Embed Size (px)
Citation preview
Controversies and agreements in
the interface between social
enterprise and health
Cam Donaldson
Yunus Chair in Social Business & Health
Glasgow Caledonian University
Presented at Fuse Quarterly Research Meeting
26th January 2016
Outline • Moving upstream:
• From third to fifth wave…
• …and in-between
• The place of social enterprise:
• Including a bit about Muhammed Yunus
• What is social enterprise?
• Why do we need to evidence it?
• ‘Evidencing’ it: Why? How? Challenges
• Social finance
28 years
How do we get to the ‘causes of the causes’?
‘Banker to the Poor’
• 1965: Fulbright Scholar
• 1971: Economics PhD from Vanderbilt
• Post Liberation War: returns to Bangladesh to work in government under Nurul Islam and then becomes Head of Economics, at Chittagong University
• 1976: Lends $27 of his own money to inhabitants of Jobra Village
• 1983: Grameen Bank (Village Bank)
• Late 90s–early 00s: Grameen II
• 2006: Nobel Peace Prize jointly awarded to Yunus and Grameen
• Later in ’00s: Social Business
• 2010: Controversies…
• 2012…
Social enterprise: venturing a definition
• Primary purpose for the common good:
– addressing social vulnerability
• Trading is main source of income:
– actual or aspiring to
• Profits used for social/community benefit:
– not individual benefit
• Assets locked or held for common benefit
• Approach includes being a good employer, democratic, empowering communities, co-operation, social justice
What we are not about
• Replacing the NHS
• Replacing public health
• Promoting benefit cuts
• Corporate social responsibility
But, ‘new relationship’ with government in:
• Not only service provision
• But also something much more pervasive than that
• May require subsidisation (e.g. HealthWORKS)
And recognising that:
• Again, long traditions in European countries
• The interest is in social vulnerability and ‘bottom-up’

Passage from India
Why do we need to ‘evidence’ it?
• Are organisations doing what they claim to
do?...
• …and what other wider societal benefit
might they engender?
Why do we need to ‘evidence’ it?
• Are organisations doing what they claim to
do?...
• …and what other wider societal benefit
might they engender?
• Seeking government attention…
• …and perhaps government resources
Why do we need to ‘evidence’ it?
• Are organisations doing what they claim to
do?...
• …and what other wider societal benefit
might they engender?
• Seeking government attention…
• …and perhaps government resources
But, most importantly…
• Communities themselves
How do we evidence it? People and studies
• 3 to 35 people in 5 years; 11 PhDs:
– Staff, students and interns from Austria, Bangladesh, Canada, China, Egypt,
France, Greece, Italy, Malaysia, Poland, South Africa, Spain
• Studentships: University; international awards; self-funding
• Develop people and disciplines: social sciences, health sciences, humanities
• Smaller studies (funded by Scottish Funding Council) with specific social
enterprises (e.g. Theatre Nemo; WeeEnterprisers)
• Other small grants (£30,000 from Santander Bank; £38,000 from Glasgow
Council for the Voluntary Sector)
• Then some ‘biggies’:
– MRC/ESRC, £1.96m, ‘Developing methods for evidencing social enterprise
as a public health intervention’ (CommonHealth)
– European Commission, €3.17m [€333,425 to GCU], ‘Enabling the flourishing and evolution of social entrepreneurship for innovative and inclusive societies’ (EFESEIIS)
– Chief Scientist Office of Scottish Government’s Health Department, £211,000, ‘Fair credit, health and wellbeing: eliciting the perspectives of low-income individuals’ (FInWell)

The CommonHealth collaboration
How do we evidence it?
• Conceptualisation
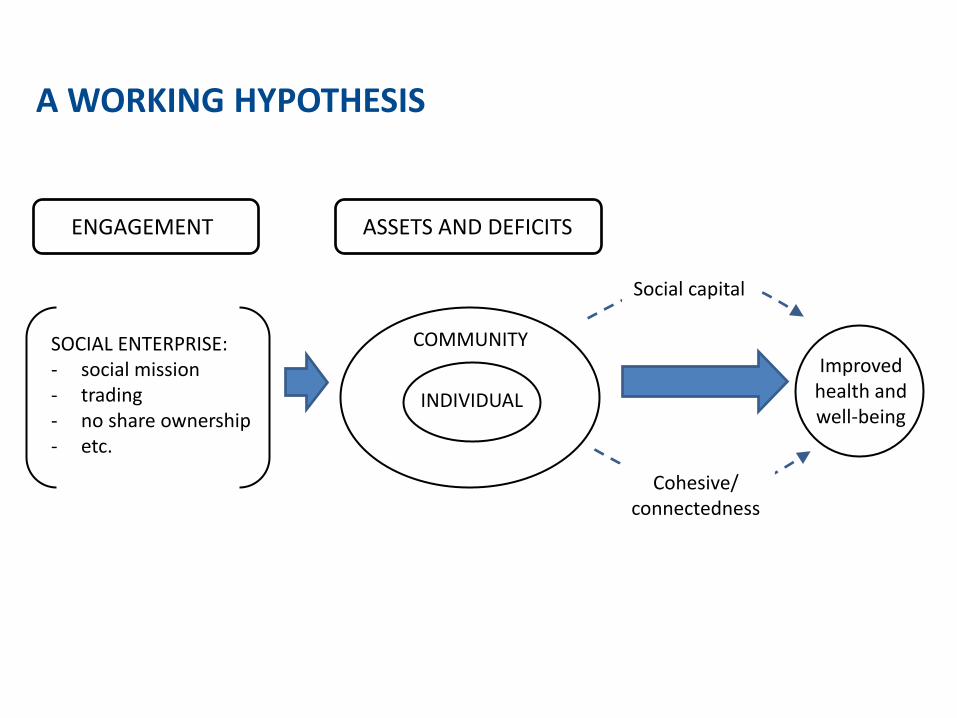
A WORKING HYPOTHESIS
SOCIAL ENTERPRISE: - social mission - trading - no share ownership - etc.
ENGAGEMENT
COMMUNITY Improved
health and well-being
ASSETS AND DEFICITS
INDIVIDUAL
Social capital
Cohesive/ connectedness
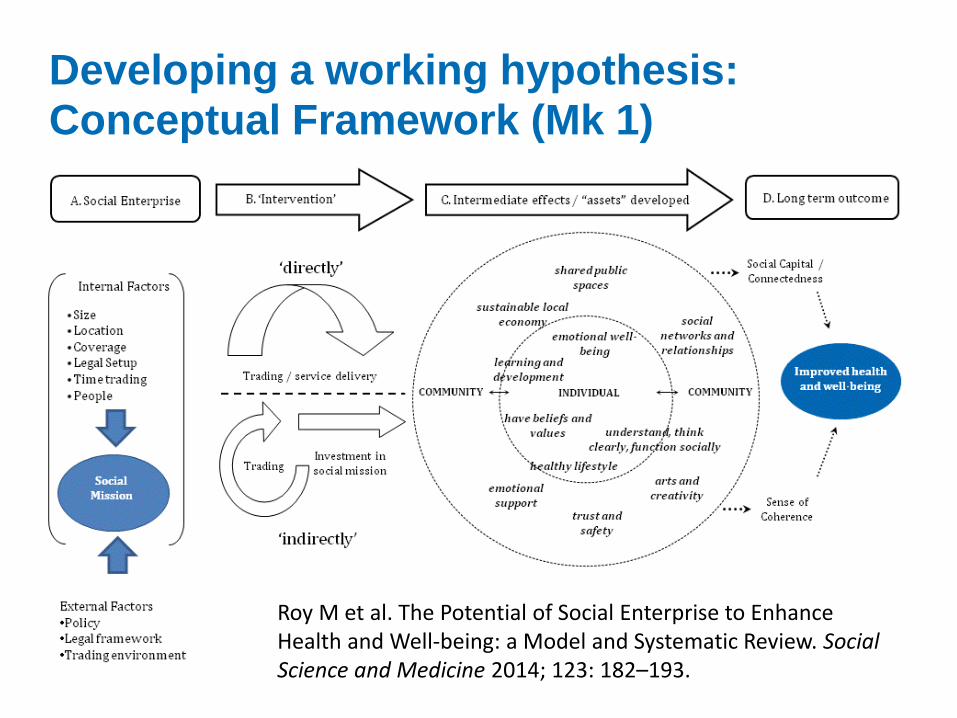
Developing a working hypothesis: Conceptual Framework (Mk 1)
Roy M et al. The Potential of Social Enterprise to Enhance Health and Well-being: a Model and Systematic Review. Social Science and Medicine 2014; 123: 182–193.
How do we evidence it?
• Conceptualisation
• Systematic review: – Social enterprise:
• as a public health initiative (Roy et al. again!)
• as an alternative provider of (community health) services
• in specific roles (preventing homelessness and social isolation)
– Microcredit: • short and longer-term impacts on health
How do we evidence it?
• Conceptualisation
• Systematic review: – Social enterprise:
• as a public health initiative (Roy et al. again!)
• as an alternative provider of (community health) services
• in specific roles (preventing homelessness and social isolation)
– Microcredit: • short and longer-term impacts on health
– Challenges of systematic review: • lack of studies; heterogeneity; comparators
How do we evidence it?
• Conceptualisation
• Systematic review
• Populate the model: – Qualitative research:
• Interviews with clients, employees, executives, policy-makers
• Embedded within organisations (‘Passage from India’)
• Financial diaries with microcredit clients
• Q methodology
– Comparative studies: • How do social enterprise clients compare with those in other
settings? (homelessness; social isolation; community-based chronic disease management)
How do we evidence it?
• Conceptualisation
• Systematic review
• Populate the model: – Challenges with primary research:
• generalisability; comparator groups; retention
What is social finance? • Monetary investment in a social policy objective
– Investor get financial return whilst public services are delivered
• Conventional view: trying to bring the discipline and resources of private investment to more ‘social’ goods
• Associated with: – debt crisis – drive to greater efficiency – outcomes-based financing
• Social investment market worth £190m in UK in 2010: – Likely worth a lot more if we include earlier ‘Private Finance Initiative’ – ‘Big Society Capital’, ‘Inspiring Scotland’, ‘Social Investment Scotland’ – Win-win: “opening up serious resources to tackle social problems in new and innovative
ways” (Nick Hurd, UK Minister for Civil Society, 2012) – Cabinet Office Centre for Social Impact Bonds
• Most famous example = HMP Peterborough: – Short-sentenced prisoners (less than one year) – Investor receives 2.5% return if 7.5% reduction in reoffending is achieved, relative to a
control group – Higher rates of reduction trigger higher returns up to maximum 13.3% – Met targets, but suspended!
Two papers by GCU Yunus Centre staff:
McHugh N, Sinclair S, Roy MJ, Huckfield L and Donaldson C. Social Impact Bonds: A Wolf in Sheep’s Clothing? Journal of Poverty and Social Justice, 2013; 21: 247-257.
Sinclair S, McHugh N, Huckfield L, Roy MJ and Donaldson C Social Impact Bonds: Shifting the Boundaries of Citizenship, Social Policy Review 26: Analysis and Debate in Social Policy 2014: 119–136.
Challenges • Measurement and attribution of social outcomes • Unintended consequences:
– Contract terms vs needs – Provider types
• Size and ‘investment readiness’: – ‘shadow state’ – ‘social enterprise readiness’
• Governance: – One less link in democratic accountability
• Further questions about the role of the market – Distortion of social priorities
• Everything is an ‘asset’: an ideological shift • But…evidence…’Ways to Wellness’

Keeping in touch
Yunus Centre for Social Business & Health – http://www.gcu.ac.uk/yunuscentre/ – Email: [email protected]
• Website: – http://www.commonhealth.uk/
• Blog: – https://commonhealthresearch.wordpress.com/