Embed Size (px)
Citation preview

INHERITED CARDIOVASCULAR DISEASE UNIT
Risk Stratification in HCM is Feasible
Using a Clinical Score (PRO)

IT’S DIFFICULT!

1. COMPLEXITY

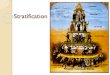
Hypertrophic Cardiomyopathy
Davies M. SGHMS

Hypertrophy
Fibrosis
Disarray
Sarcomeric protein gene mutation
Calcium
transients
Impulse
generation
Impulse
propagation
Modulators:
Fixed:
Genetic
(Histology)
Variable:
Haemodynamics
Ischaemia
Autonomic
Exercise
+ = Ventricular
Arrhythmia
Cell Organ

2. THE DATA

mean n=1238 pts
mean n=176 patients
Young, very symptomatic, ↑ LVOTO
Study marker size is weighted to study cohort size
0.81%

0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Cum
ula
tive S
urv
ival
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years
16 patients (19±8 yrs)
59% (95% CI 33-84)
at 5 years
Elliott P et al JACC 1999; J Am Coll Cardiol 1999;33:1596-601
6.1±4.0 (0.5-14.5)yrs
Secondary prevention

Youth
Genotype
Family History
NYHA III/IV
Exercise capacity
Syncope
Severe LVH
Large gradient
Diastolic dysfunction
Abn Exercise BP
Ischaemia
Atrial fibrillation
Non-sustained VT
Inducible VT/VF
Fractionation
Family History
Syncope
Exercise BP
NSVT
LVH
“Risk Factors”


1.0
0.9
0.8
0.7
0.6
0.5
0.4 0 25 50 75 100 125 150 175
Follow-up (months)
Cu
mu
lative
Su
rviv
al
Log Rank p<0.002
N=630
Elliott PM et al. Lancet 2001;357:420-24
0
2
1
3
Log Rank for Trend p=0.0001

PP Dimitrow et al. EHJ 2010


Principle of risk stratification
5 RF
4 RF
3 RF
2 RF
1 RF
No risk factors
Incre
asin
g r
isk o
f V
F
This is a clinical risk score

LVOTO
Late Gad
Apical Aneurysm
Compound mutations


IS THERE A HIERARCHY OF
RISK FACTORS?

Single Risk
Factor:
O’Mahony C. et al. Heart 2013

CAN WE USE GENETICS/CMR
AS ARBITERS?

Genetics/LGE as predictors of SCD
FH SCD
Syncope
Age
LVOTO
LA size
AF
MWT
NSVT
SCD
LGE
Genetics
?

Complex genotypes and SCD
Double mutations
• Richard et al; Circ 2003 – 7/197 (4%)
– No detailed follow-up data
• Van Driest et al; JACC 2004 – 10/397 (2.5%)
– No detailed follow-up data
• Ingles et al; JMG 2005 – 4/80 (5%)
– All SCD were not genotyped
Triple mutations
• Girolami et al; JACC
2010
– 4/488 (0.8%)
– 2 MWT>30mm
– Outcomes
• 3 dilated LV with HF
with 1 pt having ICD
shocks
• 1 pt aborted SCD

CMR AND SCD RISK PREDICTION

JC Moon et al. JACC 2004

LGE studies and SCD

• 7 centres
• N=1293 but highly selected
• FU 3.3y
• Visual greyscale method (similar to 6SD)

0
.25
.5.7
5
1
No LGE with LGEModel
ROC AUC 95% CI
SCD risk model:
1) %LGE
1) Four conventional SCD
risk factors collapsed as 1
continuous variable
1) maximal LV thickness.

A Flett et al. JACC CVS Imaging 2011

O’Mahony C et al. Eur Heart J. 2014 Aug 7;35(30):2010-20

Major limitation = group prognostication on relative risk
Patient
assessment
0 RF 0.5%/y SCD
1 RF 0.6%/y SCD
↑ risk by 1.4
≥2 RF 1.6%/y SCD
↑ risk by 3.3

O’Mahony C. et al. Heart 2013

CANDIDATE PREDICTORS
Demographic
Age
Historical
Syncope
Family history of SCD
ECG /
Holter
NSVT
Echo
MWT
LV diastolic size
LVOT gradient
LA size
C O’Mahony et al. Circ AE 2013

0
1
2
3
4
5
6Hazard Ratio
O’Mahony C et al. Eur Heart J. 2014 Aug 7;35(30):2010-20

HCM Risk-SCD model for predicting 5 year
risk
O’Mahony C et al. Eur Heart J. 2014 Aug 7;35(30):2010-20

IMPLICATIONS?

Validation: discrimination
• C-index • probability that of a randomly
selected pair of subjects, the
subject with SCD first has the
worse predicted prognosis
• HCM Risk-SCD: 0.70
(95% CI: 0.68, 0.72)
• ACC/ACCF: 0.54
(95% CI: 0.51, 0.56)
0
.25
.5.7
5
1ACCF/AHA 2011 HCM Risk-SCD
C-index 95% CI

5-year SCD probability: 10.9%
5-year SCD probability: 5.1%
Asymptomatic
MWT 25mm
NSVT
LA=45 mm
22 year old
LVOT gradient 70mmHg
56 year old
LVOT gradient 28mmHg

Prevention of Sudden Cardiac
Death
Recommendations for ICD in
each risk category take into
account not only the absolute
statistical risk, but also the
age and general health of the
patient, socio-economic
factors and the psychological
impact of therapy.

Take Home Messages
• Sudden Death is uncommon in patients with HCM
• The risk of SCD can be estimated using simple
non-invasive assessment and HCM RISK-SCD
• Future refinement of risk prediction should be
based on robust modelling and not simply “expert
opinion” alone.


REBUTTAL

“INDIVIDUALS” VERSUS
GROUPS

Majority of
deaths occur in
low risk
populations
BUT
The proportion
of patients at
low risk that die
is very small

N SCD % Annual SCD
≥ 2 RF 412.0 32.0 7.8 1.6
1 RF 1074.0 27.0 2.5 0.5
0 RF 1580.0 25.0 1.6 0.3




• Method #1: Relying on past experience and
training to make an intuitive prediction.
• Method #2: Relying wholly on a statistical
prediction model developed to be used in that
situation.
• Method #3: Taking account of the output of
the statistical prediction model but possibly
modifying it on the basis of professional
experience and intuition.

This study confirms and greatly extends previous reports that
mechanical prediction is typically as accurate or more accurate
than clinical prediction.

No SCD
SCD
No SCD
SCD
Risk of SCD
Risk of SCD
“The impossible dream”


Risk Stratification in HCM is Feasible
Using a Clinical Score
YES

• “We aren’t dealing with groups, we
are dealing with this individual
case.”
• It is doubtful that one can profitably
debate this cliché in a case
conference, since anyone who puts
it quite this way is not educable in
ten minutes.

What will Dr Maron say?
• SCD is a devastating consequence of HCM
• The ICD is life saving
• HCM is a heterogeneous disease and therefore
not suitable for complex “mathematical” solutions

What will Dr Maron say?
And yet…
• We can identify high risk patients using selected
risk factors
• When in doubt do an MRI and all will be clear

Just how unpredictable is HCM?
• LA size is associated with AF and stroke
• End-stage disease has a poor prognosis
• LVOTO responds well to surgery
• Patients over 60 have a lower incidence of SCD
Etc…