Embed Size (px)
Citation preview

Current status and future perspective of management of heart failure in Japan
Hiroaki Shimokawa, MD, PhD.
Heart Failure 2015 (May 23 – 26, 2015 , Seville, Spain)
Joint Session with HFSA and JHFS- Controversial issues in drug therapy -
Chair, Department of Cardiovascular MedicineTohoku University Graduate School of Medicine

COI disclosure
Department of Evidenced-based Medicine Research grants: Daiichi Sankyo, Bayer Yakuhin,
Kyowa Hakko Kirin, Kowa Pharmaceutical Co. ,
Novartis Pharma, Dainippon Sumitomo Pharma,
Nippon Boehringer Ingelheim Co.
Hiroaki Shimokawa, MD, PhD. Lecture fees: Daiichi Sankyo, Bayer Yakuhin, Novartis Pharma.

Paradigm Shift in HF Management- From Treatment to Prevention -
Adopted from AHA/ACCF guideline 2013
Prevention Treatment
Stage-AAt high risk for HF but without
structural hearat disease of
symptoms of HF
Stage-B
Structural heart disease but
without signs or symptoms of HF
Stage-C
Structural heart disease with
prior or current symptoms of HF
Stage-D
Refractory HF requiring
specialized interventions
Neurohormonal Activation1) Renin-angiotensin-aldosterone system 4) Inflammation2) Sympathetic nervous system 5) Arginine vasopressin3) Oxidative stress 6) Endothelin

Chronic Heart Failure Analysis and Registry in the Tohoku District (CHART) Studies
Tohoku Heart Failure AssociationFounded in 1999
ü CHART-1 (N=1,258) Study focus: Prognosis Registration:2000-2004 Follow-up: 2000-2005
ü CHART-2 (N=10,219) Study focus: Prevention, Prognosis
Registration:2006-2010Follow-up: 2006- present
Aomori
AkitaIwate
Yamagata
Miyagi
Fukushima
●Sendai

80
60
40
20
0
(%)
P<0.001
P<0.001
P<0.001
P<0.001
P<0.001
P<0.001
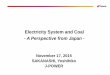
Epidemiologic Transition in Asia
CAD HT DM CAD HT DM
Japan China
2000-2004 (CHART-1)2006-2010 (CHART-2)
1993-19982003-2007
(Sakata, Shimokawa. Circ J. 2014;78:428-435.)

0
10
20
30
40
50
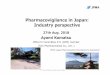
LVEF < 40%
LVEF > 40%
Ischemic heart disease Cardiomyopathy
50
40
30
20
10
0
P < 0.001
CHART-2 (2006-present, N=3,676)
CHART-1 (2000-2005, N=1,006)
Temporal Trends in HF Etiologies
(%)P < 0.001
(Ushigome, Shimokawa, et al. Circ J. 2015, in press)

80
70
60
50
40
30
20
10
0
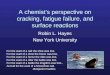
P = 0.006
P < 0.001
P < 0.001
P < 0.001
P < 0.001
RAS-I β-blockers Loopdiuretics Digitalis Aldosterone
antagonists
80
70
60
50
40
30
20
10
0ICD/CRT-D
P = 0.031
(%)
CHART-2 (2006-present, N=3,676)
CHART-1 (2000-2005, N=1,006)
Temporal Trends in Treatments for Symptomatic HF
(Ushigome, Shimokawa, et al. Circ J. 2015, in press)

All-cause death Hospitalization for HF Cardiovascular death
(yrs.)
7563.141
5992,549
4421,771
1,0063,676
(yrs.)
Cum
ulat
ive
inci
denc
e (%
)
1,0063,676
8843,448
7392,893
5682,003
No. at riskCHART-1CHART-2
(yrs.)
8843,448
7392,893
5682,893
1,0063,676
Cum
ulat
ive
inci
denc
e (%
)
Cum
ulat
ive
inci
denc
e (%
)
CHART-2 (N=3,676)
CHART-1 (N=1,006)
CHART-2 (N=3,676)
CHART-1 (N=1,006)
CHART-2 (N=3,676)
CHART-1 (N=1,006)
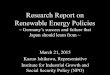
HR 0.59, 95%CI 0.50-0.69; P< 0.001HR※ 0.73, 95%CI 0.59-0.88; P= 0.001
HR 0.38, 95%CI 0.31-0.46; P< 0.001HR ※ 0.45, 95%CI 0.34-0.58; P< 0.001
HR 0.51, 95%CI 0.44-0.58; P< 0.001HR ※ 0.57, 95%CI 0.47-0.68; P< 0.001
A B C
Temporal Trends in Long-term Prognosis of Symptomatic HF Patients
※: Adjusted with age, sex, hypertension, diabetes, dyslipidemia, AF, and VT
(Ushigome, Shimokawa, et al. Circ J. 2015, in press)

1086420
CHART2
CHART1
100%80%60%40%20%0%
Stroke death
Other cardiovascular death
Heart failure death
Sudden cardiac death
(%)0 2 4 6 8 10
P= 0.189
P= 0.285
P= 0.543
0 20 40 60 80 100 (%)
P< 0.001
AMI death
Cardiovascular death
Non-cardiovascular death
Unknown death
P< 0.001
CHART-1(2000-2005)
CHART-2(20006-present)
74%
48%
23%
36%
CHART-2 (2006-Present, N = 3,676)
CHART-1 (2000-2005, N = 1,006)
ATemporal Trends in Mode of Death in Symptomatic HF
(Ushigome, Shimokawa, et al. Circ J. 2015, in press)

•RAS inhibitors
•Beta blockers
•Statins

Prescription Rates of RAS inhibitors by Age
Subjects: 4,733 patients in Stage C/D patients in the CHART-2 Study

Kaplan-Meier Curves for Composite Endpointsin the CHART-2 Study (Stage C/D)
*composite endpoints: all-cause death, HF admission, myocardial infarction and stroke.
(+) RAS inhibitors n=3,421
(-) RAS inhibitors n=1,312
Adjusted HR 1.08 (0.93-1.25), P=0.32

LVEF<40% LVEF40-50% LVEF>50%
Adjusted HR 1.10, P=0.56 Adjusted HR 1.31, P=0.13 Adjusted HR 0.98, P=0.83
β遮断薬あり n=383β遮断薬なし n=213
β遮断薬あり n=1,161β遮断薬なし n=1,485
β遮断薬あり n=465β遮断薬なし n=202
Kaplan-Meier Curves for Composite Endpointsin the CHART-2 study (Stage C/D)
(+) RAS inhibitors n=563(-) RAS inhibitors n=134
(+) RAS inhibitors n=152(-) RAS inhibitors n=58
(+) RAS inhibitors n=2,166(-) RAS inhibitors n=957

The SUPPORT Trial
(Sakata, Shimokawa, et al. Eur Heart J. 2015;36:915-923.)

Study Flow
Hypertensive patients with Stage C/D HF(n = 1147)
Randomization
Control group(n = 569)
Olmesartan group(n = 578)
Excluded (n=1)・lack of information (n=1)
Excluded (n=0)
Control group (n = 568)
Olmesartan group (n = 578)
Enrollment : 2006.10.1 – 2010.3.31
Annual follow-up ( 2013.3.31)~
The SUPPORT Trial
993 (87%) at out-patient clinics.
Titrated up to 40mg/day.
(clinicaltrials.gov-NCT00417222) (Sakata, Shimokawa, et al. Eur Heart J. 2015;36:915-923.)

Control(n=569)
Olmesartan (n=578) P-value
Age, years 65.5 ± 10.1 65.8 ± 10.4 0.445
Males, % 427 (75.2%) 429 (74.2%) 0.71
Body mass index, kg/m2 24.6 ± 4.1 24.2 ± 4.1 0.185
NYHA functional class 0.564
II 530 (93.5%) 535 (92.6%)
III 37 (6.5%) 43 (7.4%)
Baseline cardiovascular disease
Ischemic heart disease 262 (46.1%) 283 (49%) 0.337
Dilated cardiomyopathy 132 (23.2%) 110 (19%) 0.081
Diabetes mellitus 292 (51.4%) 283 (49%) 0.408
Hemodynamics and LV function
Systolic BP, mmHg 127.1 ± 18.0 128.7 ± 18.2 0.081
Diastolic BP, mmHg 73.9 ± 11.7 74.8 ± 12.2 0.311
Heart rate, bpm 71.5 ± 14.6 71.2 ± 13.8 0.808
LVDd, mm 54.0 ± 8.7 53.3 ± 9.0 0.113
LVEF, % 53.7 ± 14.5 54.5 ± 14.9 0.277
Patient CharacteristicsThe SUPPORT Trial
Control (n=569)
Olmesartan (n=578) P-value
Laboratory findings
Hemoglobin (g/dL) 13.7 ± 1.9 13.8 ± 1.7 0.279
Blood urea nitrogen (mg/dL) 18.0 ± 6.9 18.3 ± 7.5 0.556
Creatinine (mg/dL) 0.95 ± 0.36 0.94 ± 0.33 0.956
Albumin (mg/dL) 4.2 ± 0.4 4.2 ± 0.4 0.28
LDL-C (mg/dL) 107.3 ± 30.0 108.2 ± 30.8 0.775
eGFR (mL/min/1.73 m2) 70.4 ± 24.4 70.0 ± 22.6 0.887
BNP (pg/mL) 78.2 (37.8, 173.0) 84.2 (36.7, 188.8) 0.63
Baseline medication
Beta-blocker 416 (73.2%) 405 (70.1%) 0.234
ACE inhibitor 460 (81.0%) 469 (81.1%) 0.946
Diuretics 322 (56.7%) 328 (56.7%) 0.984
Calcium channel blocker 212 (37.3%) 222 (38.4%) 0.705
Statin 274 (48.2%) 287 (49.7%) 0.632
(Sakata, Shimokawa, et al. Eur Heart J. 2015;36:915-923.)

Control 568 513 483 449 317 134 28Olmesartan 578 517 474 436 293 118 47
Cum
ulat
ive
even
t rat
e
29.2% vs.33.2% HR 1.18 (0.96-1.46), P=0.112
Control Olmesartan
No. at risk
(%)
Primary EndpointThe SUPPORT Trial
(Sakata, Shimokawa, et al. Eur Heart J. 2015;36:915-923.)

Primary and Other EndpointsThe SUPPORT Trial
Control (n=568)
Olmesartan
(n=578) Hazard ratio
95% C.I.P-value
events, n (%) events, n (%) lower upper
Primary endpoint 166 ( 29.2 ) 192 ( 33.2 ) 1.183 0.961 1.457 0.112
all-cause death 85 ( 15.0 ) 98 ( 17.0 ) 1.152 0.862 1.541 0.338
non-fatal AMI 8 ( 1.4 ) 12 ( 2.1 ) 1.479 0.604 3.617 0.391
non-fatal stroke 26 ( 4.6 ) 34 ( 5.9 ) 1.313 0.788 2.188 0.296
hospitalization for HF 99 ( 17.4 ) 113 ( 19.6 ) 1.148 0.877 1.504 0.316
Secondary endpoints
CV death 38 ( 6.7 ) 48 ( 8.3 ) 1.258 0.822 1.926 0.290
HF death 18 ( 3.2 ) 10 ( 1.7 ) 0.556 0.257 1.205 0.137
sudden death 8 ( 1.4 ) 18 ( 3.1 ) 2.238 0.973 5.148 0.058
fatal arrythmia 29 ( 5.1 ) 30 ( 5.2 ) 1.017 0.611 1.695 0.947
new-onset DM 60 ( 10.6 ) 70 ( 12.1 ) 1.169 0.828 1.650 0.376
renal dysfunction 61 ( 10.7 ) 97 ( 16.8 ) 1.638 1.189 2.257 0.003
new-onset AF 31 ( 5.5 ) 21 ( 3.6 ) 0.665 0.382 1.157 0.149
Additive use of olmesartan did not improve clinical outcomes but worsened renal
function in hypertensive CHF patients treated with evidence-based medications.
(Sakata, Shimokawa, et al. Eur Heart J. 2015;36:915-923.)

P=0.588 HR=1.12(0.75, 1.66)
Control 104 95 88 80 59 37 8
Olmesartan 106 101 96 90 65 43 43
P=0.118 HR=0.66(0.39, 1.12)
C. (+)ACEI, (+)BBA. (+)ACEI, (-)BB B. (-)ACEI, (+)BB
ControlOlmesartan
Cum
ulat
ive
even
t rat
e
Cum
ulat
ive
even
t rat
e
Cum
ulat
ive
even
t rat
eControlOlmesartan
ControlOlmesartan
(%)(%) (%)
Control 312 286 270 251 168 68 45
Olmesartan 299 261 233 211 140 93 30
P=0.006 HR=1.47(1.11, 1.95)
Control 148 130 124 117 96 55 7
Olmesartan 170 154 144 135 92 37 37
Number at risk
Number at risk
Number at risk
Baseline Medications and the Primary EndpointThe SUPPORT Trial
(Sakata, Shimokawa, et al. Eur Heart J. 2015;36:915-923.)

Primary Endpoint Overall
(+) ACEI, (-) BB
(-) ACEI, (+) BB
(+) ACEI, (+) BB
Olmesartanbetter worse
HR 4.03.53.02.52.01.51.00.50.0
All-cause Death Overall
(+) ACEI, (-) BB
(-) ACEI, (+) BB
(+) ACEI, (+) BB
Olmesartanbetter worse
HR4.03.53.02.52.01.51.00.50.0
Renal Dysfunction Overall
(+) ACEI, (-) BB
(-) ACEI, (+) BB
(+) ACEI, (+) BB
Olmesartanbetter worse
HR 4.03.53.02.52.01.51.00.50.0
ACEI: ACE inhibitorsBB: Beta blockers
Triple Combination and Adverse Cardiac EventsThe SUPPORT Trial
(Sakata, Shimokawa, et al. Eur Heart J. 2015;36:915-923.)

•RAS inhibitors
•Beta blockers
•Statins

Prescription of Beta-blockers in the CHART-2 Study
Carvedilol 67.5% Bisoprolol 9.0%Metoprolol 5.1%Unknown 18.4%
Subjects: 4,733 patients in Stage C/D patients in the CHART-2 Study

30歳未満 40歳以上50歳未満60歳以上70歳未満 80歳以上
0
20
40
60
80
100
30歳未満 40歳以上50歳未満60歳以上70歳未満 80歳以上
0
20
40
60
80
100
Prescription Rates of Beta-blockers by Age
0
20
40
60
80
100 (%)
0
20
40
60
80
100 (%)
CHART-1 (N=1,006) CHART-2 (N=3,673)
<30 30-39 40-49 50-59 60-69 70-79 80< <30 30-39 40-49 50-59 60-69 70-79 80<
Age Age

Dose of Carvedilol in the CHART-2 Study
30歳未満30歳以上40歳未満40歳以上50歳未満50歳以上60歳未満60歳以上70歳未満70歳以上80歳未満80歳以上
0
2
4
6
8
10
12
0
2
4
6
8
10
(mg)12
全体 男性 女性
0
2
4
6
8
10
12
0
2
4
6
8
10
(mg)12
All Male Female <30 30-39 40-49 50-59 60-69 70-79 80<
Age
Subjects: 1,817 patients in Stage C/D patients in the CHART-2 Study

(+) Beta blockers n=2,009(-) Beta blockers n=1,900
(%)
Time (Year)
0 1 2 3 4
Kaplan-Meier Curves for All-cause Deathin the CHART-2 Study (Stage C/D)
Adjusted HR 0.80 (0.72-0.90), P<0.001
100
60
80
20
40
0
Sur
viva
l rat
e

LVEF<40% LVEF40-50% LVEF>50%
Adjusted HR 0.48, P<0.001 Adjusted HR 0.80, P=0.15 Adjusted HR 1.01, P=0.86
(%)
100
80
60
40
20
0
(%)
100
80
60
40
20
0
(%)
100
80
60
40
20
0
β遮断薬あり n=383β遮断薬なし n=213
β遮断薬あり n=1,161β遮断薬なし n=1,485
β遮断薬あり n=465β遮断薬なし n=202
0 1 2 3 4 0 1 2 3 4 0 1 2 3 4
Kaplan-Meier Curves for All-cause Deathin the CHART-2 study (Stage C/D)
(+) Beta-blockers n=465(-) Beta-blockers n=202
Time (Year)
Sur
viva
l rat
e
Time (Year) Time (Year)(+) Beta-blockers n=383(-) Beta-blockers n=213
(+) Beta-blockers n=1,161(-) Beta-blockers n=1,485

Prognostic Impacts of Beta-blockers in Stage C/D Patients with Sinus Rhythm
HFrEF(N=885)
HFpEF(N=1,803)
(Takada, Shimokawa, et al. Eur J Heart Fail. 2014;16:309-316.)
Beta-blockersbetter worse
HR
Beta-blockersbetter worse
HR

All-cause death Hospitalization for HF
CHART-1 (n=306)
Log-rank P= 0.010
CHART-2 (n=710)
(years)
Log-rank P= 0.015
(years)
CHART-1 (n=306)
CHART-2 (n=710)
(%) (%)
Sur
viva
l rat
e
Hos
pita
lizat
ion-
free
rate
306710
281666
247570
189406
306710
245611
209496
156346
HR 0.60, 95%CI 0.49-0.81; P= 0.011
HR 0.69, 95%CI 0.51-0.93;P= 0.015
No. at riskCHART-1CHART-2
No. at riskCHART-1CHART-2
DCM: Kaplan-Meier Survival Curves
(Ushigome R, Shimokawa H, et al. Circ J. 2015;79:1332-1341.)

6
Stroke death
Other death
Heart failure death
Sudden cardiac death
Non-cardiovascular death
100%80%60%40%20%0%
51.6 84.1
37.1 11.4
(%)
CHART-1
CHART-2
Cardiovascular death
Non-cardiovascular death
Unknown death
CHART-1
CHART-2
0 1 2 3 4 5
P= 0.526
P= 0.107
P= 0.257
0 20 40 60 80 100 (%)
P< 0.001
P= 0.062
84%
52%
DCM: Mode of Death
(Ushigome R, Shimokawa H, et al. Circ J. 2015;79:1332-1341.)

(%)
Surv
ival
rate
CHART-1 (n=147)
CHART-2 (n=567)
(years)
(%)
Surv
ival
rate
Log-rank P= 0.851
CHART-1 (n=159)
CHART-2 (n=143)
HR 0.94, 95%CI 0.53-1.71; P= 0.850
(years)
159143
147133
131109
11584
No. at riskCHART-1CHART-2
147567
135534
116468
79343
No. at riskCHART-1CHART-2
(+) Beta-blocker(-) Beta-blocker
Beta-blockers in DCM Patients
Log-rank P= 0.017
HR 0.53, 95%CI 0.31-0.90;P= 0.019
(Ushigome R, Shimokawa H, et al. Circ J. 2015;79:1332-1341.)

•RAS inhibitors
•Beta blockers
•Statins

Selection of HFpEF Populations
Total cohort
Matched cohort
Required past or current symptoms of HF
(Nochioka, Shimokawa, et al. Circ J. 2015;79:574-582.)

Kaplan-Meier Curves for All-cause Death in HFpEF
(Nochioka, Shimokawa, et al. Circ J. 2015;79:574-582.)

No. at risk Matched cohort No statin use Statin use Total cohort No statin use Statin use
207207
555863
Cum
ulat
ive
Inci
denc
e (%
)
193194
529769
163166
451648
106119
320441
00
No statin use in total HFrEF cohort
No statin use in matched HFrEF cohort
Statin use in total HFrEF cohort
Statin use in matched HFrEF cohort
P=0.970 for matched HFrEF cohort
P=0.001 for total HFrEF cohort
10
20
30
1 2 3 Years
Kaplan-Meier Curves for All-cause Death in HFrEF
Statin use was not associated
with improved mortality in the PS-matched HFrEF population.
(Nochioka, Shimokawa, et al. Circ J. 2015;79:574-582.)

Statin use in the total cohort
PTotal Yes No
n=3,124 n=1,163 n=1,961 HR 95%CIAll-cause death 440 113 327 0.72 0.63-0.82 <0.001 Cardiovascular 210 64 146 1.01 0.83-1.22 0.960 Heart failure 97 28 69 1.16 0.88-1.53 0.288 Sudden death 40 12 28 0.59 0.36-0.98 0.041 Stroke 25 11 14 1.25 0.72-2.15 0.426 MI 11 3 8 0.61 0.27-1.38 0.234 Other cardiovascular 37 10 27 1.07 0.68-1.64 0.758 Non-cardiovascular 206 47 159 0.53 0.62-0.82 <0.001 Cancer 75 22 53 0.74 0.53-1.03 0.078 Infection 67 14 53 0.53 0.36-0.77 0.001 Renal failure 18 5 13 0.73 0.36-1.47 0.371 Gastrointestinal bleeding 4 0 4 0.00 - - Other non-cardiovascular 42 6 36 0.21 0.11-0.39 <0.001 Unknown cause 24 2 22 0.17 0.01-0.42 <0.001
*P value is the results of the Cox hazard models adjusted by IPTW.
Mode of death in HFpEF
(Nochioka, Shimokawa, et al. Circ J. 2015;79:574-582.)

HR 95% CI P value
β-blockers CHART-1 0.96 ( 0.63 - 1.44 ) 0.829 CHART-2 0.82 ( 0.68 - 1.00 ) 0.055
RAS-I CHART-1 0.79 ( 0.55 - 1.14 ) 0.208 CHART-2 0.94 ( 0.76 - 1.15 ) 0.534
Aldosterone antagonists
CHART-1 1.36 ( 0.89 - 2.07 ) 0.154 CHART-2 1.14 ( 0.93 - 1.39 ) 0.223
Loop diuretics CHART-1 1.72 ( 1.03 - 2.87 ) 0.038 CHART-2 1.29 ( 1.05 - 1.59 ) 0.017
Digitalis CHART-1 0.97 ( 0.69 - 1.38 ) 0.875 CHART-2 1.06 ( 0.87 - 1.31 ) 0.555
CCB CHART-1 1.32 ( 0.92 - 1.90 ) 0.135 CHART-2 0.91 ( 0.75 - 1.12 ) 0.376
Statin CHART-1 NA NA NACHART-2 0.81 ( 0.65 - 1.02 ) 0.068
Effects of Medications in Symptomatic HF Patients
All patients, All-cause death
※: Adjusted with age, sex, hypertension, diabetes, dyslipidemia, AF, and VT

HR 95% CI P value
β-blockers CHART-1 0.87 ( 0.50 - 1.50 ) 0.610 CHART-2 0.59 ( 0.44 - 0.81 ) 0.001
RAS-I CHART-1 0.67 ( 0.40 - 1.12 ) 0.128 CHART-2 0.83 ( 0.60 - 1.15 ) 0.252
Aldosterone antagonists
CHART-1 1.39 ( 0.80 - 2.43 ) 0.247 CHART-2 1.23 ( 0.91 - 1.66 ) 0.172
Loop diuretics CHART-1 1.63 ( 0.78 - 3.41 ) 0.192 CHART-2 1.30 ( 0.91 - 1.85 ) 0.147
Digitalis CHART-1 0.99 ( 0.61 - 1.61 ) 0.978 CHART-2 1.10 ( 0.80 - 1.51 ) 0.558
CCB CHART-1 1.40 ( 0.82 - 2.38 ) 0.213 CHART-2 1.09 ( 0.77 - 1.54 ) 0.618
Statin CHART-1 NA NA NA CHART-2 0.84 ( 0.60 - 1.17 ) 0.299
Effects of Medications in Symptomatic HFrEF Patients
HFrEF, All-cause death
※: Adjusted with age, sex, hypertension, diabetes, dyslipidemia, AF, and VT

HR 95% CI P value
β-blockers CHART-1 0.89 ( 0.45 - 1.75 ) 0.734 CHART-2 0.94 ( 0.73 - 1.22 ) 0.654
RAS-I CHART-1 0.86 ( 0.51 - 1.47 ) 0.592 CHART-2 1.01 ( 0.77 - 1.32 ) 0.924
Aldosterone antagonists
CHART-1 1.32 ( 0.67 - 2.61 ) 0.423 CHART-2 0.96 ( 0.72 - 1.29 ) 0.808
Loop diuretics CHART-1 1.50 ( 0.72 - 3.11 ) 0.281 CHART-2 1.17 ( 0.90 - 1.52 ) 0.251
Digitalis CHART-1 0.92 ( 0.55 - 1.54 ) 0.764 CHART-2 1.07 ( 0.81 - 1.41 ) 0.632
CCB CHART-1 1.31 ( 0.77 - 2.24 ) 0.321 CHART-2 0.84 ( 0.65 - 1.08 ) 0.173
Statin CHART-1 NA NA NACHART-2 0.72 ( 0.53 - 0.98 ) 0.035
HFpEF, All-cause death
Effects of Medications in Symptomatic HFpEF Patients
※: Adjusted with age, sex, hypertension, diabetes, dyslipidemia, AF, and VT

Conclusions
1. Along with implementation of evidence-based medications, 3-year incidences of all-cause death, cardiovascular death and HF admission have been decreased in patients with HF in Japan.
2. Better implementation of beta-blockers and statins appears to have contributed to this prognostic improvement in patients with HFrEF and those with HFpEF, respectively.

Department of Cardiovascular Medicine, Tohoku University Graduate School of Medicine
Acknowledgements
Tohoku Heart Failure Society