Embed Size (px)
DESCRIPTION
Citation preview

DYSRHYTHMIASKeepin’ the beat!

Cardiac Cell/Tissue Properties
Automaticity Excitability Conductivity Contractility Refractoriness

Conduction of the Heart

Conduction Pathway

RATES: SA node
› 80–100 bpm Atrial foci
› 60–80 bpm Junctional foci
› 40–60 bpm Ventricular foci
› 20–40 bpm

Lead Placement

The anatomy of an EKG

Measuring an EKG PR interval
0.12 to 0.20 s (3 - 5 small squares)
QRS complex < 0.12 s duration
(3 small squares) QT interval
varies based on rate
QTc=Normal = 0.42 s.
ST segment no elevation or
depression

Determining Rate
Count R waves in 6 sec strip Multiply by 6! What is this heart rate?
3 seconds 3 seconds

Cardiac Output

Common Symptoms Palpitations Dizziness Syncope Chest pain Nausea/vomiting Poor perfusion
› delayed cap refill, cool/clammy extremities, pallor
Hypotension AMS- altered
mental status Cardiac arrest Weakness Fatigue

MANAGEMENT OF DYSRHYTHMIAS
Is patient symptomatic? Stable versus unstable Level of consciousness? Support ABCs Oxygen Monitor ECG, SpO2, blood pressure Identify and treat Determine cause, if possible
Code versus Rapid Response

Sinus Rhythms

Normal Sinus Rhythm
Sinus Tachycardia
Sinus Bradycardia

TREATMENT Sinus Rhythm is normal! Sinus Bradycardia
› Symptoms: loss of consciousness, pallor, dizziness, chest pain, confusion, AMS, hypotension, SOB, orthostatic blood pressure
changes› Atropine› Pacing
external, transvenous, permanent Sinus Tachycardia
› Symptoms: loss of consciousness, pallor, dizziness, chest pain, confusion, AMS, hypotension, SOB
› Normal in some circumstances› Treat the cause› Beta blockers, adenosine (SVT), Ca channel blockers

Ectopic Beats Premature Ventricular contractions (PVC)
Treatment: Symptomatic versus asymptomatic Bigeminy, trigeminy Determine cause (stimulants, dehydration, etc) Beta blockers, ablation

Premature Atrial Contractions

BUNDLE BRANCH BLOCK
RIGHT BBB LEFT BBB

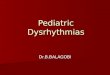
Atrial Fibrillation• Rhythm - Irregularly irregular• Rate - usually 100-160 beats per minute
but slower if on medication• QRS Duration - Usually normal• P Wave - Not distinguishable as the atria
are firing off all over• P-R Interval - Not measurable• The atria fire irregular electrical impulses
causing irregular heart rhythm

Atrial Flutter• Rhythm – Regular (usually)• Rate - Around 110 beats per minute• QRS Duration - Usually normal• P Wave - Replaced with multiple F
(flutter) waves, usually at a ratio of 2:1 (2F - 1QRS) but sometimes 3:1
• P Wave rate - 300 beats per minute• P-R Interval - Not measurableAbnormal tissue generating the rapid heart rate is in the atria

A Fib/ A Flutter Symptoms:
AMS, chest pain, syncope, SOB, hypotension
Long term risk of stroke Treatment:
Rate versus rhythm control (Atrial Kick!) Beta blockers, Ca channel
blockers, synchronized cardioversion , ablation, AV node ablation+pacemaker

FIRST DEGREE AV BLOCK
PR interval > 0.20 seconds Rarely any symptoms or treatment Can be caused by medications (beta
blockers) or be a contradiction to medications Delayed conduction through the AV node

SECOND DEGREE AV BLOCKMOBITZ TYPE 1 / WENKEBACK
• Rhythm - Regularly irregular (P waves, QRS may be irregular)• Rate - Normal or Slow• QRS Duration - Normal• P Wave - Ratio 1:1 for 2,3 or 4 cycles then 1:0.• P Wave rate - Normal but faster than QRS rate• P-R Interval - Progressive lengthening of P-R interval until a QRS complex
is dropped• Increasing delayed conduction through the AV node, eventually resulting
in non conducted beat


SECOND DEGREE AV BLOCK MOBITZ TYPE 2
• Rhythm – Regular (P Waves, QRS will be irregular)
• Rate - Normal or Slow• QRS Duration – may be
prolonged• P Wave - occur
regularly (“march out”)• P-R Interval - Normal or
prolonged but constant• Random lack of
conduction through the AV node


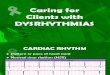
THIRD DEGREE HEART BLOCK or COMPLETE HEART BLOCK

COMPLETE HEART BLOCK
• Rhythm - Regular• Rate - Slow• QRS Duration – Prolonged • P Wave – Unrelated (but “march out”)• P Wave rate - Normal but faster than QRS rate• P-R Interval - Variable• No atrial impulses pass through the atrioventricular node and
the ventricles generate their own rhythm • A/V dissociation


HEART BLOCKS Symptoms:
› similar to bradycardia- SOB, dizziness, LOC, chest pain, pallor, confusion, AMS, hypotension, orthostatic blood pressure
changes Causes:
› Damage to the AV node – MI, scar tissue Second Degree type 2 may lead to complete heart block Complete heart block is rarely stable Treatment: Atropine is not effective (stimulates the SA node which is
usually working, it’s the AV node that’s slowing conduction or not conducting at all)
Pacing- external in emergent situations, transcutaneous or external with sedation if patient is conscious, permanent implanted pacer for long term management

Ventricular Tachycardia
• Rhythm - Regular• Rate - 180-190 Beats per minute• QRS Duration - Prolonged• P Wave - Not seen• Poor cardiac output causes the pt to go into
cardiac arrest. • Shock this rhythm if the patient is
unconscious and without a pulse

Torsades

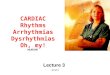
Ventricular Fibrillation
• Rhythm - Irregular• Rate - 300+, disorganized• QRS Duration - Not recognizable• P Wave - Not seen• NO PULSE• Life Threatening Arrhythmia• CPR, DEFIBRILLATE

Ventricular Arrhythmias Causes:
Ischemia, infarction, drugs, hypoxia, electrolytes (Hypo/Hyper)
Treatment:› If unstable, defibrillate› For VT, may synchronize cardiovert› Drugs (ACLS)› Torsades: Magnesium
Determine cause and correct Long term treatment: AICD

Idioventricular

Asystole

Artifact

Pacemakers

Pacemaker and AICD

Dual chamber pacemaker

Things to consider….
Is the rhythm regular? Irregular? Fast? Slow? Is there a P, QRS, T? Easily identifiable?
Is there a P wave for every QRS? What is the PR interval? Does it vary or is it the same? Is the P wave rhythm regular?(do they “march out”?)What is the atrial rate?
What does the ventricular rhythm look like? What is the rate? Fast? Slow?

PR=.20 QRS= .08 Rate: 50’s
PR=.16 QRS= .06 Rate: 70’s

PR= ? QRS= .06 Rate: 100’s
PR= .18 QRS= .08 Rate: 80’s

PR= .18 QRS= .06 Rate: 120’s
PR= ? QRS= .40 Rate: 180’s

PR= .18 QRS= .12 Rate: 80’s Rhythm- multifocal PVC’s
PR= .18 -? QRS= .08 Rate: 180’s Rhythm- SR-PSVT

PR= Varies QRS= .12 Rate: 60’s
PR= ? QRS= .? Rate: ? Rhythm- V- Fib

PR= ? QRS= .10 Rate: 80’s
PR= -? QRS= .20 Rate: 40’s

PR= varies -? QRS= .40 Rate: 40’s
PR= ? QRS= .28 Rate: 40’s

PR= .38 QRS= .08 Rate: 60’s