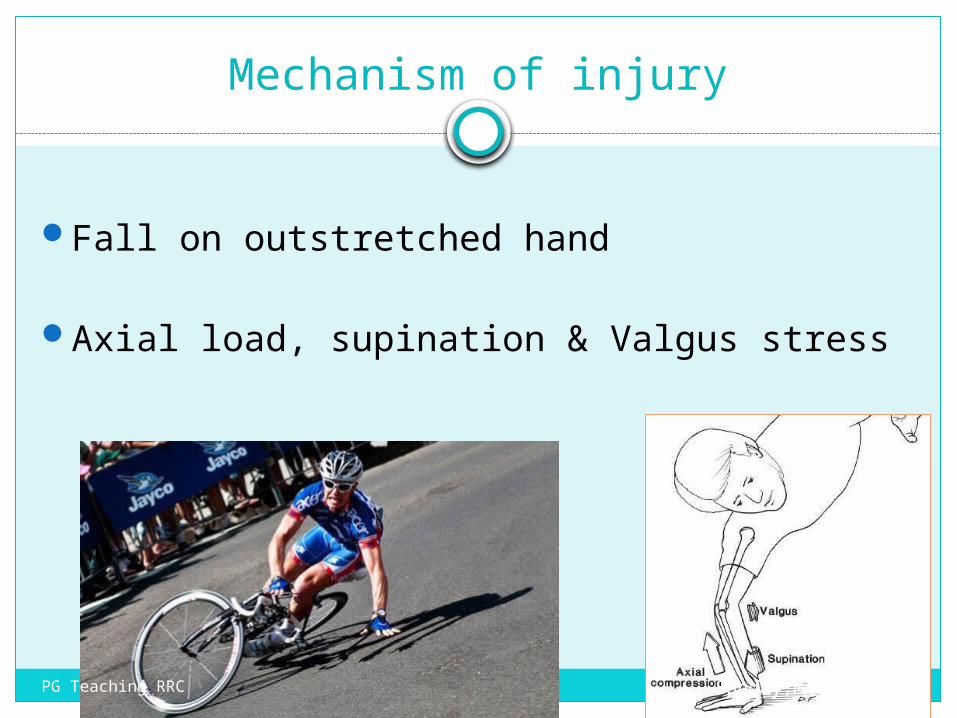
Mechanism of injury
Fall on outstretched hand
Axial load, supination & Valgus stress
Sunday,May 1, 2016PG Teaching RRC
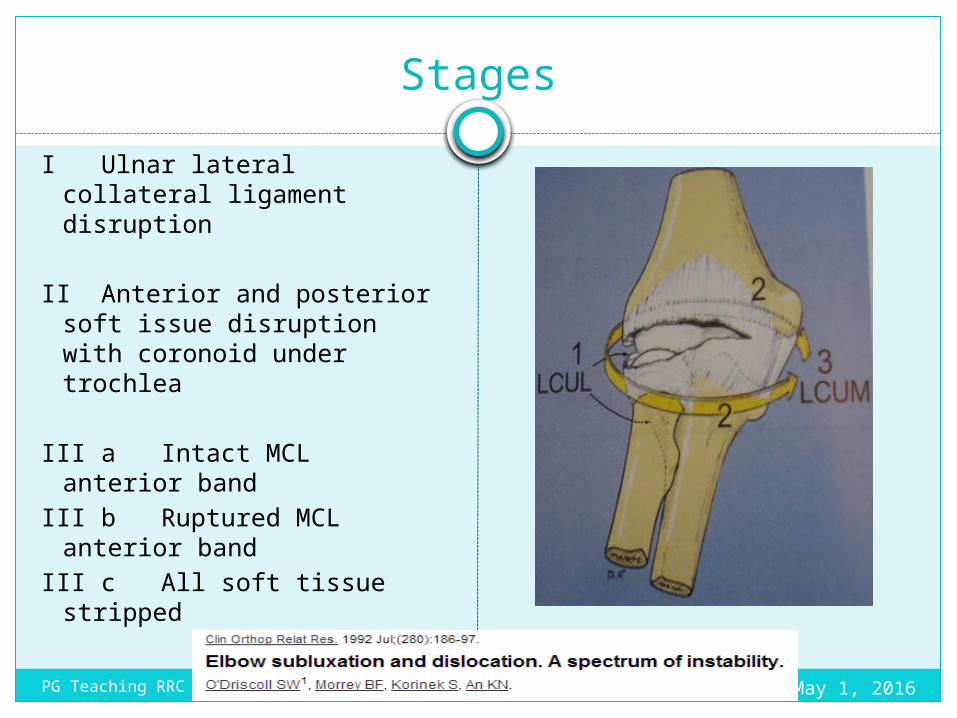
StagesI Ulnar lateral collateral
ligament disruption
II Anterior and posterior soft issue disruption with coronoid under trochlea
III a Intact MCL anterior band
III b Ruptured MCL anterior band
III c All soft tissue stripped
Sunday,May 1, 2016PG Teaching RRC
Terrible triad - Presentation
Pain ClickingLocking of elbow in extension
Varus instabilityValgus instability – ( If MCL injured )
Sunday,May 1, 2016PG Teaching RRC
What are the Dilemna
Surgical techniques challenging
Debate in surgical steps
Choices in management
Sunday,May 1, 2016PG Teaching RRC
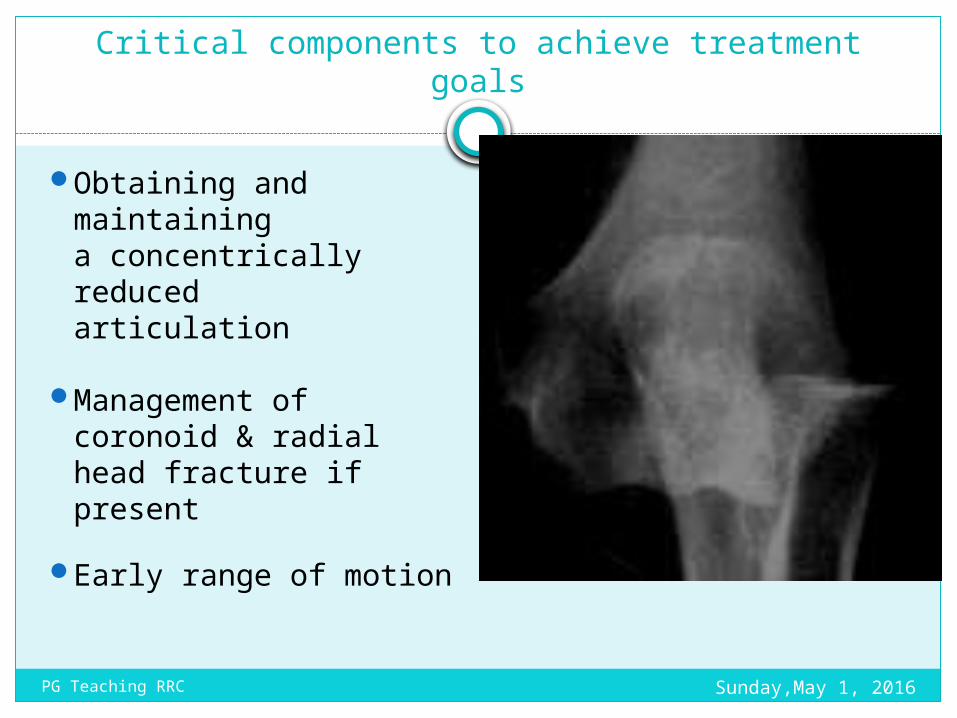
Critical components to achieve treatment goals
Obtaining and maintaining a concentrically reduced articulation
Management of coronoid & radial head fracture if present
Early range of motion
Sunday,May 1, 2016PG Teaching RRC
Examination
Unstable elbow with wrist injury - High risk of compartment syndrome
Combined distal radius and elbow fracture – 9/59 ( 15%)
Isolated distal radius # - 3/869 ( .3%)
Sunday,May 1, 2016PG Teaching RRC
Baseline neural examination
20% patient – Terrible ulnar nerve palsy
Sunday,May 1, 2016PG Teaching RRC
High risk of developing heterotopic ossification
Sunday,May 1, 2016PG Teaching RRC
Management
Dislocated elbow – reduce in emergency dept
Unstable – Do not perform repeat rereduction
Plan under anaesthesia
Sunday,May 1, 2016PG Teaching RRC
FRACTURED CAPITULUMRare articular fractureMainly occurs in adultsElbow is tender and flexion is grossly restrictedMechanism of injury
The patient falls on the hand, usually with the elbow straight.
The anterior part of the capitulum is sheared off and displaced proximally
Sunday,May 1, 2016PG Teaching RRC
X-rays
Bryan and Morrey classify these as:
i. Type I Complete fracture
ii. Type II Cartilaginous shell
iii. Type III Comminuted fracture.Sunday,May 1, 2016PG Teaching RRC
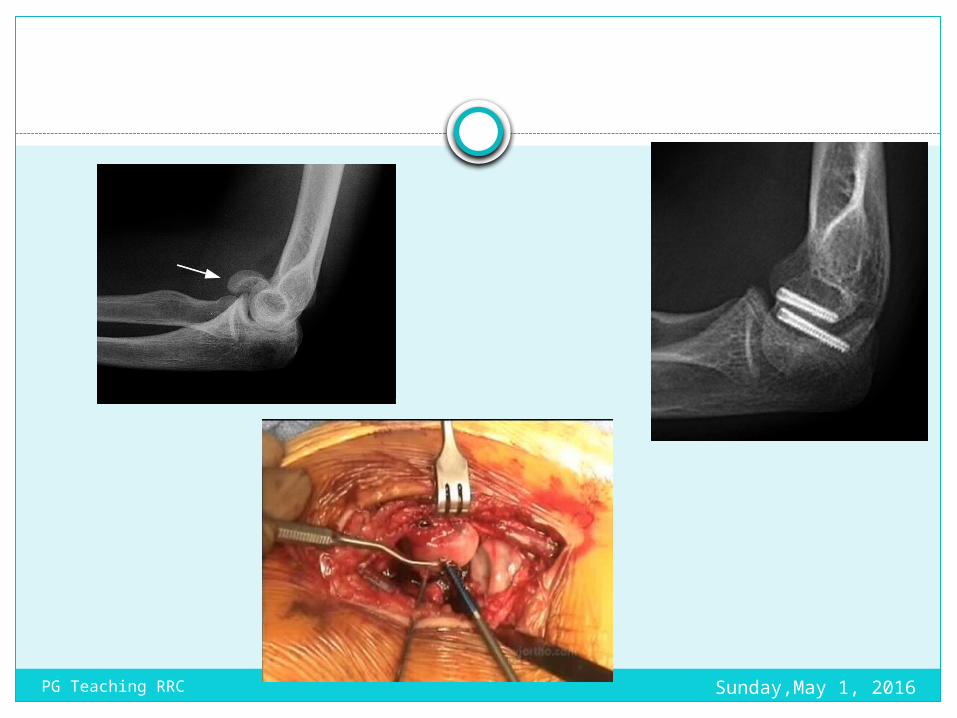
Treatment
Undisplaced fractures can be treated by simple splintage for 2 weeks.
Displaced fractures should be reduced and held.
Closed reduction is feasible, but prolonged immobilization may result in a stiff elbow.
ORIF is therefore preferred.Using headless bone screwsMovements are commenced as soon as
discomfort permitsSunday,May 1, 2016PG Teaching RRC
Sunday,May 1, 2016PG Teaching RRC
Fractures of the olecranon Two broad types of injury are seen: i. Comminuted fracture which is due to a direct
blow or a fall on the elbowii. A transverse break, due to traction when the
patient falls onto the hand while the triceps muscle is contracted.
These two types can be further sub-classified into
i. Displaced fracturesii. Undisplaced fractures. Subluxation or dislocation of the ulno-humeral
joint in severe injuriesThe fracture always enters the elbow joint and
therefore damages the articular cartilage. Sunday,May 1, 2016PG Teaching RRC
Clinical features
A graze or bruise over the elbow suggests a comminuted fracture; the triceps is intact and the elbow can be extended against gravity.
With a transverse fracture there may be a palpable gap and the patient is unable to extend the elbow against resistance.
Sunday,May 1, 2016PG Teaching RRC
TreatmentA comminuted fracture with the triceps intact
should be rested in a sling for a week; then encouraged to start active movements.
An undisplaced transverse fracture that does not separate when the elbow is in flexion can be treated closed.
The elbow is immobilized by a cast in about 60 degrees of flexion for 2–3 weeks and then exercises are begun.
Displaced transverse fracture ORIF is done. The fracture is reduced and held by tension band wiring.
Oblique fractures may need a lag screw, neutralized by a tension band system or plate.Sunday,May 1, 2016PG Teaching RRC
Treatment
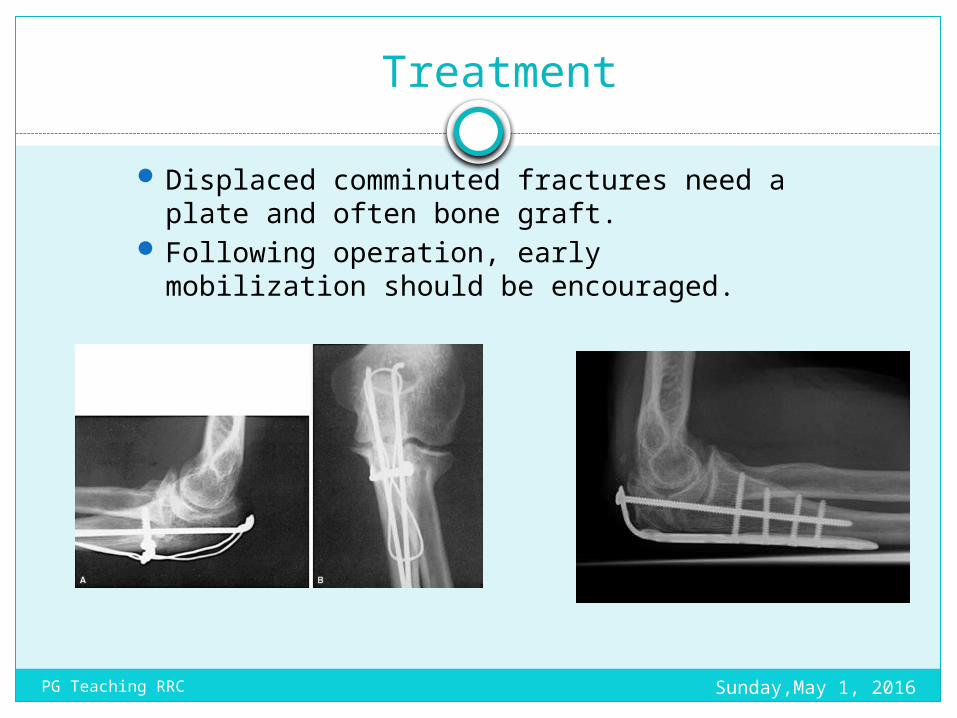
Displaced comminuted fractures need a plate and often bone graft.
Following operation, early mobilization should be encouraged.
Sunday,May 1, 2016PG Teaching RRC
Elbow Infections
Inflammatory
Infective
Tubercular Septic
Olecranon Bursitis
Non Infective
Rheumatoid Others
Sunday,May 1, 2016PG Teaching RRC
Septic arthritis can be caused by bacteria, viruses, and fungi. . The most common causes of septic arthritis are bacteria, including
Staphylococcus aureus and Haemophilus influenzae. In certain "high-risk" individuals, other bacteria may cause septic arthritis,
such as E. coli and Pseudomonas spp.
Risks for the development of septic arthritis include taking immune-suppression medicines, intravenous drug abuse, past joint disease, injury or surgery, and underlying medical illnesses, including diabetes, alcoholism, sickle cell disease, rheumatic diseases, and immune deficiency disorders.
Symptoms of septic arthritis include fever, chills, as well as joint pain, swelling, redness, stiffness, and warmth.
Septic arthritis is diagnosed by identifying infected joint fluid. Septic arthritis is treated with antibiotics and drainage of the infected
joint fluid from the joint.
Sunday,May 1, 2016PG Teaching RRC
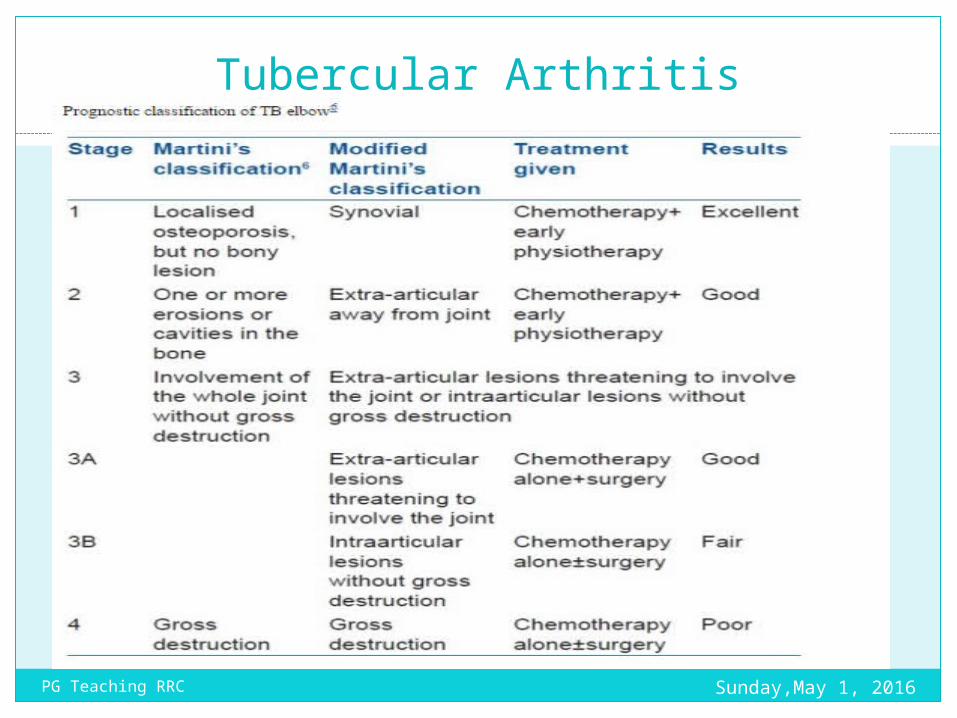
Tubercular Arthritis
Sunday,May 1, 2016PG Teaching RRC
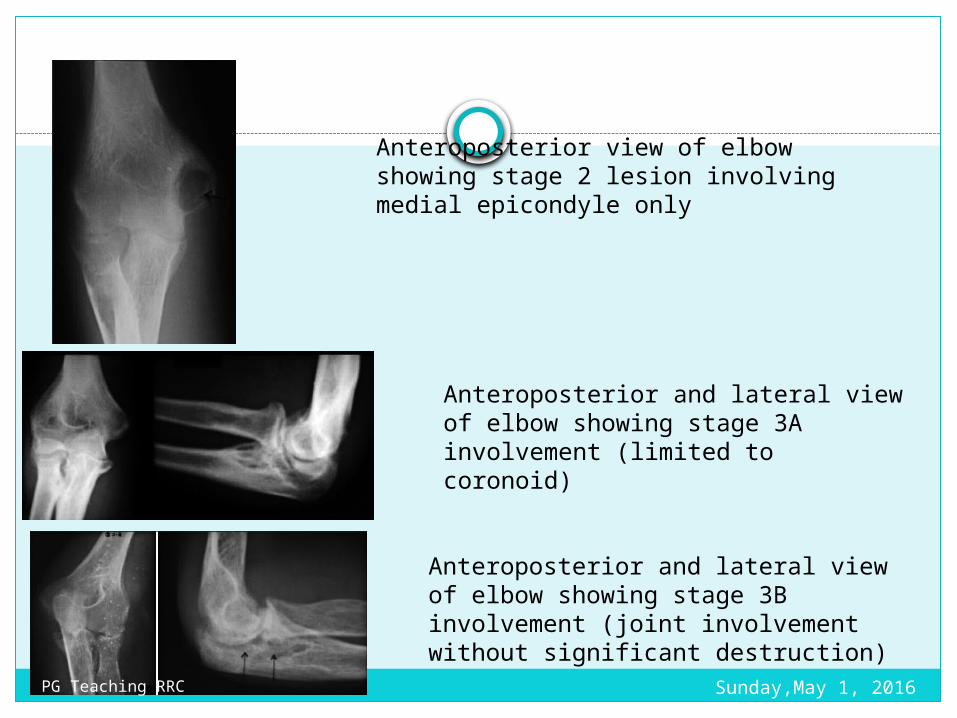
Anteroposterior view of elbow showing stage 2 lesion involving medial epicondyle only
Anteroposterior and lateral view of elbow showing stage 3A involvement (limited to coronoid)
Anteroposterior and lateral view of elbow showing stage 3B involvement (joint involvement without significant destruction)
Sunday,May 1, 2016PG Teaching RRC
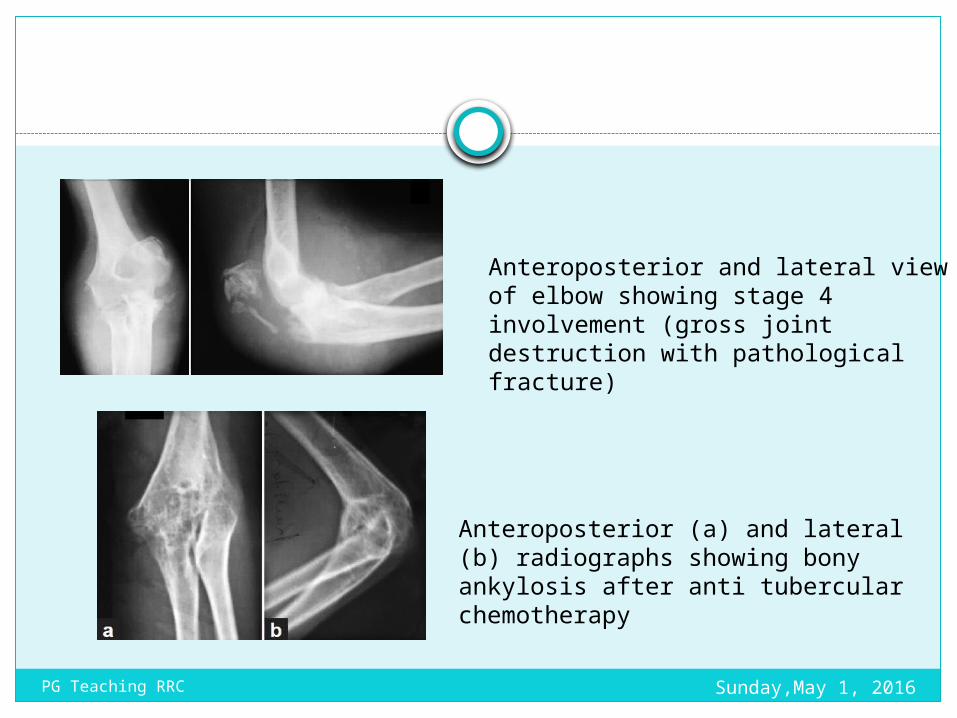
Anteroposterior and lateral view of elbow showing stage 4 involvement (gross joint destruction with pathological fracture)
Anteroposterior (a) and lateral (b) radiographs showing bony ankylosis after anti tubercular chemotherapy
Sunday,May 1, 2016PG Teaching RRC
Sunday,May 1, 2016PG Teaching RRC
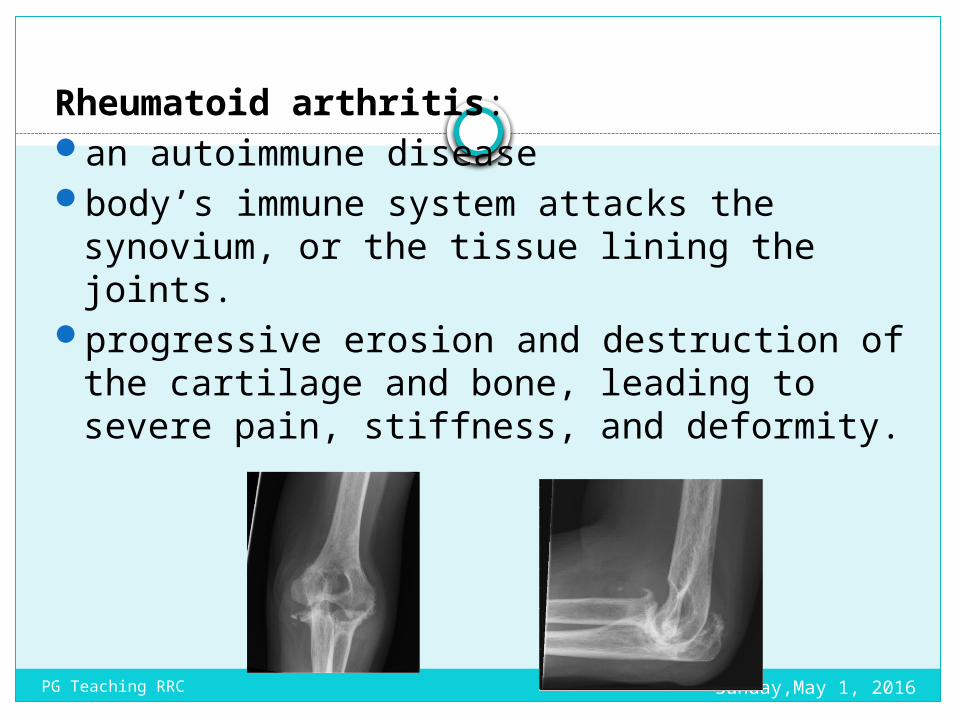
Rheumatoid arthritis: an autoimmune disease body’s immune system attacks the synovium,
or the tissue lining the joints. progressive erosion and destruction of the
cartilage and bone, leading to severe pain, stiffness, and deformity.
Sunday,May 1, 2016PG Teaching RRC
Sunday,May 1, 2016PG Teaching RRC
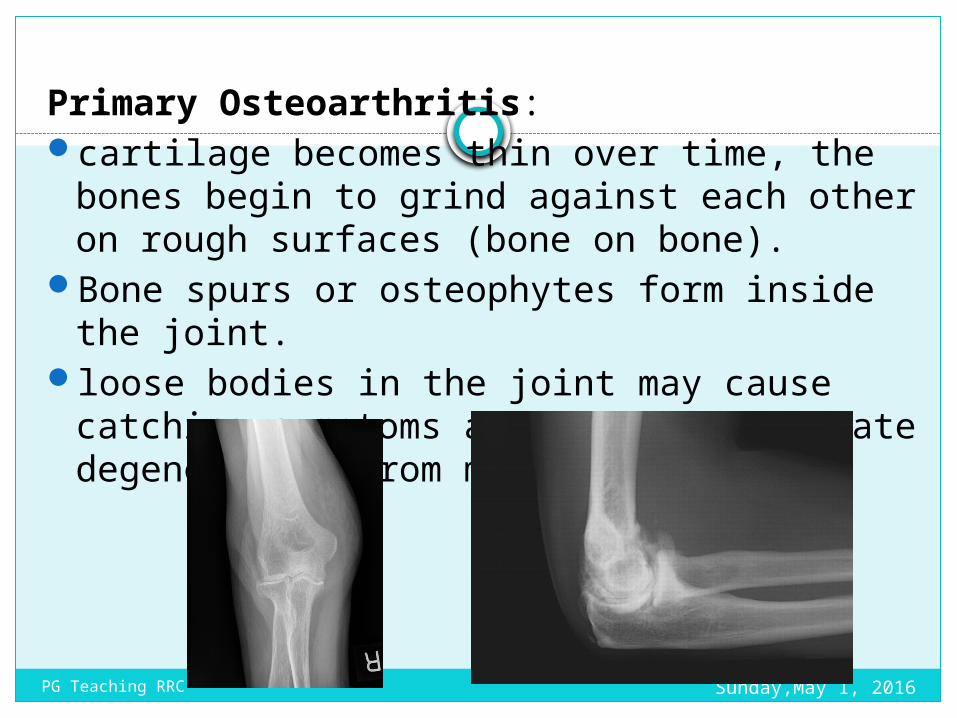
Primary Osteoarthritis: cartilage becomes thin over time, the bones
begin to grind against each other on rough surfaces (bone on bone).
Bone spurs or osteophytes form inside the joint.
loose bodies in the joint may cause catching symptoms as well as accelerate degeneration from mechanical wear.
Sunday,May 1, 2016PG Teaching RRC
Post-traumatic arthritis: One of the most common causes of arthritis Patients with a prior fracture or dislocation of
the elbow can have cartilage injury, leading to progressive deterioration of the joint.
fractures of the distal humerus, radial head fractures, and olecranon fractures. In complex injuries, there are often large cartilage defects and deformities of the elbow, leading to abnormal mechanics and rapid wear of the joint.
Sunday,May 1, 2016PG Teaching RRC
Olecranon bursitisInflammation behind the elbow.
The bursa sac experiences some sort of trauma or blunt force..When it receives a quick blow, it produces more fluid.
Elbow becomes inflamed and swollen.
Elbow will feel hot and be red in color.
Sunday,May 1, 2016PG Teaching RRC
ThanksSunday,May 1, 2016PG Teaching RRC