Embed Size (px)
Citation preview

A Whirlwind Tour of Skin/Soft Tissue Infections
Steven P. LaRosa, M.D.Division of Infectious Disease
Beverly [email protected]

Disclosure InformationSteven P. LaRosa, M.D.
• I have received fees as a member of the Scientific Advisory Board for the following companies:– Leading Biosciences– SciClone, Inc.– Atox Bio– ExThera Medical
• Consultant:– Cubist→Merck – Daptomycin, Tedizolid

THE USUAL



Patients Prone to Group A Strep Cellulitis
• Prior LN resection or irradiation (Breast CA, Vulvar CA)
• H/O SVG harvesting for CABG• H/O Lymphedema

Non-culturable cellulitis(no purulent material or wound present)Suspected organisms: β-hemolytic strep, S. aureus
Cefazolin 1 g IV q8h (<80kg), 2 g IV q8h (>80kg)
Oxacillin 2 g IV q4h Unasyn 3gms IV q 6h Penicillin allergy: clindamycin 600 mg
IV q8h (ID approval required), vancomycin 15 mg/kg IV q12h
If culture documented streptococcal infection: Aqueous PCN G 2 MU IV q4h

DO YOU NEED TO HAVE MRSA COVERAGE FOR UNCOMPLICATED CELLULITIS?

Uncomplicated Cellulitis
• Randomized, Multi-center, double blind, placebo-controlled study
• Evidence of cellulitis• Exclusions:
– DM– PVD– Hospital admission required– > 1 cc purulence– Immunocompromised or pregnant

III. Antibiotic dosing
Weight Cephalexin
Trimethoprim-sulfamethoxazole (mg trimethoprim)
Children <30 kg: 15–19 kg: 300 mg 4 times daily 40/200 mg qid 20–24 kg: 400 mg 4 times daily 60/300 mg qid 25–29 kg: 500 mg 4 times daily 72/360 mg qidAdults and children ≥30 kg: <60 kg: 500 mg 4 times daily 80/400 mg qid 60–80 kg: 1000 mg 3 times daily 160/800 mg tid >80 kg: 1000 mg 4 times daily 160/800 mg qid
153 Patients randomized to Cephalexin + TMP/SMX or placebo

Total Participants: 146Trimethoprim-Sulfamethoxazole n (% of total = 73)
Placebo n (% of total = 73)
Risk Difference % (95%CI) PValue
Cure (no failure by final follow-up at 30 d) (%) 62 (85) 60 (82) 2.7 (−9.3% to 15%) .66
Progression to abscess (%) 5 (6.8) 5 (6.8) 0 (−8.2% to 8.2%) 1.0
Any adverse event (%) 36 (49) 39 (53) −4.1 (−20% to 12%) .62
Diarrhea (%) 21 (29) 25 (34) −5.5 (−21% to 10%) .48
Nausea (%) 15 (21) 13 (18) 2.7 (−10% to 16%) .67
Vomiting (%) 5 (6.9) 8 (11) −4.1 (−13% to 5.1%) .38
Rash (%) 4 (5.5) 3 (4.1) 1.4 (−5.6% to 8.3%) .70
Pruritus (%) 5 (6.9) 3 (4.1) 2.7 (−4.6% to 10%) .47
Candidiasis (%) 1 (1.4) 3 (4.1) −2.7 (−8.0% to 2.5%) .31
Clostridium difficilecolitis (%) 0 (0) 1 (1.4) −1.4 (−4.0% to 1.3%) .32
Othera(%) 3 (4.1) 3 (4.1) 0 (−6.4% to 6.4%) 1.0

Non-culturable cellulitis(no purulent material or wound present)Suspected organisms: β-hemolytic strep, S. aureus
Cephalexin 500 mg PO q6h (<60kg), 1000 mg PO q8h (60-80kg), 1000 mg PO q6h (>80kg)
Dicloxacillin 500 mg PO q6h Penicillin allergy: clindamycin 300 mg PO q8h
Purulent cellulitis or cutaneous abscess (pus) OR h/o penetrating trauma, IVDU, MRSA infection elsewhereSuspected organisms: S. aureus (MRSA concern), β-hemolytic strep
Cephalexin 500 mg PO q6h (<60kg), 1000 mg PO q8h (60-80kg), 1000 mg PO q6h (>80kg) PLUS o TMP/SMX 1 single strength tab PO q6h
(<60kg), 1 double strength tab PO q8h (60-80kg), 1 double strength tab PO q6h (>80kg) OR
o Doxycycline 100 mg PO q12h Penicillin allergy: clindamycin 300 mg PO q8h

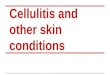
Recurrent Group A Strep cellulitis• Randomized, placebo-controlled of patients with at least 2
episode of leg cellulitis in previous 3 years, last recurrence in previous 24 weeks
• Randomized to;– PCN 250mg po BID or placebo X 12 months
• Primary outcome= Recurrence of cellulitis
Thomas KS ,et al. N Engl Jnl Med 2013;368:1695-1703

PCN prophylaxis for recurrent cellulitisPCN Placebo difference p
Median time to recurrence
626 days 532 days
Recurrence in first 12 months: prophylaxis phase
30/136 (22%) 51/138 (37%) -15% 0.01
Recurrence in years 2 and 3
26/97 (27%) 22/81 (27%) 0 0.78
NNT=5


Purulent cellulitis or cutaneous abscess (pus) OR h/o penetrating trauma, IVDU, MRSA infection elsewhereSuspected organisms: S. aureus (MRSA concern), β-hemolytic strep
Vancomycin 15 mg/kg IV q12h Vancomycin allergy:
o Ceftaroline 600 mg IV q12h (ID approval required)
o Daptomycin 500 mg IV q24h (not critically ill), 750 mg IV q24h (critically ill) (ID approval required) (STOP STATINS)
o Linezolid 600 mg IV or PO q12h (ID approval required) (NOT WITH SSRIs)

Detecting MRSA Colonization
• Study of 162 adults seeking care in ED for cutaneous abscesses
• 160 bilateral nares specimens , 142 inguinal specimens
• 19% of nares samples were positive• 26% of inguinal samples were positive• Combining culture sites detected 31% with
MRSA colonization
May L, et al. Diagn Mibrobiol Infect Dis 2014;80-79-82

DO PATIENTS WITH UNCOMPLICATED ABSCESSES NEED ANTIBIOTICS?

TMP/SMX vs placebo in patients following I&D of abscess
• Double-Blind RCT• >12 years of age• Lesion < 1 week• Lesion > or = 2cm in
diameter• Outpatient care
• Excluded:– Perineal lesion/bite– Foreign body– Chronic skin condition– Immunocompromised– Drug intolerance– Pregnancy
Talan DA, Moran GJ. ID WEEK 2014

TMP/SMX vs placebo in patients following I&D of abscess
• 1265 Patients randomized 1:1 to TMP/SMX 2 DS tabs po BID vs placebo x 7 days
• Primary Outcome: Test of cure visit Day 14-21• Secondary Outcomes:
– New skin infections– Fewer infections in household– Missed days of nl activity

TMP/SMX vs placebo in patients following I&D of abscess
Outcome TMP/SMX Placebo difference
Lesion cure rate 92.9% 85.7% -7.2% (95%CI 3.2-11.2)
New Skin infection -7.3%
Infections in household members
-2.4%
Missed days of nl activity
-0.4%
NNT to prevent 1 failure= 14

Recurrent MRSA Infections• Decolonization Regimen:
– Chlorhexidine washes daily x 7 days– Mupirocin 2% ointment to bilat ant nares TIDx 7 days– Rifampin 300mg po BID x 7 days– Doxycycline 100mg po BID x 7 days– Significantly lower MRSA colonization rate at 3 and 8 months
compared with placeboSimor AE et al. Clin Infect Dis 2007;44:178-185
Adjunctive Measures:1) FeSO4 supplementation if Iron deficiency anemia2) Vitamin C 1gm po daily- improved neutrophil function

Diabetic Foot Ulcers with Infection• Assess for arterial insufficiency and serious soft tissue
infections• Debride ulcers and get deep cultures (no superficial swabs)• Before any thought of MRI:
• If no findings of Osteo- treat for 2 weeks as SSTI• If Osteo treat for 6 weeks

Probe to Bone test

Chronic wounds, diabetic ulcerSuspected organisms: Strep, S.aureus, if chronic and previously treated Enteric GNR and Pseudomonas
Oral Therapy Choices: Cephalexin, Clinda, Levofloxacin, Augmentin
Parenteral Therapy: Ampicillin/sulbactam 3 g IV q6h Ertapenem 1 g IV q24h (ID approval required) If Pseudomonas concern:
o Piperacillin/tazobactam 3.375 g IV q8h infused over 4 hours
o If MRSA concern: consider vancomycin 15 mg/kg IV q12h
Penicillin allergy: vancomycin + levofloxacin 750 mg IV daily

Newly FDA-approved agents for Cellulitis
Dalbavancin (Dalvance) Oritavancin (Orbactiv) Tedezolid (Sivextro)
1000mg IV Day 1, 500mg on Day 8
1200mg IV X 1 200mg IV or po x 6 days
$ 4470 $2900 $235
Non-inferior to Vanco/Linezolid
Non inferior to 7-10 days of Vanco
Non inferior to linezolid
Efficacy good in Streptococcal Infections
Response rates in Strep infections don’t look as good
No SSRI interaction, less myelosuppressive
Clearance of bacteremia in patients with positive blood cxs
Increased LFT abnormalities
GI side effects, can see “red man” syndrome
Can falsely elevate PTT and PT, can increase risk of bleeding with warfarin

THE BAD

Predictors of bacteremia or poor outcome warranting admission
• Predictors of bacteremia or poor outcome warranting admission– Predictors of bacteremia:
• Absolute neutrophil count (ANC): Absolute lymphocyte count (ALC) > 10• ALC < 1000 cells/mm3
– Altered Mental status– Hypotension – Acute kidney injury (increase in creatinine 0.3 mg/dl from baseline) or a
new elevation in BUN >19mg/dl– Lactate > 2.5mmol/L– CRP > 13mg/L– CPK > 300 U/L (2X ULN)– Immunocompromised host– Non-compliant patient

Signs/Symptoms of complicated Skin/Soft Tissue Infections
-Unstable vital signs-Pain out of proportion to physical exam findings-Rapidly progressing cellulitis-Violaceous/ hemorrhagic bullae-Skin anesthesia-Skin sloughing-Gas in tissue-Cutaneous hemorrhage




Necrotizing Fasciitis TypesNF Type Incidence Etiology Organisms Clinical Progress
I 70-80% ImmunocompromisedAbdominal surgeryPeri-anal process
Polymicrobial-mixed aerobes, anaerobes, Pseudomonas, Bacteroides
More indolentBetter prognosis
II 20-30% Skin or throat derivedFollowing trauma or direct inoculationpharyngitis./ vaginitis/proctitis
Monomicrobial- Group A Strep, S. aureus
Easily missed, rapid progression, STSS
III rare Marine related organisms, seafood ingestion contaminated wounds
Vibrio vulnificusAeromonas
High mortality
IV rare Trauma, burns, immunocompromised
Candida, Zygomycetes
>47% mortality in immunocompromised
Machado NO. North American Journal of Medical Sciences 2011;3:107-118

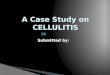
Six different variables included in the laboratory risk indicator for necrotizing fasciitis (LRINEC) score to help discriminate between necrotizing and nonnecrotizing soft-tissue
infections.
Goldstein E J C et al. Clin Infect Dis. 2007;44:705-710
© 2007 by the Infectious Diseases Society of America
Score >6 has a PPV of 92% and a NPV of 96%

Diagnosis
• The diagnosis of necrotizing fasciitis is surgical– Finger test:
• 2cm incision down to deep fascia under local anesthesia
• Index finger probing– Lack of bleeding– Dishwater pus– Lack of tissue resistance
– Radiologic tests are adjunct measures and one should not lose time waiting for a CT scan or MRI


Diagnosis –Rapid Ultrasound “STAFF exam”
• ST= subcutaneous thickening• A= air• FF= fascial fluid
– 88% sensitive and 93% specific for NF.
Castleberg E, et al. West J Emerg Med 2014;15:111-113

The Importance of Timely DebridementTime from DX to surgery
Adjusted OR 95%CI p value
< or = 14 hours 1 -
>14 hours 34.5 2.05-572 0.007
33 patients with NSTI and septic shock
Boyer A et al. Intensive Care Med 2009;35:847-853

Necrotizing fasciitis
ID consultation Piperacillin/tazobactam 3.375 g IV q8h infused
over 4 hours PLUS clindamycin 900 mg IV q8h (ID approval required)
Meropenem 500 mg IV q6h PLUS clindamycin 900 mg IV q8h (ID approval required)
Penicillin allergy: consider levofloxacin + clindamycin or aztreonam + clindamycin (ID approval required)
If MRSA concern: consider vancomycin 15 mg/kg IV q12h
Proven Group A Strep infection: Aqueous PCN G 2-4 MU IV q4h PLUS clindamycin 900 mg IV q8h (ID approval required)

Clindamycin & IVIG: Role in Group A Strep Necrotizing Fasciitis
• 84 cases of invasive Group A Strep infection of which 29 were necrotizing fasciitis
• 30 day mortality:– Clindamycin + IVIG= 7%– Clindamycin= 15%– No Clinda= 39%
Carapetis JR, et al Clin Infect Dis 2014:59:358-365

Cat Bite
- Deep penetrating injury
- Multiple Organisms including Pasteurella and anaerobes
- Often need surgery


Human BitesSuspected organisms: S. viridans S. aureus, Haemophilus spp., Eikenella corrodens, Peptostreptococcus, Fusobacterium, Porphyromonas, Prevotella
Ampicillin/sulbactam 3 g IV q6h Cefoxitin 2 g IV q8h Clindamycin 900 mg IV q8h (ID approval
required) PLUS o Levofloxacin 750 mg PO q24h OR o TMP/SMX DS 1 tab PO q12h
Animal BitesDog/cat bite suspected organisms: Pasteurella multocida, streptococci, staphylococci, Fusobacterium, Bacteroides, Porphyromonas, Prevotella Consider Capnocytophaga canimorsus in splenectomized dog bite patients.
Ampicillin/sulbactam 3 g IV q6h Ceftriaxone 1 g (2 g if >80kg) IV q24h +
metronidazole 500 mg IV q8h Levofloxacin 750 mg IV q24h + metronidazole
500 mg IV q8h

ODD DUCKS

ERYSPELIOID
-Eryspelothrix rhusopathiae- Gram positive rods-Animal Exposure- including pigs and fish-Disease of butchers and fisherman and fishmongers-Usually confined to a finger-PCN is drug of choice

Sporotrichosis
-Sporothrix schenkii- dimorphic fungus-”Rose Growers” disease-rose thorns, sphagnum moss, soil, timber-subcutaneous nodules along lymphatics-Treatment is Itraconazole

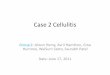
Ecthyma gangrenosum
- Occurs in immunocompromised host
- Usually chemo with prolonged neutropenia
- Pseudomonas aeruginosa to blood vessel and surrounding dermis
- Erythematous macule to hemorrhagic bullae then ulcerates with erythematous halo
- Treatment is anti-pseudomonal antibiotics
- Surgical debridement if doesn’t respond

Mimickers of Cellulitis





Pyoderma gangrenosum

Erythema migrans