Embed Size (px)
Citation preview
HOW PATHOLOGY & RADIOLOGY
ORDERING & RESULTS
MANAGEMENT HAS BEEN
IMPROVED AT A 350 BED
CHILDREN'S HOSPITAL
Dr Andrew Blanch
Lead Clinical Champion, OERR project CHQ
14/03/2017

2
How did we get to this point?
3
• What led us to want to improve… Case Scenario
• About us – the organisational context…
• Orders Entry & Results Reporting project approach…
– Governance
– Leadership
– Clinical engagement
– Usability and workflow
– Training
– Patient safety
• Lessons learned…was it a success and would we do it again?
Overview
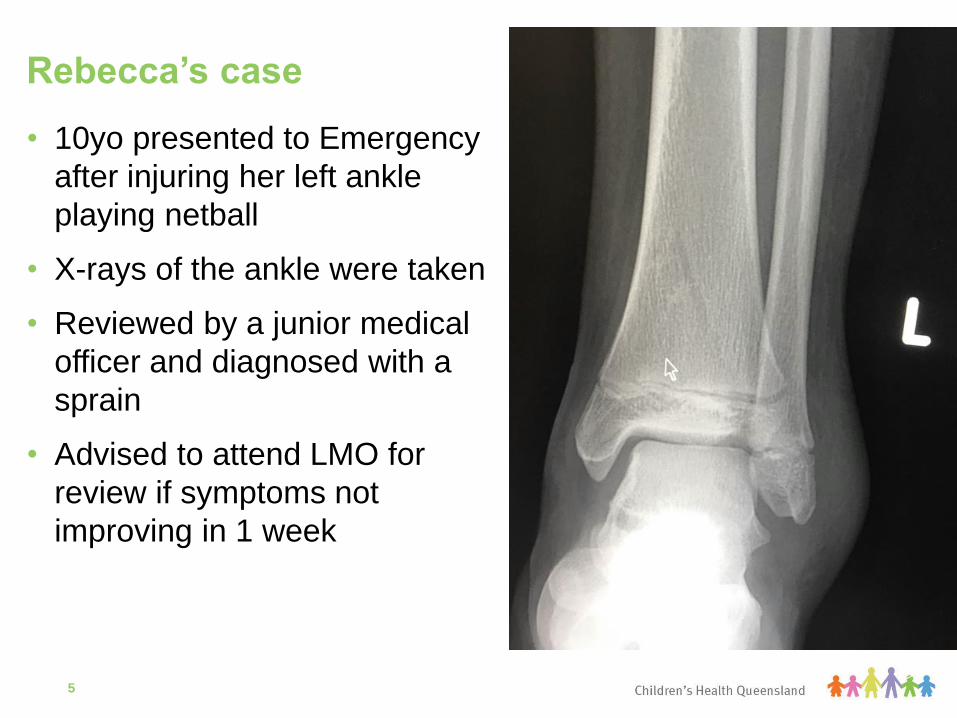
• 10yo presented to Emergency
after injuring her left ankle
playing netball
• X-rays of the ankle were taken
• Reviewed by a junior medical
officer and diagnosed with a
sprain
• Advised to attend LMO for
review if symptoms not
improving in 1 week
Rebecca’s case
5
• Rebecca’s x-ray reviewed by paediatric radiologist 1 day
after ED presentation
– Non-displaced tibial fracture present
• 3 days after ED presentation paper report arrived in ED
• 4 days after ED presentation paper report reviewed and
parents contacted and advised to attend LCCH ED
– Cast applied and follow up arranged in Orthopaedic clinic
Parents asked why it took so long for the right diagnosis
and treatment to be started?
Rebecca’s case
6
• Statewide build, single Cerner ieMR domain
• It is being rolled out in a phased approach
• ieMR is a commercial off the shelf system but with local
configuration.
– Bulk of configuration is at the state level.
• Children’s Health Queensland is one of 6 sites currently using
the ieMR
– Leading the development of the system for use in paediatric
patients
Where does CHQ fit… QHealth eMR Program
7
CHQ ieMR Timeline
8
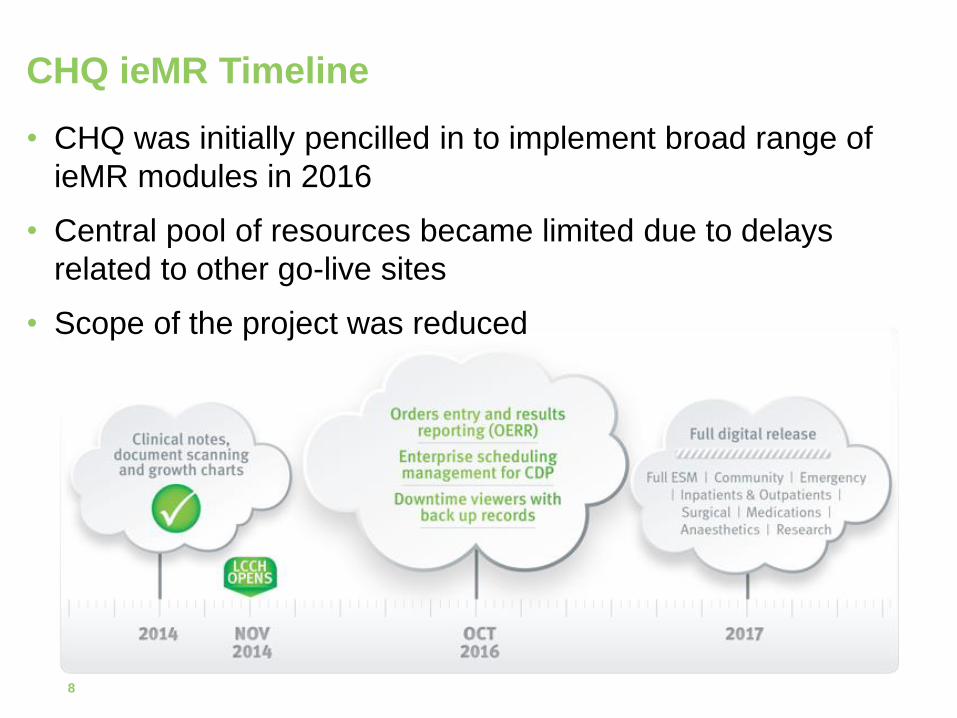
• CHQ was initially pencilled in to implement broad range of
ieMR modules in 2016
• Central pool of resources became limited due to delays
related to other go-live sites
• Scope of the project was reduced
• Governance
• Leadership
• Clinical engagement
• Usability and workflow
• Training
• Patient safety
OERR Project Overview
9
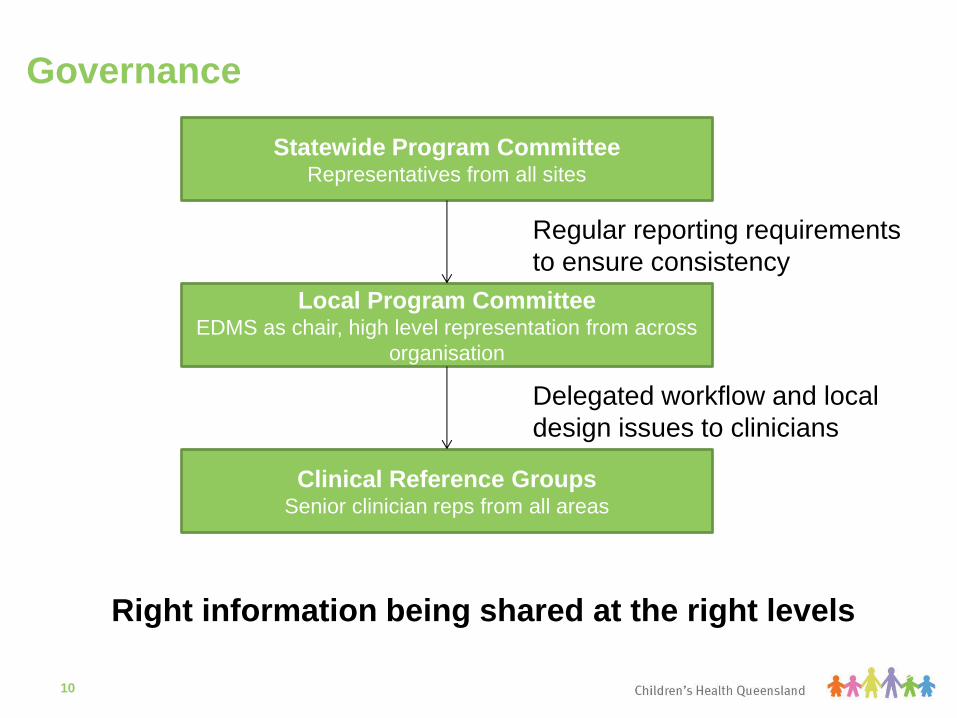
Governance
10
Statewide Program Committee Representatives from all sites
Local Program Committee EDMS as chair, high level representation from across
organisation
Clinical Reference Groups Senior clinician reps from all areas
Regular reporting requirements
to ensure consistency
Delegated workflow and local
design issues to clinicians
Right information being shared at the right levels
• Divisional leadership
– owned the operational impacts on the business
– Readiness checklists (signed off by every service lead)
– Director General visits
• Clinical project staff
– Chosen from across the organisation
– Clinical staff involved in the project had quarantined time
– Subject matter experts were identified with the inclusion of
executive recommendations
o increased the trust and buy-in of executive
Leadership
11
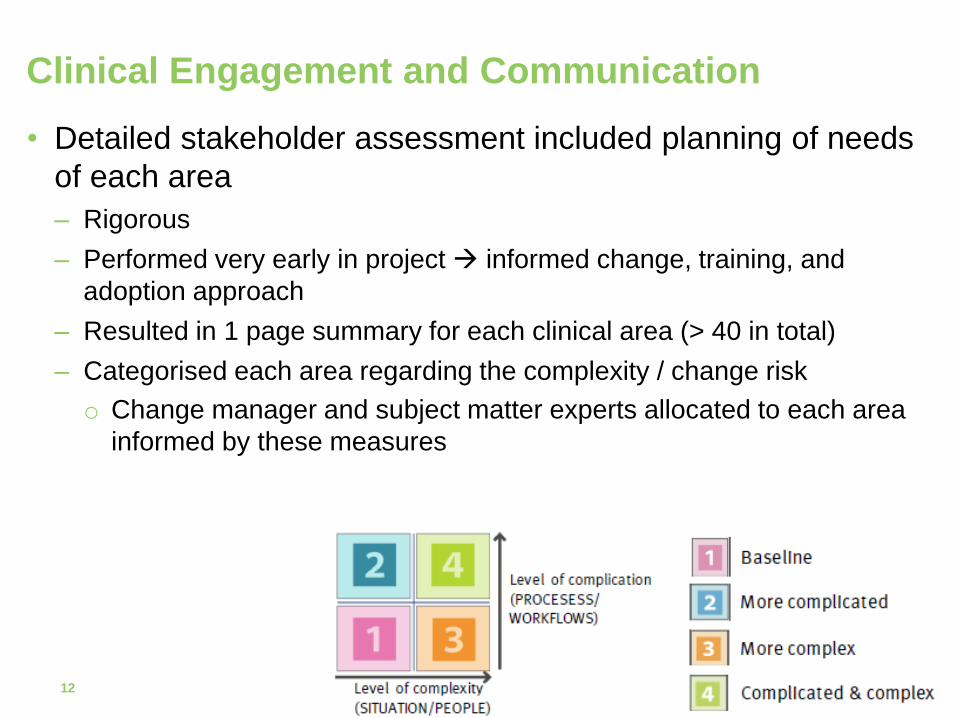
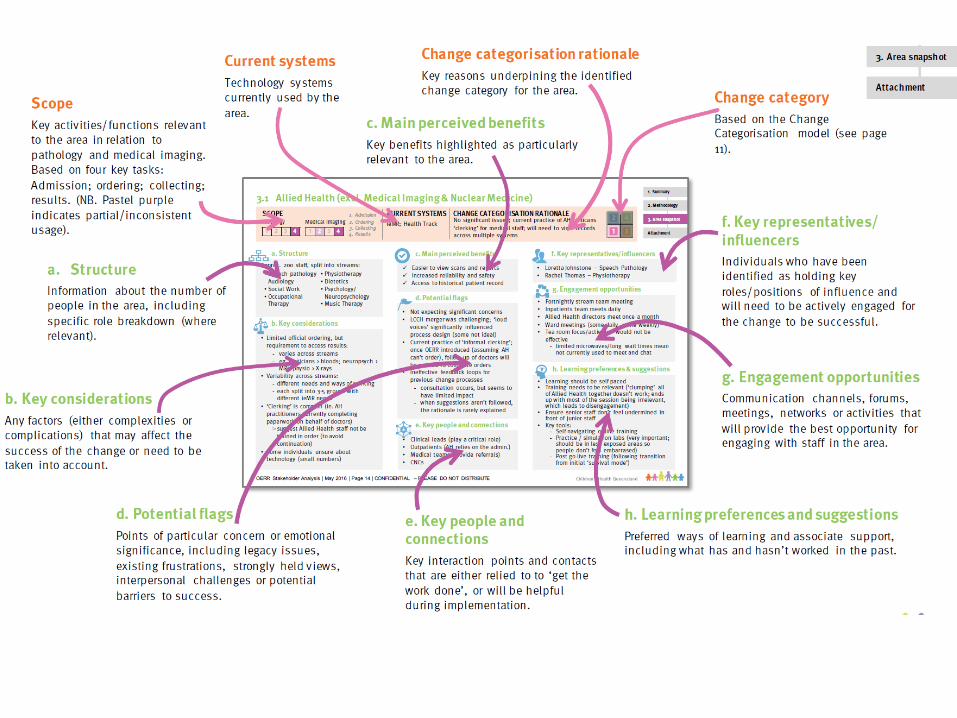
• Detailed stakeholder assessment included planning of needs
of each area
– Rigorous
– Performed very early in project informed change, training, and
adoption approach
– Resulted in 1 page summary for each clinical area (> 40 in total)
– Categorised each area regarding the complexity / change risk
o Change manager and subject matter experts allocated to each area
informed by these measures
Clinical Engagement and Communication
12
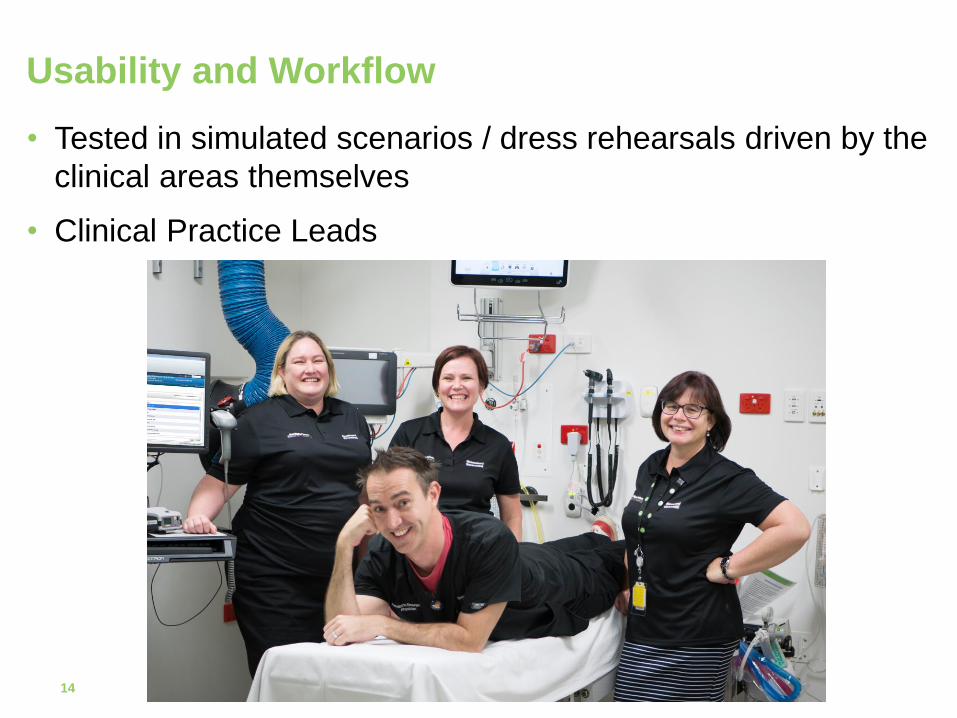
• Tested in simulated scenarios / dress rehearsals driven by the
clinical areas themselves
• Clinical Practice Leads
Usability and Workflow
14

15
• How do you train a large volume of staff quickly?
– Flexible approach – trainers on weekends and nights.
o Multiple training mediums
– Team training sessions
Training
16
• Training dashboards
– Each service / division had visibility of how their team was
tracking regarding training
• The value of “at the elbow” training
– Many people had completed classroom training well before
go-live.
– Floor walkers were available 24 hours a day at go-live.
o someone could be available to support clinicians with
their first order.
Training
17
• Need to be as honest as possible with clinicians about what
the solution is, and what it isn’t
• Stakeholder analysis
– proactively responded to risk areas
– able to provide additional support at go-live
• Roll out over 2 weeks assisted the team to effectively support
high risk areas and high volume areas
• Members of the local patient safety team were embedded
within the project go-live governance
Patient Safety
18
• Rationalisation of committees
– Program Committee became
GOLD meetings
– On the floor support (Floor
Walkers) were supported
through the BRONZE
meetings
• Number of calls for assistance
much lower than planned for:
– Floor walkers were visible
and readily available
o Proactively solved potential
problems
Go Live
19
• Nil clinical incidents related to the roll out.
• All teams across the organisation are using the system for all
pathology orders
– Within 1 week of go-live 90% of orders were within the
ieMR system
• Clinicians felt well supported and informed
• Clinicians like having access to pathology and radiology
results within the medical record
• During a recent planned downtime…we had trouble stopping
clinicians from using the electronic system (significant
hesitance in going back to the paper system)
Go Live and beyond
20
• Resourcing
– Needs to be a mix of subject matter, project management
and technical expertise
– Specialist contractor resources were brought in as required
• Timelines
– Date of go-live was changed to ensure that it didn’t coincide
with school holidays
o However this limited post go-live support
• Hybrid release – Workarounds continue to be required
– Training was able to be focussed on a key eMR
functionality
– It should make the change easier for the next release
Other Lessons Learned
21
• Improved Reliability
– 25% reduction in “No test” rate (unable to complete a
requested test)
o Improved culture of pathology and medical imaging
ordering / collection
– Improved result sign-off
o From less than 30% pre-go live to 90% currently
• The OERR project has tested the organisational readiness for
future releases and has sparked an enthusiasm for more.
– We are much readier for the “BIG” next step because of this
project
Was the pain of implementing OERR alone worth it?
22

Questions…
23




![International Energy ArbitrationJuliet Blanch Juliet Blanch Arbitration London James E. Tancula Mayer Brown LLP Chicago “[The conference] brings together an impressive group of experts](https://img.pdfslide.us/doc/110x75/60b7801f392a8449e9752af8/international-energy-arbitration-juliet-blanch-juliet-blanch-arbitration-london.jpg)