Embed Size (px)
Citation preview
Christian Connections for International Health Conference 2015
Presentation by: Mrs. Patricia Kamara
Executive Director – CHAL
June 28, 2015
Reaching the most Disadvantaged CHAL‘s Response to the Ebola Outbreak in Liberia
Understanding the Context The Ebola Epidemic in Liberia Impact of Ebola Overview of CHAL CHAL’s Interventions Results Recommendations
Liberia - a case of the most disadvantaged
Already among the five poorest nations in Africa, Liberia is a low income country (LIC) with a gross domestic product (GDP) per capita of US$ 471.8 (IMF: 2012)
Nearly 14-year civil war (1989 to 2003) killing
around 250.000 people Fragile health system – poor heath
indicators, infrastructure shattered, dependence on international orgs and FBOs for provision of services
Families increasingly exposed to hardship with
about 56% of the country’s 4.2 million population living on less than 1USD daily (Purchasing Power Parity)
Strong Christian, traditional and cultural beliefs.
Health workers (45 physicians/1000 population) Health service delivery( 656 health facilities- 404 are public health and
252 private: Faith based, concession and private individual ) Shortages of medicines and medical supplies Poor Community engagement


Health workers As of May 6, 2015 there were 4,716 deaths. 370 health workers were infected, 198 survived EVD
infection and 178 died including doctors, nurses, midwives, lab-technicians, pharmaceutical staff, cleaners, ambulance drivers, clerks (Health Assessment Draft Report: 2015).
Survivor health workers traumatised
Health Service delivery Closure (partially, short and long terms) of health facilities
o E.g. St Joseph Catholic Hospital, e.g. Phebe Hospital o Most government hospitals were closed, FBO facilities remained open o Lack of normal health services leading to the death of children and adults due to o Malaria, pneumonia, diarrhoea etc. o Pregnant women could not get assistance o Interruption of routine services such as immunisation, ART, TB Therapy, Diabetic care etc. KKEEP SAFE – KEEP SERVING
Medicine and medical supplies o Shortages or lack of essential medicines, PPEs and other medical supplies
Communities engagement o Distrust in the health system o Poor attendance at health facilities SAFE – KEEP SERVING
The Ebola outbreak disrupted potential growths; reducing GDP forecast of 5.9% to
2.5% (World Bank: 2014) Adverse impact on the food security of the nation Economic impact including loss of income for families, businesses and government
revenue
Disruption of the education calendar year leading to closure of schools
Other social impact in terms of family separation, reduced social services (water, electricity, transport) and limitation on social gatherings (funeral, wedding, sports and etc)

Founding: CHAL was founded in 1975 by the medical authorities of four church-
based hospitals (Lutheran, Episcopal, Methodist and ELWA (SIM)).
Purpose: Provide advocacy, facilitation and assistance to improve quality of health care services from members’ facilities to their local communities.
Membership: 58 Health Facilities (5 hospitals, 8 health centers and 45 clinics) in 12 of 15 counties. Health Care Workers: 2,236 health workers out of 9,587 health workers
Coverage: ~25 – 30 % of vulnerable populations in rural hard to reach areas Vision: To ensure “access to health care services and healing for people in Liberia” Mission: The mission of CHAL is “dedication to the healing ministry of our Lord and
Saviour Jesus Christ through advocacy, facilitation and providing holistic Christian health care services to people in Liberia.”


Community Engagement IPC and raising awareness on Ebola
o Trained 450 health care providers; 988 general community health volunteers (gCHVs); and 155 Religious and Community Leaders
Social and behavioural change and communication
o Religious Messaging through songs and preaching, posters flyers, jingles, sound truck o Conducted Ebola prevention awareness campaign in 109 communities in the 4 worst affected
counties.
Financial Assistance to Ebola survivors o Provided financial support to 300 Ebola survivors in 4 counties


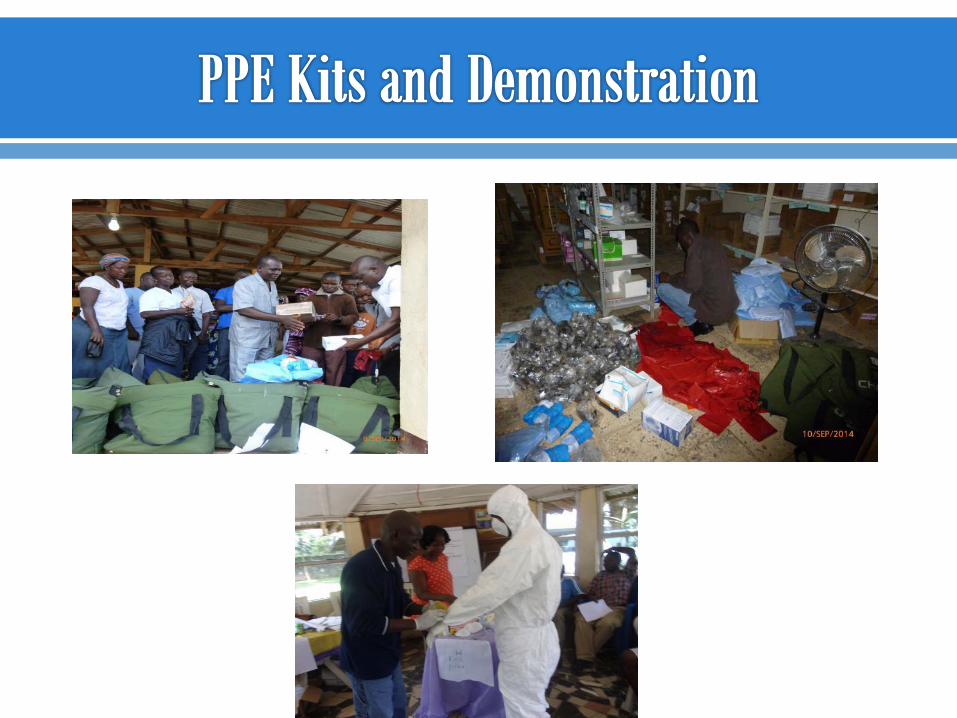
KEEP SAFE – KEEP SERVING Procurement and distribution of PPEs , essential medicines and supplies
o Distributed PPEs worth $269,563 o Distributed 17 containers of assorted medicines and medical supplies to 81 health
facilities in the 15 counties of Liberia Provision of Risk allowance to Health Workers
o Provided risk allowance to medical staff in 26 health facilities for nine months and gCHVs in 26 health facilities catchment communities
Health facility strengthening
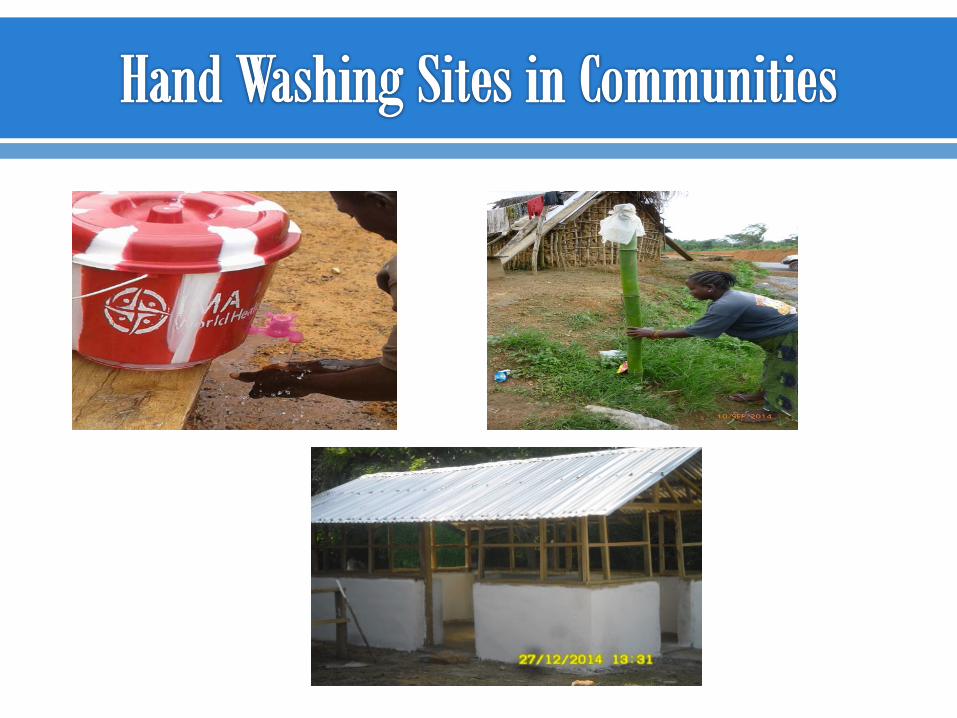
o Installation of hand washing stations at hospitals at public places in the communities.
o Construction of a triage in Gbarnga, Bong County o Donated 12 motorbikes to 12 health facilities in 4 counties as well as 1 ambulance
to Forya Bormah( to enhance community based activities) o Improved access to water, electricity and sanitation in 21 health facilities

Stronger relations with government, donor and international partners has increased CHAL membership from 48 to 58 health facilities and donors from 1 to 3
Built more trust in the CHAL secretariat among member institutions Restored the confidence of health workers and facilitated their return
to work
Restored community confidence in the health care delivery system and built their resilience in the fight against Ebola through engagement with religious leaders as well as community volunteers
Build a productive health workforce that is appropriately motivated o Place health workers on payroll o Accelerate needs-based recruitment and retention(social protection
packages, incentives) o Improve health workers capabilities in line with needs (inservice training,
post-graduate education and training, scholarships)
Strengthen epidemic preparedness and response system o Put in place surveillance and early warning and response structures
Strengthen the drug procurement and distribution system

Re-engineer health infrastructure to meet population needs for health services: o Infrastructural improvements to ensure facilities are appropriate for
outbreak response o Quality health service delivery (isolation rooms, waste management, water
and electricity) Continue investing in CHAL and member facilities
o Sustain its role in strengthening communities o Provision of emergency response to outbreaks and quality health care
services